
The Neurophysiological Effects of Virtual Reality Application and Perspectives of Using for Multitasking Training in Cardiac Surgery Patients: Pilot Study

Abstract
Featured Application
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Design and Development of the Original Multitasking CT VR System
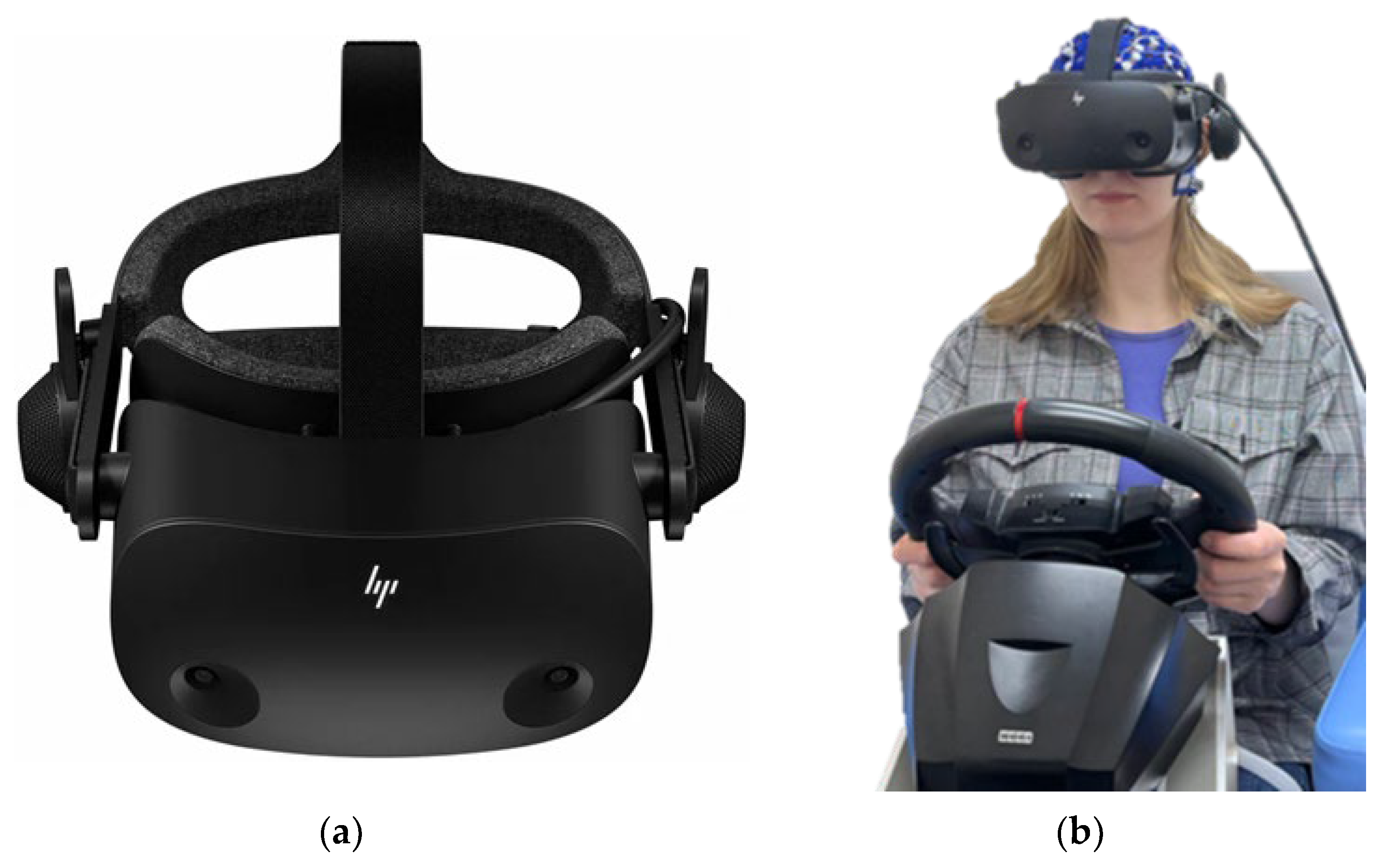
2.2.1. Hardware Components
2.2.2. Software Components
2.3. Neurophysiological Assessment
2.4. Statistical Analysis
3. Results
3.1. Study 1 (Practically Healthy Subjects)
3.1.1. Cognitive Test Indicators
3.1.2. EEG Data
3.1.3. SUS and SMEQ Scales Data
3.2. Study 2 (Cardiac Surgery Patients)
4. Discussion
Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Appendix B
| No. | Item | Amount |
| 1 | 27” display MSI G27C4 E2 | 1 |
| 2 | Hori Racing Wheel Apex | 1 |
| 3 | Speakers DEXP R350 | 1 |
| 4 | VR Cover для HP Reverb G2 | 2 |
| 5 | VR headmounted display HP Reverb G2 | 1 |
| 6 | DDR5 ADATA XPG Lancer [AX5U5200C3816G-DCLABK] 32 ГБ | 1 |
| 7 | DEEPCOOL CH560 DIGITAL [R-CH560-BKAPE4D-G-1] system unit | 1 |
| 8 | MSI GeForce RTX 4070 VENTUS 3X E 12G OC graphics card | 1 |
| 9 | MSI MAG Z790 TOMAHAWK WIFI motherboard | 1 |
| 10 | Intel Core i7-13700F chip | 1 |
| 11 | 1000GB SSD M.2 Samsung 980 PRO drive | 1 |
| 12 | OS Microsoft Windows 11 pro, 64 bit | 1 |
References
- Pan, C.W.; Wang, X.; Ma, Q.; Sun, H.P.; Xu, Y.; Wang, P. Cognitive dysfunction and health-related quality of life among older Chinese. Sci. Rep. 2015, 5, 17301. [Google Scholar] [CrossRef] [PubMed]
- Pavel, A.; Paun, R.; Matei, V.; Rosca, A.; Tudose, C. Quality of life in people with subjective cognitive decline. Alpha Psychiatry 2023, 24, 60–64. [Google Scholar] [CrossRef] [PubMed]
- Jongsiriyanyong, S.; Limpawattana, P. Mild cognitive impairment in clinical practice: A review article. Am. J. Alzheimers Dis. Dement. 2018, 33, 500–507. [Google Scholar] [CrossRef] [PubMed]
- Tarasova, I.V.; Trubnikova, O.A.; Barbarash, O.L. EEG and clinical factors associated with mild cognitive impairment in coronary artery disease patients. Dement. Geriatr. Cogn. Disord. 2018, 46, 275–284. [Google Scholar] [CrossRef]
- Lu, Y.; Zhu, Y.; Ma, Y.; Li, C.; Hua, R.; Zhong, B.; Wang, H.; Xie, W. Association of subclinical atherosclerosis and cognitive decline: A community-based cross-sectional study. BMJ Open 2022, 12, e059024. [Google Scholar] [CrossRef]
- Bangen, K.J.; Werhane, M.L.; Weigand, A.J.; Edmonds, E.C.; Delano-Wood, L.; Thomas, K.R.; Nation, D.A.; Evangelista, N.D.; Clark, A.L.; Liu, T.T.; et al. Reduced regional cerebral blood flow relates to poorer cognition in older adults with type 2 diabetes. Front. Aging Neurosci. 2018, 10, 270. [Google Scholar] [CrossRef]
- Rundek, T.; Tolea, M.; Ariko, T.; Fagerli, E.A.; Camargo, C.J. Vascular cognitive impairment (VCI). Neurotherapeutics 2022, 19, 68–88. [Google Scholar] [CrossRef]
- Chudiak, A.; Uchmanowicz, I.; Mazur, G. Relation between cognitive impairment and treatment adherence in elderly hypertensive patients. Clin. Interv. Aging 2018, 13, 1409–1418. [Google Scholar] [CrossRef]
- Indja, B.; Seco, M.; Seamark, R.; Kaplan, J.; Bannon, P.G.; Grieve, S.M.; Vallely, M.P. Neurocognitive and psychiatric issues post cardiac surgery. Heart Lung Circ. 2017, 26, 779–785. [Google Scholar] [CrossRef]
- Tarasova, I.V.; Trubnikova, O.A.; Syrova, I.D.; Barbarash, O.L. Long-term neurophysiological outcomes in patients undergoing coronary artery bypass grafting. Braz. J. Cardiovasc. Surg. 2021, 36, 629–638. [Google Scholar] [CrossRef]
- Weimar, C.; Bilbilis, K.; Rekowski, J.; Holst, T.; Beyersdorf, F.; Breuer, M.; Dahm, M.; Diegeler, A.; Kowalski, A.; Martens, S.; et al. Safety of simultaneous coronary artery bypass grafting and carotid endarterectomy versus isolated coronary artery bypass grafting: A randomized clinical trial. Stroke 2017, 48, 2769–2775. [Google Scholar] [CrossRef] [PubMed]
- Suraarunsumrit, P.; Pathonsmith, C.; Srinonprasert, V.; Sangarunakul, N.; Jiraphorncharas, C.; Siriussawakul, A. Postoperative cognitive dysfunction in older surgical patients associated with increased healthcare utilization: A prospective study from an upper-middle-income country. BMC Geriatr. 2022, 22, 213. [Google Scholar] [CrossRef] [PubMed]
- Lin, X.; Chen, Y.; Zhang, P.; Chen, G.; Zhou, Y.; Yu, X. The potential mechanism of postoperative cognitive dysfunction in older people. Exp. Gerontol. 2020, 130, 110791. [Google Scholar] [CrossRef]
- Phirom, K.; Kamnardsiri, T.; Sungkarat, S. Beneficial effects of interactive physical-cognitive game-based training on fall risk and cognitive performance of older adults. Int. J. Environ. Res. Public. Health 2020, 17, 6079. [Google Scholar] [CrossRef]
- Gavelin, H.M.; Dong, C.; Minkov, R.; Bahar-Fuchs, A.; Ellis, K.A.; Lautenschlager, N.T.; Mellow, M.L.; Wade, A.T.; Smith, A.E.; Finke, C.; et al. Combined physical and cognitive training for older adults with and without cognitive impairment: A systematic review and network meta-analysis of randomized controlled trials. Ageing Res. Rev. 2021, 66, 101232. [Google Scholar] [CrossRef]
- Montero-Odasso, M.; Zou, G.; Speechley, M.; Almeida, Q.J.; Liu-Ambrose, T.; Middleton, L.E.; Camicioli, R.; Bray, N.W.; Li, K.Z.H.; Fraser, S.; et al. Effects of exercise alone or combined with cognitive training and vitamin d supplementation to improve cognition in adults with mild cognitive impairment: A randomized clinical trial. JAMA Netw. Open. 2023, 6, e2324465. [Google Scholar] [CrossRef]
- Lin, Y.P.; Lin, I.I.; Chiou, W.D.; Chang, H.C.; Chen, R.S.; Lu, C.S.; Chang, Y.J. The executive-function-related cognitive-motor dual task walking performance and task prioritizing effect on people with Parkinson’s disease. Healthcare 2023, 11, 567. [Google Scholar] [CrossRef]
- Syrova, I.D.; Tarasova, I.V.; Trubnikova, O.A.; Kupriyanova, D.S.; Sosnina, A.S.; Temnikova, T.B.; Barbarash, O.L. A multitask approach to prevention of the cognitive decline after coronary artery bypass grafting: A prospective randomized controlled study. J. Xiangya Med. 2023, 8, 2. [Google Scholar] [CrossRef]
- Hassandra, M.; Galanis, E.; Hatzigeorgiadis, A.; Goudas, M.; Mouzakidis, C.; Karathanasi, E.M.; Petridou, N.; Tsolaki, M.; Zikas, P.; Evangelou, G.; et al. A virtual reality app for physical and cognitive training of older people with mild cognitive impairment: Mixed methods feasibility study. JMIR Serious Games 2021, 9, e24170. [Google Scholar] [CrossRef]
- Bosch-Barceló, P.; Climent-Sanz, C.; Martínez-Navarro, O.; Masbernat-Almenara, M.; Pakarinen, A.; Ghosh, P.K.; Fernández-Lago, H. A treadmill training program in a gamified virtual reality environment combined with transcranial direct current stimulation in Parkinson’s Disease: Study protocol for a randomized controlled trial. PLoS ONE 2024, 19, e0307304. [Google Scholar] [CrossRef]
- Kang, J.M.; Kim, N.; Lee, S.Y.; Woo, S.K.; Park, G.; Yeon, B.K.; Park, J.W.; Youn, J.H.; Ryu, S.H.; Lee, J.Y.; et al. Effect of cognitive training in fully immersive virtual reality on visuospatial function and frontal-occipital functional connectivity in predementia: Randomized controlled trial. J. Med. Internet Res. 2021, 23, e24526. [Google Scholar] [CrossRef] [PubMed]
- Son, C.; Park, J.H. Ecological effects of VR-based cognitive training on ADL and IADL in MCI and AD patients: A systematic review and meta-analysis. Int. J. Environ. Res. Public. Health 2022, 19, 15875. [Google Scholar] [CrossRef] [PubMed]
- Baldimtsi, E.; Mouzakidis, C.; Karathanasi, E.M.; Verykouki, E.; Hassandra, M.; Galanis, E.; Hatzigeorgiadis, A.; Goudas, M.; Zikas, P.; Evangelou, G.; et al. Effects of virtual reality physical and cognitive training intervention on cognitive abilities of elders with mild cognitive impairment. J. Alzheimers Dis. Rep. 2023, 7, 1475–1490. [Google Scholar] [CrossRef]
- Feng, H.; Li, C.; Liu, J.; Wang, L.; Ma, J.; Li, G.; Gan, L.; Shang, X.; Wu, Z. Virtual reality rehabilitation versus conventional physical therapy for improving balance and gait in Parkinson’s disease patients: A randomized controlled trial. Med. Sci. Monit. 2019, 25, 4186–4192. [Google Scholar] [CrossRef]
- Saeedi, S.; Ghazisaeedi, M.; Rezayi, S. Applying game-based approaches for physical rehabilitation of poststroke patients: A systematic review. J. Healthcare Eng. 2021, 2021, 9928509. [Google Scholar] [CrossRef]
- Saredakis, D.; Szpak, A.; Birckhead, B.; Keage, H.A.D.; Rizzo, A.; Loetscher, T. Factors associated with virtual reality sickness in head-mounted displays: A systematic review and meta-analysis. Front. Hum. Neurosci. 2020, 14, 96. [Google Scholar] [CrossRef]
- Kooijman, L.; Berti, S.; Asadi, H.; Nahavandi, S.; Keshavarz, B. Measuring vection: A review and critical evaluation of different methods for quantifying illusory self-motion. Behav. Res. Methods 2024, 56, 2292–2310. [Google Scholar] [CrossRef]
- Luu, W.; Zangerl, B.; Kalloniatis, M.; Kim, J. Effects of stereopsis on vection, presence and cybersickness in head-mounted display (HMD) virtual reality. Sci. Rep. 2021, 11, 12373. [Google Scholar] [CrossRef]
- Khoo, S.Y.; Lai, W.H.; On, S.H.; On, Y.Y.; Adam, B.M.; Law, W.C.; Ng, B.H.S.; Fong, A.Y.Y.; Anselm, S.T. Resting-state electroencephalography (EEG) microstates of healthy individuals following mild sleep deprivation. Sci. Rep. 2024, 14, 16820. [Google Scholar] [CrossRef]
- Shivdat, S.; Zhan, T.; De Palma, A.; Zheng, W.L.; Krishnamurthy, P.; Paneerselvam, E.; Snider, S.; Bevers, M.; O’Reilly, U.M.; Lee, J.W.; et al. Early burst suppression similarity association with structural brain injury severity on MRI after cardiac arrest. Neurocrit. Care 2024. online ahead of print. [Google Scholar] [CrossRef]
- Gangemi, A.; De Luca, R.; Fabio, R.A.; Lauria, P.; Rifici, C.; Pollicino, P.; Marra, A.; Olivo, A.; Quartarone, A.; Calabrò, R.S. Effects of virtual reality cognitive training on neuroplasticity: A quasi-randomized clinical trial in patients with stroke. Biomedicines 2023, 11, 3225. [Google Scholar] [CrossRef]
- Calabrò, R.S.; Naro, A.; Russo, M.; Leo, A.; De Luca, R.; Balletta, T.; Buda, A.; La Rosa, G.; Bramanti, A.; Bramanti, P. The role of virtual reality in improving motor performance as revealed by EEG: A randomized clinical trial. J. Neuroeng. Rehabil. 2017, 14, 53. [Google Scholar] [CrossRef] [PubMed]
- Vojtenko, V.P. Health of Healthy People: Introduction to Sanology; Health: Kyiv, Ukraine, 1991; 245p. [Google Scholar]
- Papandrea, M.; Peternier, A.; Frei, D.; La Porta, N.; Gelsomini, M.; Allegri, D.; Leidi, T. V-Cockpit: A Platform for the design, testing, and validation of car infotainment systems through virtual reality. Appl. Sci. 2024, 14, 8160. [Google Scholar] [CrossRef]
- Guyer, G.; Mueller, S.; Wyss, Y.; Bertholet, J.; Schmid, R.; Stampanoni, M.F.M.; Manser, P.; Fix, M.K. Technical note: A collision prediction tool using Blender. J. Appl. Clin. Med. Phys. 2023, 24, e14165. [Google Scholar] [CrossRef]
- Trubnikova, O.A.; Tarasova, I.V.; Moskin, E.G.; Kupriyanova, D.S.; Argunova, Y.A.; Pomeshkina, S.A.; Gruzdeva, O.V.; Barbarash, O.L. Beneficial effects of a short course of physical prehabilitation on neurophysiological functioning and neurovascular biomarkers in patients undergoing coronary artery bypass grafting. Front. Aging Neurosci. 2021, 13, 699259. [Google Scholar] [CrossRef]
- Tarasova, I.; Trubnikova, O.; Kupriyanova, D.; Kukhareva, I.; Syrova, I.; Sosnina, A.; Maleva, O.; Barbarash, O. Effect of carotid stenosis severity on patterns of brain activity in patients after cardiac surgery. Appl. Sci. 2023, 13, 20. [Google Scholar] [CrossRef]
- Jurcak, V.; Tsuzuki, D.; Dan, I. 10/20, 10/10, and 10/5 systems revisited: Their validity as relative head-surface-based positioning systems. NeuroImage 2007, 34, 1600–1611. [Google Scholar] [CrossRef]
- Lloréns, R.; Noé, E.; Colomer, C.; Alcañiz, M. Effectiveness, usability, and cost-benefit of a virtual reality-based telerehabilitation program for balance recovery after stroke: A randomized controlled trial. Arch. Phys. Med. Rehabil. 2015, 96, 418–425.e2. [Google Scholar] [CrossRef]
- Metzemaekers, J.; Haazebroek, P.; Smeets, M.J.G.H.; English, J.; Blikkendaal, M.D.; Twijnstra, A.R.H.; Adamson, G.D.; Keckstein, J.; Jansen, F.W. EQUSUM: Endometriosis QUality and grading instrument for SUrgical performance: Proof of concept study for automatic digital registration and classification scoring for r-ASRM, EFI and Enzian. Hum. Reprod. Open. 2020, 2020, hoaa053. [Google Scholar] [CrossRef]
- Juliano, J.M.; Schweighofer, N.; Liew, S.L. Increased cognitive load in immersive virtual reality during visuomotor adaptation is associated with decreased long-term retention and context transfer. J. Neuroeng. Rehabil. 2022, 19, 106. [Google Scholar] [CrossRef]
- Jeong, S.; Kim, J.; Lee, J. The differential effects of multisensory attentional cues on task performance in VR depending on the level of cognitive load and cognitive capacity. IEEE Trans. Vis. Comput. Graph. 2024, 30, 2703–2712. [Google Scholar] [CrossRef]
- Anglin, J.M.; Sugiyama, T.; Liew, S.L. Visuomotor adaptation in head-mounted virtual reality versus conventional training. Sci. Rep. 2017, 7, 45469. [Google Scholar] [CrossRef] [PubMed]
- Babiloni, C.; Barry, R.J.; Başar, E.; Blinowska, K.J.; Cichocki, A.; Drinkenburg, W.H.; Klimesch, W.; Knight, R.T.; da Silva, F.L.; Nunez, P.; et al. International Federation of Clinical Neurophysiology (IFCN)—EG research workgroup: Recommendations on frequency and topographic analysis of resting state EEG rhythms. Part 1: Applications in clinical research studies. Clin. Neurophysiol. 2020, 131, 285–307. [Google Scholar] [CrossRef] [PubMed]
- Soltani Zangbar, H.; Ghadiri, T.; Seyedi Vafaee, M.; Ebrahimi Kalan, A.; Fallahi, S.; Ghorbani, M.; Shahabi, P. Theta oscillations through hippocampal/prefrontal pathway: Importance in cognitive performances. Brain Connect. 2020, 10, 157–169. [Google Scholar] [CrossRef]
- Sandri Heidner, G.; O’Connell, C.; Domire, Z.J.; Rider, P.; Mizelle, C.; Murray, N.P. Concussed neural signature is substantially different than fatigue neural signature in non-concussed controls. J. Mot. Behav. 2023, 55, 302–312. [Google Scholar] [CrossRef]
- Puma, S.; Matton, N.; Paubel, P.V.; Raufaste, É.; El-Yagoubi, R. Using theta and alpha band power to assess cognitive workload in multitasking environments. Int. J. Psychophysiol. 2018, 123, 111–120. [Google Scholar] [CrossRef]
- Wascher, E.; Heppner, H.; Kobald, S.O.; Arnau, S.; Getzmann, S.; Möckel, T. Age-sensitive effects of enduring work with alternating cognitive and physical load. A study applying mobile EEG in a real-life working scenario. Front. Hum. Neurosci. 2016, 9, 711. [Google Scholar] [CrossRef]
- Cacau, L.d.A.; Oliveira, G.U.; Maynard, L.G.; Araújo Filho, A.A.; Silva, W.M., Jr.; Cerqueria Neto, M.L.; Antoniolli, A.R.; Santana-Filho, V.J. The use of the virtual reality as intervention tool in the postoperative of cardiac surgery. Rev. Bras. Cir. Cardiovasc. 2013, 28, 281–289. [Google Scholar] [CrossRef]
- Rousseaux, F.; Faymonville, M.E.; Nyssen, A.S.; Dardenne, N.; Ledoux, D.; Massion, P.B.; Vanhaudenhuyse, A. Can hypnosis and virtual reality reduce anxiety, pain and fatigue among patients who undergo cardiac surgery: A randomised controlled trial. Trials 2020, 21, 330. [Google Scholar] [CrossRef]
- Gerber, S.M.; Jeitziner, M.M.; Knobel, S.E.J.; Mosimann, U.P.; Müri, R.M.; Jakob, S.M.; Nef, T. Perception and Performance on a Virtual Reality Cognitive Stimulation for Use in the Intensive Care Unit: A Non-randomized Trial in Critically Ill Patients. Front. Med. 2019, 6, 287. [Google Scholar] [CrossRef]
- Pérez Palmer, N.; Trejo Ortega, B.; Joshi, P. Cognitive Impairment in Older Adults: Epidemiology, Diagnosis, and Treatment. Psychiatr. Clin. North. Am. 2022, 45, 639–661. [Google Scholar] [CrossRef]
- Varpaei, H.A.; Farhadi, K.; Mohammadi, M.; Khafaee Pour Khamseh, A.; Mokhtari, T. Postoperative cognitive dysfunction: A concept analysis. Aging Clin. Exp. Res. 2024, 36, 133. [Google Scholar] [CrossRef] [PubMed]
- Kaleev, O.F.; Kaleva, N.G.; Yashin, D.A. QUALITY OF HUMAN HEALTH//Contemporary Problems of Science and Education. 2016. Available online: https://science-education.ru/en/article/view?id=25004 (accessed on 10 October 2024).
- Innocenti, G.M. Defining neuroplasticity. Handb. Clin. Neurol. 2022, 184, 3–18. [Google Scholar] [CrossRef] [PubMed]
- Bredy, C.; Ministeri, M.; Kempny, A.; Alonso-Gonzalez, R.; Swan, L.; Uebing, A.; Diller, G.P.; Gatzoulis, M.A.; Dimopoulos, K. New York Heart Association (NYHA) classification in adults with congenital heart disease: Relation to objective measures of exercise and outcome. Eur. Heart J. Qual. Care Clin. Outcomes 2018, 4, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Kosaraju, A.; Goyal, A.; Grigorova, Y.; Makaryus, A.N. Left Ventricular Ejection Fraction; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Al Ghorani, H.; Götzinger, F.; Böhm, M.; Mahfoud, F. Arterial hypertension—Clinical trials update 2021. Nutr. Metab. Cardiovasc. Dis. 2022, 32, 21–31. [Google Scholar] [CrossRef]
- Tinajero, M.G.; Malik, V.S. An Update on the Epidemiology of Type 2 Diabetes: A Global Perspective. Endocrinol. Metab. Clin. North. Am. 2021, 50, 337–355. [Google Scholar] [CrossRef]
- Ismail, A.; Ravipati, S.; Gonzalez-Hernandez, D.; Mahmood, H.; Imran, A.; Munoz, E.J.; Naeem, S.; Abdin, Z.U.; Siddiqui, H.F. Carotid Artery Stenosis: A Look Into the Diagnostic and Management Strategies, and Related Complications. Cureus 2023, 15, e38794. [Google Scholar] [CrossRef]
- Chandiramani, R.; Spirito, A.; Johnson, J.W.; Mehta, A.; Vogel, B.; Faillace, R.T.; Mehran, R. Antiplatelet therapy for coronary artery disease in 2023: Current status and future prospects. Expert Rev. Cardiovasc. Ther. 2023, 21, 311–328. [Google Scholar] [CrossRef]
- Ogrodowczyk, M.; Dettlaff, K.; Jelinska, A. Beta-Blockers: Current State of Knowledge and Perspectives. Mini Rev. Med. Chem. 2016, 16, 40–54. [Google Scholar] [CrossRef]
- Turner, J.M.; Kodali, R. Should Angiotensin-Converting Enzyme Inhibitors ever Be Used for the Management of Hypertension? Curr. Cardiol. Rep. 2020, 22, 95. [Google Scholar] [CrossRef]
- Koch, C.G. Statin therapy. Curr. Pharm. Des. 2012, 18, 6284–6290. [Google Scholar] [CrossRef]
- Hessel, E.A., 2nd. What’s New in Cardiopulmonary Bypass. J. Cardiothorac. Vasc. Anesth. 2019, 33, 2296–2326. [Google Scholar] [CrossRef] [PubMed]
- Girardeau, G.; Lopes-Dos-Santos, V. Brain neural patterns and the memory function of sleep. Science 2021, 374, 560–564. [Google Scholar] [CrossRef] [PubMed]
- Lopez, S.; Hampel, H.; Chiesa, P.A.; Del Percio, C.; Noce, G.; Lizio, R.; Teipel, S.J.; Dyrba, M.; González-Escamilla, G.; Bakardjian, H.; et al. The association between posterior resting-state EEG alpha rhythms and functional MRI connectivity in older adults with subjective memory complaint. Neurobiol. Aging 2024, 137, 62–77. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | |
|---|---|
| Study 1 (practically healthy subjects), n = 25 | |
| Age, years, M (SD) | 22.9 ± 2.57 |
| Male/female, n | 10/15 |
| Educational attainment, years, M (SD) | 16.1 ± 1.29 |
| Self-assessment of health status (according to V.P. Vojtenko, 1991), scores, M (SD) | 7.1 ± 2.58 |
| Study 2 (cardiac surgery patients), n = 25 | |
| Age, years, M (SD) | 62.2 ± 7.35 |
| Male/female, n | 23/2 |
| MoCA, scores, M (SD) | 25.6 ± 2.59 |
| Educational attainment, years, M (SD) | 13.6 ± 2.93 |
| Functional class NYHA, n (%) | |
| I–II | 23 (92) |
| III | 2 (8) |
| Ejection fraction of left ventricle, %, M (SD) | 58.9 ± 9.29 |
| Arterial hypertension, n (%) | 22 (88) |
| Diabetes mellitus type 2, n (%) | 6 (24) |
| Carotid artery stenoses, n (%) | 14 (56) |
| Antiplatelet therapy, n (%) | 24 (96) |
| Beta-blocker therapy, n (%) | 24 (96) |
| ACEi therapy, n (%) | 23 (92) |
| Statin therapy, n (%) | 23 (92) |
| Cardiopulmonary bypass time, min, M (SD) | 85.8 ± 25.11 |
| Variable | Before VR | After VR | p-Value |
|---|---|---|---|
| Functional mobility of nervous processes | |||
| Reaction time, ms, M (SD) | 401.3 ± 31.21 | 379.6 ± 20.97 | 0.0016 |
| Errors, n, M (SD) | 26.1 ± 3.71 | 27.8 ± 3.44 | 0.14 |
| Missed signals, n, M (SD) | 10.3 ± 4.86 | 7.7 ± 3.41 | 0.006 |
| Performance of the brain responses to feedback | |||
| Reaction time, M (SD) | 391.4 ± 24.62 | 378.0 ± 23.56 | 0.001 |
| Errors, n, M (SD) | 154.5 ± 19.68 | 163.1 ± 24.52 | 0.002 |
| Missed signals, n, M (SD) | 51.0 ± 22.05 | 48.8 ± 29.30 | 0.56 |
| The Bourdon’s test | |||
| Processed symbols per 1th min, n, M (SD) | 105.9 ± 47.24 | 138.6 ± 37.16 | 0.01 |
| Processed symbols per 4th min, n, M (SD) | 151.3 ± 34.41 | 142.0 ± 39.23 | 0.35 |
| Attention ratio, scores, M (SD) | 54.8 ± 25.55 | 69.2 ± 30.41 | 0.01 |
| Short-term memory | |||
| Visual memory test, scores, M (SD) | 9.6 ± 0.77 | 9.4 ± 0.79 | 0.48 |
| Mental rotation | |||
| Clock-turn test, scores, M (SD) | 26.4 ± 5.82 | 31.9 ± 7.05 | 0.0005 |
| EEG Ranges | Log10 Power Before VR, mcV2/Hz | Log10 Power After VR, mcV2/Hz | Δ, % | p-Value |
|---|---|---|---|---|
| Theta 1 (4–6 Hz), M (SD) | 0.42 ± 0.13 | 0.38 ± 0.15 | 6.1 | 0.04 |
| Theta 2 (6–8 Hz), M (SD) | 0.40 ± 0.18 | 0.44 ± 0.24 | −15.8 | 0.13 |
| Alpha 1 (8–10 Hz), M (SD) | 0.70 ± 0.31 | 0.85 ± 0.36 | −50.4 | 0.00007 |
| Alpha 2 (10–13 Hz), M (SD) | 0.81 ± 0.36 | 0.86 ± 0.43 | −19.5 | 0.04 |
| Beta 1 (13–20 Hz), M (SD) | −0.03 ± 0.17 | −0.02 ± 0.25 | −5.7 | 0.68 |
| Beta 2 (20–30 Hz), M (SD) | −0.39 ± 0.15 | −0.41 ± 0.18 | 0.9 | 0.42 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tarasova, I.; Trubnikova, O.; Kukhareva, I.; Kupriyanova, D.; Sosnina, A. The Neurophysiological Effects of Virtual Reality Application and Perspectives of Using for Multitasking Training in Cardiac Surgery Patients: Pilot Study. Appl. Sci. 2024, 14, 10893. https://doi.org/10.3390/app142310893
Tarasova I, Trubnikova O, Kukhareva I, Kupriyanova D, Sosnina A. The Neurophysiological Effects of Virtual Reality Application and Perspectives of Using for Multitasking Training in Cardiac Surgery Patients: Pilot Study. Applied Sciences. 2024; 14(23):10893. https://doi.org/10.3390/app142310893
Chicago/Turabian StyleTarasova, Irina, Olga Trubnikova, Irina Kukhareva, Darya Kupriyanova, and Anastasia Sosnina. 2024. "The Neurophysiological Effects of Virtual Reality Application and Perspectives of Using for Multitasking Training in Cardiac Surgery Patients: Pilot Study" Applied Sciences 14, no. 23: 10893. https://doi.org/10.3390/app142310893
APA StyleTarasova, I., Trubnikova, O., Kukhareva, I., Kupriyanova, D., & Sosnina, A. (2024). The Neurophysiological Effects of Virtual Reality Application and Perspectives of Using for Multitasking Training in Cardiac Surgery Patients: Pilot Study. Applied Sciences, 14(23), 10893. https://doi.org/10.3390/app142310893