1. Introduction
Impacted teeth are often encountered during the diagnosis and treatment of malocclusions in adolescent orthodontic patients [
1]. Impaction occurs when a tooth does not erupt into its designated position in the dental arch within the expected developmental period. The upper canine is one of the teeth that mostly undergoes impaction, preceded only by third molars, with a prevalence range from 0.8% to 5.2% depending on the population examined. Canine impaction is more frequent on the palatal than labial side; it is twice as common in female than in male patients and it has a clear tendency toward being unilateral rather than bilateral [
2,
3].
The etiology of maxillary canine impaction is multifactorial: as reported by Becker and Chaushu [
4] in their review, different reasons concur to upper canine impaction such as local obstruction (e.g., odontoma, deciduous teeth, supernumerary teeth, etc.), local pathology (e.g., cysts, granuloma, etc.), the disturbance of normal development, malshaped or missing lateral incisors, crowded or delayed eruptive pathways, known as guidance theory, genetic factors, known as genetic theory, and environmental alterations.
Several authors independently reported a higher prevalence of palatal displacement of maxillary canines in cases where lateral incisors were congenitally absent. They hypothesized that the absence of the lateral incisor disrupts the normal eruptive guidance pathway of the canine, thereby facilitating its palatal migration. However, these conclusions were primarily derived from clinical observations rather than from systematic investigations involving large, well-defined cohorts and appropriately matched control groups [
5].
Supporting these initial impressions, a subsequent study conducted on a large sample of individuals with palatally displaced canines found that only about half of the subjects exhibited normally developed lateral incisors. The remaining half presented with lateral incisor anomalies, including agenesis, peg-shaped morphology, or microdontia. These findings are consistent with the earlier clinical observations and further suggest a strong association between lateral incisor abnormalities and the palatal displacement of maxillary canines [
6].
In accordance with the guidance theory and based on the previously discussed evidence, if the lateral incisor is absent, delayed in development, peg-shaped, or significantly undersized with only the initial stage of root formation, the canine will lack the proper guidance to follow its normal eruptive path. Consequently, the canine may deviate downward along a more palatal trajectory within the alveolar ridge, converging apically toward the medial aspect of the alveolar process. In this scenario, the periosteum in this region may serve as a secondary guide, promoting further eruption of the canine over the following one to two years. In cases where the lateral incisor is completely absent, the canine may undergo a self-correcting eruption along the natural curvature of the dental arch around the ages of 11–12 years. However, when a late-developing, aberrant lateral incisor is present and has already erupted, this self-correction mechanism is no longer available. Instead, the malformed incisor may act as a physical barrier, impeding the eruption of the canine by obstructing its path on the palatal side [
4].
The hypothesis that canine impaction is predominantly governed by genetic factors remains contentious and lacks widespread acceptance. If impaction were chiefly under genetic control, a symmetrical pattern of expression would be expected, resulting in a higher prevalence of bilateral impactions. Unilateral presentations would be anticipated only in a minority of cases, potentially attributable to differential gene expression or incomplete penetrance. Nonetheless, epidemiological data from a wide range of orthodontic studies consistently reveal a predominance of unilateral canine impaction, reported in approximately 60% to 75% of cases. This observed asymmetry undermines the notion of a strictly genetic etiology and suggests the involvement of additional environmental or local factors in the pathogenesis [
2,
7].
There is substantial evidence indicating that spontaneous alterations in the eruption path of the maxillary canine can occur as a result of changes in environmental conditions. Both the guidance theory and the genetic theory acknowledge that certain genetically influenced conditions, such as congenitally missing, peg-shaped, or undersized lateral incisors, spaced dentitions, and delayed dental development, are associated with the etiology of palatal displacement of the maxillary canine. The primary divergence between the two theories concerns their interpretation of the underlying etiological mechanism. The genetic theory posits that the palatal displacement of the canine is itself a genetically determined trait, representing one manifestation within a broader spectrum of genetically linked dental anomalies. In contrast, the guidance theory asserts that these traits constitute a genetically influenced environment that, by depriving the developing canine of its normal eruptive guide, predisposes it to deviate from its physiological eruption path [
4].
Based on the aforementioned evidence, it appears that the eruption pathway of the palatally displaced canine is not primarily under direct genetic control in most cases [
4].
An early diagnosis of ectopic eruption is essential for implementing preventive measures: the extraction of primary canines and/or creating space with the expansion of the upper dental arch [
8].
A variety of management strategies for palatally impacted maxillary canines have been described in the literature. Among these, the most widely adopted approach is a combined surgical–orthodontic protocol, which entails the surgical exposure of the impacted tooth followed by its guided orthodontic eruption into the dental arch.
Two principal surgical techniques are employed to achieve exposure of the palatally impacted canine: the open technique and the closed technique. The open technique involves the excision of the overlying palatal mucosa, thereby leaving the crown of the impacted tooth exposed to the oral environment. In contrast, the closed technique consists of raising a full-thickness mucoperiosteal flap to access the impacted tooth, after which an attachment is bonded to the crown and the flap is repositioned and sutured. This method facilitates the orthodontic traction of the tooth through a biologically favorable environment, ensuring eruption through an adequate band of keratinized gingiva, which is critical for long-term periodontal health [
9,
10].
In addition to conventional surgical techniques, the use of laser surgery has been proposed by numerous authors as a viable alternative to the traditional cold blade approach in dentistry. Laser-assisted procedures with high intensity laser therapy (HILT) offer several clinical advantages, including enhanced visibility of the surgical field, improved hemostasis, and greater precision in the management of delicate soft tissues. These benefits are particularly valuable in anatomically challenging or limited-access areas. As a result, laser surgery has increasingly gained acceptance and is currently employed by some clinicians as the preferred method for soft tissue management in the exposure of impacted teeth [
8,
9,
10].
The primary indication for HILT in orthodontics pertains to soft tissue procedures, including gingivectomy, frenectomy, and fiberotomy [
11].
Furthermore, lasers used for biostimulatory purposes—specifically for promoting regenerative and healing processes—are classified as low-level laser therapy (LLLT) devices and operate at power outputs below 500 milliwatts [
11].
Different authors [
12,
13,
14] studied the effectiveness of photobiomodulation therapy (PBMT), performed with a low-level intensity laser, on different orthodontic applications. It was found to be useful in accelerating tooth movement [
12], thanks to its cell-mediated alveolar bone remodeling induction; it also appeared to have a positive impact on the reduction of orthodontic treatment-related pain due to its analgesic, anti-inflammatory and biostimulant effects [
13], and minimized anchoring loss during orthodontic treatment [
14].
Research indicates that laser light promotes the proliferation of osteoclasts, osteoblasts, and fibroblasts, thereby influencing bone remodeling and accelerating tooth movement. The underlying mechanism behind this acceleration involves ATP production and the activation of cytochrome C. Studies [
15,
16,
17] have demonstrated that low-energy laser irradiation enhances tooth movement speed through the RANK/RANKL pathway and the expression of the macrophage colony-stimulating factor and its receptor.
PBMT influences the release of inflammatory mediators in periodontal tissues, enhances collagen synthesis, and stimulates the proliferation of osteoblasts and osteoclasts. This process promotes bone remodeling through the receptor activator of nuclear factor-kB ligand (RANKL)/RANK/osteoprotegerin pathway, ultimately accelerating orthodontic tooth movement [
18,
19,
20,
21].
Some studies have investigated the application of photobiomodulation therapy on impacted teeth, primarily focusing on its efficacy in reducing postoperative inflammation and pain. However, these investigations did not assess its potential role in enhancing or accelerating tooth movement [
22].
Despite the well-documented ability of low-level laser therapy to stimulate orthodontic tooth movement, its stimulation effect on impacted teeth movement—particularly palatally impacted maxillary canines—has not yet been thoroughly explored. Further research is warranted to evaluate the potential of PBMT as an adjunctive tool in facilitating the guided eruption of impacted elements.
In this case report, a patient with bilateral palatal impaction of the maxillary canines underwent surgical conventional exposure of both teeth. Following the surgery, only one of the canines received photobiomodulation therapy with a low-level laser, in accordance with a split-mouth protocol. Orthodontic traction was avoided on both dental elements to assess and compare only the extent of spontaneous eruption movement, without introducing variables that might interfere with these assessments. The objective of this study was to evaluate potential differences in eruption rate and extent between the canine treated with photobiomodulation therapy (PBMT) and the untreated canine in order to investigate the stimulatory effects of PBMT on tooth eruption.
2. Case Presentation
This case report was carried out on a 16-year-old male patient who was referred to the Department of Oral and Maxillo-Facial Sciences of “Sapienza” University of Rome to make an initial orthodontic examination in absence of symptomatology. The study was conducted in accordance with the Declaration of Helsinki and the protocol was approved by Institutional Ethics Committee of Sapienza University of Rome (#4389) on 22 June 2018.
A familiarity for included canines on the paternal side was noted in the medical history.
The clinical evaluation revealed that the maxillary primary canines persisted, and there was no noticeable prominence, suggesting the eruption of the permanent canines.
Orthopanoramic X-ray (
Figure 1) showed the impaction of both permanent maxillary canines. The patient had no symptoms or discomfort related to dental inclusions.
Cone Beam Computed Tomography (CBCT) was requested from the patient at the beginning of therapy to accurately evaluate the case before surgery.
Canines’ impaction prognosis was analyzed on OPT according to Ericson and Kurol analysis. The major axis of the canine and perpendicular to the alveolar margin, imagining this as the axis of the canine in its presumed ideal seat, were plotted on OPT and the α angle was calculated for both the impacted canines. Element 1.3 had an angle of 40°, while the angle of element 2.3 was 37°. Therefore, both canines have a negative prognosis according to Ericson and Kurol.
CBCT showed a palatal and osteomucosal impaction with mesio-inclination of both upper canines, close to the roots of central and lateral incisors (
Figure 2).
Three-dimensional digital impressions were performed with the intraoral scanner Medit i700 (Medit Corp., Seoul, Republic of Korea) and the initial photos were taken (
Figure 3). The patient was informed through surgical consent about the risks and benefits of the operation.
After collecting the initial documentation, the patient underwent the surgical procedure. Initially, local anesthesia was performed with 2% mepivacaine and 1:100,000 adrenaline solution. Subsequently, a cold blade was used to perform the operculectomy on the elements 1.3 and 2.3. This technique exposes the crown of the impacted teeth by cutting the tissue surface and then raising the palatal mucosa using a periosteal elevator. Afterwards, the osteotomy is performed using a handpiece with an ISO 018 diameter rosette bur (Maillefer®, Ballaigues, Switzerland), and simultaneously, abundant saline solution irrigates the spot to prevent the tissues from overheating. The crown of the canines was progressively uncovered by directing the drill tangentially along the bone surface (
Figure 4).
Once the surgical procedure was completed, element 2.3, exposed on the palatal surface, was stimulated through PBMT, and finally a periodontal compress (Coe-Pak, GC Dental, Tokyo, Japan) was applied to cover and protect the treated area. No orthodontic anchoring and traction were placed on the canines’ exposed surfaces.
The patient was advised not to eat anything hot or spicy and to only eat plain foods, and to also refrain from brushing the surgical site for a full day.
Check-up appointments after surgery were organized as follows: one week (T1), four weeks (T2), eight weeks (T3), and sixteen weeks (T4) (
Figure 5).
During each control, a clinical evaluation was carried out and intraoral photos of canine eruption were taken. Intraoral scans were performed to monitor the eruption movements of the canines at T4. At T1 the periodontal patch was removed, and the patient did not report pain, discomfort, or the necessity to take painkillers.
Additional PBMT was performed at T2 and T3, for a total of three photobiomodulation sessions, only for the element 2.3.
PBMT was performed using a Lumix 2 laser device (Fisioline, Verduno, Italy), which is a bidiodic laser; this combines a high-power laser diode in the pulsed infrared wavelength and continuous laser diode in the red wavelength, which allows energy to be transmitted to the tissue at different subcutaneous levels.
The LUMIX 2 laser was used at a wavelength of 910 nm with a total energy fluence of 12 J/cm2, a super-pulsed frequency of 30 kHz, and a total energy delivery of 180 J to stimulate deep tissues and accelerate orthodontic tooth movement for a 15 min-long session on the exposed teeth. All the laser sessions were performed by the same operator.
No pain was reported and no inflammation was evident following PBMT.
The DICOM files from the initial CBCT were converted into an STL file through an open-source software called 3D Slicer (version 5.8.1) and this was used as a starting point (T0) to assess the movement of the canines following surgery. The STL file of the intraoral scans and of the CBCT were imported and superimposed to perform a comparison between the starting (T0) and final (T4) canines’ position. The accuracy of 3D Slicer in measuring orthodontic tooth movement has been confirmed in multiple studies, demonstrating sub-millimetric precision when using CBCT image registration and digital surface models [
23,
24].
In light of its accuracy reported in the literature, it was chosen as the software to perform the measurements of this study.
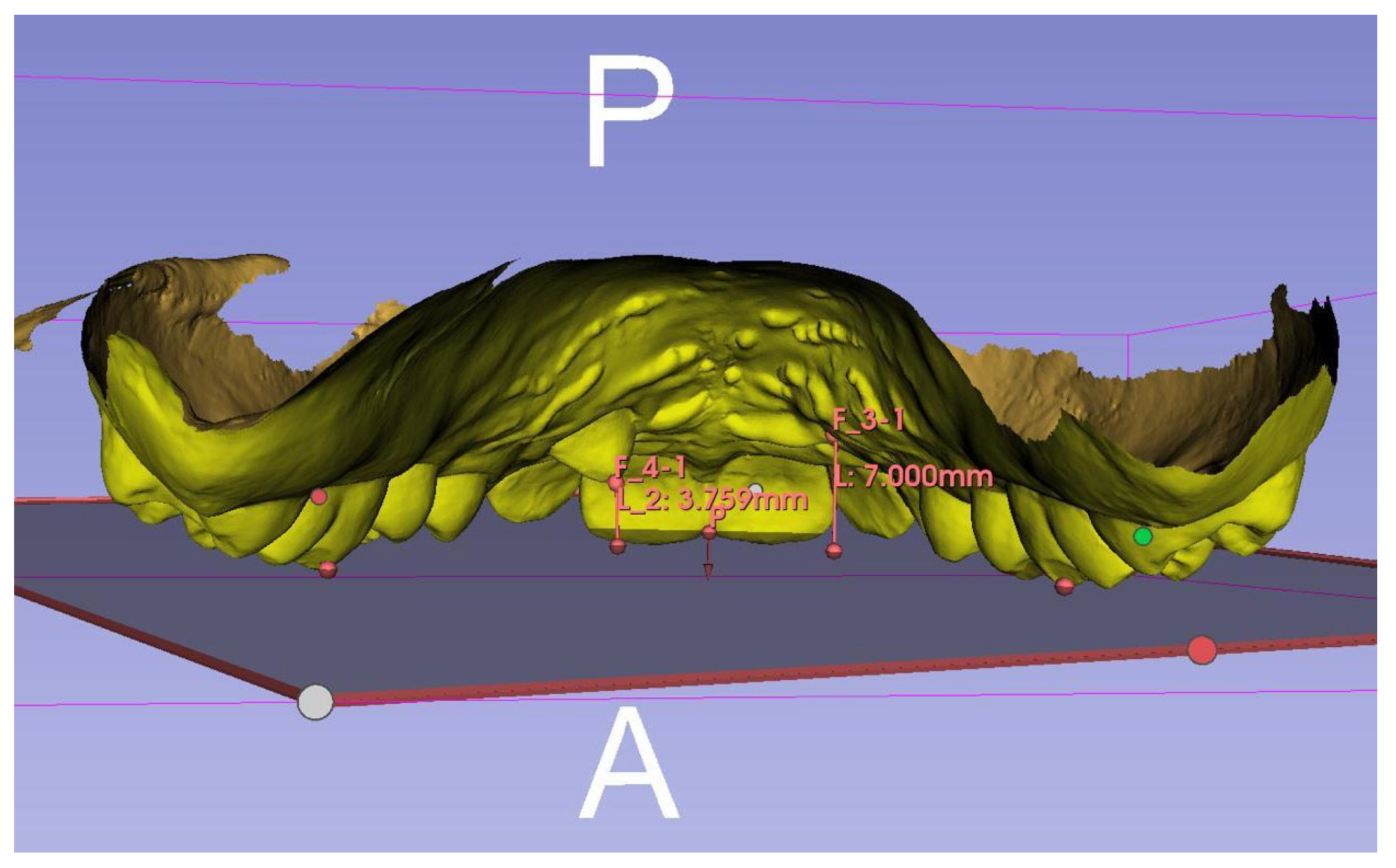
The 3D Slicer measuring tool was used for both STL files to quantify the distance between the occlusal plane and the canine cusp at T0 and T4 and so verified the actual eruption movement (
Figure 6).
This measurement was performed by tracing the occlusal plane using three reference points: the mesial–palatal cusps of the upper first molars and the incisal edge of the upper incisors in correspondence with the inter-incisive midline. A line was then drawn perpendicularly from the cusps of the impacted maxillary canines to the occlusal plane, obtaining the millimetric value of canine inclusion height. In this case, element 1.3 had an inclusion height of 7.21 mm, while element 2.3 had a height of 6.92 mm. At T4 the inclusion height of element 1.3 was 7.00 mm and of element 2.3 was 3.76 mm; this means that the canine eruption was of 0.21 mm for 1.3 and 3.16 mm for 2.3 (
Figure 7). Since this is a case report, no statistical analysis was performed.
3. Discussion
Many authors have extensively investigated the surgical disinclusion approach with a cold blade in the absence of orthodontic traction. Kokich et al. used this technique in their study and reported that it facilitates the spontaneous eruption of palatally impacted canines. They reported that within six to eight months, the canine crown naturally emerges into the palate without the need for fixed or removable orthodontic devices. Typically, the crown erupts at a distance from the roots of the central and lateral incisors, moving toward the center of the palate [
25]. It was therefore decided to use this surgical protocol in this case report.
In addition, there are several studies demonstrating the biostimulation effects of a low-intensity laser (PBMT), which results in speeding up tooth movement when applied in the orthodontic field. Photobiomodulation therapy modulates the inflammatory response in periodontal tissues, boosts collagen production, and encourages the growth of osteoblasts and osteoclasts. These effects support bone remodeling via the RANKL/RANK/osteoprotegerin signaling pathway, thereby contributing to a faster rate of orthodontic tooth movement. Research indicates that laser light promotes the proliferation of osteoclasts, osteoblasts, and fibroblasts, thereby influencing bone remodeling and accelerating tooth movement [
26,
27,
28].
Despite the well-documented ability of low-level laser therapy to stimulate orthodontic tooth movement, its stimulation effect on impacted teeth movement—particularly palatally impacted maxillary canines—has not yet been thoroughly explored.
The objective of this study was to evaluate potential differences in eruption rate and extent between the element 2.3 treated with photobiomodulation therapy (PBMT) and the untreated element 1.3 in order to investigate the effects of PBMT on tooth eruption.
At the end of the monitoring time of 16 weeks, at T4, the inclusion height of element 1.3 was 7.00 mm and of element 2.3 was 3.76 mm. This means that the canines erupted to an extent of 0.21 mm and 3.16 mm, respectively.
The difference in eruption between the PBMT-treated element and the non-irradiated element is therefore evident. In addition, element 1.3, undergoing operculectomy with a cold blade, erupted poorly in comparison to that reported by Kokich, suggesting the possible influence of other factors on the response of the canine after surgery. It is important to consider that various factors may influence the differential eruptive response between the two sides, particularly the initial position, depth, and angulation of the impacted canines. However, by employing a split-mouth study design, it was possible to compare two elements within the same subject, thereby eliminating interindividual variability—one of the most unpredictable factors in clinical outcomes.
The results suggest a positive effect of low-intensity laser application on the autonomous eruption of impacted canines toward the occlusal plane following conventional surgical exposure. Unlike the traditional approach, which typically requires surgical exposure followed by mechanical orthodontic traction, PBMT could have the potential to biologically stimulate the eruption process without the need for physical force application.
The combined use of surgery and PBMT may offer several advantages. First, it can significantly reduce overall treatment time by accelerating the natural eruptive movement, as PBMT has been shown to stimulate cellular activity in the periodontal ligament, increase vascularization, and enhance bone remodeling. Second, it may eliminate or substantially minimize the need for orthodontic traction, thereby reducing the mechanical stress on surrounding tissues and lowering the risk of root resorption, tissue irritation, and anchorage loss [
21,
22].
Additionally, this biologically driven approach can improve patient comfort and compliance by avoiding the discomfort and esthetic concerns often associated with prolonged orthodontic appliances. Fewer clinical visits and simpler post-surgical management may also contribute to better patient adherence and satisfaction.
While these benefits are promising, randomized controlled trials are necessary to confirm the effectiveness of PBMT in replacing or reducing orthodontic traction, to determine optimal treatment protocols, and to establish long-term outcomes compared to conventional methods.


 ,
, 

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}