
Comparison of Air Abrasion and Mechanical Decontamination for Managing Inflammatory Reactions around Dental Implants: A Systematic Review and Meta-Analysis

 , , , , , , and
, , , , , , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Protocol and Eligibility Criteria
2.2. Information Sources and Search Strategy
2.3. Study Selection and Data Extraction
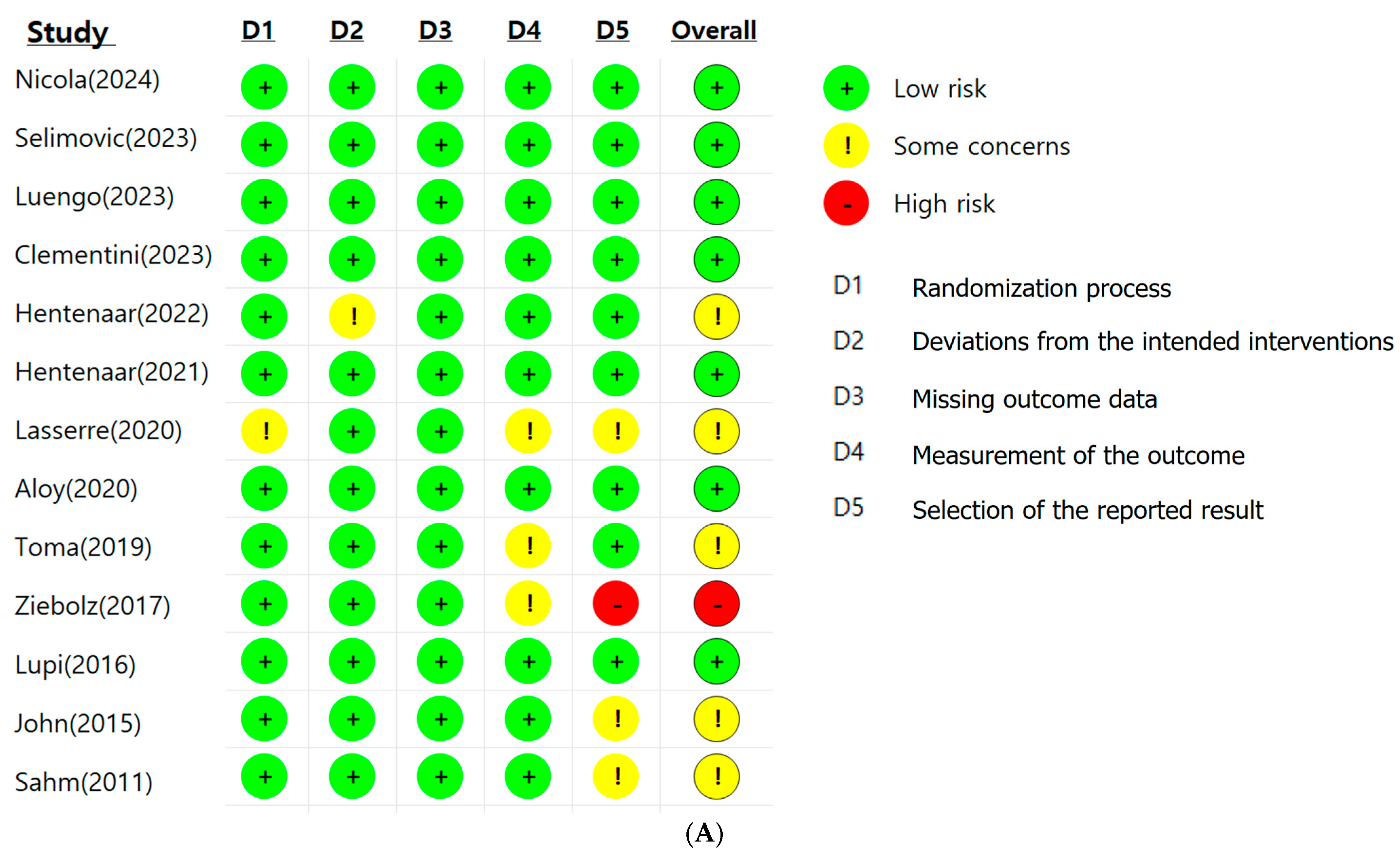
2.4. Risk-of-Bias Assessment
2.5. Data Synthesis and Analysis
3. Results
3.1. Study Selection and Data Extraction
3.2. Risk of Bias Assessment
3.3. Meta-Analysis
3.3.1. Probing Depth
3.3.2. Bleeding on Probing
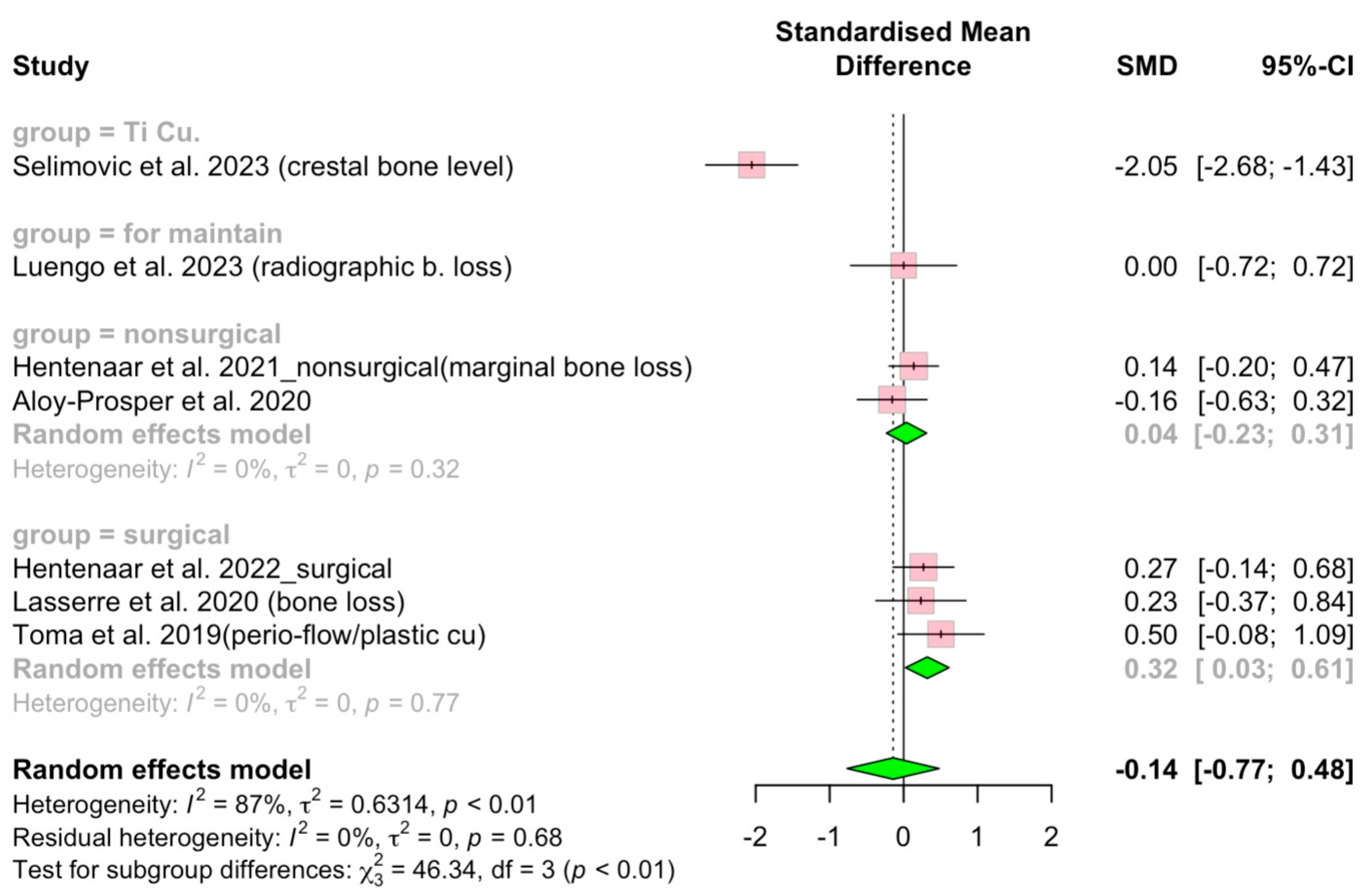
3.3.3. Alveolar Bone Level
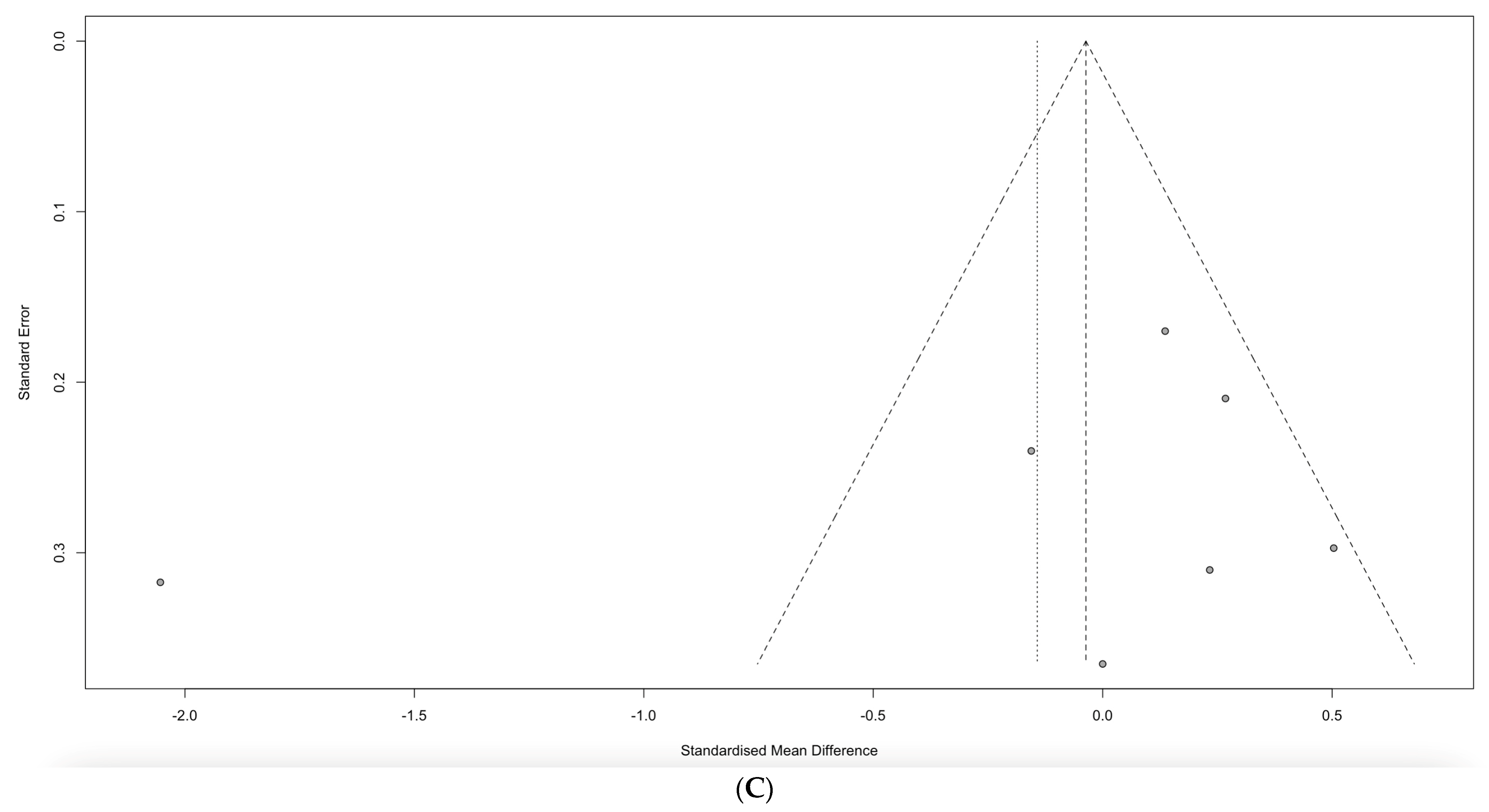
3.4. Publication Bias Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Database | Search | Search Strategy |
|---|---|---|
| PubMed | #1 | “Titanium”[Mesh] |
| #2 | “Titanium”[TW] OR “titanium surface”[TW] OR “titanium surfaces”[TW] OR “rough surface”[TW] | |
| #3 | “Peri-Implantitis”[Mesh] | |
| #4 | “Peri-Implantitis”[TW] OR “Peri Implantitis”[TW] OR “Peri-Implantitides”[TW] OR “Periimplantitis”[TW] OR “Periimplantitides”[TW] | |
| #5 | “Prostheses and Implants”[Mesh] | |
| #6 | “Prostheses and Implants”[TW] OR “Implants and Prostheses”[TW] OR “Prosthetic Implants”[TW] OR “Prostheses and Implant”[TW] OR “Implant and Prostheses”[TW] OR “Prosthetic Implant”[TW] OR “Implant, Prosthetic”[TW] OR “Implants, Prosthetic”[TW] OR “Endoprosthesis”[TW] OR “Endoprostheses”[TW] OR “Prostheses”[TW] OR “Prosthesis”[TW] OR “Implants, Artificial”[TW] OR “Artificial Implant”[TW] OR “Artificial Implants”[TW] OR “Implant, Artificial”[TW] | |
| #7 Combine | #1 OR #2 OR #3 OR #4 OR #5 OR #6 | |
| #8 | “Air Abrasion, Dental”[Mesh] | |
| #9 | “Air Abrasion, Dental”[TW] OR “Abrasion, Dental Air”[TW] OR “Abrasions, Dental Air”[TW] OR “Air Abrasions, Dental”[TW] OR “Dental Air Abrasions”[TW] OR “Dental Air Abrasion”[TW] OR “air abrasive”[TW] OR “air polishing”[TW] OR “abrasive powder”[TW] | |
| #10 Combine | #8 OR #9 | |
| #11 | “Periodontal Index”[Mesh] | |
| #12 | “Periodontal Index”[TW] OR “Index, Periodontal”[TW] OR “Indices, Periodontal”[TW] OR “Periodontal Indices”[TW] OR “Periodontal Indexes”[TW] OR “Indexes, Periodontal”[TW] OR “Community Periodontal Index of Treatment Needs”[TW] OR “CPITN”[TW] OR “Bleeding on Probing, Gingival”[TW] OR “Gingival Bleeding on Probing”[TW] OR “Gingival Index”[TW] OR “Gingival Indices”[TW] OR “Index, Gingival”[TW] OR “Indices, Gingival”[TW] OR “Gingival Indexes”[TW] OR “Indexes, Gingival”[TW] | |
| #13 | “bleeding on probing”[TW] OR “BOP”[TW] OR “probing pocket depth”[TW] OR “PPD”[TW] OR “bone level”[TW] | |
| #14 | “Dental Plaque Index”[Mesh] | |
| #15 | “Indexes, Dental Plaque”[TW] OR “Indices, Dental Plaque”[TW] OR “Dental Plaque Indexes”[TW] OR “Dental Plaque Indices”[TW] OR “Index, Dental Plaque”[TW] OR “Plaque index”[TW] | |
| #16 Combine | #11 OR #12 OR #13 OR #14 OR #15 | |
| #17 Combine | #7 AND #10 AND #16 | |
| #18 Limit | #17 AND (randomizedcontrolledtrial[Filter]) | |
| #19 Limit | #17 AND (“Randomized Controlled Trial” [Publication Type] OR “Controlled Clinical Trial” [Publication Type] OR “Randomized Controlled Trials as Topic”[Mesh] OR “Random Allocation”[Mesh] OR “Double-Blind Method”[Mesh] OR “Single-Blind Method”[Mesh] OR “Clinical Trial” [Publication Type] OR “Clinical Trials as Topic”[Mesh] OR “Clinical Trial”[TW] OR ((singl*[TW] OR doubl*[TW] OR trebl*[TW] OR tripl*[TW]) AND (mask*[TW] OR blind*[TW])) OR “Placebos”[Mesh] OR placebo*[TW] OR random*[TW] OR “Research Design”[Mesh:NoExp]) NOT (“Animals”[Mesh] NOT “Humans”[Mesh]) | |
| #20 Combine | #18 OR #19 | |
| #20 Limit | #20 NOT “In Vitro Techniques”[Mesh] | |
| EMBASE | #1 | “titanium”/exp |
| #2 | “Titanium”:ti,ab,kw,de OR “titanium surface”:ti,ab,kw,de OR “titanium surfaces”:ti,ab,kw,de OR “rough surface”:ti,ab,kw,de | |
| #3 | “periimplantitis”/exp | |
| #4 | “Peri-Implantitis”:ti,ab,kw,de OR “Peri Implantitis”:ti,ab,kw,de OR “Peri-Implantitides”:ti,ab,kw,de OR “Periimplantitis”:ti,ab,kw,de OR “Periimplantitides”:ti,ab,kw,de | |
| #5 | “prostheses and orthoses”/exp | |
| #6 | “Prostheses and Implants”:ti,ab,kw,de OR “Implants and Prostheses”:ti,ab,kw,de OR “Prosthetic Implants”:ti,ab,kw,de OR “Prostheses and Implant”:ti,ab,kw,de OR “Implant and Prostheses”:ti,ab,kw,de OR “Prosthetic Implant”:ti,ab,kw,de OR “Implant, Prosthetic”:ti,ab,kw,de OR “Implants, Prosthetic”:ti,ab,kw,de OR “Endoprosthesis”:ti,ab,kw,de OR “Endoprostheses”:ti,ab,kw,de OR “Prostheses”:ti,ab,kw,de OR “Prosthesis”:ti,ab,kw,de OR “Implants, Artificial”:ti,ab,kw,de OR “Artificial Implant”:ti,ab,kw,de OR “Artificial Implants”:ti,ab,kw,de OR “Implant, Artificial”:ti,ab,kw,de | |
| #7 Combine | #1 OR #2 OR #3 OR #4 OR #5 OR #6 | |
| #8 | “dental surgery”/exp | |
| #9 | “Air Abrasion, Dental”:ti,ab,kw,de OR “Abrasion, Dental Air”:ti,ab,kw,de OR “Abrasions, Dental Air”:ti,ab,kw,de OR “Air Abrasions, Dental”:ti,ab,kw,de OR “Dental Air Abrasions”:ti,ab,kw,de OR “Dental Air Abrasion”:ti,ab,kw,de OR “air abrasive”:ti,ab,kw,de OR “air polishing”:ti,ab,kw,de OR “abrasive powder”:ti,ab,kw,de OR “dental surgery”:ti,ab,kw,de | |
| #10 Combine | #8 OR #9 | |
| #11 | “periodontal index”/exp | |
| #12 | “Periodontal Index”:ti,ab,kw,de OR “Index, Periodontal”:ti,ab,kw,de OR “Indices, Periodontal”:ti,ab,kw,de OR “Periodontal Indices”:ti,ab,kw,de OR “Periodontal Indexes”:ti,ab,kw,de OR “Indexes, Periodontal”:ti,ab,kw,de OR “Community Periodontal Index of Treatment Needs”:ti,ab,kw,de OR “CPITN”:ti,ab,kw,de OR “Bleeding on Probing, Gingival”:ti,ab,kw,de OR “Gingival Bleeding on Probing”:ti,ab,kw,de OR “Gingival Index”:ti,ab,kw,de OR “Gingival Indices”:ti,ab,kw,de OR “Index, Gingival”:ti,ab,kw,de OR “Indices, Gingival”:ti,ab,kw,de OR “Gingival Indexes”:ti,ab,kw,de OR “Indexes, Gingival”:ti,ab,kw,de | |
| #13 | “bleeding on probing”/exp OR “periodontal pocket depth”/exp | |
| #14 | “bleeding on probing”:ti,ab,kw,de OR “BOP”:ti,ab,kw,de OR “probing pocket depth”:ti,ab,kw,de OR “PPD”:ti,ab,kw,de OR “bleed on probing”:ti,ab,kw,de OR “bleeding on probe”:ti,ab,kw,de OR “BoP (bleeding on probing)”:ti,ab,kw,de OR “depth of periodontal pocket”:ti,ab,kw,de OR “periodontal probe depth”:ti,ab,kw,de OR “periodontal probing depth”:ti,ab,kw,de OR “pocket depth (periodontal)”:ti,ab,kw,de OR “pocket probing depth”:ti,ab,kw,de OR “probing depth (periodontal)”:ti,ab,kw,de OR “probing pocket depth”:ti,ab,kw,de OR “periodontal pocket depth”:ti,ab,kw,de | |
| #15 | “bone level”/exp OR “bone level”:ti,ab,kw,de | |
| #16 | “plaque index”/exp | |
| #17 | “Indexes, Dental Plaque”:ti,ab,kw,de OR “Indices, Dental Plaque”:ti,ab,kw,de OR “Dental Plaque Indexes”:ti,ab,kw,de OR “Dental Plaque Indices”:ti,ab,kw,de OR “Index, Dental Plaque”:ti,ab,kw,de OR “Plaque index”:ti,ab,kw,de | |
| #18 Combine | #11 OR #12 OR #13 OR #14 OR #15 OR #16 OR #17 | |
| #19 Combine | #7 AND #10 AND #18 | |
| #20 Limit | #19 AND [randomized controlled trial]/lim | |
| #21 Limit | #20 NOT ‘in vitro study’/exp | |
| Cochrane Library | #1 | [mh “Titanium”] |
| #2 | “Titanium”:ti,ab,kw OR “titanium surface”:ti,ab,kw OR “titanium surfaces”:ti,ab,kw OR “rough surface”:ti,ab,kw | |
| #3 | [mh “Peri-Implantitis”] | |
| #4 | “Peri-Implantitis”:ti,ab,kw OR “Peri Implantitis”:ti,ab,kw OR “Peri-Implantitides”:ti,ab,kw OR “Periimplantitis”:ti,ab,kw OR “Periimplantitides”:ti,ab,kw | |
| #5 | [mh “Prostheses and Implants”] | |
| #6 | “Prostheses and Implants”:ti,ab,kw OR “Implants and Prostheses”:ti,ab,kw OR “Prosthetic Implants”:ti,ab,kw OR “Prostheses and Implant”:ti,ab,kw OR “Implant and Prostheses”:ti,ab,kw OR “Prosthetic Implant”:ti,ab,kw OR “Implant, Prosthetic”:ti,ab,kw OR “Implants, Prosthetic”:ti,ab,kw OR “Endoprosthesis”:ti,ab,kw OR “Endoprostheses”:ti,ab,kw OR “Prostheses”:ti,ab,kw OR “Prosthesis”:ti,ab,kw OR “Implants, Artificial”:ti,ab,kw OR “Artificial Implant”:ti,ab,kw OR “Artificial Implants”:ti,ab,kw OR “Implant, Artificial”:ti,ab,kw | |
| #7 Combine | #1 OR #2 OR #3 OR #4 OR #5 OR #6 | |
| #8 | [mh “Air Abrasion, Dental”] | |
| #9 | “Air Abrasion, Dental”:ti,ab,kw OR “Abrasion, Dental Air”:ti,ab,kw OR “Abrasions, Dental Air”:ti,ab,kw OR “Air Abrasions, Dental”:ti,ab,kw OR “Dental Air Abrasions”:ti,ab,kw OR “Dental Air Abrasion”:ti,ab,kw OR “air abrasive”:ti,ab,kw OR “air polishing”:ti,ab,kw OR “abrasive powder”:ti,ab,kw | |
| #10 Combine | #8 OR #9 | |
| #11 | [mh “Periodontal Index”] | |
| #12 | “Periodontal Index”:ti,ab,kw OR “Index, Periodontal”:ti,ab,kw OR “Indices, Periodontal”:ti,ab,kw OR “Periodontal Indices”:ti,ab,kw OR “Periodontal Indexes”:ti,ab,kw OR “Indexes, Periodontal”:ti,ab,kw OR “Community Periodontal Index of Treatment Needs”:ti,ab,kw OR “CPITN”:ti,ab,kw OR “Bleeding on Probing, Gingival”:ti,ab,kw OR “Gingival Bleeding on Probing”:ti,ab,kw OR “Gingival Index”:ti,ab,kw OR “Gingival Indices”:ti,ab,kw OR “Index, Gingival”:ti,ab,kw OR “Indices, Gingival”:ti,ab,kw OR “Gingival Indexes”:ti,ab,kw OR “Indexes, Gingival”:ti,ab,kw | |
| #13 | “bleeding on probing”:ti,ab,kw OR “BOP”:ti,ab,kw OR “probing pocket depth”:ti,ab,kw OR “PPD”:ti,ab,kw OR “bone level”:ti,ab,kw | |
| #14 | [mh “Dental Plaque Index”] | |
| #15 | “Indexes, Dental Plaque”:ti,ab,kw OR “Indices, Dental Plaque”:ti,ab,kw OR “Dental Plaque Indexes”:ti,ab,kw OR “Dental Plaque Indices”:ti,ab,kw OR “Index, Dental Plaque”:ti,ab,kw OR “Plaque index”:ti,ab,kw | |
| #16 Combine | #11 OR #12 OR #13 OR #14 OR #15 | |
| #17 Combine | #7 AND #10 AND #16 |
| PD | BOP | Bone Level | ||
|---|---|---|---|---|
| Original analysis | SMD (95% CI) | 0.28 (−0.20 to 0.76) | 0.51 (0.07 to 0.95) | −0.14 (−0.77 to 0.48) |
| p-value | p < 0.01 | p < 0.01 | p < 0.01 | |
| Trim-and-Fill analysis | SMD (95% CI) | −0.19 (−0.76 to 0.38) | 0.12 (−0.44 to 0.68) | −0.14 (−0.77 to 0.48) |
| Filled studies /total studies | 5/22 | 3/12 | 0/7 | |
| Egger’s regression test | t-value | 1.76 | 3.15 | −0.81 |
| df | 15 | 7 | 5 | |
| p-value | 0.10 | 0.02 | 0.45 | |
| Bias estimate | 5.85 (SE = 3.32) | 5.65 (SE = 1.67) | −3.51 (SE = 4.31) |
References
- Esposito, M.; Maghaireh, H.; Grusovin, M.G.; Ziounas, I.; Worthington, H.V. Interventions for replacing missing teeth: Management of soft tissues for dental implants. Cochrane Database Syst. Rev. 2012, 2012, Cd006697. [Google Scholar] [CrossRef] [PubMed]
- Gaviria, L.; Salcido, J.P.; Guda, T.; Ong, J.L. Current trends in dental implants. J. Korean Assoc. Oral Maxillofac. Surg. 2014, 40, 50–60. [Google Scholar] [CrossRef] [PubMed]
- De Jong, T.; Bakker, A.D.; Everts, V.; Smit, T.H. The intricate anatomy of the periodontal ligament and its development: Lessons for periodontal regeneration. J. Periodontal Res. 2017, 52, 965–974. [Google Scholar] [CrossRef] [PubMed]
- Marco, F.; Milena, F.; Gianluca, G.; Vittoria, O. Peri-implant osteogenesis in health and osteoporosis. Micron 2005, 36, 630–644. [Google Scholar] [CrossRef] [PubMed]
- Ivanovski, S.; Lee, R. Comparison of peri-implant and periodontal marginal soft tissues in health and disease. Periodontology 2000 2018, 76, 116–130. [Google Scholar] [CrossRef]
- De Araújo, M.F.; Filho, A.F.; da Silva, G.P.; de Melo, M.L.; Napimoga, M.H.; Rodrigues, D.B.; Alves, P.M.; de Lima Pereira, S.A. Evaluation of peri-implant mucosa: Clinical, histopathological and immunological aspects. Arch. Oral Biol. 2014, 59, 470–478. [Google Scholar] [CrossRef]
- Aoki, A.; Mizutani, K.; Schwarz, F.; Sculean, A.; Yukna, R.A.; Takasaki, A.A.; Romanos, G.E.; Taniguchi, Y.; Sasaki, K.M.; Zeredo, J.L.; et al. Periodontal and peri-implant wound healing following laser therapy. Periodontology 2000 2015, 68, 217–269. [Google Scholar] [CrossRef] [PubMed]
- Shah, F.A.; Thomsen, P.; Palmquist, A. Osseointegration and current interpretations of the bone-implant interface. Acta Biomater. 2019, 84, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Carcuac, O.; Berglundh, T. Composition of human peri-implantitis and periodontitis lesions. J. Dent. Res. 2014, 93, 1083–1088. [Google Scholar] [CrossRef] [PubMed]
- Figuero, E.; Graziani, F.; Sanz, I.; Herrera, D.; Sanz, M. Management of peri-implant mucositis and peri-implantitis. Periodontology 2000 2014, 66, 255–273. [Google Scholar] [CrossRef]
- Araujo, M.G.; Lindhe, J. Peri-implant health. J. Periodontol. 2018, 89, S249–S256. [Google Scholar] [CrossRef] [PubMed]
- Pavithra, D.; Doble, M. Biofilm formation, bacterial adhesion and host response on polymeric implants--issues and prevention. Biomed. Mater. 2008, 3, 034003. [Google Scholar] [CrossRef] [PubMed]
- Berglundh, T.; Armitage, G.; Araujo, M.G.; Avila-Ortiz, G.; Blanco, J.; Camargo, P.M.; Chen, S.; Cochran, D.; Derks, J.; Figuero, E.; et al. Peri-implant diseases and conditions: Consensus report of workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Clin. Periodontol. 2018, 45, S286–S291. [Google Scholar] [CrossRef] [PubMed]
- Dukka, H.; Saleh, M.H.A.; Ravidà, A.; Greenwell, H.; Wang, H.L. Is bleeding on probing a reliable clinical indicator of peri-implant diseases? J. Periodontol. 2021, 92, 1669–1674. [Google Scholar] [CrossRef]
- Ramanauskaite, A.; Juodzbalys, G. Diagnostic Principles of Peri-Implantitis: A Systematic Review and Guidelines for Peri-Implantitis Diagnosis Proposal. J. Oral Maxillofac. Res. 2016, 7, e8. [Google Scholar] [CrossRef] [PubMed]
- Mordini, L.; Sun, N.; Chang, N.; De Guzman, J.P.; Generali, L.; Consolo, U. Peri-Implantitis Regenerative Therapy: A Review. Biology 2021, 10, 773. [Google Scholar] [CrossRef]
- Zhu, Y.; Lu, H.; Yang, S.; Liu, Y.; Zhu, P.; Li, P.; Waal, Y.C.M.; Visser, A.; Tjakkes, G.E.; Li, A.; et al. Predictive factors for the treatment success of peri-implantitis: A protocol for a prospective cohort study. BMJ Open 2024, 14, e072443. [Google Scholar] [CrossRef]
- Pujarern, P.; Klaophimai, A.; Amornsettachai, P.; Panyayong, W.; Chuenjitkuntaworn, B.; Rokaya, D.; Suphangul, S. Efficacy of Biofilm Removal on the Dental Implant Surface by Sodium Bicarbonate and Erythritol Powder Airflow System. Eur. J. Dent. 2024, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Corsalini, M.; Montagnani, M.; Charitos, I.A.; Bottalico, L.; Barile, G.; Santacroce, L. Non-Surgical Therapy and Oral Microbiota Features in Peri-Implant Complications: A Brief Narrative Review. Healthcare 2023, 11, 652. [Google Scholar] [CrossRef] [PubMed]
- Tripathi, R.; Vasudevan, S.; Palle, A.R.; Gedela, R.K.; Punj, A.; Vaishnavi, V. Awareness and management of peri-implantitis and peri-mucositis among private dental Practitioners in Hyderabad-A cross-sectional study. J. Indian Soc. Periodontol. 2020, 24, 461–466. [Google Scholar] [CrossRef] [PubMed]
- Citterio, F.; Zanotto, E.; Pellegrini, G.; Annaratore, L.; Barbui, A.M.; Dellavia, C.; Baima, G.; Romano, F.; Aimetti, M. Comparison of Different Chemical and Mechanical Modalities for Implant Surface Decontamination: Activity against Biofilm and Influence on Cellular Regrowth-An In Vitro Study. Front. Surg. 2022, 9, 886559. [Google Scholar] [CrossRef] [PubMed]
- Munakata, M.; Suzuki, A.; Yamaguchi, K.; Kataoka, Y.; Sanda, M. Effects of implant surface mechanical instrumentation methods on peri-implantitis: An in vitro study using a circumferential bone defect model. J. Dent. Sci. 2022, 17, 891–896. [Google Scholar] [CrossRef]
- Tan, N.C.P.; Miller, C.M.; Antunes, E.; Sharma, D. Impact of physical decontamination methods on zirconia implant surface and subsequent bacterial adhesion: An in-vitro study. Clin. Exp. Dent. Res. 2022, 8, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Cobb, C.M.; Daubert, D.M.; Davis, K.; Deming, J.; Flemmig, T.F.; Pattison, A.; Roulet, J.F.; Stambaugh, R.V. Consensus Conference Findings on Supragingival and Subgingival Air Polishing. Compend. Contin. Educ. Dent. 2017, 38, e1–e4. [Google Scholar]
- Liu, C.C.; Dixit, N.; Hatz, C.R.; Janson, T.M.; Bastendorf, K.D.; Belibasakis, G.N.; Cosgarea, R.; Karoussis, I.K.; Mensi, M.; O’Neill, J.; et al. Air powder waterjet technology using erythritol or glycine powders in periodontal or peri-implant prophylaxis and therapy: A consensus report of an expert meeting. Clin. Exp. Dent. Res. 2024, 10, e855. [Google Scholar] [CrossRef]
- Keim, D.; Nickles, K.; Dannewitz, B.; Ratka, C.; Eickholz, P.; Petsos, H. In vitro efficacy of three different implant surface decontamination methods in three different defect configurations. Clin. Oral Implant. Res. 2019, 30, 550–558. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 89. [Google Scholar] [CrossRef] [PubMed]
- Nicola, D.; Isabella, R.; Carolina, C.; Baldini, N.; Raffaele, M. Treatment of peri-implant mucositis: Adjunctive effect of glycine powder air polishing to professional mechanical biofilm removal. 12 months randomized clinical study. Clin. Implant Dent. Relat. Res. 2024, 26, 415–426. [Google Scholar] [CrossRef] [PubMed]
- Selimović, A.; Bunæs, D.F.; Lie, S.A.; Lobekk, M.A.; Leknes, K.N. Non-surgical treatment of peri-implantitis with and without erythritol air-polishing a 12-month randomized controlled trial. BMC Oral Health 2023, 23, 240. [Google Scholar] [CrossRef] [PubMed]
- Luengo, F.; Sanz-Esporrín, J.; Sanz-Sánchez, I.; Solonko, M.; Herrera, D.; Sanz, M. Clinical, microbiological and biochemical impact of a supportive care protocol with an air-polishing device, after surgical treatment of peri-implantitis: Randomized clinical trial. Clin. Oral Implant. Res. 2023, 34, 378–392. [Google Scholar] [CrossRef] [PubMed]
- Clementini, M.; Fabrizi, S.; Discepoli, N.; Minoli, M.; De Sanctis, M. Evaluation of the adjunctive use of Er:YAG laser or erythritol powder air-polishing in the treatment of peri-implant mucositis: A randomized clinical trial. Clin. Oral Implant. Res. 2023, 34, 1267–1277. [Google Scholar] [CrossRef]
- Hentenaar, D.F.M.; De Waal, Y.C.M.; Stewart, R.E.; Van Winkelhoff, A.J.; Meijer, H.J.A.; Raghoebar, G.M. Erythritol air polishing in the surgical treatment of peri-implantitis: A randomized controlled trial. Clin. Oral Implant. Res. 2022, 33, 184–196. [Google Scholar] [CrossRef]
- Hentenaar, D.F.M.; De Waal, Y.C.M.; Stewart, R.E.; Van Winkelhoff, A.J.; Meijer, H.J.A.; Raghoebar, G.M. Erythritol airpolishing in the non-surgical treatment of peri-implantitis: A randomized controlled trial. Clin. Oral Implant. Res. 2021, 32, 840–852. [Google Scholar] [CrossRef] [PubMed]
- Lasserre, J.F.; Brecx, M.C.; Toma, S. Implantoplasty Versus Glycine Air Abrasion for the Surgical Treatment of Peri-implantitis: A Randomized Clinical Trial. Int. J. Oral Maxillofac. Implant. 2020, 35, 197–206. [Google Scholar] [CrossRef]
- Aloy-Prósper, A.; Pellicer-Chover, H.; Peñarrocha-Oltra, D.; Peñarrocha-Diago, M. Effect of a single initial phase of non-surgical treatment of peri-implantitis: Abrasive air polishing versus ultrasounds. A prospective randomized controlled clinical study. J. Clin. Exp. Dent. 2020, 12, e902–e908. [Google Scholar] [CrossRef] [PubMed]
- Toma, S.; Brecx, M.C.; Lasserre, J.F. Clinical Evaluation of Three Surgical Modalities in the Treatment of Peri-Implantitis: A Randomized Controlled Clinical Trial. J. Clin. Med. 2019, 8, 966. [Google Scholar] [CrossRef] [PubMed]
- Ziebolz, D.; Klipp, S.; Schmalz, G.; Schmickler, J.; Rinke, S.; Kottmann, T.; Fresmann, S.; Einwag, J. Comparison of different maintenance strategies within supportive implant therapy for prevention of peri-implant inflammation during the first year after implant restoration. A randomized, dental hygiene practice-based multicenter study. Am. J. Dent. 2017, 30, 190–196. [Google Scholar] [PubMed]
- Lupi, S.M.; Granati, M.; Butera, A.; Collesano, V.; Rodriguez, Y.B.R. Air-abrasive debridement with glycine powder versus manual debridement and chlorhexidine administration for the maintenance of peri-implant health status: A six-month randomized clinical trial. Int. J. Dent. Hyg. 2017, 15, 287–294. [Google Scholar] [CrossRef]
- John, G.; Sahm, N.; Becker, J.; Schwarz, F. Nonsurgical treatment of peri-implantitis using an air-abrasive device or mechanical debridement and local application of chlorhexidine. Twelve-month follow-up of a prospective, randomized, controlled clinical study. Clin. Oral Investig. 2015, 19, 1807–1814. [Google Scholar] [CrossRef]
- Sahm, N.; Becker, J.; Santel, T.; Schwarz, F. Non-surgical treatment of peri-implantitis using an air-abrasive device or mechanical debridement and local application of chlorhexidine: A prospective, randomized, controlled clinical study. J. Clin. Periodontol. 2011, 38, 872–878. [Google Scholar] [CrossRef]
- Vilarrasa, J.; Soldini, M.C.; Pons, R.; Valles, C.; Blasi, G.; Monje, A.; Nart, J. Outcome indicators of non-surgical therapy of peri-implantitis: A prospective case series analysis. Clin. Oral Investig. 2023, 27, 3125–3138. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.N.; Koldsland, O.C.; Roos-Jansåker, A.M.; Wohlfahrt, J.C.; Verket, A.; Mdala, I.; Magnusson, A.; Salvesen, E.; Hjortsjö, C. Non-surgical treatment of mild to moderate peri-implantitis with an oscillating chitosan brush or a titanium curette-12-month follow-up of a multicenter randomized clinical trial. Clin. Oral Implant. Res. 2023, 34, 684–697. [Google Scholar] [CrossRef] [PubMed]
- Roccuzzo, M.; Mirra, D.; Roccuzzo, A. Surgical treatment of peri-implantitis. Br. Dent. J. 2024, 236, 803–808. [Google Scholar] [CrossRef] [PubMed]
- Ramanauskaite, A.; Cafferata, E.A.; Begic, A.; Schwarz, F. Surgical interventions for the treatment of peri-implantitis. Clin. Implant Dent. Relat. Res. 2023, 25, 682–695. [Google Scholar] [CrossRef] [PubMed]
- Louropoulou, A.; Slot, D.E.; Van der Weijden, F.A. Titanium surface alterations following the use of different mechanical instruments: A systematic review. Clin. Oral Implant. Res. 2012, 23, 643–658. [Google Scholar] [CrossRef] [PubMed]
- Tan, N.C.P.; Khan, A.; Antunes, E.; Miller, C.M.; Sharma, D. The effects of physical decontamination methods on zirconia implant surfaces: A systematic review. J. Periodontal Implant Sci. 2021, 51, 298–315. [Google Scholar] [CrossRef] [PubMed]
- Corbella, S.; Radaelli, K.; Alberti, A.; Francetti, L.; Taschieri, S. Erythritol powder airflow for the treatment of peri-implant mucositis: A randomized controlled clinical trial. Int. J. Dent. Hyg. 2024. online ahead of print. [Google Scholar] [CrossRef]
- Toma, S.; Lasserre, J.F.; Taïeb, J.; Brecx, M.C. Evaluation of an air-abrasive device with amino acid glycine-powder during surgical treatment of peri-implantitis. Quintessence Int. 2014, 45, 209–219. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, F.; Becker, K.; Renvert, S. Efficacy of air polishing for the non-surgical treatment of peri-implant diseases: A systematic review. J. Clin. Periodontol. 2015, 42, 951–959. [Google Scholar] [CrossRef] [PubMed]
- Chen, I.C.; Su, C.Y.; Tu, J.J.; Kao, D.W.; Fang, H.W. In vitro studies of factors affecting debridement of dental implants by tricalcium phosphate powder abrasive treatment. Sci. Rep. 2023, 13, 8271. [Google Scholar] [CrossRef] [PubMed]
- Abuhajar, E.; Salim, N.A.; Satterthwaite, J.D.; Silikas, N.; Anweigi, L.M. Effect of bioceramic powder abrasion on different implant surfaces. J. Prosthodont. 2024. online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Patil, C.; Agrawal, A.; Abullais, S.S.; Arora, S.; Khateeb, S.U.; Fadul, A.E.M. Effectiveness of Different Chemotherapeutic Agents for Decontamination of Infected Dental Implant Surface: A Systematic Review. Antibiotics 2022, 11, 593. [Google Scholar] [CrossRef] [PubMed]
- Müller, N.; Moëne, R.; Cancela, J.A.; Mombelli, A. Subgingival air-polishing with erythritol during periodontal maintenance: Randomized clinical trial of twelve months. J. Clin. Periodontol. 2014, 41, 883–889. [Google Scholar] [CrossRef]
- Kotsakis, G.A.; Lan, C.; Barbosa, J.; Lill, K.; Chen, R.; Rudney, J.; Aparicio, C. Antimicrobial Agents Used in the Treatment of Peri-Implantitis Alter the Physicochemistry and Cytocompatibility of Titanium Surfaces. J. Periodontol. 2016, 87, 809–819. [Google Scholar] [CrossRef] [PubMed]





| Study (Country, Year) | Groups | Intervention Device | Test Powder for Intervention | Control Group |
|---|---|---|---|---|
| Nicola, D., et al., Italy (2024) [28] | Participants in the test group were treated with an additional debridement using a glycine powder air polishing device (StarJet®, Mectron, Carasco, Italy) at each of the experimental sites (mesial, lingual, distal, and buccal) for 5 s with a subgingival nozzle, following the manufacturer’s instructions. | Glycine powder air polishing device (StarJet®, Mectron) | Glycine powder (Glycine Powder, Mectron) | Both groups underwent comprehensive full-mouth ultrasonic debridement using a magnetostrictive device (Cavitron Select SPS®, a product of Dentsply Sirona) that featured fine ultrasonic tips and a silicone insert (SlimLine 30 k insert, SofTip implant 30 k insert, also from Dentsply). |
| Selimović, A., et al., Norway (2023) [29] | The test subjects were also given a low-abrasive erythritol powder (Air-flow Plus, EMS, Nyon, Switzerland; particle size of 14 μm) through a PerioFlow handpiece that included an airflow unit (Airflow One, EMS, Nyon, Switzerland). The handpiece had a special nozzle designed for sub-mucosal peri-implant delivery that directed the air jet perpendicularly to the implant surface from the nozzle’s tip (PerioFlow nozzle, EMS, Nyon, Switzerland). | Airflow unit (Airflow One®, EMS, Nyon, Switzerland) | Low abrasive erythritol powder (Air-flow® Plus, EMS, Nyon, Switzerland; particle size 14 μm) | Conventional ultrasonic/curette instrumentation only |
| Luengo, F., et al., Spain (2023) [30] | The use of an ultrasonic instrument with a PEEK tip (Instrument PI, EMS, Nyon, Switzerland) was employed for decontaminating the implant surface both above and below the mucosal layer for a period of one minute. Following this, the implant surface was refined with the aid of a glycine powder air-polishing device, specifically the Perio AIR-flow® and Airflow Master Piezon® (EMS). | Glycine powder air-polishing device (Perio AIR-flow® and Airflow Master Piezon®, EMS) | Glycine powder | Patients employed the identical implant debridement approach, with polishing being performed using a rubber cup and polishing paste (Detartrine®, Septodont, Saint Maur, France). |
| Clementini, M., et al., Italy (2023) [31] | In the test group, the Perio-Flow nozzle (AIR-FLOW Master Piezon; EMS) was placed at each site of the peri-implant pocket (mesial, oral, distal, and buccal), enabling the erythritol powder (AIR-FLOW Powder PERIO; EMS) to exit for a duration of 5 s at an angle ranging from 60 to 90 degrees. | Perio-Flow nozzle (AIR-FLOW Master Piezon; EMS) | Erythritol powder (AIR-FLOW Powder PERIO; EMS) | Mechanical instrumentation of implant surfaces was performed using titanium curettes (Hu-Friedy) in all treatment groups (Appendix A Table A1). After that, subjects were randomly assigned to one of three treatment groups: no adjunctive methods (control group). |
| Hentenaar, D. et al., Netherlands (2022) [32] | The Airflow® Master Piezon® device, which is manufactured by EMS and based in Nyon, Switzerland, was used to treat the implant surface with an erythritol-based powder containing 0.3% chlorhexidine. This powder had a particle size of 14 μm and was marketed under the brand name PLUS Powder by EMS. The treatment was performed using the Airflow® device to achieve a higher quality surface finish. | Airflow®, using the Airflow Master Piezon® device, EMS, Nyon, Switzerland | Erythritol-based powder containing 0.3% chlorhexidine (14 μm, PLUS Powder, EMS) | Mechanically cleaned with gauzes soaked in saline. |
| Hentenaar, D. et al., Netherlands (2021) [33] | The air powder was applied subgingivally through a handpiece with a plastic nozzle. | N/A | Erythritol-based powder (grain size 14 μm) containing 0.3% chlorhexidine (PLUS® powder, Electro Medical Systems (EMS), Nyon, Switzerland) | Treated once using a piezoelectric ultrasonic scaler with a PEEK-coated plastic tip (PI instrument, EMS). |
| Lasserre, J. et al., Belgium (2020) [34] | The Air-Flow Perio system (Air-Flow Handy 3.0 Perio, EMS) was used to treat contaminated implant surfaces in the glycine air-polishing group, utilizing amino acid glycine powder (Ø 25 μm) (Air-Flow Perio powder, EMS). A special plastic nozzle (1.7 cm in length, with a 0.8 mm tip diameter) was connected to a dedicated handpiece (Air-Flow EL-542/A, EMS) and applied in a non-contact mode using a circular motion that moved from the coronal to the apical and tangential to the implant surface. The treatment time for each implant aspect was 15 s, and a high-speed aspiration system was used to prevent powder accumulation in the tissues and on the implant surface. | Air-Flow Perio (Air-Flow Handy 3.0 Perio, EMS); The specially designed plastic nozzle (length 1.7 cm; Ø 0.8 mm at the tip) was fixed on a dedicated handpiece (Air-Flow EL-542/A, EMS) | Amino acid glycine powder (Ø 25 µm) (Air-Flow Perio powder, EMS) | In the implantoplasty group, exposed and accessible titanium surfaces were treated with a resective approach, the aim of which was to polish the macro- and microtopography of the implant to remove the microbial biofilm mechanically. To limit tissue recession, the supra- and intrabony components of the contaminated implants were treated without osteoplasty. Round diamond burs (particle size, 30 μm) of various diameters (1.8, 2.3, and 3.5 mm) (Komet, Gerb. Brasseler, Lemgo, Germany) were assembled on a handpiece (KaVo Dental, Allgan, Germany) working at 15,000 rpm under copious saline irrigation. Small-diameter burs were necessary for adequate access to narrow intrabony defects. The whole implantoplasty procedure lasted approximately 5 min. |
| Aloy-Prósper, A. et al., Spain (2020) [35] | The instructions provided by the manufacturer were adhered to, and an abrasive air polisher was utilized on each implant surface for a duration of 5 s. | EMS Air-Flow Master Piezon® System (E.M.S. Electro Medical Systems S.A, Nyon, Switzerland) | Glycine powder | Mechanical debridement using titanium curettes in every case. |
| Toma, S. et al.,. Belgium (2019) [36] | Utilizing a specialized nozzle aligned parallel to the implant surface at each angle, from the coronal to the apical, with a 5-s duration of non-contact mode circular movement, followed by sterile saline flushing. | Perio-Flow® device (Perio-Flow Handy, Perio-Flow nozzle; EMS Medical, Nyon, Switzerland) | Amino acid glycine powder (Air-Flow Perio Powder, EMS Medical) | Treated using the Ti-Brush®, a plastic curette developed by the Straumann company based in Basel, Switzerland. |
| Ziebolz, D., et al., Germany (2017) [37] | Utilizing manual curettes and an air polishing system (Air-Flow Master, EMS) containing glycine powder (Perio-Flow, EMS) for therapeutic purposes. | Air polishing system (Air-Flow Master) | Glycine powder (Perio-Flow) | Plaque removal was performed by using manual curettes, a sonic-driven scaler, and a prophylaxis brush. |
| Lupi, S. M., et al., Italy (2017) [38] | The Perio-Flow nozzle, which is manufactured by EMS in Nyon, Switzerland, was utilized for 5 s on each of the lingual, distal, mesial, and palatal sides, as suggested by the manufacturer. | Air-abrasive device (AIR-FLOW Master 4; EMS) | Glycine powder (AIR-FLOW Powder SOFT; EMS) | Using plastic curettes (Implant Deplaquers, Kerr) and following with pocket irrigation using a 0.1% chlorhexidine digluconate solution (Corsodyls; GlaxoSmithKline Consumer Healthcare, Brentford, Middlesex, United Kingdom) (CHX) and sub-mucosal application of 1% CHX gel (Corsodyls Gel; GlaxoSmithKline Consumer Healthcare, Brentford, Middlesex, UK) was used to perform mechanical debridement. |
| John, G., et al., Germany (2015) [39] | A circular motion with the Hand-piece (Air-Flow® EL-308/A, EMS) was performed from coronal to apical parallel to the implant surface in a non-contact manner. The time allocated for each aspect, including mesial, distal, vestibular, and oral, was limited to 5 s. | AIR-FLOW Master®; PERIO-FLOW® nozzle, EMS, Nyon Switzerland | Amino acid glycine powder (Air-Flow® Perio Powder, EMS) (dv10 = 5 μm, dv50 = 20 μm, dv90 = 63 μm; corresponding to the size below which is 10, 50 (median particle size) and 90% of the total material volume, respectively) | Treated with carbon curettes (Straumann, Waldenburg, Switzerland) followed by pocket irrigation with a 0.1% chlorhexidine digluconate solution (Corsodyl®, GlaxoSmithKline Consumer Healthcare, Bühl, Germany) (CHX) and sub-mucosal application of 1% CHX gel (Corsodyl® Gel, GlaxoSmithKline Consumer Healthcare, Bühl, Germany) until the operator felt that the implant surfaces were adequately cleaned. |
| Sahm, N., et al., Germany (2011) [40] | The Air Flows EL-308/A handpiece (EMS) was moved in a circular motion from the coronal to the apical region, parallel to the implant surface, in a non-contact mode. The instrumentation time at each aspect, including the mesial, distal, vestibular, and oral regions, was limited to 5 s. | Air Flow Masters, Perio-Flows nozzle, EMS | Amino acid glycine powder (Air-Flows Perio Powder, EMS) (dv10: 5 mm, dv50: 20 mm, dv90: 63 mm; corresponding to the size below which is 10%, 50% (median particle size), and 90% of the total material volume, respectively) | Treated with carbon curettes (Straumann, Waldenburg, Switzerland) in conjunction with pocket irrigation using a 0.1% chlorhexidine digluconate solution (Corsodyls, GlaxoSmithKline Consumer Healthcare, Bühl, Germany) (CHX) and sublingual application of 1% CHX gel (Corsodyls Gel, GlaxoSmithKline Consumer Healthcare). |
| Study (Country, Year) | Peri-Implant Disease Diagnosis Parameter | Study Population | Follow-Up Period | Outcome | Results |
|---|---|---|---|---|---|
| Nicola, D., et al., Italy (2024) [28] | The presence of an implant in place for at least one year prior to the patient’s referral, as well as the presence of bleeding from multiple sites and/or suppuration after gentle probing. | Initial: n = 52; 157 implants F(t:69%, c:84%), M(t:31%, c:15%) Final: test: n = 25; 69 implants; control: n = 22; 68 implants. Mean age: test: 57.92; control: 60.96 | 3, 12 months | BOP, mPI, PPD, REC | Glycine powder air polishing does not provide a significant additional benefit over full-mouth ultrasonic debridement alone in resolving peri-implant mucositis. The higher the initial level of bleeding and probing depth, the lower the likelihood of disease resolution. |
| Selimović, A., et al., Norway (2023) [29] | Progress bone loss (CBL loss ≥ 2 mm) PD ≥ 4 mm BOP(+), SOP(+) | Initial: n = 43, 62 implants (22F, 21M) Final: t: n = 23, 31 implants; c: n = 20, 31 implants. Mean age: t65.8 ± 11.6, c64.5 ± 13.6 | Baseline and 3, 6, 9, and 12 months | BOP, plaque (%), PD, KMW, crestal bone level | The study concluded that adjunctive erythritol air polishing did not provide a significant additional benefit over conventional non-surgical management in peri-implantitis. Both treatments failed to effectively resolve peri-implantitis, highlighting the need for ongoing management strategies and more effective non-surgical treatments. |
| Luengo, F., et al., Spain (2023) [30] | Bone loss > 2 mm BOP(+), SOP(+) PD ≥ 5 mm | Initial: n = 30 (12M, 18F) Final: t; n = 15; c: n = 15. Mean age: t62.2, c65.5 | 12 months | BOP, PI, PD, REC, RBL | Adding glycine powder air polishing to supportive peri-implant care protocol resulted in better clinical outcomes, including reduced probing depth, compared to conventional methods. |
| Clementini, M., et al., Italy (2023) [31] | Bone loss < 2 mm BOP(+), SOP(+) | Initial: n = 75 (39M, 36F) Final: T1: n = 25, 62 implants, T2: n = 25, 59 implants C: n = 25, 58 implants. Mean age: T1: 58.2 ± 9.6, T2: 57.5 ± 9.8 C: 55.7 ± 10.1 | 6 months | BOP, PI, PD | The utilization of air polishing and erythritol in non-surgical PM therapy appears to offer no substantial or clinically relevant advantages over the use of submarginal curettes alone in terms of reducing BOP and PPD, as well as achieving complete disease resolution. Baseline PPD of less than 4 mm, the presence of oral KM, and the presence of submucosal restorative margins are critical factors in achieving complete resolution of peri-implant mucositis. |
| Hentenaar, D., et al., Netherlands (2022) [32] | Probing pocket depth (PPD) ≥ 5 mm with concomitant bleeding and/or suppuration on probing (BOP/SOP) and progressive loss of marginal bone (MBL) ≥2 mm | Initial: n = 58 (33M, 25F) Final: T: n = 27, 54 implants C: n = 31, 40 implants. Mean age: T: 59.6; C: 59.3 | At baseline and 3, 6, 9, and 12 months after intervention | BOP, PI, PPD, MBL | Erythritol air polishing was not more effective than saline irrigation in clinical, radiographic, and microbiological parameters for peri-implantitis surgical treatment. Both treatments resulted in low treatment success. |
| Hentenaar, D., et al., Netherlands (2021) [33] | Bone loss ≥ 2 mm BOP(+), SOP (+) PD ≥ 5 mm | Initial: n = 80, 139 implants (45M, 35F) Final: T: n = 40, 66 implants, C: n = 39, 73 implants. Mean age: T: 62 ± 8.9, C: 55 ± 14.1 | 3 months (successful cases up to 6, 9, 12 months) | BOP, peri-implant SOP (%), Plq (%), PPD, MBL | Erythritol air polishing and piezoelectric ultrasonic scaling seem to be equally effective when it comes to treating peri-implantitis non-surgically, as they show similar results in clinical, radiographic, and microbiological aspects. However, neither of these therapies can completely resolve peri-implantitis, which means that most patients will require additional surgical treatment. Fortunately, non-surgical maintenance was successful for a period of 12 months in the cases that were successful. |
| Lasserre, J., et al., Belgium (2020) [34] | PPD ≥ 5 mm Bone loss ≥ 2 mm BOP(+), SOP(+) | Initial: n = 31, 42 implants (9M, 22F) Final: T: n = 15 (20 implants); C: n = 16 (22 implants). Mean age: T: 71, C: 62.3 | 3, 6 months | PI, BOP, PPD, CAL, REC, BL | According to a six-month follow-up study, implantoplasty is as successful as glycine air polishing in addressing peri-implantitis during surgical treatment. |
| Aloy-Prósper, A., et al., Spain (2020) [35] | None | Initial: n = 34, 70 implants (18M, 16F) Final: T: n = 17 (32 implants); C: n = 17 (38 implants). Mean age: 58.4 ± 9.9 | 3 weeks | PI, BOP, PPD, CAL, REC, BL, mod. GI | Although the specific technique of debridement appears to have little impact, the initial stage still manages to lessen inflammation, which enables the tissues to be more prepared for the surgical intervention. |
| Toma, S., et al.,. Belgium (2019) [36] | PPD ≥ 5 mm Bone loss ≥ 2 mm No mobility | Initial: n = 47, 70 implants (8M, 39F) Final: PC: n = 15, 25 implants; PF: n = 16, 22 implants; TB: n = 16, 23 implants. Mean age: PC: 68.9 ± 15.8; PF: 67.5 ± 12.9; TB: 61.7 ± 13.4 | 3, 6 months | PI, BOP, GI, PPD, RAL, BL | Titanium brush and glycine air polishing exhibited superior effectiveness compared to other methods; however, the treatment success rate remained relatively low. To enhance the effectiveness of these procedures, incorporating antimicrobials and/or antibiotics may prove to be a more promising approach, and further investigation is warranted to explore this potential. |
| Ziebolz, D., et al., Germany (2017) [37] | None | Initial: n = 105, 167 implants (35M, 27F) Final: total n = 62, 101 implants; A (cu, us, br) n = 17, 24 implants; B (cu, ap, br) n = 15, 26 implants; C (cu, us, br, chx) n = 16, 30 implants, D (cu, ap, br, chx) n = 14, 21 implants. Mean age: 55.21 ± 11.3 | 12 months | BOP, PPD, MR | All strategies employed were effective in preventing peri-implant inflammation. |
| Lupi, S. M., et al., Italy (2017) [38] | Probing depth (PD) ≥ 4 mm, suppuration (+), bone resorption ≥ 30% compared to the initial situation | Initial: n = 46, 88 implants (35PE, 11TE) Final: T: n = 24, 51 implants; C: n = 22, 37 implants. Mean age: T: 54.58 ± 15.52; C: 53.77 ± 12.28 | 3, 6 months | BOP, PI, CAL, PD, BS | The use of glycine appears to be a more effective and suitable choice for maintaining peri-implant health compared to traditional treatments involving plastic curettes and chlorhexidine. |
| John, G., et al., Germany (2015) [39] | Probing depth ≥ 4 mm, BOP (+), suppuration (+), radiographic (loss of supporting bone ≤ 30% compared to the situation after implant placement) | Initial: n = 25, 36 implants (11M, 14F) Final: T: n = 12, 18 implants; C: n = 13, 18 implants. Mean age: 62.0 ± 13.2 | Baseline, 12 months | BOP, PI, PD, MR, CAL | Both air-abrasive device and mechanical debridement are effective in the non-surgical management of peri-implantitis, with the air-abrasive device particularly effective in reducing inflammation as measured by BOP. Both methods are part of an effective management strategy for peri-implantitis. |
| Sahm, N., et al., Germany (2011) [40] | Probing depth ≥ 4 mm, BOP and suppuration, radiographic (loss of supporting bone 30% compared with the situation after implant placement) | Initial: n = 32, 43 implants (12M, 20F) Final: T: n = 15, 22 implants; C: n = 15, 19 implants. Mean age: 60.6 ± 38.6 | Baseline, 3, 6 months | BOP, PI, PD, MR, CAL | This study found that both the air-abrasive device and mechanical debridement treatments resulted in similar improvements in clinical attachment levels and probing depths, but the air-abrasive device was more effective in reducing bleeding on probing. The results suggest that both treatments may be effective, but air-abrasive device may better control inflammation in the short term. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jang, K.-J.; Lyu, A.; Han, S.-H.; Kim, N.J.; Han, S.-B.; Song, H.-J.; Park, W.-J.; Park, J.-B. Comparison of Air Abrasion and Mechanical Decontamination for Managing Inflammatory Reactions around Dental Implants: A Systematic Review and Meta-Analysis. Appl. Sci. 2024, 14, 7775. https://doi.org/10.3390/app14177775
Jang K-J, Lyu A, Han S-H, Kim NJ, Han S-B, Song H-J, Park W-J, Park J-B. Comparison of Air Abrasion and Mechanical Decontamination for Managing Inflammatory Reactions around Dental Implants: A Systematic Review and Meta-Analysis. Applied Sciences. 2024; 14(17):7775. https://doi.org/10.3390/app14177775
Chicago/Turabian StyleJang, Ki-Jung, Ahrim Lyu, Sung-Hoon Han, Na Jin Kim, Saet-Byeol Han, Hye-Jung Song, Won-Jong Park, and Jun-Beom Park. 2024. "Comparison of Air Abrasion and Mechanical Decontamination for Managing Inflammatory Reactions around Dental Implants: A Systematic Review and Meta-Analysis" Applied Sciences 14, no. 17: 7775. https://doi.org/10.3390/app14177775
APA StyleJang, K.-J., Lyu, A., Han, S.-H., Kim, N. J., Han, S.-B., Song, H.-J., Park, W.-J., & Park, J.-B. (2024). Comparison of Air Abrasion and Mechanical Decontamination for Managing Inflammatory Reactions around Dental Implants: A Systematic Review and Meta-Analysis. Applied Sciences, 14(17), 7775. https://doi.org/10.3390/app14177775