

Investigation of the Clinical Value of Three-Dimensional-Printed Personalised Vascular Models for the Education and Training of Clinicians When Performing Interventional Endovascular Procedures



Abstract
1. Introduction
2. Materials and Methods
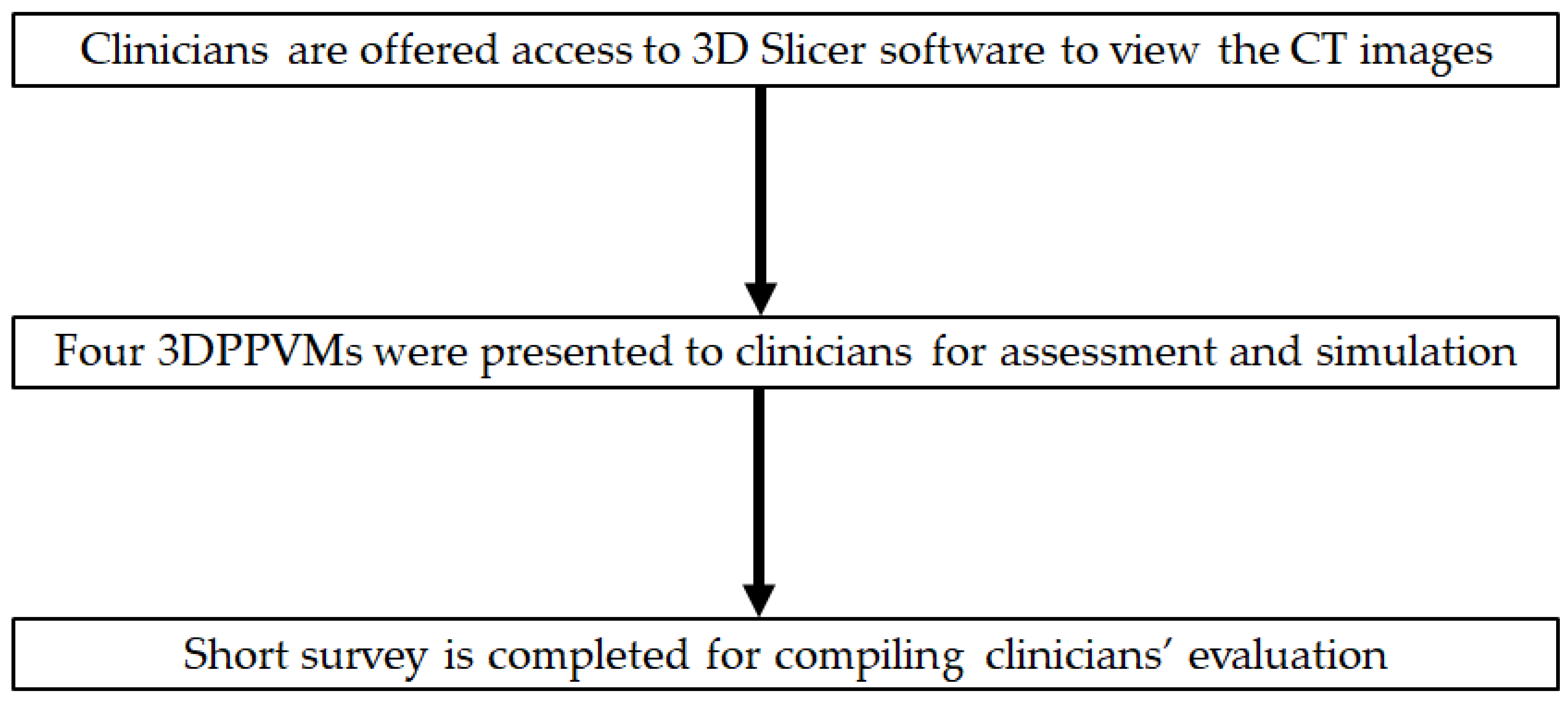
2.1. Study Strategy
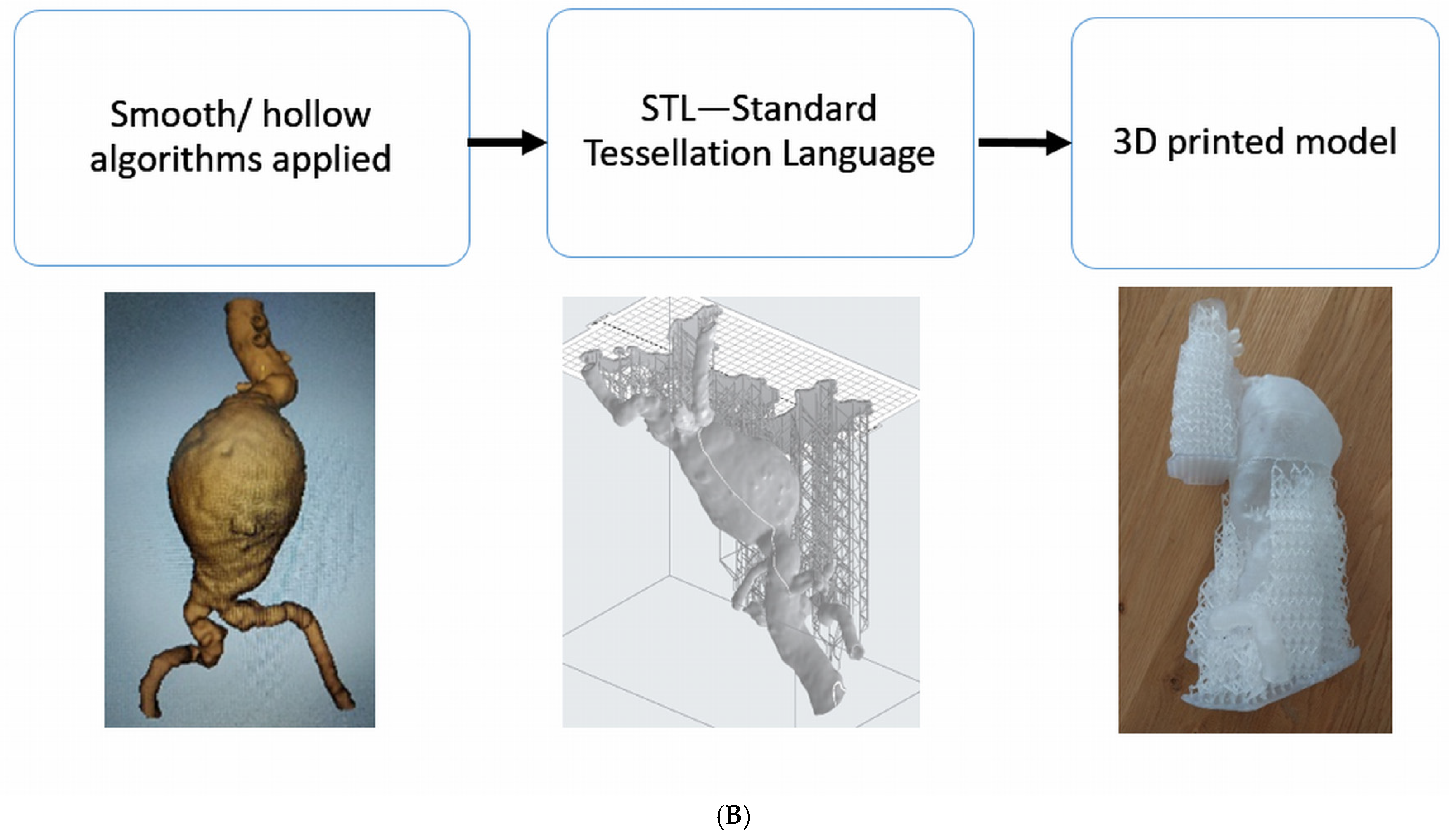
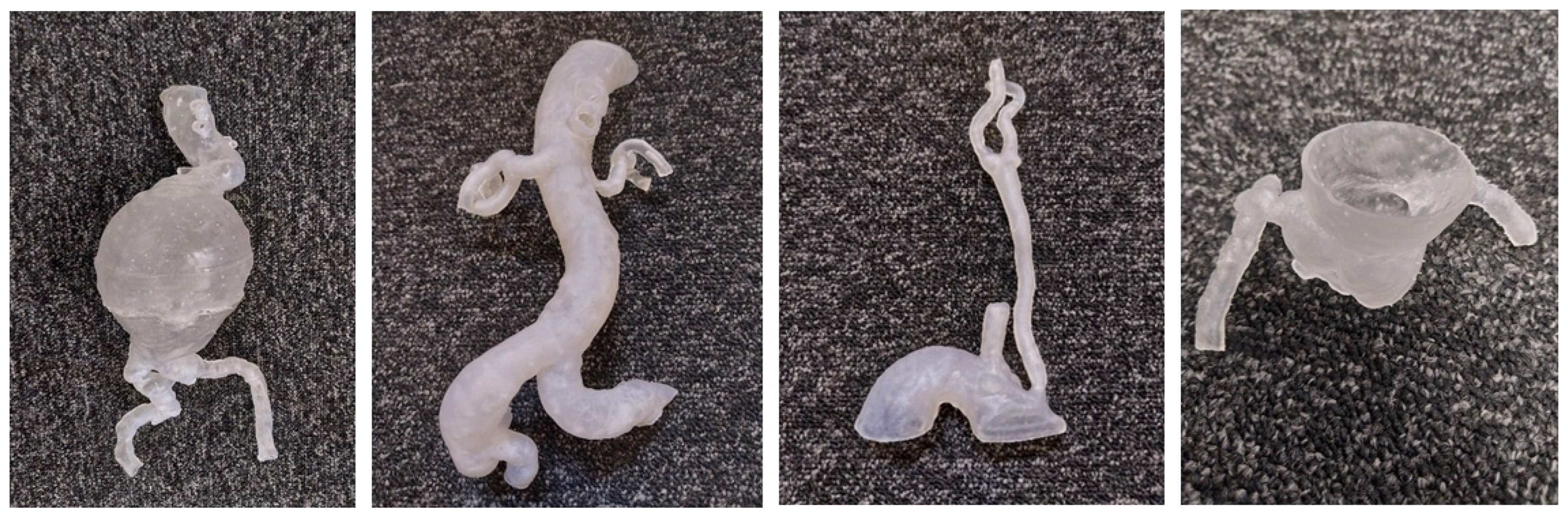
2.2. Development of 3D-Printed Vascular Models
2.3. Material Selection
2.4. Participant Recruitment
2.5. Statistical Analysis
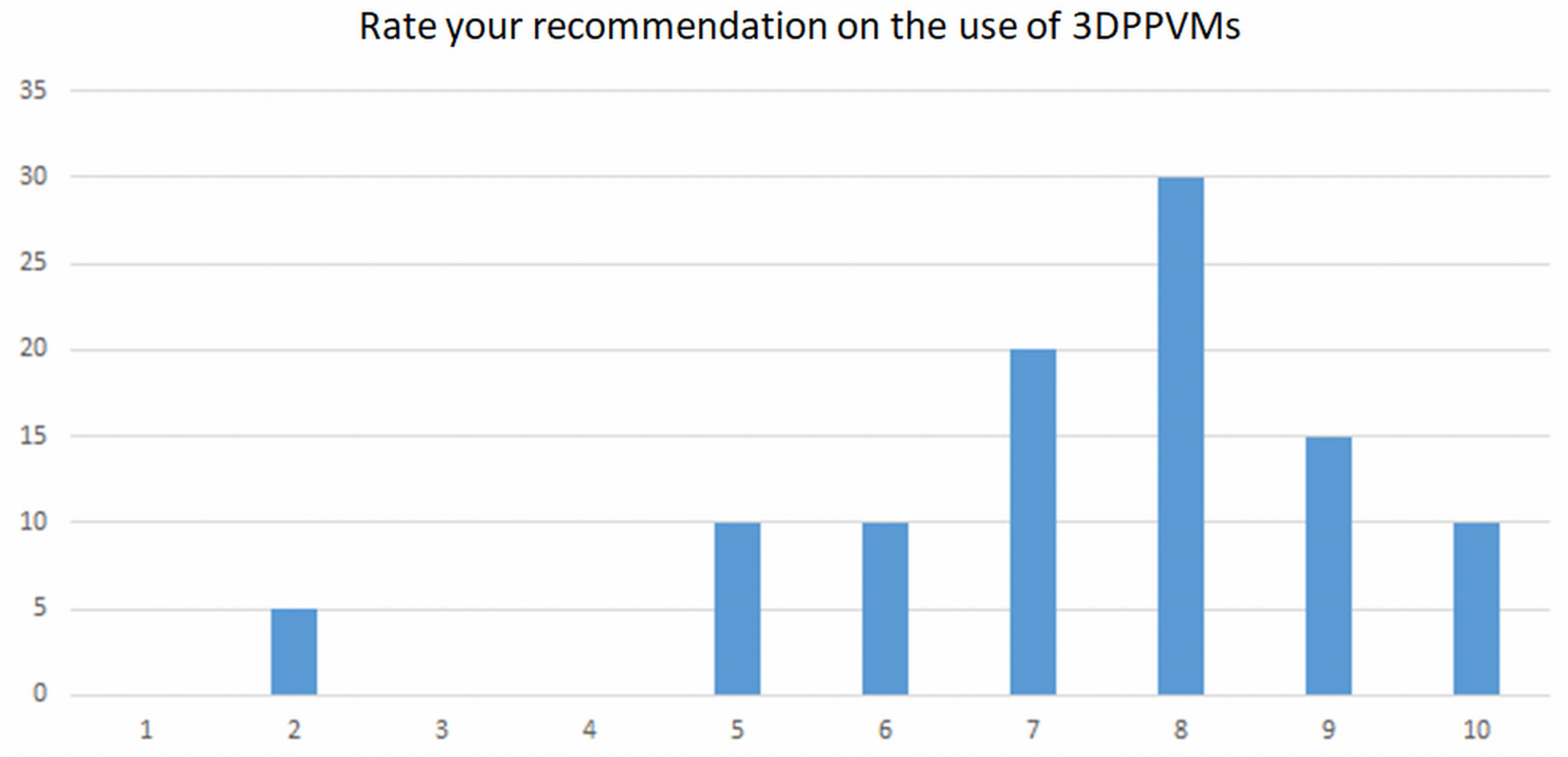
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Correction Statement
References
- Yaprak, F.; Ozer, M.A.; Govsa, F.; Cinkooglu, A.; Pinar, Y.; Gokmen, G. Prespecialist perceptions of three-dimensional heart models in anatomical education. Surg. Radiol. Anat. 2023, 45, 1165–1175. [Google Scholar] [CrossRef]
- Bonvini, S.; Raunig, I.; Demi, L.; Spadoni, N.; Tasselli, S. Unsuspected limitations of 3D printed model in planning of complex aortic aneurysm endovascular treatment. Vasc. Endovasc. Surg. 2024, 58, 645–650. [Google Scholar] [CrossRef]
- Arango, S.; Gorbaty, B.; Brigham, J.; Iaizzo, P.A.; Perry, T.E. A role for ultra-high resolution three-dimensional printed human heart models. Echocardiography 2023, 40, 703–710. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.A.; Squelch, A.; Sun, Z. Investigation of three-dimensional printing materials for printing aorta model replicating type B aortic dissection. Curr. Med. Imaging 2021, 17, 843–849. [Google Scholar] [CrossRef] [PubMed]
- Rynio, P.; Kazimierczak, A.; Jedrzejczak, T.; Gutowski, P. A 3-dimensional printed aortic arch template to facilitate the creation of physician-modified stent-grafts. J. Endovasc. Ther. 2018, 25, 554–558. [Google Scholar] [CrossRef] [PubMed]
- Rynio, P.; Wojtun, M.; Wojcik, K.; Kawa, M.; Falkowski, A.; Gutowski, P.; Kazimierczak, A. The accuracy and reliability of 3D printed aortic templates: A comprehensive three-dimensional analysis. Quant. Imaging Med. Surg. 2022, 12, 1385–1396. [Google Scholar] [CrossRef]
- Tang, F.; Hu, C.; Huang, S.; Long, W.; Wang, Q.; Xu, G.; Liu, S.; Qang, B.; Zhang, L.; Li, L. An innovative customized stent graft manufacture system assisted by three-dimensional printing technology. Ann. Thorac. Surg. 2021, 112, 308–314. [Google Scholar] [CrossRef]
- Zheng, R.; Huayuan, X.; Zhu, F.; Cheng, C.; Huang, W.; Zhang, H.; He, X.; Shen, K.; Liu, Y.; Lu, Q.; et al. Clinical comparative analysis of 3D printing-assisted extracorporeal pre-fenestration and Castor integrated branch stent techniques in treating type B aortic dissections with inadequate proximal landing zones. BMC. Cardiovasc. Dis. 2024, 24, 124. [Google Scholar] [CrossRef]
- Huang, J.; Lo, G.; Wang, W.; Wu, K.; Le, T. 3D printing guiding stent graft fenestration: A novel technique for fenestration in endovascular aneurysm repair. Vascular 2017, 25, 442–446. [Google Scholar] [CrossRef]
- Tong, Y.H.; Yu, T.; Zhou, M.J.; Liu, C.; Zhou, M.; Jiang, Q.; Liu, C.J.; Li, X.Q.; Liu, Z. Use of 3D printing to guide creation of fenestrations in physician-modified stent grafts for treatment of thoracoabdominal aortic disease. J. Endovasc. Ther. 2020, 27, 385–393. [Google Scholar] [CrossRef]
- Zhou, J.; Xu, J.; Wang, X.; Shu, Y. Personalized 3D-print-covered stent grafts for endovascular treatment of complicated abdominal aortic dissection with Marfan syndrome. Asian J. Surg. 2023, 46, 1387–1389. [Google Scholar] [CrossRef] [PubMed]
- Wibowo, G.; Anggrahini, D.W.; Rismawanti, R.I.; Fatimah, V.A.N.; Hakim, A.; Hidayah, R.N.; Gharini, P.P.R. 3D-Printing-Based Fluoroscopic Coronary Angiography Simulator Improves Learning Capability Among Cardiology Trainees. Adv. Med. Educ. Pract. 2023, 14, 763–771. [Google Scholar] [CrossRef]
- Nasr, B.; Lareyre, F.; Guigo, S.; Bellenger, K.; Raffort, J.; Goueffic, Y. 3-dimensional printing in vascular disease: From manufacturer to clinical use. Semin. Vasc. Surg. 2024, 37, 326–332. [Google Scholar] [CrossRef]
- Bernhard, B.; Illi, J.; Gloeckler, M.; Pilgrim, T.; Praz, F.; Windecker, S.; Haeberlin, A.; Grani, C. Imaging-Based, Patient-Specific Three-Dimensional Printing to Plan, Train, and Guide Cardiovascular Interventions: A Systematic Review and Meta-Analysis. Heart Lung. Circ. 2022, 31, 1203–1218. [Google Scholar] [CrossRef] [PubMed]
- Tam, M.D.; Latham, T.R.; Lewis, M.; Khanna, K.; Zaman, A.; Parker, M.; Grunwald, I.Q. A pilot study assessing the impact of 3-D printed models of aortic aneurysms on management decisions in EVAR planning. Vasc. Endovascular. Surg. 2016, 50, 4–9. [Google Scholar] [CrossRef]
- Torres, I.O.; Luccia, N.D. A simulator for training in endovascular aneurysm repair: The use of three-dimensional printers. Eur. J. Vasc. Endovasc. Surg. 2017, 54, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Sakai, A.K.F.; Cestai, I.N.; de Sales, E.; Mazzetto, M.; Cestai, I.A. Metamaterial design for aortic aneurysm simulation using 3D printing. 3D Print. Med. 2024, 10, 29. [Google Scholar] [CrossRef]
- Lau, I.; Gupta, A.; Ihdayhid, A.; Sun, Z. Clinical applications of mixed reality and 3D printing in congenital heart disease. Biomolecules 2022, 12, 1548. [Google Scholar] [CrossRef] [PubMed]
- Coles-Black, J.; Barber, T.; Bolton, D.; Chuen, J. A systematic review of three-dimensional printed template-assisted physician-modified stent grafts for fenestrated endovascular aneurysm repair. J. Vasc. Surg. 2021, 74, 296–306. [Google Scholar] [CrossRef]
- Coles-Black, J.; Bolton, D.; Chuen, J. Accessing 3D printed vascular phantoms for procedural simulation. Front. Surg. 2021, 7, 626212. [Google Scholar] [CrossRef]
- Patel, H.; Choi, P.; Ku, J.C.; Vergara, R.; Malgor, R.; Patel, D.; Li, Y. Application of three-dimensional printing in the planning and execution of aortic aneurysm repair. Front. Cardiovasc. Med. 2025, 11, 1485267. [Google Scholar] [CrossRef] [PubMed]
- Rhee, Y.; Park, S.J.; Kim, T.; Kim, N.; Yang, D.H.; Kim, J.B. Pre-sewn multi-branched aortic graft and 3D-printing guidance for Crawford extent II or III thoracoabdominal aortic aneurysm repair. Semin. Thorac. Cardiovasc. Surg. 2021, 34, 816–822. [Google Scholar] [CrossRef]
- Raffort, J.; Adam, C.; Carrier, M.; Ballaith, A.; Coscas, R. Jen-Baptise, E; Hassen-Khodja, R.; Chakfé, N.; Lareyre, F. Artificial intelligence in abdominal aortic aneurysm. J. Vasc. Surg. 2020, 72, 321–323.E1. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.Y.; Squelch, A.; Sun, Z. Investigation of the clinical value of four visualization modalities for congenital heart disease. J. Cardiovasc. Dev. Dis. 2024, 11, 278. [Google Scholar] [CrossRef]
- Ganguli, A.; Pagan-Diaz, G.J.; Grant, L.; Cvetkovic, C.; Bramlet, M.; Vozenilek, J.; Kesavadas, T.; Bashir, R. 3D printing for preoperative planning and surgical training. A review. Biomed. Microdevices 2018, 20, 65. [Google Scholar] [CrossRef]
- Sun, Z.; Wee, C. 3D printed models in cardiovascular disease: An exciting future to deliver personalized medicine. Micromachines 2022, 13, 1575. [Google Scholar] [CrossRef] [PubMed]
- Catasta, A.; Martini, C.; Mersanne, A.; Foresti, R.; Bianchini Massoni, C.; Freyrie, A.; Perini, P. Systematic review on the use of 3D-printed models for planning, training and simulation in vascular surgery. Diagnostics 2024, 14, 1658. [Google Scholar] [CrossRef]
- McGuire, L.S.; Fuentes, A.; Alaraj, A. Three-dimensional modelling in training, simulation, and surgical planning in open vascular and endovascular neurosurgery: A systematic review of the literature. World Neurosurg. 2021, 154, 53–63. [Google Scholar] [CrossRef]
- El Sabbagh, A.; Eleid, M.F.; Al-Hijji, M.; Anavekar, N.S.; Holmes, D.R.; Nkomo, V.T.; Oderich, G.S.; Cassiv, S.D.; Said, S.M.; Rihal, C.S.; et al. The various applications of 3D printing in cardiovascular diseases. Curr. Cardiol. Rep. 2018, 20, 7. [Google Scholar] [CrossRef]
- Gomes, E.N.; Dias, R.R.; Rocha, B.A.; Santiago, J.A.D.; de Souza Dinato, F.J.; Saadi, E.K.; Gomes, W.J.; Jatene, F.B. Use of 3D printing in preoperative planning and training for aortic endovascular repair and aortic valve disease. Braz. J. Cardiovasc. Surg. 2018, 33, 490–495. [Google Scholar] [CrossRef]
- Measanne, A.; Foresti, R.; Martini, C.; Malvezzi, C.C.; Rossi, G.; Fornasari, A.; De Filippo, M.; Freyrie, A.; Perini, P. In-house fabrication and validation of 3D-printed custom-made medical devices for planning and simulation of peripheral endovascular therapies. Diagnostics 2024, 15, 8. [Google Scholar] [CrossRef] [PubMed]
- Fu, D.S.; Jin, Y.; Zhao, Z.H.; Wang, C.; Shi, Y.H.; Zhou, M.J.; Zhao, J.X.; Liu, C.; Qiao, T.; Liu, C.J.; et al. Three-dimensional printing to guide fenestrated/branched TEVAR in triple aortic arch branch reconstruction with curative effect analysis. J. Endovasc. Ther. 2024, 31, 1088–1097. [Google Scholar] [CrossRef] [PubMed]
- Karkkainen, J.M.; Sandri, G.; Tenorio, E.R.; Alexander, A.; Bjellum, K.; Matsumoto, J.; Morris, J.; Mendes, B.C.; DeMartino, R.R.; Oderich, G.S. Simulation of endovascular aortic repair using 3D printed abdominal aortic aneurysm model and fluid pump. Cardiovasc. Interv. Radiol. 2019, 42, 1627–1634. [Google Scholar] [CrossRef] [PubMed]
- Kaschwich, M.; Sieren, M.; Matysiak, F.; Bouchagiar, J.; Dell, A.; Bayer, A.; Ernst, F.; Ellebrecht, D.; Kleemann, M.; Horn, M. Feasibility of an endovascular training and research environment with exchangeable patient specific 3D printed vascular anatomy: Simulator with exchangeable patient-specific 3D-printed vascular anatomy for endovascular training and research. Ann. Anat. 2020, 231, 151519. [Google Scholar] [CrossRef] [PubMed]
- Silberstein, J.; Tran, S.; Wong, Y.H.; Yeong, C.H.; Sun, Z. Development of a 3D-printed chest phantom with simulation of lung nodules for studying ultra-low-dose computed tomography protocols. Appl. Sci. 2025, 15, 309. [Google Scholar] [CrossRef]
- Kargul, M.; Skorka, P.; Gutowski, P.; Kazimierczak, A.; Rynio, P. Empowering EVAR: Revolutionizing patient understanding and qualification with 3D Printing. J. Cardiovasc. Dev. Dis. 2024, 11, 365. [Google Scholar] [CrossRef]
- Grab, M.; Hundertmark, F.; Thierfelder, N.; Fairchild, M.; Mela, P.; Hagl, C.; Grefen, L. New perspectives in patient education for cardiac surgery using 3D-printing and virtual reality. Front. Cardiovasc. Med. 2023, 10, 1092007. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Questions | Artery Models | Mean | SD | p-Value |
|---|---|---|---|---|
| Do the 3DPPVMs… | ||||
| Demonstrate realism | Coronary | 3.85 | 0.93 | 0.23 |
| Carotid | 3.90 | 0.97 | 0.23 | |
| Aorta | 4.10 | 0.89 | 0.002 | |
| Renal | 3.85 | 0.93 | 0.001 | |
| Accurately display anatomical structures | Coronary | 4.25 | 0.72 | 0.59 |
| Carotid | 4.30 | 0.73 | 0.54 | |
| Aorta | 4.29 | 0.85 | 0.53 | |
| Renal | 4.20 | 0.77 | 0.15 | |
| Enhance understanding of the disease shown | Coronary | 3.95 | 1.23 | 0.19 |
| Carotid | 3.89 | 1.24 | 0.36 | |
| Aorta | 3.86 | 1.20 | 0.11 | |
| Renal | 3.80 | 1.28 | 0.21 | |
| Enhance interventional radiology procedure required | Coronary | 3.65 | 0.88 | 0.46 |
| Carotid | 3.70 | 0.80 | 0.60 | |
| Aorta | 3.57 | 1.08 | 0.29 | |
| Renal | 3.50 | 1.00 | 0.29 | |
| Enhance planning of interventions | Coronary | 3.80 | 0.95 | 0.04 |
| Carotid | 3.85 | 0.99 | 0.14 | |
| Aorta | 3.90 | 1.12 | 0.09 | |
| Renal | 3.75 | 1.07 | 0.04 | |
| Enhance pre-intervention simulation | Coronary | 3.80 | 1.06 | 0.68 |
| and selection of interventional radiology devices | Carotid | 3.95 | 0.95 | 0.31 |
| Aorta | 4.05 | 0.95 | 0.24 | |
| Renal | 3.80 | 1.01 | 0.28 | |
| Develop haptic skills | Coronary | 3.50 | 0.99 | 0.61 |
| Carotid | 3.50 | 0.99 | 0.61 | |
| Aorta | 3.56 | 0.98 | 0.61 | |
| Renal | 3.50 | 0.99 | 0.61 | |
| Reduce procedure time | Coronary | 3.26 | 1.05 | 0.80 |
| Carotid | 3.32 | 1.06 | 0.65 | |
| Aorta | 3.47 | 1.12 | 0.59 | |
| Renal | 3.22 | 1.00 | 0.65 | |
| Clarify pathology to patients | Coronary | 4.21 | 0.92 | 0.49 |
| Carotid | 4.26 | 0.87 | 0.68 | |
| Aorta | 4.33 | 0.69 | 0.70 | |
| Renal | 4.17 | 0.92 | 0.49 | |
| Clarify pathology to health professionals | Coronary | 4.00 | 1.20 | 0.54 |
| Carotid | 4.00 | 1.11 | 0.66 | |
| Aorta | 4.00 | 1.05 | 0.61 | |
| Renal | 3.83 | 1.20 | 0.54 |
| Theme | Response | Total |
|---|---|---|
| 3DPPVM static lumen | Beneficial for simulating blood fluid flow | (n = 3) |
| 3DPPVM show disease | Demonstrate disease well to health professionals | (n = 3) |
| 3DPPVM education | Good for clinician training | (n = 3) |
| 3DPPVM access vessels | Longer access to vessels for simulation | (n = 2) |
| 3DPPVM visualisation | More realistic than CTA images | (n = 1) |
| N | Minimum | Maximum | Sum | Mean | Std. Deviation | |
|---|---|---|---|---|---|---|
| Pre-interventional planning | 19 | 1 | 4 | 48 | 2.53 | 1.219 |
| Pre-interventional simulation | 19 | 1 | 5 | 58 | 3.05 | 1.508 |
| Interventional orientation | 19 | 1 | 5 | 66 | 3.47 | 1.429 |
| Communication in medical practice | 19 | 1 | 5 | 54 | 2.84 | 1.675 |
| Education/training | 19 | 1 | 5 | 40 | 2.11 | 1.370 |
| N | Minimum | Maximum | Sum | Mean | Std. Deviation | |
|---|---|---|---|---|---|---|
| Static nature | 20 | 1 | 5 | 54 | 2.70 | 1.490 |
| Softness | 20 | 1 | 5 | 66 | 3.30 | 1.031 |
| Lack of surrounding structures | 20 | 1 | 5 | 44 | 2.20 | 1.281 |
| Orientation for simulation | 20 | 1 | 5 | 77 | 3.85 | 1.309 |
| Education/training | 20 | 4 | 5 | 91 | 4.55 | 0.510 |
| Themes | Responses | Total |
|---|---|---|
| General comments on | Excellent potential tool (n = 2) | |
| 3DPPVM | (n = 2) | |
| Visual advantages of | Visually more realistic than CTA images (n = 1) | |
| 3DPPVM | Excellent for visualising complex pathology, | |
| which cannot be achieved by imaging alone (n = 1) | (n = 2) | |
| Use of 3DPPVM as a training aid | Useful for education in complex cases (n = 2) | |
| Helpful tool for patient education (n = 3) | (n = 5) | |
| Use of 3DPPVM for | Useful for surgical planning of complex cases (n = 2) | (n = 2) |
| surgical planning | ||
| Use of 3DPPVM to | Excellent for complex pathology (n = 1) | |
| demonstrate disease to | ||
| health professionals | (n = 1) | |
| Limitations of 3DPPVM | Include blood flow to remedy static model nature (n = 2) | |
| Introduce arterial pressure for realism (n = 1) | ||
| Extend access vessels for aortic simulation (n = 1) | (n = 4) | |
| Participant suggestions | Model the supporting scaffold to mimic surrounding | |
| for 3DPPVM improvement | anatomy (n = 1) | |
| Have access site to lesion for true orientation (n = 1) | ||
| Create a clear model to visualise simulation (n = 1) | (n = 3) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Daring, D.L.; Sun, Z. Investigation of the Clinical Value of Three-Dimensional-Printed Personalised Vascular Models for the Education and Training of Clinicians When Performing Interventional Endovascular Procedures. Appl. Sci. 2025, 15, 5695. https://doi.org/10.3390/app15105695
Daring DL, Sun Z. Investigation of the Clinical Value of Three-Dimensional-Printed Personalised Vascular Models for the Education and Training of Clinicians When Performing Interventional Endovascular Procedures. Applied Sciences. 2025; 15(10):5695. https://doi.org/10.3390/app15105695
Chicago/Turabian StyleDaring, Deborah L., and Zhonghua Sun. 2025. "Investigation of the Clinical Value of Three-Dimensional-Printed Personalised Vascular Models for the Education and Training of Clinicians When Performing Interventional Endovascular Procedures" Applied Sciences 15, no. 10: 5695. https://doi.org/10.3390/app15105695
APA StyleDaring, D. L., & Sun, Z. (2025). Investigation of the Clinical Value of Three-Dimensional-Printed Personalised Vascular Models for the Education and Training of Clinicians When Performing Interventional Endovascular Procedures. Applied Sciences, 15(10), 5695. https://doi.org/10.3390/app15105695