

Comparative Analysis of Lower Limb Muscle Activity During Isometric External Rotation in Static and Dynamic Modeling Approaches
 , , , and
, , , and 
Abstract
1. Introduction
2. Materials and Methods
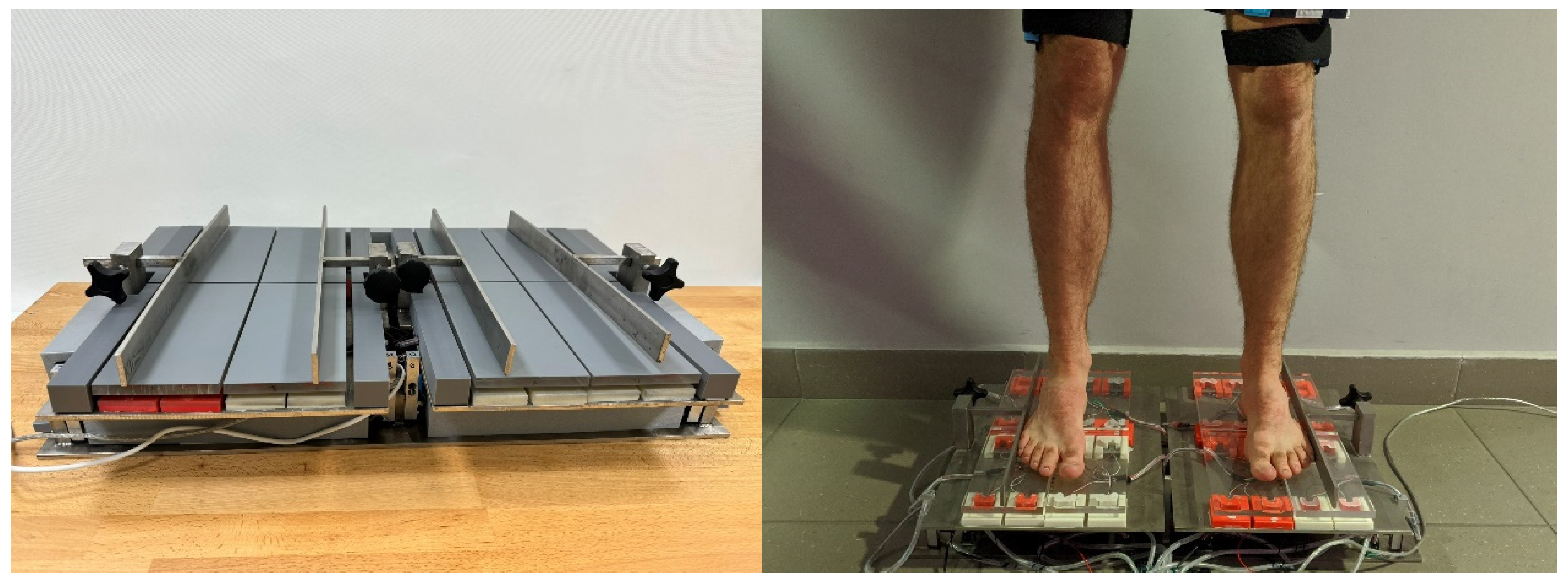
2.1. Description of the Measuring Device
2.2. Participants
2.3. Test Setup
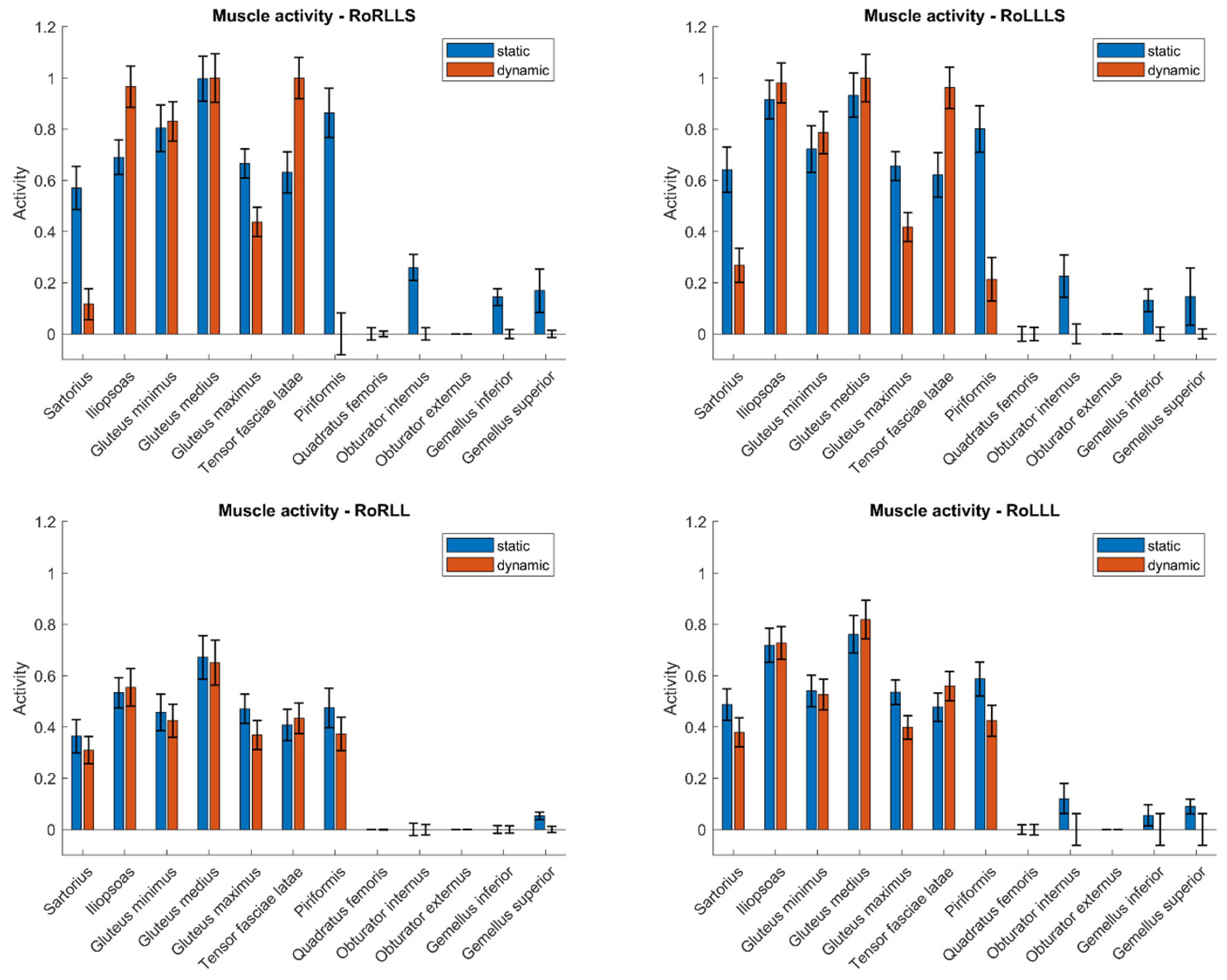
- Maximum external isometric rotation of the right and left lower limbs simultaneously (RoRLLS, RoLLLS) applied in the hip joints for 10 s.
- Maximum external isometric rotation of the right lower limb (RoRLL) applied in the hip joint for 10 s.
- Maximum external isometric rotation of the left lower limb (RoLLL) applied in the hip joint for 10 s.
2.4. Description of Model Studies
- Objective function:
- Limiting conditions:
- fM—muscular force;
- Ni—maximum muscle forces;
- nM—number of muscles;
- C—matrix of arms of muscular strength action and reactions in relation to a given joint;
- f—matrix of muscular forces and reactions present in the system;
- d—resultant moments of external forces determined in relation to a given joint.
- pelvic tilt in the sagittal plane,
- rotational moments of the left and right limbs,
- load on the inner forefoot of the left and right limbs,
- load on the outer forefoot of the left and right limbs,
- load on the hindfoot of the left and right limbs.
2.5. Statistics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Obrębska, P.; Skubich, J.; Piszczatowski, S. Gender Differences in the Knee Joint Loadings during Gait. Gait Posture 2020, 79, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Baffour-Awuah, B.; Pearson, M.J.; Dieberg, G.; Wiles, J.D.; Smart, N.A. An Evidence-Based Guide to the Efficacy and Safety of Isometric Resistance Training in Hypertension and Clinical Implications. Clin. Hypertens. 2023, 29, 9. [Google Scholar] [CrossRef] [PubMed]
- Widodo, A.F.; Tien, C.-W.; Chen, C.-W.; Lai, S.-C. Isotonic and Isometric Exercise Interventions Improve the Hamstring Muscles’ Strength and Flexibility: A Narrative Review. Healthcare 2022, 10, 811. [Google Scholar] [CrossRef]
- Clifford, C.; Challoumas, D.; Paul, L.; Syme, G.; Millar, N.L. Effectiveness of Isometric Exercise in the Management of Tendinopathy: A Systematic Review and Meta-Analysis of Randomised Trials. BMJ Open Sport Exerc. Med. 2020, 6, e000760. [Google Scholar] [CrossRef]
- Anwer, S.; Alghadir, A. Effect of Isometric Quadriceps Exercise on Muscle Strength, Pain, and Function in Patients with Knee Osteoarthritis: A Randomized Controlled Study. J. Phys. Ther. Sci. 2014, 26, 745–748. [Google Scholar] [CrossRef] [PubMed]
- Topp, R.; Woolley, S.; Hornyak, J.; Khuder, S.; Kahaleh, B. The Effect of Dynamic versus Isometric Resistance Training on Pain and Functioning among Adults with Osteoarthritis of the Knee. Arch. Phys. Med. Rehabil. 2002, 83, 1187–1195. [Google Scholar] [CrossRef]
- Phillips, D.A.; Del Vecchio, A.R.; Carroll, K.; Matthews, E.L. Developing a Practical Application of the Isometric Squat and Surface Electromyography. Biomechanics 2021, 1, 145–151. [Google Scholar] [CrossRef]
- Brown, I.E.; Cheng, E.J.; Loeb, G.E. Measured and Modeled Properties of Mammalian Skeletal Muscle. II. The Effects of Stimulus Frequency on Force-Length and Force-Velocity Relationships. J. Muscle Res. Cell Motil. 1999, 20, 627–643. [Google Scholar] [CrossRef]
- Solomonow, M.; Baratta, R.; Zhou, B.H.; Shoji, H.; D’Ambrosia, R.D. The EMG-Force Model of Electrically Stimulated Muscles: Dependence on Control Strategy and Predominant Fiber Composition. IEEE Trans. Biomed. Eng. 1987, 34, 692–703. [Google Scholar] [CrossRef]
- Mokri, C.; Bamdad, M.; Abolghasemi, V. Muscle Force Estimation from Lower Limb EMG Signals Using Novel Optimised Machine Learning Techniques. Med. Biol. Eng. Comput. 2022, 60, 683–699. [Google Scholar] [CrossRef]
- Langenderfer, J.E.; Patthanacharoenphon, C.; Carpenter, J.E.; Hughes, R.E. Variability in Isometric Force and Moment Generating Capacity of Glenohumeral External Rotator Muscles. Clin. Biomech. 2006, 21, 701–709. [Google Scholar] [CrossRef] [PubMed]
- Kian-Bostanabad, S.; Azghani, M.; Parnianpour, M. Evaluation of the Lumbar and Abdominal Muscles Behavior in Different Sagittal Plane Angles during Maximum Voluntary Isometric Extension. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2024, 238, 301–312. [Google Scholar] [CrossRef] [PubMed]
- Damsgaard, M.; Rasmussen, J.; Christensen, S.T.; Surma, E.; de Zee, M. Analysis of Musculoskeletal Systems in the AnyBody Modeling System. Simul. Model. Pract. Theory 2006, 14, 1100–1111. [Google Scholar] [CrossRef]
- Shourijeh, M.S.; Mehrabi, N.; McPhee, J. Forward Static Optimization in Dynamic Simulation of Human Musculoskeletal Systems: A Proof-of-Concept Study. J. Comput. Nonlinear Dyn. 2017, 12, 051005. [Google Scholar] [CrossRef]
- Rasmussen, J.; Damsgaard, M.; Voigt, M. Muscle Recruitment by the Min/Max Criterion—A Comparative Numerical Study. J. Biomech. 2001, 34, 409–415. [Google Scholar] [CrossRef]
- Lund, M.E.; Andersen, M.S.; de Zee, M.; Rasmussen, J. Scaling of Musculoskeletal Models from Static and Dynamic Trials. Int. Biomech. 2015, 2, 1–11. [Google Scholar] [CrossRef]
- Mateus, R.; João, F.; Veloso, A.P. Differences Between Static and Dynamical Optimization Methods in Musculoskeletal Modeling Estimations to Study Elite Athletes. In Proceedings of the Computer Methods, Imaging and Visualization in Biomechanics and Biomedical Engineering, New York, NY, USA, 7–9 September 2021; Ateshian, G.A., Myers, K.M., Tavares, J.M.R.S., Eds.; Springer International Publishing: Cham, Switzerland, 2020; pp. 624–631. [Google Scholar]
- Pandy, M.G. Computer Modeling and Simulation of Human Movement. Annu. Rev. Biomed. Eng. 2001, 3, 245–273. [Google Scholar] [CrossRef]
- Zajac, F.E. Understanding Muscle Coordination of the Human Leg with Dynamical Simulations. J. Biomech. 2002, 35, 1011–1018. [Google Scholar] [CrossRef]
- Chrzan, M.; Michnik, R.; Myśliwiec, A.; Wodarski, P.; Suchoń, S.; Gzik, M.; Mitas, A. The Influence of Isometric Rotation of the Lower Limb on the Functioning of the Knee Joint Stabilizers and Rotator Muscles. Acta Bioeng. Biomech. 2022, 24, 139–146. [Google Scholar] [CrossRef]
- Michnik, R.; Zadoń, H.; Nowakowska-Lipiec, K.; Jochymczyk-Woźniak, K.; Myśliwiec, A.; Mitas, A.W. The Effect of the Pelvis Position in the Sagittal Plane on Loads in the Human Musculoskeletal System. Acta Bioeng. Biomech. 2020, 22, 33–42. [Google Scholar] [CrossRef]
- AnyBody Technology. AnyBody Modeling System Documentation. Available online: https://anyscript.org/ammr/ (accessed on 3 June 2025).
- Ehreiser, S.; Asseln, M.; Radermacher, K. Personalized Prediction of Total Knee Arthroplasty Mechanics Based on Sparse Input Data—Model Validation Using In Vivo Force Data. Biomechanics 2025, 5, 8. [Google Scholar] [CrossRef]
- Dupré, T.; Dietzsch, M.; Komnik, I.; Potthast, W.; David, S. Agreement of Measured and Calculated Muscle Activity during Highly Dynamic Movements Modelled with a Spherical Knee Joint. J. Biomech. 2019, 84, 73–80. [Google Scholar] [CrossRef]
- Semciw, A.I.; Pizzari, T.; Murley, G.S.; Green, R.A. Gluteus Medius: An Intramuscular EMG Investigation of Anterior, Middle and Posterior Segments during Gait. J. Electromyogr. Kinesiol. 2013, 23, 858–864. [Google Scholar] [CrossRef]
- Andersson, E.; Oddsson, L.; Grundström, H.; Thorstensson, A. The Role of the Psoas and Iliacus Muscles for Stability and Movement of the Lumbar Spine, Pelvis and Hip. Scand. J. Med. Sci. Sports 1995, 5, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Arshad, R.; Schmidt, H.; El-Rich, M.; Moglo, K. Sensitivity of the Cervical Disc Loads, Translations, Intradiscal Pressure, and Muscle Activity Due to Segmental Mass, Disc Stiffness, and Muscle Strength in an Upright Neutral Posture. Front. Bioeng. Biotechnol. 2022, 10, 751291. [Google Scholar] [CrossRef]
- Liu, T.; Hulleck, A.A.; El-Rich, M. Sensitivity of Subject-Specific Upper Body Musculoskeletal Model Predictions to Mass Scaling Methods. Comput. Biol. Med. 2023, 165, 107376. [Google Scholar] [CrossRef] [PubMed]
- Zander, T.; Dreischarf, M.; Schmidt, H. Sensitivity Analysis of the Position of the Intervertebral Centres of Reaction in Upright Standing—A Musculoskeletal Model Investigation of the Lumbar Spine. Med. Eng. Phys. 2016, 38, 297–301. [Google Scholar] [CrossRef]
- Wibawa, A.D.; Verdonschot, N.; Halbertsma, J.P.K.; Burgerhof, J.G.M.; Diercks, R.L.; Verkerke, G.J. Musculoskeletal Modeling of Human Lower Limb during Normal Walking, One-Legged Forward Hopping and Side Jumping: Comparison of Measured EMG and Predicted Muscle Activity Patterns. J. Biomech. 2016, 49, 3660–3666. [Google Scholar] [CrossRef]
- Jessup, L.N.; Kelly, L.A.; Cresswell, A.G.; Lichtwark, G.A. Validation of a Musculoskeletal Model for Simulating Muscle Mechanics and Energetics during Diverse Human Hopping Tasks. R. Soc. Open Sci. 2023, 10, 230393. [Google Scholar] [CrossRef]
- Imani Nejad, Z.; Khalili, K.; Hosseini Nasab, S.H.; Schütz, P.; Damm, P.; Trepczynski, A.; Taylor, W.R.; Smith, C.R. The Capacity of Generic Musculoskeletal Simulations to Predict Knee Joint Loading Using the CAMS-Knee Datasets. Ann. Biomed. Eng. 2020, 48, 1430–1440. [Google Scholar] [CrossRef]
- Mokhtarzadeh, H.; Perraton, L.; Fok, L.; Muñoz, M.A.; Clark, R.; Pivonka, P.; Bryant, A.L. A Comparison of Optimisation Methods and Knee Joint Degrees of Freedom on Muscle Force Predictions during Single-Leg Hop Landings. J. Biomech. 2014, 47, 2863–2868. [Google Scholar] [CrossRef]
- Jing, Z.; Han, J.; Zhang, J. Comparison of Biomechanical Analysis Results Using Different Musculoskeletal Models for Children with Cerebral Palsy. Front. Bioeng. Biotechnol. 2023, 11, 1217918. [Google Scholar] [CrossRef] [PubMed]
- Delp, S.L.; Hess, W.E.; Hungerford, D.S.; Jones, L.C. Variation of Rotation Moment Arms with Hip Flexion. J. Biomech. 1999, 32, 493–501. [Google Scholar] [CrossRef] [PubMed]
- Assila, N.; Pizzolato, C.; Martinez, R.; Lloyd, D.G.; Begon, M. EMG-Assisted Algorithm to Account for Shoulder Muscles Co-Contraction in Overhead Manual Handling. Appl. Sci. 2020, 10, 3522. [Google Scholar] [CrossRef]
- Jeon, I. Comparison of Test-Retest Measurement Reliability of Iliopsoas Strength between Break and Make Test in Subjects with Lumbar Extension Syndrome. J. Musculoskelet. Sci. Technol. 2019, 3, 54–58. [Google Scholar] [CrossRef]
- Shah, A.; Bordoni, B. Anatomy, Bony Pelvis and Lower Limb: Gluteus Medius Muscle; StatPearls Publishing: Treasure Island, FL, USA, 2025. [Google Scholar]
- De Luca, C.J. The Use of Surface Electromyography in Biomechanics. J. Appl. Biomech. 1997, 13, 135–163. [Google Scholar] [CrossRef]
- Xu, D.; Zhou, H.; Quan, W.; Ma, X.; Chon, T.-E.; Fernandez, J.; Gusztav, F.; Kovács, A.; Baker, J.S.; Gu, Y. New Insights Optimize Landing Strategies to Reduce Lower Limb Injury Risk. Cyborg Bionic Syst. 2024, 5, 0126. [Google Scholar] [CrossRef]
- Lezak, B.; Varacallo, M.A. Anatomy, Bony Pelvis and Lower Limb: Calf Peroneus Longus Muscle; StatPearls Publishing: Treasure Island, FL, USA, 2025. [Google Scholar]
- Neumann, D.A. Kinesiology of the Musculoskeletal System—E-Book; Mosby: Maryland Heights, MO, USA, 2016; ISBN 9780323527996. [Google Scholar]

{kind=link}
{kind=link}
| RoRLLS | RoLLLS | RoRLL | RoLLL | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | Std | 95% CI | Mean | Std | 95% CI | Mean | Std | 95% CI | Mean | Std | 95% CI | |
| Sartorius | 0.12 | 0.16 | 0.06 to 0.17 | 0.1 | 0.11 | 0.06 to 0.14 | 0.07 | 0.11 | 0.03 to 0.11 | 0.03 | 0.03 | 0.02 to 0.05 |
| Iliopsoas | 0.17 | 0.2 | 0.1 to 0.24 | 0.12 | 0.17 | 0.06 to 0.18 | 0.1 | 0.09 | 0.07 to 0.14 | 0.03 | 0.02 | 0.03 to 0.04 |
| Gluteus minimus | 0.08 | 0.13 | 0.03 to 0.13 | 0.04 | 0.05 | 0.02 to 0.06 | 0.03 | 0.06 | 0.01 to 0.06 | 0.01 | 0.02 | 0.01 to 0.02 |
| Gluteus medius | 0.11 | 0.12 | 0.07 to 0.16 | 0.12 | 0.08 | 0.09 to 0.14 | 0.11 | 0.07 | 0.08 to 0.13 | 0.13 | 0.06 | 0.11 to 0.15 |
| Gluteus maximus | 0.24 | 0.16 | 0.18 to 0.29 | 0.2 | 0.12 | 0.16 to 0.24 | 0.16 | 0.1 | 0.12 to 0.19 | 0.14 | 0.08 | 0.11 to 0.17 |
| Piriformis | 0.15 | 0.23 | 0.07 to 0.23 | 0.09 | 0.14 | 0.04 to 0.14 | 0.05 | 0.11 | 0.01 to 0.09 | 0.04 | 0.06 | 0.02 to 0.06 |
| Quadratus femoris | 0.02 | 0.04 | 0 to 0.03 | 0.01 | 0.05 | 0 to 0.03 | 0 | 0 | 0 to 0 | 0 | 0.01 | 0 to 0.01 |
| Obturator internus | 0.11 | 0.10 | 0.07 to 0.15 | 0.16 | 0.18 | 0.1 to 0.22 | 0.05 | 0.06 | 0.03 to 0.08 | 0.05 | 0.06 | 0.03 to 0.08 |
| Obturator externus | 0 | 0 | 0 to 0 | 0 | 0 | 0 to 0 | 0 | 0 | 0 to 0 | 0 | 0 | 0 to 0 |
| Gemellus inferior | 0.07 | 0.07 | 0.05 to 0.09 | 0.07 | 0.07 | 0.05 to 0.1 | 0.03 | 0.04 | 0.02 to 0.05 | 0.04 | 0.07 | 0.02 to 0.07 |
| Gemellus superior | 0.13 | 0.22 | 0.05 to 0.2 | 0.17 | 0.29 | 0.07 to 0.27 | 0.03 | 0.03 | 0.01 to 0.04 | 0.04 | 0.1 | 0.01 to 0.08 |
| Tensor fasciae latae | 0.07 | 0.13 | 0.03 to 0.12 | 0.07 | 0.1 | 0.04 to 0.11 | 0.02 | 0.06 | 0 to 0.04 | 0.01 | 0.03 | 0.01 to 0.02 |
| Sartorius | Iliopsoas | Gluteus minimus | Gluteus medius | Gluteus maximus | Piriformis | Quadratus femoris | Obturator internus | Obturator externus | Gemellus inferior | Gemellus superior | Tensor fasciae latae | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| RoRLLS | p-value | 0.38 | 0.00 | 0.00 | 0.00 | 0.00 | 0.01 | 0.01 | 0.15 | 0.01 | 0.17 | 0.02 | 0.03 |
| RoLLLS | p-value | 0.05 | 0.00 | 0.00 | 0.06 | 0.00 | 0.02 | 0.20 | 0.13 | 0.01 | 0.55 | 0.03 | 0.13 |
| RoRLL | p-value | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.75 | 0.34 | 0.00 | 0.99 | 0.00 | 0.01 | 0.00 |
| RoLLL | p-value | 0.60 | 0.00 | 0.00 | 0.00 | 0.00 | 0.08 | 0.04 | 0.86 | 0.12 | 0.66 | 0.87 | 0.89 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chrzan, M.; Michnik, R.; Suchoń, S.; Burkacki, M.; Nowakowska-Lipiec, K. Comparative Analysis of Lower Limb Muscle Activity During Isometric External Rotation in Static and Dynamic Modeling Approaches. Appl. Sci. 2025, 15, 6354. https://doi.org/10.3390/app15116354
Chrzan M, Michnik R, Suchoń S, Burkacki M, Nowakowska-Lipiec K. Comparative Analysis of Lower Limb Muscle Activity During Isometric External Rotation in Static and Dynamic Modeling Approaches. Applied Sciences. 2025; 15(11):6354. https://doi.org/10.3390/app15116354
Chicago/Turabian StyleChrzan, Miłosz, Robert Michnik, Sławomir Suchoń, Michał Burkacki, and Katarzyna Nowakowska-Lipiec. 2025. "Comparative Analysis of Lower Limb Muscle Activity During Isometric External Rotation in Static and Dynamic Modeling Approaches" Applied Sciences 15, no. 11: 6354. https://doi.org/10.3390/app15116354
APA StyleChrzan, M., Michnik, R., Suchoń, S., Burkacki, M., & Nowakowska-Lipiec, K. (2025). Comparative Analysis of Lower Limb Muscle Activity During Isometric External Rotation in Static and Dynamic Modeling Approaches. Applied Sciences, 15(11), 6354. https://doi.org/10.3390/app15116354