
Efficacy of Maxillary Expansion with Clear Aligner in the Mixed Dentition: A Systematic Review

 ,
,  ,
,  , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Information Sources
2.3. Search Strategy
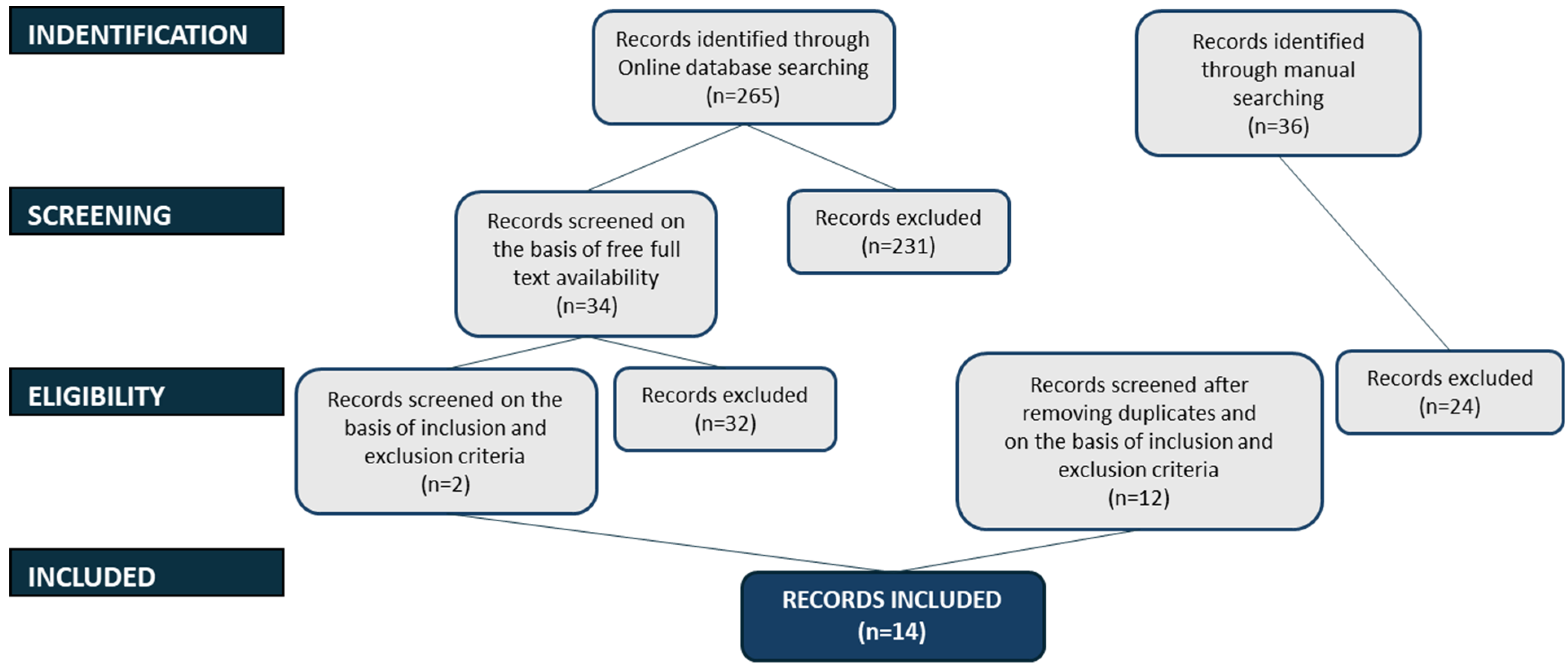
2.4. Selections Process
2.5. Data Collection Process
- Study features: authors, year and source of publication, study design;
- Sample characteristics: size, gender, and age of the population;
- Clinical evaluation characteristics: type of measured outcomes;
- The type of intervention;
- Characteristics of the results: Maxillary arch changes.
2.6. Data Items
2.7. Study Risk of Bias Assessment
2.8. Effect Measures and Synthesis Methods
2.9. Certainty Assessment
3. Results
3.1. Study Characteristics
Type of Study and Location
3.2. Characteristics of the Participants
3.3. Characteristics of the Intervention and Comparisons
3.4. Characteristics of the Outcomes
3.5. Reporting Bias Assessment
3.6. Assessment of Risk of Bias Within Studies and Quality of Evidence
3.7. Overall Risk
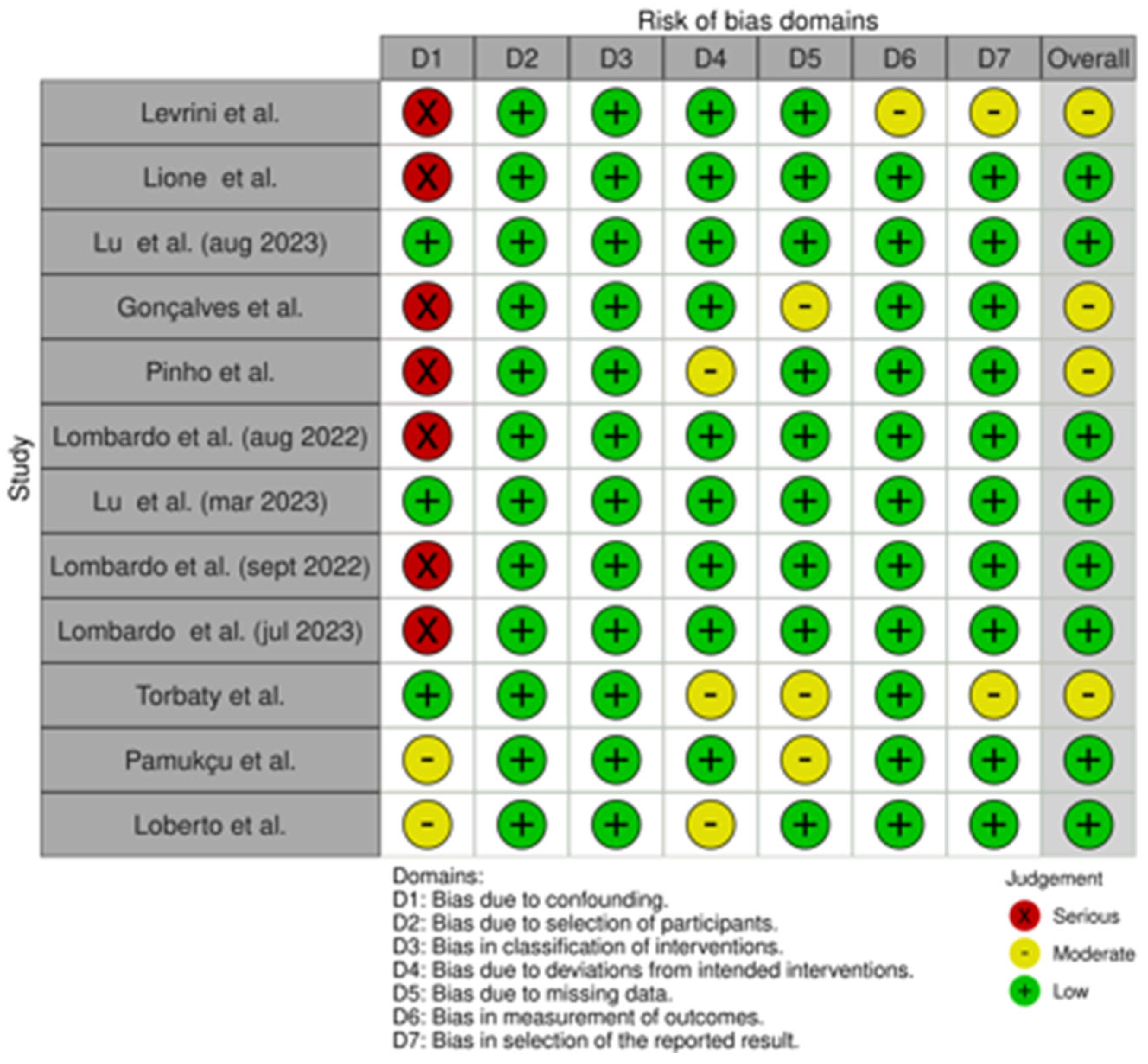
- Levrini et al. [7] was considered at moderate risk of bias because it showed a high risk of bias in D1 and a moderate risk in D6 and D7.
- Lione et al. [27] was considered at low risk of bias because it only showed a high risk of bias in D1.
- Lu et al. [29] was considered at low risk of bias because it showed a low risk in all domains.
- Gonçalves et al. [30] was considered at moderate risk of bias because it showed a high risk of bias in D1 and a moderate risk in D5.
- Pinho et al. [9] was considered at moderate risk of bias because it showed a high risk of bias in D1 and a moderate risk in D4.
- Lombardo et al. [11] was considered at low risk of bias because it only showed a high risk of bias in D1.
- Lu et al. [28] was considered at low risk of bias because it showed a low risk in all domains.
- Lombardo et al. [15] was considered at low risk of bias because it only showed a high risk of bias in D1.
- Lombardo et al. [26] was considered at low risk of bias because it only showed a high risk of bias in D1.
- Torbaty et al. [19] was considered at moderate risk of bias because it showed a moderate risk of bias in D4, D5 and D7.
- Pamukçu et al. [25] was considered at low risk of bias because it only showed a moderate risk of bias in D1 and D5.
- Loberto et al. [18] was considered at low risk of bias because it only showed a moderate risk of bias in D1 and D4.
3.8. Certainty of Evidence and Risk of Reporting Biases in Syntheses
4. Discussion
4.1. Intercanine Width
4.2. Intercanine Transpalatal Width
4.3. First and Second Interdeciduous Molar Width
4.4. Second Interdeciduous Molar Width, First Interpremolar Width, and Intercanine Dentoalveolar Width
- -
- Intercanine dentoalveolar width (from the most prominent buccal bulge on the alveolus superior to the maxillary first canine)
- -
- Second interdeciduous molar width (linear distance between the sulcus of the second deciduous molars, deciduous teeth were substituted when present)
- -
- First interpremolar width (linear distance between the buccal cusp tips of the first premolars)
4.5. First and Second Interdeciduous Molar Transpalatal Width
4.6. First Intermolar Mesial Width
4.7. First Intermolar Distal Width
4.8. First Intermolar Transpalatal Width
4.9. Molar Inclination, Arch Depth, and Arch Perimeter
4.10. Intermolar Dentoalveolar Width
4.11. First and Second Interdeciduous Molar Width, First and Second Interpremolar Width, and First Intermolar Width
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bruni, A.; Ferrillo, M.; Gallo, V.; Parrini, S.; Garino, F.; Castroflorio, T.; Deregibus, A. Efficacy of clear aligners vs. rapid palatal expanders on palatal volume and surface area in mixed dentition patients: A randomized controlled trial. Am. J. Orthod. Dentofac. Orthop. 2024, 166, 203–214. [Google Scholar] [CrossRef]
- Bruni, A.; Gallo, V.; Parrini, S.; Ferrillo, M.; Garino, F.; Deregibus, A.; Castroflorio, T. Effectiveness of Aligners Versus Rapid Palatal Expander on Palatal Volume in Mixed Dentition Patients: A Randomized Controlled Trial. Res. Sq. 2022. [Google Scholar] [CrossRef]
- Artese, F. A broader look at Interceptive Orthodontics: What can we offer? Dent. Press. J. Orthod. 2019, 24, 7–8. [Google Scholar] [CrossRef]
- Oancea, R.; Funieru, C.; Sfeatcu, R.; Jumanca, D. Interceptive Orthodontics in Primary and Mixed Dentition: The Importance of Early Diagnosis. Jurnalul Pediatrului 2019, 18. [Google Scholar]
- Lione, R.; Gazzani, F.; Moretti, S.; Danesi, C.; Cretella Lombardo, E.; Pavoni, C. Gingival Margins’ Modifications during Orthodontic Treatment with Invisalign First((R)): A Preliminary Study. Children 2022, 9, 1423. [Google Scholar] [CrossRef]
- Howe, R.P.; McNamara, J.A., Jr.; O’Connor, K.A. An examination of dental crowding and its relationship to tooth size and arch dimension. Am. J. Orthod. 1983, 83, 363–373. [Google Scholar] [CrossRef] [PubMed]
- Levrini, L.; Carganico, A.; Abbate, L. Maxillary expansion with clear aligners in the mixed dentition: A preliminary study with Invisalign(R) First system. Eur. J. Paediatr. Dent. 2021, 22, 125–128. [Google Scholar] [CrossRef]
- McNamara, J.A. Maxillary transverse deficiency. Am. J. Orthod. Dentofac. Orthop. 2000, 117, 567–570. [Google Scholar] [CrossRef]
- Pinho, T.; Rocha, D.; Ribeiro, S.; Monteiro, F.; Pascoal, S.; Azevedo, R. Interceptive Treatment with Invisalign((R)) First in Moderate and Severe Cases: A Case Series. Children 2022, 9, 1176. [Google Scholar] [CrossRef]
- Bouserhal, J.; Bassil-Nassif, N.; Tauk, A.; Will, L.; Limme, M. Three-dimensional changes of the naso-maxillary complex following rapid maxillary expansion. Angle Orthod. 2014, 84, 88–95. [Google Scholar] [CrossRef]
- Cretella Lombardo, E.; Paoloni, V.; Fanelli, S.; Pavoni, C.; Gazzani, F.; Cozza, P. Evaluation of the Upper Arch Morphological Changes after Two Different Protocols of Expansion in Early Mixed Dentition: Rapid Maxillary Expansion and Invisalign((R)) First System. Life 2022, 12, 1323. [Google Scholar] [CrossRef]
- Kilic, N.; Oktay, H. Effects of rapid maxillary expansion on nasal breathing and some naso-respiratory and breathing problems in growing children: A literature review. Int. J. Pediatr. Otorhinolaryngol. 2008, 72, 1595–1601. [Google Scholar] [CrossRef] [PubMed]
- Machado-Junior, A.J.; Zancanella, E.; Crespo, A.N. Rapid maxillary expansion and obstructive sleep apnea: A review and meta-analysis. Med. Oral Patol. Oral Cir. Bucal 2016, 21, e465–e469. [Google Scholar] [CrossRef] [PubMed]
- Rutili, V.; Nieri, M.; Franceschi, D.; Pierleoni, F.; Giuntini, V.; Franchi, L. Comparison of rapid versus slow maxillary expansion on patient-reported outcome measures in growing patients: A systematic review and meta-analysis. Prog. Orthod. 2022, 23, 47. [Google Scholar] [CrossRef]
- Lombardo, E.C.; Fanelli, S.; Paoloni, V.; Cozza, P.; Lione, R. Comparison between two different expansion protocols in early mixed dentition:Clear Aligners vs. Rapid Maxillary Expansion. Semin. Orthod. 2022. [Google Scholar] [CrossRef]
- Rossini, G.; Parrini, S.; Castroflorio, T.; Deregibus, A.; Debernardi, C.L. Efficacy of clear aligners in controlling orthodontic tooth movement: A systematic review. Angle Orthod. 2015, 85, 881–889. [Google Scholar] [CrossRef] [PubMed]
- Weir, T. Clear aligners in orthodontic treatment. Aust. Dent. J. 2017, 62 (Suppl. S1), 58–62. [Google Scholar] [CrossRef]
- Loberto, S.; Pavoni, C.; Fanelli, S.; Lugli, L.; Cozza, P.; Lione, R. Predictability of expansion movements performed by clear aligners in mixed dentition in both arches: A retrospective study on digital casts. BMC Oral Health 2024, 24, 694. [Google Scholar] [CrossRef]
- Moravedje Torbaty, P.; Suh, H.; Tai, S.K.; Baird, M.; Boyd, R.L.; Oh, H. Vertical and transverse treatment effects of Invisalign First system compared to Hyrax maxillary expanders with fixed appliances in mixed dentition patients. Angle Orthod. 2024, 94, 496–503. [Google Scholar] [CrossRef]
- Galluccio, G.; De Stefano, A.A.; Horodynski, M.; Impellizzeri, A.; Guarnieri, R.; Barbato, E.; Di Carlo, S.; De Angelis, F. Efficacy and Accuracy of Maxillary Arch Expansion with Clear Aligner Treatment. Int. J. Environ. Res. Public Health 2023, 20, 4634. [Google Scholar] [CrossRef]
- Lin, E.; Julien, K.; Kesterke, M.; Buschang, P.H. Differences in finished case quality between Invisalign and traditional fixed appliances. Angle Orthod. 2022, 92, 173–179. [Google Scholar] [CrossRef] [PubMed]
- Lynch, N.M.; Shroff, B.; Carrico, C.K.; Sawicki, V.; Sabol, M.; Lindauer, S.J. Clear aligner therapy in the mixed dentition: Indications and practitioner perspectives. Am. J. Orthod. Dentofac. Orthop. 2023, 164, 172–182. [Google Scholar] [CrossRef] [PubMed]
- Papadimitriou, A.; Mousoulea, S.; Gkantidis, N.; Kloukos, D. Clinical effectiveness of Invisalign(R) orthodontic treatment: A systematic review. Prog. Orthod. 2018, 19, 37. [Google Scholar] [CrossRef]
- Upadhyay, M.; Arqub, S.A. Biomechanics of clear aligners: Hidden truths & first principles. J. World Fed. Orthod. 2022, 11, 12–21. [Google Scholar] [CrossRef]
- Pamukcu, H.; Ozsoy, S.; Aksoy, P.C.; Polat Ozsoy, O. Evaluation of maxillary dimensional changes in the mixed dentition: Clear aligners vs. acrylic expanders. Angle Orthod. 2024, 94, 392–399. [Google Scholar] [CrossRef] [PubMed]
- Lombardo, E.C.; Fanelli, S.; Pavoni, C.; Cozza, P.; Lione, R. Maxillary Response Induced by Rapid Palatal Expansion vs. Clear Aligners: A Short-Term Retrospective Evaluation of the Dento-Alveolar Effects in Mixed Dentition. Appl. Sci. 2023, 13, 8675. [Google Scholar] [CrossRef]
- Lione, R.; Cretella Lombardo, E.; Paoloni, V.; Meuli, S.; Pavoni, C.; Cozza, P. Upper arch dimensional changes with clear aligners in the early mixed dentition: A prospective study. J. Orofac. Orthop. 2023, 84, 33–40. [Google Scholar] [CrossRef]
- Lu, L.; Zhang, L.; Li, C.; Yi, F.; Lei, L.; Lu, Y. Effects of maxillary expansion in mixed dentition with Invisalign First System and Hass: A prospective cohort study. Rev. Prepr. 2023. [Google Scholar] [CrossRef]
- Lu, L.; Zhang, L.; Li, C.; Yi, F.; Lei, L.; Lu, Y. Treatment effects after maxillary expansion using invisalign first system vs. acrylic splint expander in mixed dentition: A prospective cohort study. BMC Oral Health 2023, 23, 598. [Google Scholar] [CrossRef]
- Goncalves, A.; Ayache, S.; Monteiro, F.; Silva, F.S.; Pinho, T. Efficiency of Invisalign First(R) to promote expansion movement in mixed dentition: A retrospective study and systematic review. Eur. J. Paediatr. Dent. 2023, 24, 112–123. [Google Scholar] [CrossRef]
- Kirmayr, M.; Quilodran, C.; Valente, B.; Loezar, C.; Garegnani, L.; Franco, J.V.A. The GRADE approach, Part 1: How to assess the certainty of the evidence. Medwave 2021, 21, e8109. [Google Scholar] [CrossRef]
- Quilodran, C.; Kirmayr, M.; Valente, B.; Perez-Bracchiglione, J.; Garegnani, L.; Franco, J.V.A. The GRADE approach, Part 2: Evidence to decision frameworksoutlining decision-making in health. Medwave 2021, 21, e8182. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.; Kunz, R.; Brozek, J.; Alonso-Coello, P.; Montori, V.; Akl, E.A.; Djulbegovic, B.; Falck-Ytter, Y.; et al. GRADE guidelines: 4. Rating the quality of evidence--study limitations (risk of bias). J. Clin. Epidemiol. 2011, 64, 407–415. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Woodcock, J.; Brozek, J.; Helfand, M.; Alonso-Coello, P.; Glasziou, P.; Jaeschke, R.; Akl, E.A.; et al. GRADE guidelines: 7. Rating the quality of evidence--inconsistency. J. Clin. Epidemiol. 2011, 64, 1294–1302. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Woodcock, J.; Brozek, J.; Helfand, M.; Alonso-Coello, P.; Falck-Ytter, Y.; Jaeschke, R.; Vist, G.; et al. GRADE guidelines: 8. Rating the quality of evidence--indirectness. J. Clin. Epidemiol. 2011, 64, 1303–1310. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Brozek, J.; Alonso-Coello, P.; Rind, D.; Devereaux, P.J.; Montori, V.M.; Freyschuss, B.; Vist, G.; et al. GRADE guidelines 6. Rating the quality of evidence--imprecision. J. Clin. Epidemiol. 2011, 64, 1283–1293. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Montori, V.; Vist, G.; Kunz, R.; Brozek, J.; Alonso-Coello, P.; Djulbegovic, B.; Atkins, D.; Falck-Ytter, Y.; et al. GRADE guidelines: 5. Rating the quality of evidence--publication bias. J. Clin. Epidemiol. 2011, 64, 1277–1282. [Google Scholar] [CrossRef]
- McGuinness, L.A.; Higgins, J.P.T. Risk-of-bias VISualization (robvis): An R package and Shiny web app for visualizing risk-of-bias assessments. Res. Synth. Methods 2021, 12, 55–61. [Google Scholar] [CrossRef]
- Sterne, J.A.; Hernan, M.A.; Reeves, B.C.; Savovic, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savovic, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Participants |
|
| Intervention | Maxillary expansion treatment using Invisalign® First clear aligners |
| Comparison | Patients treated with other orthodontic expanders and patients not treated orthodontically |
| Outcome | Maxillary arch changes achievable with Invisalign® First treatment |
| Study design | Retrospective studies, prospective studies, preliminary studies, randomized controlled trials, and case series The exclusion criteria were: meta-analyses, systematic reviews, literature reviews, case reports, and expert opinions |
| References (Authors, Year of Publication) | Study Design | Sample Size and (Number of Female) | Mean Age ± DS and/or Interval (Years) | Type of Appliance Used | Measurement Technique | Average Duration of Treatment (Months) |
|---|---|---|---|---|---|---|
| Lu et al., 2023 [29] | Prospective cohort study | 51 (N.R.) IF group: 17 RME group: 17 NG group: 17 | 6–10 | IF, RME | Digital Impression | 6 |
| Lione et al., 2023 [27] | Prospective study | 23 (9) | 9.4 ± 1.2 | IF | Digital Impression | 8.1 |
| Gonçalves et al., 2023 [30] | Retrospective study | 24 (13) | 6–12 | IF | Digital Impression | 18 |
| Levrini et al., 2021 [7] | Preliminary study | 20 (12) | 8.9 (ranged from 6.9 to 11.2) | IF | Digital Impression | 8 |
| Pinho et al., 2022 [9] | Case series | 23 (13) | Children in the mixed dentition | IF | Digital Impression | 18 |
| Lombardo et al., 2022 [11] | Retrospective study | 32 (17) IF group: 15 (8) RME Group: 17 (9) | RME group: 8.1 ± 0.8 IF group: 8.4 ± 1.1 | IF, RME | Digital Impression | 8 |
| Bruni et al., 2022 [2] | Randomized Controlled Trial | 39 (22) IF group: 19 (14) RME group: 20 (8) | IF group: 8.48 ± 1.42 RME group: 7.83 ± 1.19 | IF, RME | Digital Impression | IF group: 8 ± 3 RME group: 9 ± 2 |
| Lu et al., 2023 [28] | Prospective cohort study | 51 (N.R.) IF group: 17 RME group: 17 NG group: 17 | 6–10 | IF, RME | Digital Impression | 8 |
| Lombardo et al., 2022 [15] | Retrospective study | 32 (17) IF group: 15 (8) RME Group: 17 (9) | RME group: 8.1 ± 0.8 IF group: 8.4 ± 1.1 | IF, RME | Digital Impression | 8 |
| Lombardo et al., 2023 [26] | Retrospective study | 32 (17) IF group: 15 (8) RME Group: 17 (9) | RME group: 8.1 ± 0.8 IF group: 8.4 ± 1.1 | IF, RME | Digital Impression | 8 |
| Torbaty et al., 2024 [19] | Retrospective study | 120 (72) IF group: 40 (21) RME group: 40 (26) NG group: 40 (25) | IF group: 8.91 ± 1.2 RME group: 9.07 ± 1.08 NG group: 8.88 ± 1.25 | IF, RME | Digital Impression | IF group: 1.19 ± 0.45 RME group: 1.22 ± 0.46 NG group: 1.32 ± 0.51 |
| Bruni et al., 2024 [1] | Randomized Controlled Trial | 41 (22) IF group: 19 (14) RME group: 20 (8) | IF group: 8.48 ± 1.42 RME group: 7.83 ± 1.19 | IF, RME | Digital Impression | IF group: 8 ± 3 RME group: 9 ± 1 |
| Pamukçu et al., 2024 [25] | Retrospective study | 34 (20) IF group: 17 (11) RME group: 17 (9) | IF group: 8.79 ± 0.82 RME group: 8.83 ± 1.02 | IF, RME | Digital Impression | IF group: 7.66 ± 3.09 RME group: 8.86 ± 5.67 |
| Loberto et al., 2024 [18] | Retrospective study | 36 (20) | 8.3 ± 1.5 | IF | Digital Impression | 15 ± 2.2 |
| References (Authors, Year of Publication) | Inclusion Criteria | Exclusion Criteria | Type of Outcomes Evaluated |
|---|---|---|---|
| Lu et al., 2023 [29] |
|
|
|
| Lione et al., 2023 [27] |
|
|
|
| Gonçalves et al., 2023 [30] |
|
|
|
| Levrini et al., 2021 [7] |
|
|
|
| Pinho et al., 2022 [9] |
|
|
|
| Lombardo et al., 2022 [11] |
|
|
|
| Bruni et al., 2022 [2] |
|
|
|
| Lu et al., 2023 [28] |
|
|
|
| Lombardo et al., 2022 [15] |
|
|
|
| Lombardo et al., 2023 [26] |
|
|
|
| Torbaty et al., 2024 [19] |
| RME group:
|
|
| Bruni et al., 2024 [1] |
|
|
|
| Pamukçu et al., 2024 [25] |
|
|
|
| Loberto et al., 2024 [18] |
|
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Levrini, L.; Zecca, P.A.; Borgese, M.; Scurati, E.I.; Deppieri, A.; Saran, S.; Caccia, M.; Carganico, A. Efficacy of Maxillary Expansion with Clear Aligner in the Mixed Dentition: A Systematic Review. Appl. Sci. 2025, 15, 7233. https://doi.org/10.3390/app15137233
Levrini L, Zecca PA, Borgese M, Scurati EI, Deppieri A, Saran S, Caccia M, Carganico A. Efficacy of Maxillary Expansion with Clear Aligner in the Mixed Dentition: A Systematic Review. Applied Sciences. 2025; 15(13):7233. https://doi.org/10.3390/app15137233
Chicago/Turabian StyleLevrini, Luca, Piero Antonio Zecca, Marina Borgese, Eleonora Ivonne Scurati, Alessandro Deppieri, Stefano Saran, Margherita Caccia, and Andrea Carganico. 2025. "Efficacy of Maxillary Expansion with Clear Aligner in the Mixed Dentition: A Systematic Review" Applied Sciences 15, no. 13: 7233. https://doi.org/10.3390/app15137233
APA StyleLevrini, L., Zecca, P. A., Borgese, M., Scurati, E. I., Deppieri, A., Saran, S., Caccia, M., & Carganico, A. (2025). Efficacy of Maxillary Expansion with Clear Aligner in the Mixed Dentition: A Systematic Review. Applied Sciences, 15(13), 7233. https://doi.org/10.3390/app15137233