
Pathogenesis of Psoriasis vulgaris and Current Management and Therapeutic Strategies Including the Role of Emollients—A Review of the Current Literature

 ,
,  , , and
, , and
Abstract
1. Introduction
2. Mechanisms of Changes Occurring in Psoriatic Skin—Characteristics of the Clinical Picture of Psoriasis
3. Ways to Assess Psoriasis Severity and Therapeutic Strategies for Psoriasis Treatment
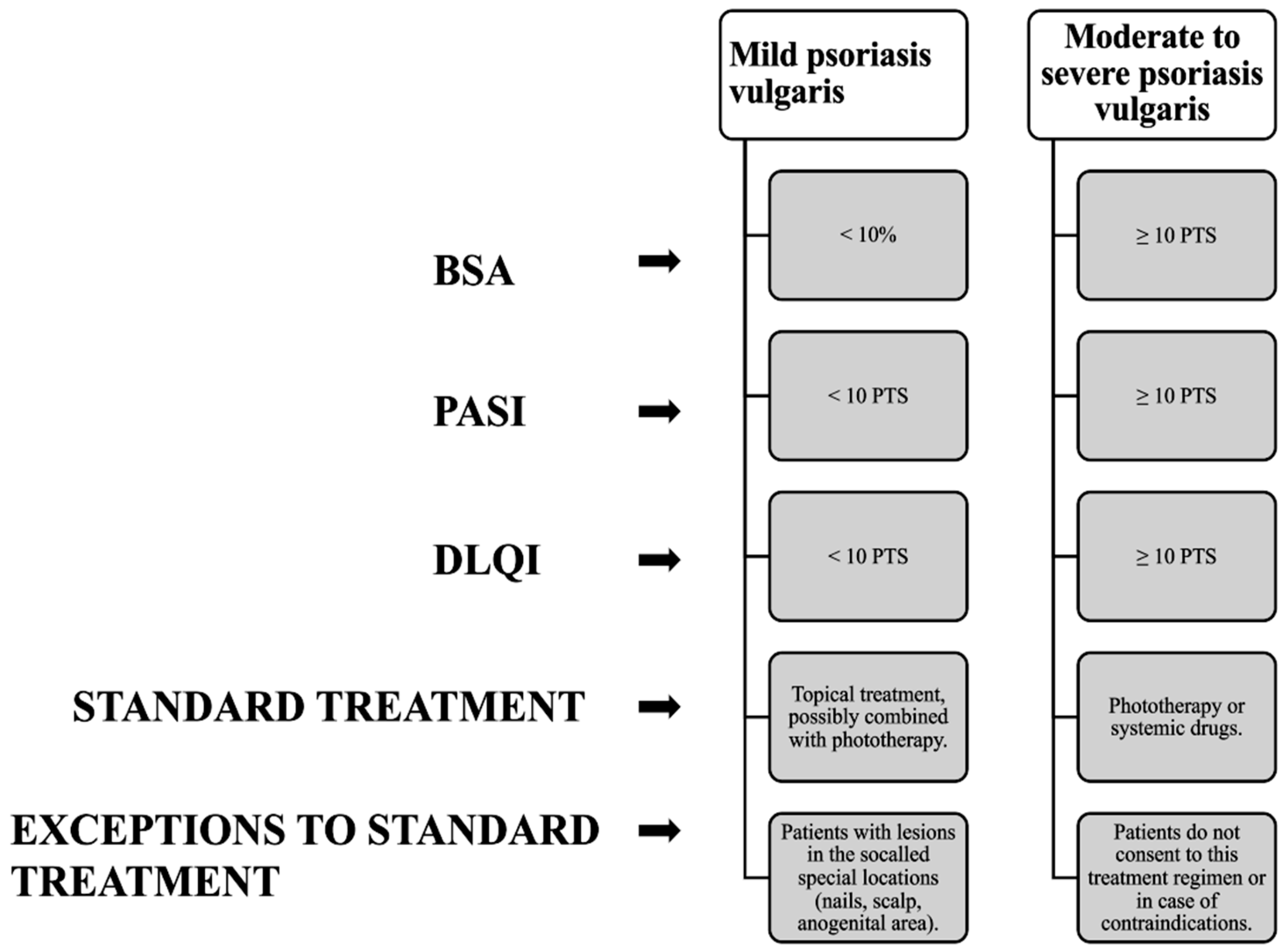
3.1. Methods for Determining the Severity of Psoriasis
3.2. Therapeutic Strategies in the Treatment of Psoriasis
3.2.1. Topical Treatment
3.2.2. Use of Phototherapy in the Treatment of Psoriasis
3.2.3. Systemic Treatment
3.3. New Therapeutic Approaches in the Treatment of Psoriasis
3.3.1. Topical Therapy
3.3.2. Biologic Drugs as a New Era of Psoriasis Treatment
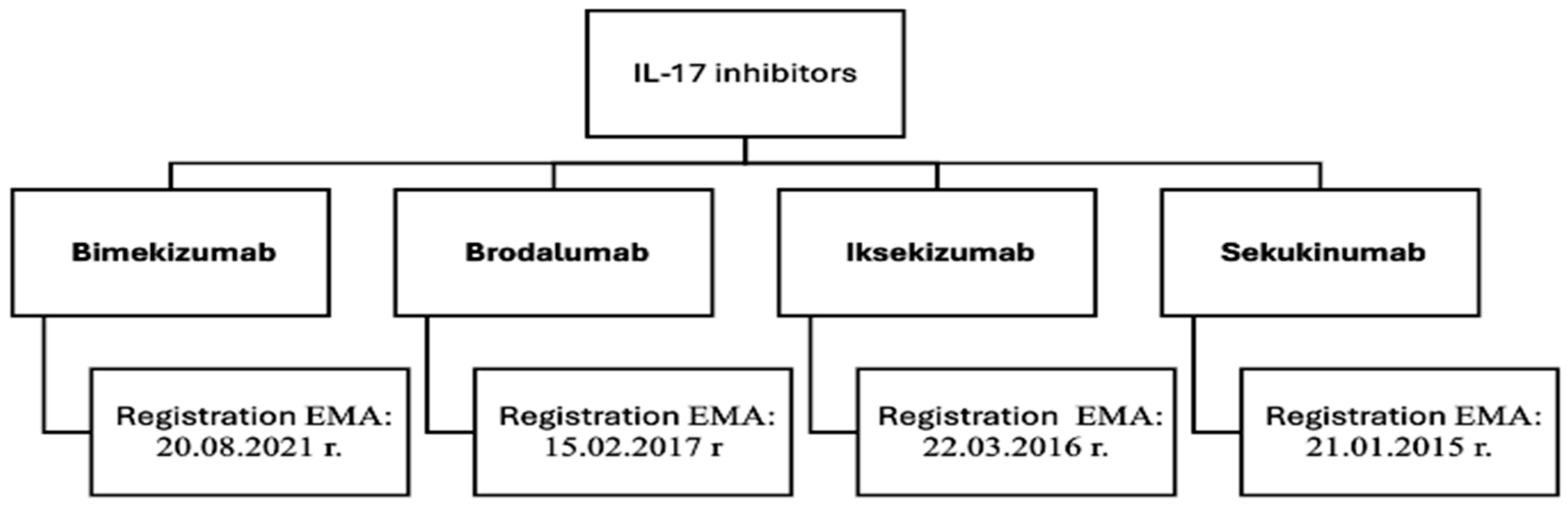
Interleukin-17 Inhibitors
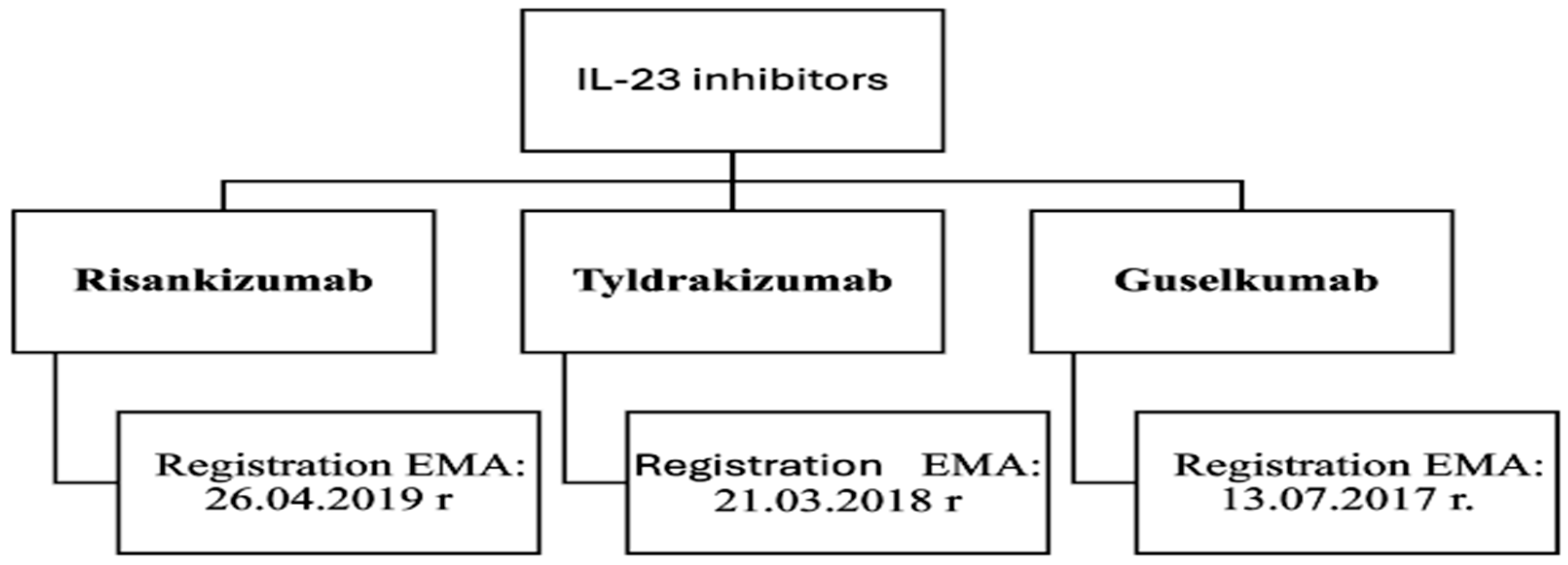
Interleukin 23 Inhibitors
4. Emollients and Their Role in the Treatment of Psoriasis
4.1. Lipid Emollients
4.2. Occlusive Emollients
4.3. Emollients “Plus”
5. Substances, Standards, Methods—New Trends in Psoriatic Skin Care
5.1. Keratolytics and Exfoliating Substances
5.2. Barrier-Restoring Substances
5.3. Modern Active Substances and Synergistic Combinations (Niacinamide, AHA + Steroids)
5.4. Cosmetological Procedures Supporting Therapy (Sonophoresis, Carboxytherapy)
6. New Approaches in the Use of Natural Raw Materials in the Treatment of Psoriasis
7. Summary and Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Nowak, A.; Popko, M.; Klimowicz, A. Preparaty pochodzenia roślinnego w pielęgnacji skóry u chorych z łuszczycą. Postep. Fitoter. 2016, 17, 332–337. [Google Scholar]
- Thaçi, D.; Augustin, M.; Krutmann, J.; Luger, T. Importance of Basic Therapy in Psoriasis. J. Dtsch. Dermatol. Ges. 2015, 13, 415–418. [Google Scholar] [CrossRef]
- Jurel, P.; Bahadur, S.; Bajpai, M. Treatment of Chronic Plaque Psoriasis: An Overview on Current Update. Pharmacol. Res. Rep. 2024, 2, 100004. [Google Scholar] [CrossRef]
- Man, A.-M.; Orăsan, M.S.; Hoteiuc, O.-A.; Olănescu-Vaida-Voevod, M.-C.; Mocan, T. Inflammation and Psoriasis: A Comprehensive Review. Int. J. Mol. Sci. 2023, 24, 16095. [Google Scholar] [CrossRef]
- Griffiths, C.E.M.; Armstrong, A.W.; Gudjonsson, J.E.; Barker, J.N.W.N. Psoriasis. Lancet 2021, 397, 1301–1315. [Google Scholar] [CrossRef] [PubMed]
- Parisi, R.; Iskandar, I.Y.K.; Kontopantelis, E.; Augustin, M.; Griffiths, C.E.M.; Ashcroft, D.M. Global Psoriasis Atlas. National, Regional, and Worldwide Epidemiology of Psoriasis: Systematic Analysis and Modelling Study. BMJ 2020, 369, m1590. [Google Scholar] [CrossRef]
- Dascălu, R.C.; Bărbulescu, A.L.; Stoica, L.E.; Dinescu, Ș.C.; Biță, C.E.; Popoviciu, H.V.; Ionescu, R.A.; Vreju, F.A. A Contemporary, Multifaced Insight into Psoriasis Pathogenesis. J. Pers. Med. 2024, 14, 535. [Google Scholar] [CrossRef] [PubMed]
- Brownstone, N. Psoriasis Therapies in 2024 and Beyond. Dermatol. Times 2024, 45, 1–34. [Google Scholar]
- Jakubowska, W.; Pisera, P.; Kiełkowicz, A.; Pactwa, F.; Popińska, Z.; Ślusarczyk, D.; Żmuda, B.; Żuberek, M. From Pathogenesis to Current Treatment of the Cutaneous Psoriasis—A Literature Review. J. Educ. Health Sport 2023, 49, 56–70. [Google Scholar] [CrossRef]
- Mrowietz, U.; Domm, S. Systemic steroids in the treatment of psoriasis: What is fact, what is fiction? J. Eur. Acad. Dermatol. Venereol. 2013, 27, 1022–1025. [Google Scholar] [CrossRef]
- Sugumaran, D.; Yong, A.C.H.; Stanslas, J. Advances in psoriasis research: From pathogenesis to therapeutics. Life Sci. 2024, 355, 122991. [Google Scholar] [CrossRef]
- Dall’Oglio, F.; Verzì, A.E.; Guglielmi, G.; Zappulla, S.; Micali, G. A New Prescription Emollient Device (PED) for Psoriasis of Sensitive Areas and Folds: A Randomized Prospective Open Trial. Psoriasis 2024, 14, 135–142. [Google Scholar] [CrossRef]
- Nowicka, D. Łuszczyca—Pielęgnacja i postępowanie w gabinecie kosmetycznym. Kosmetol. Estet. 2018, 5, 529–532. [Google Scholar]
- Narbutt, J.; Woźniacka, A.; Lesiak, A. Efficacy and tolerability of Cerkobaza and Cerkoderm 15 emollients in combination with narrow band UVB phototherapy in psoriatic patients. Forum Dermatol. 2016, 2, 68–72. [Google Scholar]
- Schreve, B.S.; Boehncke, W.H. Psoriasis. In Psoriatic Arthritis and Psoriasis; Adebajo, A., Boehncke, W.H., Gladman, D., Mease, P., Eds.; Springer: Cham, Switzerland, 2016; pp. 129–137. [Google Scholar] [CrossRef]
- Kangle, S.; Amladi, S.; Sawant, S. Scaly signs in dermatology. Indian J. Dermatol. Venereol. Leprol. 2006, 72, 161–164. [Google Scholar] [CrossRef] [PubMed]
- Rendon, A.; Schäkel, K. Psoriasis Pathogenesis and Treatment. Int. J. Mol. Sci. 2019, 20, 1475. [Google Scholar] [CrossRef]
- Romańska-Gocka, K. Farmakoterapia łuszczycy. Pol. Tow. Farm. 2009, 65, 647–654. [Google Scholar]
- Krzaczyński, J.; Strzałka-Mrozik, B. Farmakologiczne i niefarmakologiczne metody terapii łuszczycy ze szczególnym uwzględnieniem leków biologicznych. Pol. Tow. Farm. 2020, 76, 333–343. [Google Scholar]
- Kiełtyka, K.; Romańska-Kistela, A.; Rymarczyk-Kapuścik, A. Metody leczenia łuszczycy w oparciu o informacje uzyskane od pacjentów dotkniętych tą chorobą. Medsportpress 2019, 4, 185–190. [Google Scholar] [CrossRef]
- Szepietowski, J.; Adamski, Z.; Chodorowska, G.; Gliński, W.; Kaszuba, A.; Placek, W.; Rudnicka, L.; Reich, A. Leczenie łuszczycy zwyczajnej—Rekomendacje ekspertów Polskiego Towarzystwa Dermatologicznego. Część I: Łuszczyca łagodna, łuszczyca wieku dziecięcego. Prz. Dermatol. 2012, 99, 83–96. [Google Scholar]
- Bożek, A.; Reich, A. W jaki sposób miarodajnie oceniać nasilenie łuszczycy? Forum Dermatol. 2016, 2, 6–11. [Google Scholar]
- Reich, A.; Adamski, Z.; Chodorowska, G.; Kaszuba, A.; Krasowska, D.; Lesiak, A.; Maj, J.; Narbutt, J.; Osmola-Mańkowska, A.; Owczarczyk-Saczonek, A.; et al. Łuszczyca. rekomendacje diagnostyczno-terapeutyczne Polskiego towarzystwa Dermatologicznego. część I: Łuszczyca łagodna. Prz. Dermatol. 2018, 105, 225–243. [Google Scholar] [CrossRef]
- Finlay, A.Y. Current Severe Psoriasis and the Rule of Tens. Br. J. Dermatol. 2005, 152, 861–867. [Google Scholar] [CrossRef] [PubMed]
- Jacobi, A.; Mayer, A.; Augustin, M. Keratolytics and Emollients and Their Role of Psoriasis a Systematic Review. Dermatol. Ther. 2015, 5, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Kircik, L. Salicylic Acid 6% in an ammonium lactate emollient foam vehicle in the treatment of mild-to-moderate scalp psoriasis. J. Drugs Dermatol. 2011, 10, 270–273. [Google Scholar]
- Li, H.J.; Kim, M. Challenges and Future Trends in the Treatment of Psoriasis. Int. J. Mol. Sci. 2023, 24, 13313. [Google Scholar] [CrossRef]
- Elmets, C.A.; Korman, N.J.; Prater, E.F.; Wong, E.S.; Rupani, R.N.; Kivelevitch, D.; Armstrong, A.W.; Connor, C.; Cordoro, K.M.; Davis, D.M.R.; et al. Wspólne wytyczne AAD–NPF dotyczące opieki nad pacjentem i leczeniem łuszczycy za pomocą terapii miejscowej i alternatywnych metod leczenia w celu zmniejszenia nasilenia objawów łuszczycy. Am. Acad. Dermatol. 2020, 84, 432–470. [Google Scholar] [CrossRef]
- Baran, A.; Flisiak, I. Jaka Jest Klasyfikacja Miejscowych Glikokortykosteroidów ze Względu na Siłę Działania i Jakie Jest Znaczenie Praktyczne Podziału? Medycyna Praktyczna. 2018. Available online: https://www.mp.pl/pytania/pediatria/chapter/B25.QA.7.1.40 (accessed on 15 June 2025).
- Sadowska, M.; Lesiak, A.; Narbutt, J. Zastosowanie fototerapii w leczeniu łuszczycy zwyczajnej. Prz. Dermatol. 2019, 106, 198–209. [Google Scholar] [CrossRef]
- Lapolla, W.; Brad, A.; Yentzer; Bagel, J.; Halvorson, C.R.; Feldman, S.R. Przegląd metod fototerapii w leczeniu łuszczycy. Dermatol. Dyplomie 2012, 3, 8–23. [Google Scholar] [CrossRef]
- Elmets, C.A.; Lim, H.W.; Stoff, B.; Connor, C.; Cordoro, K.M.; Lebwohl, M.; Armstrong, A.W.; Davis, D.M.; Elewski, B.E.; Gelfand, J.M. Wspólne wytyczne Amerykańskiej Akademii Dermatologii i Narodowej Fundacji Łuszczycy dotyczące opieki nad leczeniem łuszczycy za pomocą fototerapii. Am. Acad. Dermatol. 2019, 81, 775–804. [Google Scholar] [CrossRef]
- Menter, A.; Strober, B.E.; Kaplan, D.H.; Kivelevitch, D.; Prater, E.F.; Stoff, B.; Armstrong, A.W.; Connor, C.; Cordoro, K.M.; Davis, D.M.; et al. Wspólne wytyczne AAD-NPF dotyczące postępowania i leczenia łuszczycy lekami biologicznymi. Am. Acad. Dermatol. 2018, 80, 1029–1072. [Google Scholar] [CrossRef] [PubMed]
- Menter, A.; Gelfand, J.M.; Connor, C.; Armstrong, A.W.; Cordoro, K.M.; Davis, D.M.; Elewski, B.E.; Gordon, K.B.; Gottlieb, A.B.; Kaplan, D.H.; et al. Wspólne wytyczne Amerykańskiej Akademii Dermatologii i Narodowej Fundacji Łuszczycy dotyczące leczenia łuszczycy za pomocą ogólnoustrojowych terapii niebiologicznych. Am. Acad. Dermatol. 2020, 82, 1445–1486. [Google Scholar] [CrossRef] [PubMed]
- Nogueira, S.; Rodrigues, M.A.; Vender, R.; Torres, T. Tapinarof w leczeniu łuszczycy. Dermatol. Ther. 2022, 35, e15931. [Google Scholar] [CrossRef]
- Konarska, I. FDA Zatwierdziła Miejscowy Tapinarof w Leczeniu Łuszczycy Plackowatej. Medscape. 2022. Available online: https://www.termedia.pl/dermatologia/FDA-zatwierdzila-miejscowy-tapinarof-w-leczeniu-luszczycy-plackowatej,47231.html (accessed on 15 June 2025).
- Megna, M.; Camela, E.; Ruggiero, A.; Battista, T.; Martora, F.; Cacciapuoti, S.; Potestio, L. Use of biological therapies for the management of pustular psoriasis: A new era? Clin. Cosmet. Investig. Dermatol. 2023, 16, 1677–1690. [Google Scholar] [CrossRef]
- Pietrzak, B.; Zwierzyńska, E.; Hytroś, E. Łuszczyca cz. 1—Obraz kliniczny, patogeneza, leczenie systemowe. Farm. Pol. 2023, 79, 91–100. [Google Scholar] [CrossRef]
- Strober, B.; Pau, C.; Blauvelt, A.; Deherder, D.; Nunez Gomez, N.; Eyerich, K. Skuteczność i bezpieczeństwo bimekizumabu u pacjentów z umiarkowaną do ciężkiej łuszczycą plackowatą: Dwuletnie wyniki pośrednie otwartego rozszerzenia randomizowanego badania fazy 3b BE RADIANT. Am. Acad. Dermatol. 2023, 89, 486–495. [Google Scholar] [CrossRef]
- Dubois Declercq, S.; Pouliot, R. Promising New Treatments for Psoriasis. Sci. World J. 2013, 2013, 980419. [Google Scholar] [CrossRef] [PubMed]
- Bimekizumab—Medicine Overview; European Medicines Agency: Amsterdam, The Netherlands. 2024. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/bimzelx (accessed on 15 June 2025).
- Adams, R.; MarooF, A.; Baker, T.; DG Lawson, A.; Oliver, R.; Paveley, R.; Rapecki, S.; Shaw, S.; Vajjah, P.; Zachód, S.; et al. Bimekizumab, a Novel Humanized IgG1 Antibody That Neutralizes Both IL-17A and IL-17F. Front. Immunol. 2020, 11, 1894. [Google Scholar] [CrossRef]
- Lesiak, A.; Ciążyńska, M. Risankizumab Jako Skuteczna i Długodziałająca Opcja Terapeutyczna w Leczeniu Łuszczycy; Wiadomości dermatologiczne; Forum Media Polska: Poznań, Poland, 2020; Available online: https://www.wiadomoscidermatologiczne.pl/artykul/risankizumab-jako-skuteczna-i-dlugodzialajaca-opcja-terapeutyczna-w-leczeniu-luszczycy (accessed on 15 June 2025).
- Ruggiero, A.; Fabbrocicni, G.; Cacciapuoti, S.; Potestio, L.; Gallo, Ł.; Megna, M. Tildrakizumab for the Treatment of Moderate-to-Severe Psoriasis: Results from 52 Weeks Real-Life Retrospective Study. Clin. Cosmet. Investig. Dermatol. 2023, 16, 529–536. [Google Scholar] [CrossRef]
- Szepietowski, J.; Kaszuba, A.; Adamski, Z.; Placek, W.; Salomon, J. Emollients in dermatological treatment: Position paper of the experts’ group. Dermatol. Klin. 2011, 13, 3–15. [Google Scholar]
- Mijaljica, D.; Spada, F.; Harrison, I.P. Topical moisturisers for the management of psoriasis vulgaris. In Psoriasis-New Research; IntechOpen: London, UK, 2022. [Google Scholar] [CrossRef]
- Almeida, C.; Madeira, A.; Marto, J.; Graça, A.; Pinto, P.; Ribeiro, H. Monfortinho Thermal Water-Based Creams: Effects on Skin Hydration, Psoriasis, and Eczema in Adults. Cosmetics 2019, 6, 56. [Google Scholar] [CrossRef]
- Torsekar, R.; Gautam, M.M. Topical Therapies in Psoriasis. Indian Dermatol. Online J. 2017, 8, 235–245. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.-Y.; Um, J.-Y.; Chung, B.-Y.; Lee, S.-Y.; Park, J.-S.; Kim, J.-C.; Park, C.-W.; Kim, H.-O. Moisturizer in Patients with Inflammatory Skin Diseases. Medicina 2022, 58, 888. [Google Scholar] [CrossRef]
- August, S.; Granier, S.; Tighe, M.P.; Tbaily, L.W.; Chowdhury, S.; Ahlbom, H. A Clinical Investigation of the Performance and Safety of Epaderm®, an Emollient Cream. Clin. Cosmet. Investig. Dermatol. 2021, 14, 909–920. [Google Scholar] [CrossRef]
- Maroto-Morales, D.; Montero-Vilchez, T.; Arias-Santiago, S. Study of Skin Barrier Function in Psoriasis: The Impact of Emollients. Life 2021, 11, 651. [Google Scholar] [CrossRef] [PubMed]
- Lodén, M. Role of topical emollients and moisturizers in the treatment of dry skin barrier disorders. Am. J. Clin. Dermatol. 2003, 4, 771–788. [Google Scholar] [CrossRef]
- Man, M.Q.; Ye, L.; Hu, L.; Jeong, S.; Elias, P.M.; Lv, C. Improvements in epidermal function prevent relapse of psoriasis: A self-controlled study. Clin. Exp. Dermatol. 2019, 44, 654–657. [Google Scholar] [CrossRef]
- Li, X.; Yang, Q.; Zheng, J.; Gu, H.; Chen, K.; Jin, H.; He, C.; Xu, A.E.; Xu, J.; Zhang, J.; et al. Efficacy and safety of a topical moisturizer containing linoleic acid and ceramide for mild-to-moderate psoriasis vulgaris: A multicenter randomized controlled trial. Dermatol. Ther. 2020, 33, e14263. [Google Scholar] [CrossRef]
- Kowalska, M.K.; Orłowska, S.M.; Bednarczyk, Ł. Applied Research on Atopic Dermatitis with Special Emphasis on the Role of Emollients in This Disorder: A Review. Appl. Sci. 2024, 14, 8315. [Google Scholar] [CrossRef]
- Gorski, J.; Proksch, E.; Baron, J.M.; Schmid, D.; Zhang, L. Dexpanthenol in Wound Healing after Medical and Cosmetic Interventions (Postprocedure Wound Healing). Pharmaceuticals 2020, 13, 138. [Google Scholar] [CrossRef]
- Marquardt, Y.; Amann, P.M.; Heise, R.; Czaja, K.; Steiner, T.; Merk, H.F.; Skazik-Voogt, C.; Baron, J.M. Characterization of a novel standardized human three-dimensional skin wound healing model using non-sequential fractional ultrapulsed CO2 laser treatments. Lasers Surg. Med. 2015, 47, 257–265. [Google Scholar] [CrossRef]
- Thouvenin, M.D.; Dalmon, S.; Theunis, J.; Lauze, C.; Coubetergues, H.; Mengeaud, V.; Calvet, B. Tolerance and efficacy of a new celastrol-containing balm as adjunct care in psoriasis. J. Eur. Acad. Dermatol. Venereol. 2020, 34 (Suppl. S6), 10–16. [Google Scholar] [CrossRef]
- Uchida, Y.; Park, K. Ceramides in Skin Health and Disease: An Update. Am. J. Clin. Dermatol. 2021, 22, 853–866. [Google Scholar] [CrossRef]
- Zwierzyńska, E.; Hytroś, E.; Pietrzak, B. Łuszczyca cz. 2—Leczenie miejscowe, fototerapia oraz pielęgnacja skóry. Farm. Pol. 2023, 79, 473–481. [Google Scholar] [CrossRef] [PubMed]
- Ramic, L.; Sator, P. Topical Treatment of Psoriasis Vulgaris. J. Dtsch. Dermatol. Ges. 2023, 21, 631–642. [Google Scholar] [CrossRef]
- Matwiejuk, M.; Mysliwiec, H.; Chabowski, A.; Flisiak, I. The Role of Sphingolipids in the Pathogenesis of Psoriasis. Metabolites 2020, 12, 1171. [Google Scholar] [CrossRef] [PubMed]
- Kozłowska, D.; Harasim-Symbor, E.; Myśliwiec, H.; Milewska, A.J.; Chabowski, A.; Flisiak, I. Serum sphingolipid level in psoriatic patients with obesity. Postep. Dermatol. Alergol. 2019, 36, 714–721. [Google Scholar] [CrossRef] [PubMed]
- Araviiskaia, E.; Pincelli, C.; Sparavigna, A.; Luger, T. The Role of a Novel Generation of Emollients, ‘Emollients Plus’, in Atopic Dermatitis. Clin. Cosmet. Investig. Dermatol. 2022, 15, 2705–2719. [Google Scholar] [CrossRef]
- Proksch, E.; de Bony, R.; Trapp, S.; Boudon, S. Topical use of dexpanthenol: A 70th anniversary article. J. Dermatol. Treat. 2017, 28, 766–773. [Google Scholar] [CrossRef]
- Augustin, M.; Berardesca, E.; Blume-Peytavi, U.; Elsner, P.; Scafa, D.; Schmeel, L.C.; Proksch, E. Managing dry skin in patients with comorbidities or with advanced age: Unmet needs and roles for products containing potential emollient-plus ingredients. J. Dermatol. Treat. 2024, 35, 2326171. [Google Scholar] [CrossRef]
- Blauvelt, A.; Chiricozzi, A. The Immunologic Role of IL-17 in Psoriasis and Psoriatic Arthritis Pathogenesis. Clin. Rev. Allergy Immunol. 2018, 55, 379–390. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Zhang, J.; Yu, J.; Chen, X.; Zhang, F.; Wei, W.; Zhang, L.; Chen, W.; Lin, N.; Wu, Y. Hyperforin Ameliorates Imiquimod-Induced Psoriasis-Like Murine Skin Inflammation by Modulating IL-17A-Producing γδ T Cells. Front. Immunol. 2021, 12, 635076. [Google Scholar] [CrossRef]
- Wielowieyska-Szybińska, D.; Wojas-Pelc, A. Przebieg i postępowanie w łuszczycy zwykłej. In Przebieg i Postępowanie w Łuszczycy Zwykłej; Katedra i Klinika Dermatologii Collegium Medicum Uniwersytetu Jagiellońskiego: Kraków, Poland, 2012. [Google Scholar]
- Naldi, L.; Rzany, B. Psoriasis (Chronic Plaque). Clin. Evid. 2009, 2009, 1706. [Google Scholar]
- Kostarelos, K.; Teknetzis, A.; Lefaki, I.; Ioannides, D.; Minas, A. Double-Blind Clinical Study Reveals Synergistic Action Between Alpha-Hydroxy Acid and Betamethasone Lotions Towards Topical Treatment of Scalp Psoriasis. J. Eur. Acad. Dermatol. Venereol. 2000, 14, 5–9. [Google Scholar] [CrossRef]
- Mari, N.L.; Simão, A.N.C.; Dichi, I. n-3 Polyunsaturated Fatty Acids Supplementation in Psoriasis: A Review. Nutrire 2017, 42, 5. [Google Scholar] [CrossRef]
- Fluhr, J.W.; Cavallotti, C.; Berardesca, E. Emollients, Moisturizers and Keratolytic Agents in Psoriasis. Clin. Dermatol. 2008, 26, 380–386. [Google Scholar] [CrossRef] [PubMed]
- Piquero-Casals, J.; Morgado-Carrasco, D.; Granger, C.; Trullàs, C.; Jesús-Silva, A.; Krutmann, J. Urea in Dermatology: A Review of its Emollient, Moisturizing, Keratolytic, Skin Barrier Enhancing and Antimicrobial Properties. Dermatol. Ther. 2021, 11, 1905–1915. [Google Scholar] [CrossRef]
- Levine, D.; Even-Chen, Z.; Lipets, I.; Pritulo, O.A.; Svyatenko, T.V.; Andrashko, Y.; Lebwohl, M.; Gottlieb, A. Pilot, Multicenter, Double-Blind, Randomized Placebo-Controlled Bilateral Comparative Study of a Combination of Calcipotriene and Nicotinamide for the Treatment of Psoriasis. J. Am. Acad. Dermatol. 2010, 63, 775–781. [Google Scholar] [CrossRef]
- Majchrzycka, M.; Adamska, K.; Rachwalska, K.; Adamski, Z. The Role of the Adjuvant Aesthetic Therapy in the Lives of Patients with Psoriatic Disease. Adv. Dermatol. Allergol. 2022, 39, 1106–1109. [Google Scholar] [CrossRef]
- Michalska, A.D. Łuszczyca—Etiopatogeneza i Leczenie. In Problemy Nauk Medycznych i Nauk o Zdrowiu; Tom 11; Pujer, K., Ed.; Exante Wydawnictwo Naukowe: Wrocław, Poland, 2020; pp. 44–53. [Google Scholar]
- Ghaseminejad-Bandpey, A.; Etemadmoghadam, S.; Jabbari, B. Botulinum Toxin Treatment of Psoriasis—A Comprehensive Review. Toxins 2024, 16, 449. [Google Scholar] [CrossRef]
- Juntongjin, P.; Srisinlapakig, S.; Nitayavardhana, S. Botulinum Toxin Injection Shows Promise in Nail Psoriasis: A Comparative Randomized Controlled Trial. JAAD Int. 2024, 16, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Le, S.; Wu, X.; Dou, Y.; Song, T.; Fu, H.; Luo, H.; Zhang, F.; Cao, Y. Promising strategies in natural products treatments of psoriasis-update. Front. Med. 2024, 11, 1386783. [Google Scholar] [CrossRef]
- Neema, S.; Sandhu, S.; Gupta, A.; Jagadeesan, S.; Vasudevan, B. Unconventional treatment options in psoriasis: A review. Indian J. Dermatol. Venereol. Leprol. 2022, 88, 137–143. [Google Scholar] [CrossRef]
- Elkhawaga, O.Y.; Ellety, M.M.; Mofty, S.O.; Ghanem, M.S.; Mohamed, A.O. Review of natural compounds for potential psoriasis treatment. Inflammopharmacology 2023, 31, 1183–1198. [Google Scholar] [CrossRef]
- Dhanabal, S.P.; Priyanka Dwarampudi, L.; Muruganantham, N.; Vadivelan, R. Evaluation of the antipsoriatic activity of Aloe vera leaf extract using a mouse tail model of psoriasis. Phytother. Res. 2012, 26, 617–619. [Google Scholar] [CrossRef]
- Gendrisch, F.; Haarhaus, B.; Krieger, N.; Quirin, K.W.; Schempp, C.M.; Wölfle, U. The Effect of Herbal Medicinal Products on Psoriasis-Like Keratinocytes. Biomolecules 2021, 11, 371. [Google Scholar] [CrossRef]
- Kolahdooz, S.; Karimi, M.; Esmaili, N.; Zargaran, A.; Kordafshari, G.; Mozafari, N.; Ayati, M.H. Evaluation of the efficacy of a topical chamomile-pumpkin oleogel for the treatment of plaque psoriasis: An intra-patient, double-blind, randomized clinical trial. Biomed. Res. Ther. 2018, 5, 2811–2819. [Google Scholar] [CrossRef]
- Asadi, Z.; Ghazanfari, T.; Hatami, H. Anti-inflammatory Effects of Matricaria chamomilla Extracts on BALB/c Mice Macrophages and Lymphocytes. Iran. J. Allergy Asthma Immunol. 2020, 19, 63–73. [Google Scholar] [CrossRef] [PubMed]
- Lairikyengbam, D.; Wetterauer, B.; Schmiech, M.; Jahraus, B.; Kirchgessner, H.; Wetterauer, P.; Berschneider, K.; Beier, V.; Niesler, B.; Balta, E.; et al. Comparative analysis of whole plant, flower and root extracts of Chamomilla recutita L. and characteristic pure compounds reveals differential anti-inflammatory effects on human T cells. Front. Immunol. 2024, 15, 1388962. [Google Scholar] [CrossRef]
- Szeleszczuk, Ł.; Zielińska-Pisklak, M. Matricaria chamomilla—Why is it worth to keep it in home first aid kit? Med. Pol. 2013, 23, 72–79. [Google Scholar]
- Chen, G.; Lv, C.; Nie, Q.; Li, X.; Lv, Y.; Liao, G.; Liu, S.; Ge, W.; Chen, J.; Du, Y. Essential Oil of Matricaria chamomilla Alleviate Psoriatic-Like Skin Inflammation by Inhibiting PI3K/Akt/mTOR and p38MAPK Signaling Pathway. Clin. Cosmet. Investig. Dermatol. 2024, 17, 59–77. [Google Scholar] [CrossRef] [PubMed]
- Martins, M.D.; Marques, M.M.; Bussadori, S.K.; Martins, M.A.; Pavesi, V.C.; Mesquita-Ferrari, R.A.; Fernandes, K.P. Comparative analysis between Chamomilla recutita and corticosteroids on wound healing. An in vitro and in vivo study. Phytother. Res. 2009, 23, 274–278. [Google Scholar] [CrossRef] [PubMed]
- Seyedjavadi, S.S.; Khani, S.; Eslamifar, A.; Ajdary, S.; Goudarzi, M.; Halabian, R.; Akbari, R.; Zare-Zardini, H.; Imani Fooladi, A.A.; Amani, J.; et al. The Antifungal Peptide MCh-AMP1 Derived From Matricaria chamomilla Inhibits Candida albicans Growth via Inducing ROS Generation and Altering Fungal Cell Membrane Permeability. Front. Microbiol. 2020, 10, 3150. [Google Scholar] [CrossRef] [PubMed]
- Stanojevic, L.P.; Marjanovic-Balaban, Z.R.; Kalaba, V.D.; Stanojevic, J.S.; Cvetkovic, D.J. Chemical Composition, Antioxidant and Antimicrobial Activity of Chamomile Flowers Essential Oil (Matricaria chamomilla L.). J. Essent. Oil Bear. Plants 2016, 19, 2017–2028. [Google Scholar] [CrossRef]
- Alesci, A.; Lauriano, E.R.; Fumia, A.; Irrera, N.; Mastrantonio, E.; Vaccaro, M.; Gangemi, S.; Santini, A.; Cicero, N.; Pergolizzi, S. Relationship between Immune Cells, Depression, Stress, and Psoriasis: Could the Use of Natural Products Be Helpful? Molecules 2022, 27, 1953. [Google Scholar] [CrossRef]
- Niculet, E.; Radaschin, D.S.; Nastase, F.; Draganescu, M.; Baroiu, L.; Miulescu, M.; Arbune, M.; Tatu, A.L. Influence of phytochemicals in induced psoriasis (Review). Exp. Ther. Med. 2020, 20, 3421–3424. [Google Scholar] [CrossRef]
- Kaur, S.; Bains, K. Aloe Barbadensis Miller (Aloe Vera). Int. J. Vitam. Nutr. Res. 2024, 94, 308–321. [Google Scholar] [CrossRef]
- Hamman, J.H. Composition and applications of Aloe vera leaf gel. Molecules 2008, 13, 1599–1616. [Google Scholar] [CrossRef]
- Adlakha, K.; Koul, B.; Kumar, A. Value-added products of Aloe species: Panacea to several maladies. S. Afr. J. Bot. 2022, 147, 1124–1135. [Google Scholar] [CrossRef]
- Hekmatpou, D.; Mehrabi, F.; Rahzani, K.; Aminiyan, A. The Effect of Aloe Vera Clinical Trials on Prevention and Healing of Skin Wound: A Systematic Review. Iran. J. Med. Sci. 2019, 44, 1–9. [Google Scholar]
- Catalano, A.; Ceramella, J.; Iacopetta, D.; Marra, M.; Conforti, F.; Lupi, F.R.; Gabriele, D.; Borges, F.; Sinicropi, M.S. Aloe vera-An Extensive Review Focused on Recent Studies. Foods 2024, 13, 2155. [Google Scholar] [CrossRef] [PubMed]
- Syed, T.A.; Ahmad, S.A.; Holt, A.H.; Ahmad, S.A.; Ahmad, S.H.; Afzal, M. Management of psoriasis with Aloe vera extract in a hydrophilic cream: A placebo-controlled, double-blind study. Trop. Med. Int. Health 1996, 1, 505–509. [Google Scholar] [CrossRef]
- Sánchez, M.; González-Burgos, E.; Iglesias, I.; Gómez-Serranillos, M.P. Pharmacological Update Properties of Aloe vera and its Major Active Constituents. Molecules 2020, 25, 1324. [Google Scholar] [CrossRef]
- Meza-Valle, K.Z.; Saucedo-Acuña, R.A.; Tovar-Carrillo, K.L.; Cuevas-González, J.C.; Zaragoza-Contreras, E.A.; Melgoza-Lozano, J. Characterization and Topical Study of Aloe Vera Hydrogel on Wound-Healing Process. Polymers 2021, 13, 3958. [Google Scholar] [CrossRef] [PubMed]
- Wahedi, H.M.; Jeong, M.; Chae, J.K.; Do, S.G.; Yoon, H.; Kim, S.Y. Aloesin from Aloe vera accelerates skin wound healing by modulating MAPK/Rho and Smad signaling pathways in vitro and in vivo. Phytomed. Int. J. Phytother. Phytopharm. 2017, 28, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Hormozi, M.; Assaei, R.; Boroujeni, M.B. The effect of aloe vera on the expression of wound healing factors (TGFβ1 and bFGF) in mouse embryonic fibroblast cell: In vitro study. Biomed. Pharmacother. Biomed. Pharmacother. 2017, 88, 610–616. [Google Scholar] [CrossRef]
- Jales, S.T.L.; Barbosa, R.M.; de Albuquerque, A.C.; Duarte, L.H.V.; da Silva, G.R.; Meirelles, L.M.A.; da Silva, T.M.S.; Alves, A.F.; Viseras, C.; Raffin, F.N.; et al. Development and characterization of aloe vera mucus-based hydrogels for the treatment of psoriasis. J. Compos. Sci. 2022, 6, 231. [Google Scholar] [CrossRef]
- Leng, H.; Pu, L.; Xu, L.; Shi, X.; Ji, J.; Chen, K. Effects of aloe polysaccharide, a polysaccharide extracted from Aloe vera, on TNF-α-induced HaCaT cell proliferation and the underlying mechanism in psoriasis. Mol. Med. Rep. 2018, 18, 3537–3543. [Google Scholar] [CrossRef]
- Dwarampudi, L.P.; Palaniswamy, D.; Nithyanantham, M.; Raghu, P.S. Antipsoriatic activity and cytotoxicity of ethanolic extract of Nigella sativa seeds. Pharmacogn. Mag. 2012, 8, 268–272. [Google Scholar] [CrossRef]
- Sallehuddin, N.; Nordin, A.; Bt Hj Idrus, R.; Fauzi, M.B. Nigella sativa and Its Active Compound, Thymoquinone, Accelerate Wound Healing in an In Vivo Animal Model: A Comprehensive Review. Int. J. Environ. Res. Public Health 2020, 17, 4160. [Google Scholar] [CrossRef]
- Ashraf, M.; El-Sawy, H.S.; El Zaafarany, G.M.; Abdel-Mottaleb, M.M.A. Can Essential Oils/Botanicals Smart-Nanoformulations Be Winning Cards in the Fight Against Psoriasis? Pharmaceutics 2023, 15, 750. [Google Scholar] [CrossRef] [PubMed]
- Kmail, A.; Said, O.; Saad, B. How Thymoquinone from Nigella sativa Accelerates Wound Healing through Multiple Mechanisms and Targets. Curr. Issues Mol. Biol. 2023, 45, 9039–9059. [Google Scholar] [CrossRef]
- Malik, S.; Singh, A.; Negi, P.; Kapoor, V.K. Thymoquinone: A small molecule from nature with high therapeutic potential. Drug Discov. Today 2021, 26, 2716–2725. [Google Scholar] [CrossRef]
- Nasiri, N.; Ilaghi Nezhad, M.; Sharififar, F.; Khazaneha, M.; Najafzadeh, M.J.; Mohamadi, N. The Therapeutic Effects of Nigella sativa on Skin Disease: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Evid. Based Complement. Altern. Med. 2022, 2022, 7993579. [Google Scholar] [CrossRef]
- Negi, P.; Sharma, I.; Hemrajani, C.; Rathore, C.; Bisht, A.; Raza, K.; Katare, O.P. Thymoquinone-loaded lipid vesicles: A promising nanomedicine for psoriasis. BMC Complement. Altern. Med. 2019, 19, 334. [Google Scholar] [CrossRef] [PubMed]
- Farasati Far, B.; Gouranmohit, G.; Naimi-Jamal, M.R.; Neysani, E.; El-Nashar, H.A.S.; El-Shazly, M.; Khoshnevisan, K. The potential role of Hypericum perforatum in wound healing: A literature review on the phytochemicals, pharmacological approaches, and mechanistic perspectives. Phytother. Res. 2024, 38, 3271–3295. [Google Scholar] [CrossRef] [PubMed]
- Singh, N.; Yadav, S.D.; Gupta, P.; Ali, F.; Arora, S. Dermal Delivery of Hypericum perforatum (L.) Loaded Nanogel: Formulation to Preclinical Psoriasis Assessment. Recent Adv. Drug Deliv. Formul. 2024, 18, 138–154. [Google Scholar] [CrossRef]
- Mansouri, P.; Mirafzal, S.; Najafizadeh, P.; Safaei-Naraghi, Z.; Salehi-Surmaghi, M.H.; Hashemian, F. The impact of topical Saint John’s Wort (Hypericum perforatum) treatment on tissue tumor necrosis factor-alpha levels in plaque-type psoriasis: A pilot study. J. Postgrad. Med. 2017, 63, 215–220. [Google Scholar] [CrossRef]
- Kang, D.; Li, B.; Luo, L.; Jiang, W.; Lu, Q.; Rong, M.; Lai, R. Curcumin shows excellent therapeutic effect on psoriasis in mouse model. Biochimie 2016, 123, 73–80. [Google Scholar] [CrossRef]
- Antiga, E.; Bonciolini, V.; Volpi, W.; Del Bianco, E.; Caproni, M. Oral Curcumin (Meriva) Is Effective as an Adjuvant Treatment and Is Able to Reduce IL-22 Serum Levels in Patients with Psoriasis Vulgaris. BioMed Res. Int. 2015, 2015, 283634. [Google Scholar] [CrossRef]
- Zhang, S.; Wang, J.; Liu, L.; Sun, X.; Zhou, Y.; Chen, S.; Lu, Y.; Cai, X.; Hu, M.; Yan, G.; et al. Efficacy and safety of curcumin in psoriasis: Preclinical and clinical evidence and possible mechanisms. Front. Pharmacol. 2022, 13, 903160. [Google Scholar] [CrossRef]
- Janeczek, M.; Moy, L.; Lake, E.P.; Swan, J. Review of the Efficacy and Safety of Topical Mahonia aquifolium for the Treatment of Psoriasis and Atopic Dermatitis. J. Clin. Aesthetic Dermatol. 2018, 11, 42–47. [Google Scholar]
- Hurkul Muhammed, M.; Sarialtin, S.Y.; Koroglu, A.; Coban, T. Potencial inhibidor in vitro de frutos de aguacate, Persea americana (Lauraceae) contra la oxidacion, inflamacion y enzimas clave vinculadas a enfermedades de la piel. Rev. Biol. Trop. 2021, 69, 472–482. [Google Scholar]
- de Oliveira, A.P.; Franco, E.S.; Rodrigues Barreto, R.; Cordeiro, D.P.; de Melo, R.G.; de Aquino, C.M.; Silva, A.A.r.E.; de Medeiros, P.L.; da Silva, T.G.; Góes, A.J.D.S.; et al. Effect of semisolid formulation of Persea americana mill (avocado) oil on wound healing in rats. Evid. Based Complement. Altern. Med. 2013, 2013, 472382. [Google Scholar] [CrossRef] [PubMed]
- Stücker, M.; Memmel, U.; Hoffmann, M.; Hartung, J.; Altmeyer, P. Vitamin B(12) cream containing avocado oil in the therapy of plaque psoriasis. Dermatology 2001, 203, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Ashwani, T. Natural Compounds Used in the Treatment and Management of Psoriasis: A Review. Int. J. Pharmacogn. 2023, 10, 489–510. [Google Scholar]
- Michalsen, A.; Eddin, O.; Salama, A. A case series of the effects of a novel composition of a traditional natural preparation for the treatment of psoriasis. J. Tradit. Complement. Med. 2016, 6, 395–398. [Google Scholar] [CrossRef]
- Basharat, S.; Gilani, S.A.; Iftikhar, F.; Murtaza, M.A.; Basharat, A.; Sattar, A.; Qamar, M.M.; Ali, M. Capsaicin: Plants of the Genus Capsicum and Positive Effect of Oriental Spice on Skin Health. Ski. Pharmacol. Physiol. 2020, 33, 331–341. [Google Scholar] [CrossRef]
- Chan, T.C.; Lee, M.S.; Huang, W.C.; Chang, W.Y.; Krueger, J.G.; Tsai, T.F. Capsaicin attenuates imiquimod-induced epidermal hyperplasia and cutaneous inflammation in a murine model of psoriasis. Biomed. Pharmacother. Biomed. Pharmacother. 2021, 141, 111950. [Google Scholar] [CrossRef]
- Gupta, R.; Gupta, M.; Mangal, S.; Agrawal, U.; Vyas, S.P. Capsaicin-loaded vesicular systems designed for enhancing localized delivery for psoriasis therapy. Artif. Cells Nanomed. Biotechnol. 2016, 44, 825–834. [Google Scholar] [CrossRef]
- Anzar, C.A.; Joseph, M.V.; Vadiraj, G.; Shariq Afsar Thandu, B.; Anjaneya Reddy Lebaka, P. In vitro anti-inflammatory and skin protective properties of Virgin coconut oil. J. Tradit. Complement. Med. 2019, 9, 5–14. [Google Scholar]
- Chadha, H.; Chandra, P.; Meher, B.; Sachan, N. Molecular Docking Analysis of Psoriasis Specific Mediator IL-17 with Active Phytoconstituents from Cocos nucifera, Carica papaya, Ichnocarpus frutescens. Lett. Appl. NanoBioScience 2024, 14, 18. [Google Scholar] [CrossRef]
- Cardia, G.F.E.; Silva-Filho, S.E.; Silva, E.L.; Uchida, N.S.; Cavalcante, H.A.O.; Cassarotti, L.L.; Salvadego, V.E.C.; Spironello, R.A.; Bersani-Amado, C.A.; Cuman, R.K.N. Effect of Lavender (Lavandula angustifolia) Essential Oil on Acute Inflammatory Response. Evid. Based Complement. Altern. Med. 2018, 2018, 1413940. [Google Scholar] [CrossRef]
- Rai, V.K.; Sinha, P.; Yadav, K.S.; Shukla, A.; Saxena, A.; Bawankule, D.U.; Tandon, S.; Khan, F.; Chanotiya, C.S.; Yadav, N.P. Anti-psoriatic effect of Lavandula angustifolia essential oil and its major components linalool and linalyl acetate. J. Ethnopharmacol. 2020, 261, 113127. [Google Scholar] [CrossRef]
- Moreira, P.; Sousa, F.J.; Matos, P.; Brites, G.S.; Gonçalves, M.J.; Cavaleiro, C.; Figueirinha, A.; Salgueiro, L.; Batista, M.T.; Branco, P.C.; et al. Chemical Composition and Effect against Skin Alterations of Bioactive Extracts Obtained by the Hydrodistillation of Eucalyptus globulus Leaves. Pharmaceutics 2022, 14, 561. [Google Scholar] [CrossRef] [PubMed]
- Ashraf, M.; El-Sawy, H.S.; El Zaafarany, G.M.; Abdel-Mottaleb, M.M.A. Eucalyptus oil nanoemulsion for enhanced skin deposition of fluticasone propionate in psoriatic plaques: A combinatorial anti-inflammatory effect to suppress implicated cytokines. Arch. Pharm. 2025, 358, e2400557. [Google Scholar] [CrossRef]
- Lee, J.H.; Lee, M.-Y. Aktywność przeciwłuszczycowa ekstraktów z owoców Ficus carica in vitro i in vivo poprzez modulację JAK-STAT. Life 2023, 13, 1671. [Google Scholar] [CrossRef]
- Zhang, L.; Ma, X.; Shi, R.; Zhang, L.; Zhao, R.; Duan, R.; Qin, Y.; Gao, S.; Li, X.; Duan, J.; et al. Allicin ameliorates imiquimod-induced psoriasis-like skin inflammation via disturbing the interaction of keratinocytes with IL-17A. Br. J. Pharmacol. 2023, 180, 628–646. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Symptom Name | Characteristics of the Symptom |
|---|---|
| Stearin candle symptom | The symptom appears when scratching the scales fall off forming thin flakes (which resembles scraping from a candle) making the shiny surface of the psoriatic papules visible |
| Auspitz symptom | Characteristic phenomenon of fine droplet bleeding observed after scratching the papules and removing the scale |
| Koebner phenomenon | After scratching the lesion after about 7–12 days, seeding of primary lesions appears along the lesion line. Characteristics of the active phase of the disease. |
| Clinical Form of Psoriasis | Characteristics of Changes |
|---|---|
| Plaque psoriasis | in the course of plaque psoriasis, erythematous scaly plaques of various sizes are observed, located mainly on the scalp, elbows, knees and lumbosacral region. |
| Pustular psoriasis | present on the skin are small sterile pustules, which are formed by the accumulation of multinucleated leukocytes. Various forms of pustular psoriasis are distinguished depending on the localization of the skin lesions, including a form limited to the hands and feet, a limited diffuse form and a generalized form (von zumbusch generalized pustular psoriasis). |
| Psoriatic arthritis | in 25% of patients with psoriatic arthritis, joint lesions appear after the onset of skin lesions. is a seronegative inflammation (no rheumatoid factor in the blood serum) various forms of psoriatic arthritis, symmetric polyarthritis, among others |
| Nail psoriasis | thimble nails—small, limited depressions on the surface of the nail about 1 mm in diameter subungual psoriatic papules shining through the plate (oil drop sign) onycholysis (separation of the free edge of the nail from the matrix, co-occurs with hyperkeratosis) |
| Erythrodermic psoriasis | psoriatic lesions cover most of the skin surface >90% confluent, exfoliative dermatitis with increased exfoliation pruritus of varying severity and elevated body temperature |
| Inverted (flexural) psoriasis | interdigital localization erosive erythematous plaques and spots |
| Local Treatment | Phototherapy and Photochemotherapy | Systemic Treatment | Supportive Methods |
|---|---|---|---|
|
|
|
|
| SCALE | PASI | BSA | DLQI |
|---|---|---|---|
| Parameter Evaluated | Extent Severity | Body surface area occupied by lesions | Quality of life—the impact of the disease on the patient’s life |
| Point | Each parameter evaluated separately. The score is the sum of the evaluation points of both parameters. Extent-evaluated is the affected area: head, trunk, upper and lower extremities on a scale of 0 (<10%) to 6 (90–100%). Severity-The following is evaluated: thickness of lesions, erythema, scale build-up, on a scale of 0 (no lesions) to 4 points (very severe lesions). | Calculation using the, “rule of nines”. Occupation of each of the following locations means obtaining 9% (head and neck, right upper limb, left upper limb, chest, abdomen, upper back, lower back, right thigh, left thigh, right shank, left shank) Occupation of the perineal area = obtaining 1% | The patient answers 10 questions. Each question can be scored from 0 to 3 points. The score is the sum of points. 0–1 pts—no impact of the disease on quality of life, 2–5 pts—slightly reduced quality of life, 6–10 pts—moderately reduced quality of life, 11–20 pts—severely reduced quality of life, 21–30 pts—very severely reduced quality of life |
| Max. score | 72 PTS | 100% | 30 PTS |
| Mini. score | 0 PTS | 0% | 0 PTS |
| Emollients | Substance | Effects |
|---|---|---|
| Basic emollients | Vaseline, paraffin | They maintain the integrity of the skin barrier, resulting in a reduction in transepidermal water loss. |
| Lipid emollients | Linoleic acid, ceramides | They form a tight lipid barrier, thereby reducing transepidermal water loss and preventing the penetration of pathogenic microorganisms into deeper layers of the skin. |
| Occlusive emollients | Beeswax, lanolin, and mineral oils | Form an occlusive layer that reduces transepidermal water loss. Additionally, they create a protective barrier that shields the skin from irritating factors. |
| Emollients “plus” | Enriched emollient: celastrol polidocanol dexpanthenol | They exhibit additional immunomodulatory, antipruritic, moisturizing, anti-inflammatory, emollient, and reepithelialization-accelerating effects |
| Natural Substance | Its Mechanism of Action | Its Confirmed Anti-Psoriatic Effect |
|---|---|---|
| Common Mahonia Mahonia aquifolium | Mahonia has an adjunctive effect on the treatment of psoriatic skin, showing anti-inflammatory and antiproliferative effects. Berberine, the main alkaloid found in the plant, is involved in both mechanisms of action [120]. Upon application of M. common extract, 5-lipoxygenase and lipid peroxidation in liposomes are inhibited, preventing the release of inflammatory mediators. Regarding the antiproliferative effect, berberine inhibits cell growth by penetrating DNA, resulting in disruption of DNA replication and keratinocyte proliferation [120]. | Janeczek et al. in 2018 reviewed studies of Mahonia common’s effects on psoriasis. The first human study conducted in Germany in 1995 confirmed the efficacy of Mahonia common [120]. The study included 433 patients diagnosed with plaque psoriasis. After 12 weeks of treatment with a 10% ointment containing M. vulgaris, improvements were noted in 81% of patients. Improvement was assessed by dermatologists using the PASI. Subsequent authors [120] in the following years confirmed the aforementioned conclusions indicating the therapeutic effect of Mahonia common in the treatment of psoriasis. |
| Avocado Persea americana | Methanolic extracts of avocado seeds have shown efficacy in eliminating free radicals and inhibiting lipid peroxidation in liposomes [121]. Avocado oil accelerates wound healing by increasing collagen synthesis and reducing inflammation [122]. | The purpose of a study conducted by Stücker et al. in 2001 was to evaluate the efficacy of an ointment containing avocado oil compared to calcipotriol in the treatment of psoriasis. The 13 patients used an ointment with avocado oil and vitamin B12 on one hand and a vitamin D3 analog (calcipotriol) on the other hand for 12 weeks. After 12 weeks of treatment, the psoriatic lesions on both hands went into remission after the above-mentioned ointments were applied. Both ointments demonstrated treatment efficacy. The effects of the treatment were evaluated using 20 MHz sonography. The results, which were reported using the PASI, showed no differences between the two treatments [123]. |
| Tea tree Melaleuca alternifolia | Tea tree oil (TTO) is rich in terpenes. One of the main substances is terpinen-4-ol, which is responsible for its anti-inflammatory effect in the treatment of psoriasis [124]. TTO reduces TNF, IL-1 and IL-8 which is due to a decrease in the production and infiltration of CD4+ T lymphocytes [109]. | A study conducted by Michalsen et al. (2016) involved 12 patients with moderate to severe psoriasis. The patients used an ointment containing natural ingredients such as nigella, tea tree oil, olive oil and, cocoa butter. After 12 weeks of twice-daily application of the ointment composed of the above ingredients, 10 patients showed a reduction in PASI score of more than 75%, confirming therapeutic efficacy [125]. |
| Paprika Capsicum | Capsaicin (CAP) is the active ingredient in hot peppers, and is included in the group of compounds with antipyretic activity. The substance binds to the TRPV1 receptor, the activation of which is essential for antioxidant and anti-inflammatory activity [126]. A study by Tom C. Chan et al. (….) indicates that the anti-inflammatory effect of CAP is to reduce cytokines such as IL-23, IL-17A, IL-22, TNF-α and IL-6. In turn, the authors [127] showed that capsaicin reduces epidermal hyperplasia, which is often present in psoriasis as a result of excessive epidermal proliferation. | Gupta et al. (2016) conducted a study examining the effect of a gel containing carrier systems (emulsomes) filled with capsaicin and a therapeutic substance commonly used on psoriasis-like skin lesions. The results of the study showed that the use of CAP-enriched vesicles increased the penetration of the drug through the skin affected by hyperproliferation. As a consequence of this action, there is a higher concentration of the drug in the different layers of the skin, resulting in a more effective topical treatment of psoriasis [128]. |
| Coconut Cocos nucifera | Extracted oil from ripe coconut seeds is used in the treatment of psoriasis [109]. Coconut oil (VCO) suppresses pro-inflammatory cytokines at the level of protein expression and inhibits gene expression. Thus showing anti-inflammatory effects [129]. | Chadha et al. in. 2024 conducted a study on the interaction between caffeic acid (CA) obtained from cocos nucifera, and interleukin 17A. The study showed an inhibitory effect of CA on IL-17A, which is actively involved in the pathogenesis of psoriasis [130]. |
| Lavender Lavandula angustifolia | Thanks to two components in lavender oil, such as linalool and linalyl acetate, lavender exhibits anti-inflammatory effects [109]. Topical application of lavender oil reduces nitric oxide (NO) production and decreased myeloperoxidase (MPO) activity, whose decrease in MPO suggests a reduction in neutrophil infiltration… [131]. | In a study conducted on mice with induced psoriasis, lavender oil was applied topically at three different concentrations: 2%, 5%, 10%. The therapeutic dose for mice with psoriasis was lavender oil at 10%, which showed a reduction in PASI, by as much as 73.67% [132]. |
| Eucalyptus Eucalyptus globulus | The anti-inflammatory effect of eucalyptus is attributed to the presence of 1,8-cyneol, which has an inhibitory effect on cytokines [133]. Essential oils extracted from eucalyptus exhibit antioxidant activity by scavenging free radicals and activating antioxidant enzymes. In addition, the essential oils also promote anti-inflammatory effects by inhibiting lipoxygenase and decreasing NO [133]. | The study compared the synergistic effect of a nanoemulsion containing eucalyptus oil and fluticasone propionate (FP) with a commercially available ointment containing FP. The combination of eucalyptus oil and FP in the nanoemulsion has been shown to increase the concentration of FP in different layers of the skin, thus resulting in a reduced PASI and levels of inflammatory cytokines as a result of treatment: IL-1α, IL-6, IL17a involved in the pathogenesis of psoriasis [134]. |
| Fig tree Ficus carica | The common fig tree is rich in polyphenols and flavonoids, which give the plant its antioxidant properties [135]. Following the application of fig fruit extract (FFE), inflammatory factors such as iNOS and COX-2 are reduced, which results in a decrease in NO production. In addition, the anti-inflammatory mechanism of action of FFE is also based on modulating signaling pathways involved in the pathogenesis of psoriasis, in this case, FFE specifically affects the JAK-STAT pathway [135]. | The authors [135] used imiquimod on mice for 7 days, after which the appearance of psoriasis-like lesions on their skin was observed. FEE was applied to the skin of mice in three study groups, with each group differing in the concentration of Ficus carica extract. The result was a reduction in erythema and desquamation of the skin in each group. In the study group that received the high dose of the extract, the reduction in desquamation and erythema was comparable to the study group that received dexamethasone [135]. |
| Garlic Allium sativum | Allicin is an active substance found mainly in garlic. It exhibits anti-inflammatory, anti-proliferative effects and induces apoptosis of keratinocytes [136]. The anti-inflammatory action involves blocking the signaling cascade induced by IL-17 in keratinocytes. In contrast, the inhibition of keratinocyte proliferation by the action of allicin involves the induction of cell cycle arrest in the G2/M phase [136]. | The authors [136] conducted a study in mice that examined the effects of topical allicin application on imiquimod-induced psoriasis-like lesions. A reduction in erythema, desquamation and skin thickness was observed in the study groups that were treated with allicin ointment. In addition, immunohistochemical examination of psoriasis-like lesions showed a reduction in the expression of inflammatory factors and the cell proliferation marker(Ki67) [136]. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kowalska, M.K.; Orłowska, S.M.; Bednarczyk, Ł.; Majewska, J.E.; Hudecka, W. Pathogenesis of Psoriasis vulgaris and Current Management and Therapeutic Strategies Including the Role of Emollients—A Review of the Current Literature. Appl. Sci. 2025, 15, 6811. https://doi.org/10.3390/app15126811
Kowalska MK, Orłowska SM, Bednarczyk Ł, Majewska JE, Hudecka W. Pathogenesis of Psoriasis vulgaris and Current Management and Therapeutic Strategies Including the Role of Emollients—A Review of the Current Literature. Applied Sciences. 2025; 15(12):6811. https://doi.org/10.3390/app15126811
Chicago/Turabian StyleKowalska, Małgorzata Katarzyna, Sara Małgorzata Orłowska, Łukasz Bednarczyk, Joanna Elżbieta Majewska, and Weronika Hudecka. 2025. "Pathogenesis of Psoriasis vulgaris and Current Management and Therapeutic Strategies Including the Role of Emollients—A Review of the Current Literature" Applied Sciences 15, no. 12: 6811. https://doi.org/10.3390/app15126811
APA StyleKowalska, M. K., Orłowska, S. M., Bednarczyk, Ł., Majewska, J. E., & Hudecka, W. (2025). Pathogenesis of Psoriasis vulgaris and Current Management and Therapeutic Strategies Including the Role of Emollients—A Review of the Current Literature. Applied Sciences, 15(12), 6811. https://doi.org/10.3390/app15126811