Abstract
Prolonged driving is associated with fatigue and reduced comfort, jeopardizing driver safety. This study proposes an innovative Anti-Fatigue Massage Function (AFMF) system integrated into a driver’s seat to improve subjective comfort and decrease compensatory movements during extended driving due to fatigue. In total, 24 participants (12 males, 12 females) completed two 60 min simulated driving sessions—one with the AFMF activated and one with it deactivated. Subjective comfort was measured every 10 min using a 5-point Likert scale, while objective In-Chair Movements (ICMs) were manually recorded by expert researchers from dual-camera recordings. ART ANOVA revealed that the AFMF-equipped seat significantly enhanced comfort ratings and reduced ICM frequencies compared to the deactivated condition. These findings suggest that the AFMF system can enhance driver well-being and mitigate fatigue-related risks during prolonged driving.
1. Introduction
Driver comfort has become a critical priority in the automotive industry, evolving from a secondary consideration to an essential feature in an increasingly competitive market [1]. Recognizing that comfort enhances overall safety, vehicle manufacturers now prioritize increasing physical comfort to sustain driver focus [1]. This emphasis is especially significant for long-distance driving, where maintaining concentration is vital for safe operation. As demand for comfortable vehicles grows, the industry is driven to develop innovations that address driver’s comfort and safety.
Inadequate comfort can play a significant role in contributing to fatigue, which, in turn, compromises road safety and elevates the likelihood of accidents [2]. Research indicates reduced comfort can rapidly lead to fatigue, impairing driver alertness and reaction times. Fatigue-related accidents represent a major global issue, with fatigued drivers being three times more likely to be involved in a car accident [2]. In the United States, drowsy driving is responsible for approximately 328,000 accidents each year, leading to 109,000 injuries and 6400 fatalities [2]. Between 2017 and 2021, drowsy driving was linked to over 17% of fatal accidents [2]. These statistics underscore the urgent need to enhance comfort as a means to mitigate both driver fatigue and the cumulative stress that contributes to MSDs.
Drivers who spend extended periods seated are at increased risk for developing MSDs, a major concern related to automotive seating. Long-term drivers, who experience continuous stress on the spine, muscles, and joints, are particularly vulnerable [3,4,5,6]. Research reveals that individuals who drive more than 20 h per week report almost six times higher incidences of lower back pain due to MSDs than those who drive less than 10 h per week [3,4]. Additionally, prolonged sitting while driving has been closely linked to the prevalence of MSDs among drivers [5,7]. Studies found that long-term drivers experience a 61.75% prevalence of MSDs, with the upper body being the most affected area [6]. Addressing these health implications is essential for enhancing a driver’s well-being and productivity.
The driver’s seat is a crucial component of any vehicle, with modern designs incorporating features like lumbar support, massage functions, and active seat systems to enhance comfort and reduce fatigue during long journeys [8,9,10,11,12,13]. Research has shown that lumbar support systems effectively alleviate lower back strain and improve posture during extended driving, and they have been found to reduce the prevalence of lower back pain among drivers [8,10]. Additionally, lumbar support systems have decreased the prevalence of lower back pain among drivers. However, drivers who depend on these supports may reduce body movement and neglect regular breaks to walk or stretch, further exacerbating the risk of muscular weakening. Massage seats further enhance driver comfort by utilizing dynamic pressure points that stimulate blood flow and alleviate muscle tension. Mechanical massage systems integrated into seats effectively reduce muscle tension and alleviate lower back pain through vibrations [9,14]. However, these systems have limitations; while they effectively increase short-term comfort and muscle tension, their impact on long-term fatigue is less well-documented. Another innovation, active seat systems, introduce subtle movements to prevent static posture and have shown promise in reducing driver fatigue [11,12]. Research on seat suspension systems suggests that they can improve ride comfort by actively counteracting vehicle vibrations. However, active systems also come with limitations, including increased complexity, potential distractions or safety risks, potential maintenance challenges, and the possibility of reduced comfort for certain users [11]. Consequently, there remains a critical need for continued advancements in seat-specific comfort technologies that effectively enhance immediate comfort and overall driver safety.
This study aims to develop a vehicle seat with an Anti-Fatigue Massage Function (AFMF) to promote regular pelvic movement in drivers and enhance comfort during extended driving sessions. AFMF employs a unique alternating inflation and deflation mechanism, dynamically adjusting the seat to prompt subtle posture changes and actively counteract the onset of fatigue. To evaluate the effectiveness of the AFMF-equipped seat, subjective survey data were collected alongside the analysis of In-Chair Movements (ICMs), an indirect measure of reduced comfort. Building on previous literature, ICM was categorized by its magnitude, offering a standardized framework for a comprehensive assessment of comfort level [15,16,17,18]. The research questions guiding this investigation were as follows: “Does the AFMF-equipped driving seat improve seat-specific driver comfort during long-term driving?” and “Can the AFMF-equipped seat reduce ICM during extended driving?” It was hypothesized that drivers using the AFMF-equipped seat would report significantly higher comfort levels and experience less ICM compared to those using a standard seat. The standard seat, in this context, refers to the seat without the AFMF system. By integrating both subjective comfort evaluations and objective ICM measurements, this study assessed the potential of the AFMF system to improve driver comfort and reduce fatigue-related movements during long drives. The anticipated outcome was that the AFMF-equipped seat would enhance comfort by providing subtle, nearly imperceptible massage movements that reduce physical strain and minimize distractions, making it an effective solution for extended driving.
2. Materials and Methods
2.1. The AFMF Driver’s Seat
The AFMF-equipped driver’s seat (Figure 1a) was designed and manufactured specifically for this study to enhance comfort during extended driving sessions by integrating massage patterns that promote regular pelvic movement in drivers. The seat was securely positioned on a stable base within the testing environment, ensuring consistent performance and minimizing external influences that might affect the results.

Figure 1.
(a) The AFMF Driver Seat; (b) Bladder Locations.
The AFMF seat utilized an advanced modular configuration that included inflatable bladders, pumps, pressure sensors, and a central control system to dynamically adjust the seat’s surface contours, ensuring sustained comfort during long periods of driving. The system incorporated a combination of bladders strategically placed within the seat structure (Figure 1b) to target specific anatomical regions (Table 1).

Table 1.
Bladder Locations and Functions in the AFMF Driver Seat.
The AFMF system was organized into nine independent modules, each controlling specific bladders, pumps, and pressure sensors. These modules communicate through a Local Interconnect Network, enabling seamless data exchange between the central controller and individual components. This modular design facilitates scalability and allows for precise regulation of bladder inflation and deflation cycles. The system was distributed across the seat’s backrest, cushion, and bolsters, with strategic placement aimed at addressing key pressure points and it incorporated high-precision pumps and pressure sensors, which modulate bladder inflation in real time, working in concert with a centralized Pressure Sensor Controller to dynamically adjust pressure distribution.
The pumps were controlled using Pulse Width Modulation (PWM), which allowed for variable speed adjustments to regulate air delivery to the bladders. PWM settings were determined in a pilot study, with values established at Low (70), Medium (80), and High (100). These settings were selected to balance noise levels, inflation speed, and energy efficiency of the pump.
Massage intensity settings were refined through a pilot study to accommodate various user comfort preferences. The configurations were set to Low (0.2 kPa), Medium (0.3 kPa), and High (0.5 kPa) based on user feedback. These intensity values, measured in kilopascals (kPa), provide a quantifiable measure of comfort.
A series of inflation and deflation patterns were assessed in a pilot study with three participants to evaluate their effectiveness in promoting dynamic posture adjustments, enhancing comfort, and redistributing pressure. While the sample size was limited, the inclusion of three participants is consistent with established engineering usability research, where studies have shown that 3–5 users are typically sufficient to identify the majority of usability issues and to refine system parameters effectively [19,20]. In this pilot study, a series of inflation and deflation patterns were evaluated to determine their effectiveness in promoting dynamic posture adjustments, alleviating fatigue, and redistributing pressure. These patterns varied in terms of targeted areas, inflation sequences, and directional flow, as illustrated in Figure 2. Based on participant feedback, the Balanced Mix (BM) pattern was selected as the most effective, offering the optimal balance of comfort and support.

Figure 2.
Several of the Patterns Generated for Inflation and Deflation. The Letters in Each Part of the Figure Represent the Bladders in the Seat.
A subsequent pilot study employed a 3 × 3 factorial design, varying pump speed (Low = 70, Medium = 80, High = 100) and power (Low = 0.2 kPa, Medium = 0.3 kPa, High = 0.5 kPa), resulting in nine experimental trials. Based on these trials, a combination of Medium pump speed (80) and High massage intensity (0.5 kPa) was identified as the most effective configuration for providing consistent comfort and supporting dynamic posture adjustments. The research and subsequent experiments were based on these settings.
2.2. SimGear Driving Simulator
The study employed the SimGear driving simulator (Figure 3) to replicate a realistic and immersive driving environment. The simulator consists of a steering wheel and accelerator and brake pedals, complemented by three high-definition LCD monitors that provide a wide field of view, thereby delivering a lifelike driving experience. This setup allowed for the assessment of the effects of prolonged sitting and the AFMF system. The Carla driving simulation software was integrated with the SimGear system to create driving scenarios. Carla’s advanced capabilities include the creation of virtual road networks, the design of complex traffic scenarios, pre-simulation rehearsals, and the collection of vehicle trajectory data for subsequent analysis. Throughout the experiment, participants navigated a pre-determined standardized route displayed on the simulator’s screens. The software’s ability to produce consistent, repeatable conditions ensured uniformity across trials, thereby bolstering the reliability and validity of the study’s findings.
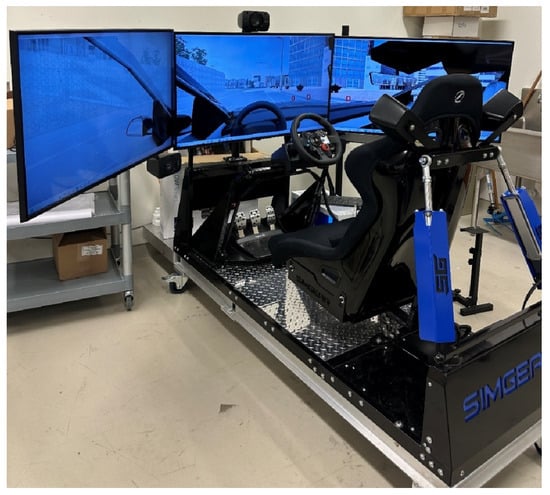
Figure 3.
SimGear Driving Simulator.
2.3. Participants
In total, 24 participants (12 males and 12 females) were recruited for a driving simulator experiment. Inclusion criteria required that participants hold a valid Ontario driver’s license (G1/G2/G), have at least one year of driving experience, and be free from any musculoskeletal or heart-related disorders that could affect their ability to participate or impact their comfort ratings. Conversely, individuals with any such disorders or insufficient driving experience were excluded from the study. The sample size of 24 was determined based on prior literature and recommendations from Human Factors Guidance—which suggests a minimum of 15 test participants per intended user group—to ensure robust testing and sufficient statistical power [20,21,22,23]. Given the within-participant design of our study, 24 participants provide a balanced representation and are adequate to achieve reliable results. The mean (SD) age, body mass, and height of the participants are presented in Table 2. The study received ethical approval from the University of Windsor Research Ethics Board (REB #43635).
Table 2.
Participants’ Demographics.
2.4. Experimental Setup
The experimental protocol consisted of two 60 min trials for each participant, one with the AFMF system activated and another with it deactivated. To mitigate order effects, the assignment of AFMF conditions was randomized across participants. During each trial, participants were instructed to drive within a simulated environment (Figure 4), following a standardized route with on-screen instructions to ensure consistency across trials. A 20 min rest period was incorporated between trials, after which participants were asked to repeat the driving protocol under the alternate AFMF condition.

Figure 4.
(a) Two Participants Seated in the Driver’s Seat of the Simulator; (b) the Driving Route is Displayed on the Simulator Screen along with Directions.
Throughout the trials, participants rated their perceived comfort at 10 min intervals using a 5-point Likert scale (Table 3), thereby providing real-time feedback on their comfort levels (Table 3). Collecting comfort ratings in real time minimizes recall bias by capturing immediate perceptions rather than relying on retrospective assessments. Moreover, using a consistent and simple Likert scale across all participants ensures uniformity and reduces variability associated with subjective judgment. The repeated measures design further controls for individual differences in baseline comfort levels, enhancing the reliability of the subjective data.
Table 3.
Subjective Comfort Ratings.
2.5. ICM Measurement
Video recordings were used throughout the trials to capture seat-related fidgeting and movements, which served as indicators of ICM [18]. ICM measurements are based on the premise that lower levels of comfort prompt more frequent movements, particularly after 30 to 40 min of continuous seating [17,24,25]. ICM was measured directly by trained researchers through careful, manual observation of the video recordings. A dual-camera setup was employed for comprehensive, unobtrusive observation: a Canon Vixia HF R800 HD camera was positioned at a 45-degree angle, approximately 200 cm (6.56 feet) away from the participant, to capture a full-body view, and a 4K webcam was mounted above the simulator screen to record a frontal view. This dual-camera configuration facilitated a thorough evaluation of participants’ movement patterns without restricting their natural postural adjustments.
The recorded ICMs were classified into three categories based on established literature [18]:
- Type 1: Movements of the limbs not directly related to driving tasks (e.g., arm or leg movements, excluding routine hand positioning on the steering wheel or minor movements such as scratching);
- Type 2: Movements of the torso that are not required for driving (e.g., shifting or twisting in the seat);
- Type 3: Full-body adjustments unrelated to driving tasks.
The time and type of each ICM were meticulously documented from the video records to assess how the AFMF system influenced posture adjustments and comfort levels during simulated driving sessions.
2.6. Statistical Analysis
Statistical analyses were performed using R 4.4.2. As the data did not meet the assumption of normality, as assessed by the Shapiro–Wilk test (p < 0.05), non-parametric methods were applied. For subjective comfort rating, the independent variables were driver seat type and time, and the dependent variable was the subjective comfort rating; for ICM, the independent variables were driver seat type, movement type, and time, and the dependent variable was ICM. Specifically, an Aligned Rank Transform (ART) ANOVA was used to analyze the data; this approach not only handles non-normal distributions but also accommodates mixed-effects models. Pairwise comparisons were then conducted to probe specific contrasts, providing a comprehensive understanding of the observed effects. All statistical tests were conducted with a significance level set at 0.05. This framework provided a robust assessment of the impact of the AFMF system on driver comfort and ICM patterns.
3. Results
3.1. Subjective Comfort Rating Results
The result of the Shapiro–Wilk normality test indicated a significant deviation from normality in the comfort data (p < 0.05). Following this, an ART ANOVA was conducted, which revealed only significant main effect of the driver seat condition on comfort ratings (p < 0.001) with a large effect size ( = 0.32). As shown in Figure 5, participants in the AFMF-equipped seat condition reported mean comfort scores of approximately 4.11, while those in the standard seat condition reported scores closer to 3.07. This suggests that the AFMF-equipped seat enhanced comfort compared to the standard seat condition. However, neither the main effect of time nor the interaction between the driver seat condition and time were found to be statistically significant (p > 0.05).
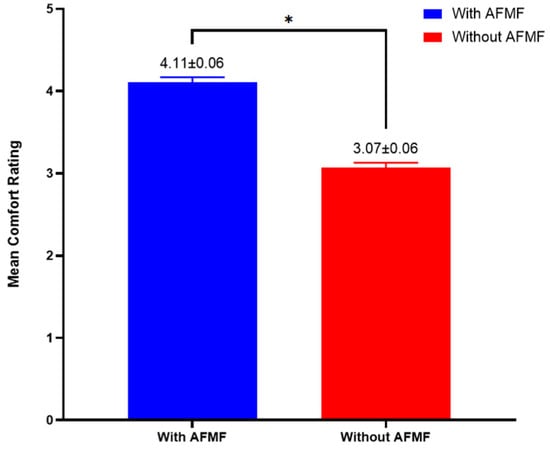
Figure 5.
Subjective Ratings of Comfort Level (* p < 0.05; Error Bars Indicate Standard Errors [SE]).
3.2. ICM Results
The means for the different motion types with the massage function, recorded at 10 min intervals, are presented in Table 4. Given that the ICM data did not conform to a normal distribution, as indicated by the Shapiro–Wilk normality test (p < 0.05), an ART ANOVA was performed.
Table 4.
Means (SD) of Motion Types with Massage at Intervals of 10 Min.
The results of the ART ANOVA (Table 5) demonstrate that all three factors—Driver Seat, Time, and Type of Movement—significantly influence ICM (p < 0.001). Among these, the Driver Seat factor had the most substantial effect, followed by the Type of Movement factor, while the influence of Time was comparatively smaller. Furthermore, significant interaction effects were observed (p < 0.001).
Table 5.
Results of ANOVA of Movement Frequencies (* p-value < 0.05).
Figure 6 illustrates the interaction between Driver Seat Condition and Movement Type with respect to movement frequencies. Participants in the AFMF condition consistently exhibited lower movement frequencies across all movement types compared to those in the standard seat condition.
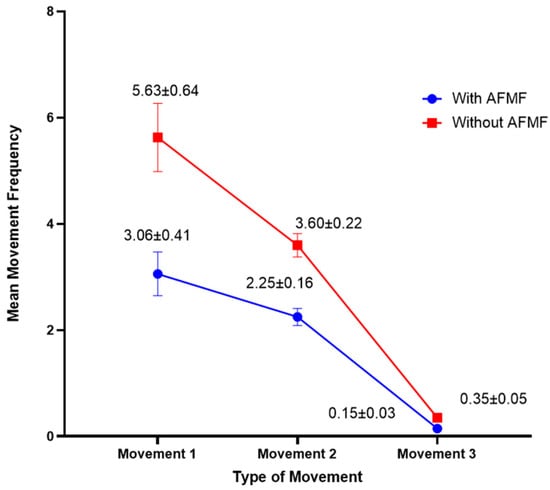
Figure 6.
Interaction Between Driver Seat Condition and Movement Type on Movement Frequencies (Error Bars Indicate Standard Errors (Mean [SE])).
The interaction between Time and Movement Type (Figure 7) demonstrates a general increase in movement frequencies as the trials progressed. Type 1 movements showed the most pronounced rise, while Type 2 movements exhibited a more moderate increase. In contrast, Type 3 movements remained largely stable, with only minimal variation over time. Pairwise comparisons were conducted at each time interval to determine whether the differences in mean movement frequency between Movement Types were statistically significant. At all time intervals, the results indicated significant differences between Type 1 and Type 3 (p < 0.001) and between Type 2 and Type 3 (p < 0.001). However, no statistically significant differences were found between Type 1 and Type 2 (p > 0.05) at any of the time intervals.
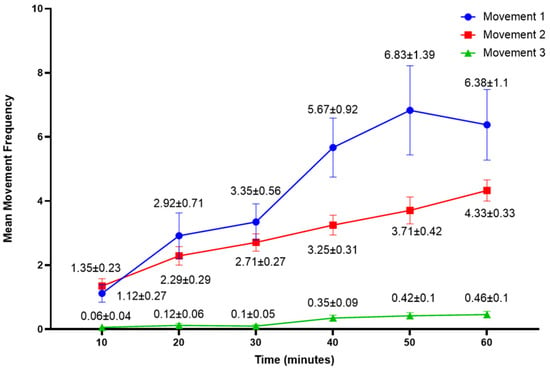
Figure 7.
Interaction Plot of Movement Frequency by Time Interval and Movement Type (Error Bars Indicate Standard Errors (Mean [SE])).
The interaction between Time and Driver Seat Condition (Figure 8) reveals a general increase in movement frequencies as time progressed. The seat without the AFMF system showed the most notable rise in movement frequencies, while the AFMF-equipped seat exhibited a more gradual increase, with consistently lower movement frequencies throughout all time intervals. Pairwise comparisons were conducted at each time interval to determine whether the differences in mean movement frequency between the driver seat conditions were statistically significant. The results revealed significant differences at 30 min (p < 0.001), 40 min (p < 0.001), and 60 min (p < 0.001). However, no statistically significant differences were found at the time intervals 10, 20, and 50 min (p > 0.05).
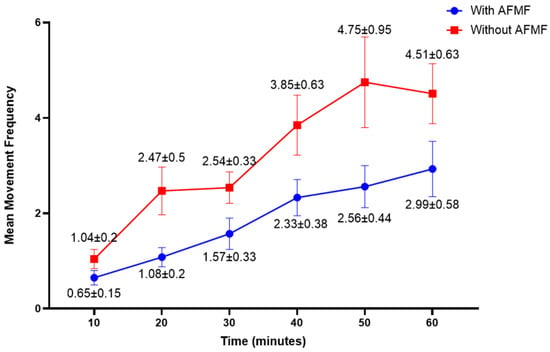
Figure 8.
Interaction between Time and Driver Seat Condition on Movement Frequencies (Error Bars Indicate Standard Errors [SE]).
4. Discussion
The present study illustrates that the integration of the AFMF system into the driver’s seat substantially elevates self-reported comfort and diminishes compensatory movements during extended driving sessions. By combining subjective comfort assessments with objective measures of ICMs, our investigation offers an evaluation of the AFMF system’s effectiveness, thereby providing insights into enhancing driver safety and overall well-being in practical settings.
Although the collection of subjective comfort ratings meant that participants were aware of the seat condition, several methodological strategies were employed to minimize bias. Specifically, each participant experienced both conditions (AFMF activated and deactivated) in a randomized, counterbalanced design, which mitigated order effects and individual differences, ensuring that any bias was uniformly distributed. Moreover, all participants received standardized, neutral instructions that refrained from highlighting an expected superiority of one condition, thereby reducing the influence of demand characteristics. In addition to these subjective ratings, objective measures in the form of ICMs were recorded, offering an unbiased complement to the self-reported data.
The ART ANOVA analysis of comfort ratings indicated a statistically significant effect on the driver seat condition, with the AFMF-equipped seat demonstrating a clear advantage over the standard seating configuration in terms of comfort. The AFMF-equipped seat, which integrates dynamic massage patterns, significantly alleviates fatigue compared to a standard seat, supporting the hypothesis that such systems can enhance comfort during extended driving sessions. No significant effects were observed for time or the interaction between seat condition and time, suggesting that the AFMF system’s influence on comfort is sustained throughout the trial, independent of the duration of the drive.
The analysis of ICMs offers further insight into the mechanisms by which the AFMF system improves comfort. The ART ANOVA (Table 5) demonstrated that the driver seat condition, time, and movement type all significantly influenced ICM, with the seat condition having the most substantial effect. This finding suggests that the AFMF system reduces the need for compensatory movements that typically arise from prolonged sitting. Previous research has also shown that reducing comfort is frequently associated with an increase in ICM, and the AFMF system’s ability to reduce these movements underscores its potential to alleviate ICM [15,16,17,18]. In addition, the AFMF system’s ability to reduce these movements, highlights its potential to alleviate ICM.
The interaction plot (Figure 6) illustrates that participants in the AFMF condition demonstrated lower mean movement frequencies across all movement types in comparison to those in the standard seat condition. This suggests that the AFMF system may effectively mitigate fatigue, thereby reducing the need for compensatory movements. The AFMF system appears to promote a more comfortable sitting posture over extended periods, potentially alleviating some of the fatigue that typically leads to frequent shifts and fidgeting.
When analyzing the interaction between time and movement type (Figure 7), it became evident that Type 1 and Type 2 movements exhibited the most substantial increase over time. This suggests that as fatigue escalated, participants compensated by adjusting their limbs and torso. The pairwise comparisons suggest that Type 1 and Type 2 movements were more frequently engaged than Type 3. However, the absence of significant differences between Type 1 and Type 2 movements indicates that these movement types may serve similar functional roles in responding to fatigue, with their frequency not differing significantly over time.
The significant interaction effects between driver seat condition and time (Figure 8) highlight the varying efficacy of the AFMF system throughout the experiment. The AFMF condition consistently exhibited lower movement frequencies across all time intervals, highlighting its ability to sustain comfort over the duration of the drive. In contrast, participants in the standard seat condition displayed a marked increase in movement frequency as time progressed, indicating that participants in the standard seat experienced greater fatigue, which led to increased non-driving-related movements over time. The pairwise comparisons revealed significant differences between the two-seat conditions at 30 min, 40 min, and 60 min (p < 0.001), highlighting that the AFMF system had a notable impact on movement frequencies as the duration of the trial increased. However, no significant differences were observed at the earlier time intervals (10 and 20 min), suggesting that the effects of the AFMF system on movement frequency may become more evident after prolonged sitting. The lack of significant differences at the 50 min time interval shows that, while the AFMF system may reduce movement frequency, the differences might become more noticeable at the later 60 min interval, where the cumulative effect is stronger.
These results are important in the context of driver health, safety, and well-being, particularly for long-duration driving. By reducing fatigue-related movements and maintaining comfort, the AFMF system has the potential to help drivers stay focused on the road, thereby reducing fatigue and the associated risk of accidents. The reduction in ICMs also suggests that the AFMF system could play a role in preventing musculoskeletal disorders, which are prevalent among drivers who spend long periods sitting in suboptimal positions [3,4,5,6]. The AFMF system’s effectiveness in reducing fatigue and promoting more natural postural adjustments could serve as a preventive measure against such health risks.
While our findings underscore the potential benefits of the AFMF system, several limitations warrant acknowledgment. First, although real-world driving scenarios may typically extend beyond 3–4 h, our experimental protocol was limited to two 60 min sessions. This duration was deliberately selected to maintain a controlled environment and ensure experimental feasibility for an initial evaluation. Future studies should extend the trial duration to more accurately replicate prolonged driving conditions. Real-world scenarios introduce variables such as road conditions, vehicle vibrations, and traffic-related stress, all of which could influence both driver comfort and the AFMF system’s efficacy. Future studies should incorporate these dynamic factors by evaluating the system in naturalistic driving environments to provide a more accurate understanding of its performance under real-world conditions. Additionally, this study primarily examined general participants rather than the high-risk population of professional drivers, who may experience different fatigue patterns due to longer hours and higher frequencies of extended sitting. Investigating the AFMF system’s effects on truck drivers or other professional drivers could yield insights into its efficacy for the populations most affected by prolonged sitting. Furthermore, the current analysis did not examine participant anthropometrics (e.g., height, body mass) as potential moderators of comfort ratings or ICM frequency. Future research should explore whether such individual characteristics modulate the effects of AFMF interventions, which could ultimately support the development of personalized seating solutions tailored to diverse user profiles. Lastly, other solutions, such as active seating systems and dynamic driving aids, are designed to continuously adapt to road and driving conditions, promoting natural postural adjustments and reducing strain. Future research should explore how AFMF performs in comparison to these solutions and investigate the potential benefits of using AFMF in combination with them. This integrated approach could provide insights into the most effective strategies for comprehensive fatigue reduction, supporting both immediate and long-term driver comfort and well-being.
5. Conclusions
This study demonstrates that the AFMF system significantly enhances driver comfort and reduces fatigue-driven movements, supporting its effectiveness as an ergonomic intervention for prolonged sitting. Participants using the AFMF-equipped seat consistently reported higher comfort levels and exhibited fewer ICM. These results suggest that the AFMF system can effectively alleviate the accumulation of fatigue over time, contributing to a more stable and relaxed sitting posture. The AFMF system’s impact on reducing ICM and promoting sustained comfort may benefit drivers who face extended sitting durations, potentially reducing fatigue and improving overall safety by enabling drivers to maintain focus. While these findings provide strong evidence for the AFMF system’s effectiveness, future research in real-world driving conditions and with professional driver populations is essential to further validate its benefits.
Author Contributions
Conceptualization, D.M.A., S.C., K.L.A. and E.K.; methodology, D.E., A.B. and I.M.; software, S.C. and K.L.A.; validation, D.E., A.B. and I.M.; formal analysis, A.B. and I.M.; investigation, D.E., A.B. and I.M.; resources, S.C. and K.L.A.; writing—original draft preparation, A.B.; writing—review and editing, D.M.A. and E.K.; supervision, D.M.A. and E.K.; project administration, K.L.A.; funding acquisition, D.M.A. and E.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by a Mitacs Accelerate grant, number IT39538.
Institutional Review Board Statement
The animal study protocol was approved by the University of Windsor Research Ethics Board (REB Number: 43635 and 24 June 2024).
Informed Consent Statement
Informed consent was obtained from all participants involved in the study.
Data Availability Statement
Data are unavailable due to privacy or ethical restrictions.
Acknowledgments
The authors would like to express their sincere gratitude to Leggett & Platt Automotive for providing essential resources, equipment, and technical support throughout this study. Special thanks are extended to the study participants for their time and cooperation.
Conflicts of Interest
Authors Shane Cole and Katherine L. Arthurs were employed by the company Leggett & Platt Canada Co. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| AFMF | Anti-Fatigue Massage Function |
| ICMs | In-Chair Movements |
| MSDs | Musculoskeletal Disorders |
| PWM | Pulse Width Modulation |
| BM | Balanced Mix |
| ART | Aligned Rank Transform |
References
- Cășeriu, B.; Blaga, P. Automotive Comfort: State of the Art and Challenges. In Proceedings of the 16th International Conference Interdisciplinarity in Engineering, Târgu Mureș, Romania, 6–7 October 2022; Springer: Cham, Switzerland, 2023; pp. 375–387. [Google Scholar]
- Martin, S. Drowsy Driving Statistics and Facts. 2024. Available online: https://www.bankrate.com/insurance/car/drowsy-driving-statistics/ (accessed on 20 October 2024).
- Mozafari, A.; Vahedian, M.; Mohebi, S.; Najafi, M. Work-Related Musculoskeletal Disorders in Truck Drivers and Official Workers. Acta Medica Iran. 2015, 53, 432–438. [Google Scholar]
- Porter, J.M.; Gyi, D.E. The Prevalence of Musculoskeletal Troubles among Car Drivers. Occup. Med. 2002, 52, 4–12. [Google Scholar]
- Rezaei, E.; Shahmahmoudi, F.; Makki, F.; Salehinejad, F.; Marzban, H.; Zangiabadi, Z. Musculoskeletal Disorders among Taxi Drivers: A Systematic Review and Meta-Analysis. BMC Musculoskelet. Disord. 2024, 25, 663. [Google Scholar] [CrossRef] [PubMed]
- Tahernejad, S.; Makki, F.; Bameri, A.; Zangiabadi, Z.; Rezaei, E.; Marzban, H. Musculoskeletal Disorders among Truck Drivers: A Systematic Review and Meta-Analysis. BMC Public Health 2024, 24, 3146. [Google Scholar] [CrossRef]
- Asli, K. Risk Factors Associated with Musculoskeletal Disorders Among Professional Drivers in Asian Countries: A Systematic Review. J. Sains Kesihat. Malays. 2023, 21, 143–155. [Google Scholar]
- De Carvalho, D.E.; Callaghan, J.P. Influence of Automobile Seat Lumbar Support Prominence on Spine and Pelvic Postures: A Radiological Investigation. Appl. Ergon. 2012, 43, 876–882. [Google Scholar] [CrossRef]
- Durkin, J.L.; Harvey, A.; Hughson, R.L.; Callaghan, J.P. The Effects of Lumbar Massage on Muscle Fatigue, Muscle Oxygenation, Low Back Discomfort, and Driver Performance during Prolonged Driving. Ergonomics 2006, 49, 28–44. [Google Scholar] [CrossRef]
- Jhinkwan, A.; Singh, J. Design Specifications and Ergonomic Evaluation of Car Seat (A Review). Int. J. Eng. Res. Technol. 2014, 3, 611–613. [Google Scholar]
- Lee, S.; Kim, M.; Jung, H.; Kwon, D.; Choi, S.; You, H. Effects of a Motion Seat System on Driver’s Passive Task-Related Fatigue: An On-Road Driving Study. Sensors 2020, 20, 2688. [Google Scholar] [CrossRef]
- Schneider, L.; Frings, K.; Rothe, S.; Schrauf, M.; Jaitner, T. Effects of a Seat-Integrated Mobilization System during Passive Driver Fatigue. Accid. Anal. Prev. 2021, 150, 105883. [Google Scholar] [CrossRef]
- Tilwani, P. Ergonomics Modelling and Evaluation of Automobile Seat Comfort. Manipal J. Sci. Technol. 2020, 5, 3. [Google Scholar]
- Franz, M.; Zenk, R.; Vink, P.; Hallbeck, S. The Effect of a Lightweight Massage System in a Car Seat on Comfort and Electromyogram. J. Manip. Physiol. Ther. 2011, 34, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Cascioli, V.; Liu, Z.; Heusch, A.; McCarthy, P. A Methodology Using In-Chair Movements as an Objective Measure of Discomfort for the Purpose of Statistically Distinguishing between Similar Seat Surfaces. Appl. Ergon. 2016, 54, 100–109. [Google Scholar] [CrossRef] [PubMed]
- Fenety, P.A.; Putnam, C.; Walker, J.M. In-Chair Movement: Validity, Reliability and Implications for Measuring Sitting Discomfort. Appl. Ergon. 2000, 31, 383–393. [Google Scholar] [CrossRef] [PubMed]
- Jackson, C.; Emck, A.J.; Hunston, M.J.; Jarvis, P.C. Pressure Measurements and Comfort of Foam Safety Cushions for Confined Seating. Aviat. Space Environ. Med. 2009, 80, 565–569. [Google Scholar] [CrossRef]
- Sammonds, G.M.; Fray, M.; Mansfield, N.J. Effect of Long Term Driving on Driver Discomfort and Its Relationship with Seat Fidgets and Movements (SFMs). Appl. Ergon. 2017, 58, 119–127. [Google Scholar] [CrossRef]
- Why You Only Need to Test with 5 Users. Available online: https://www.nngroup.com/articles/why-you-only-need-to-test-with-5-users/ (accessed on 19 April 2025).
- Virzi, R.A. Refining the Test Phase of Usability Evaluation: How Many Subjects Is Enough? Hum Factors 1992, 34, 457–468. [Google Scholar] [CrossRef]
- Faulkner, L. Beyond the Five-User Assumption: Benefits of Increased Sample Sizes in Usability Testing. Behav. Res. Methods Instrum. Comput. 2003, 35, 379–383. [Google Scholar] [CrossRef]
- Oliveira, A.S.; Pirscoveanu, C.I. Implications of Sample Size and Acquired Number of Steps to Investigate Running Biomechanics. Sci. Rep. 2021, 11, 3083. [Google Scholar] [CrossRef]
- VanVoorhis, C.W.; Morgan, B.L. Understanding Power and Rules of Thumb for Determining Sample Sizes. Tutor. Quant. Methods Psychol. 2007, 3, 43–50. [Google Scholar] [CrossRef]
- Bendix, T.; Winkel, J.; Jessen, F. Comparison of Office Chairs with Fixed Forwards or Backwards Inclining, or Tiltable Seats. Eur. J. Appl. Physiol. Occup. Physiol. 1985, 54, 378–385. [Google Scholar] [CrossRef] [PubMed]
- Jensen, C.V.; Bendix, T. Spontaneous Movements with Various Seated-Workplace Adjustments. Clin. Biomech. 1992, 7, 87–90. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).