
The Effect of Tongkat Ali Supplementation on Body Composition in Exercise-Trained Males and Females

 ,
,  , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Body Composition
2.3. Profile of Mood States
- Tension: feelings of tension, nervousness, and apprehension.
- Depression: feelings of sadness, discouragement, and low morale.
- Anger: feelings of anger, irritability, and hostility.
- Vigor: feelings of energy, enthusiasm, and alertness.
- Fatigue: feelings of tiredness, weariness, and low energy.
- Confusion: feelings of confusion, uncertainty, and lack of clarity.
2.4. Psychomotor Vigilance (PVT) Test
- Stimulus presentation: participants are asked to fixate on a screen where a visual stimulus (i.e., a number) appears at random intervals.
- Response: as soon as the stimulus appears, participants must tap the iPad or computer as quickly as possible.
- Duration: the test lasts five minutes.
- Reaction time (RT): The primary measure is the time it takes for a participant to respond (i.e., by tapping the iPad or computer) to the stimulus. This is usually recorded in milliseconds.
- False starts: Responses that occur before the stimulus are presented. That is, the subject taps the iPad or computer before a stimulus appears.
2.5. The Pittsburgh Sleep Quality Index (PSQI)
- Subjective sleep quality: an individual’s overall perception of their sleep quality.
- Sleep latency: the amount of time it takes to fall asleep.
- Sleep duration: the total amount of sleep obtained per night.
- Sleep efficiency: the ratio of total sleep time to time spent in bed.
- Sleep disturbances: factors that interrupt sleep, such as waking up in the middle of the night, bathroom trips, and other disruptions.
- Use of sleep medication: the frequency of medication use to aid sleep.
- Daytime dysfunction: the impact of poor sleep on daily functioning, including difficulty staying awake during the day and maintaining enthusiasm for daily activities.
2.6. Salivary Cortisol and Free Testosterone
2.7. Statistics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bhat, R.; Karim, A.A. Tongkat Ali (Eurycoma longifolia Jack): A review on its ethnobotany and pharmacological importance. Fitoterapia 2010, 81, 669–679. [Google Scholar] [CrossRef] [PubMed]
- Kotirum, S.; Ismail, S.B.; Chaiyakunapruk, N. Efficacy of Tongkat Ali (Eurycoma longifolia) on erectile function improvement: Systematic review and meta-analysis of randomized controlled trials. Complement. Ther. Med. 2015, 23, 693–698. [Google Scholar] [CrossRef] [PubMed]
- Henkel, R.R.; Wang, R.; Bassett, S.H.; Chen, T.; Liu, N.; Zhu, Y.; Tambi, M.I. Tongkat Ali as a potential herbal supplement for physically active male and female seniors—A pilot study. Phytother. Res. 2014, 28, 544–550. [Google Scholar] [CrossRef] [PubMed]
- Talbott, S.M.; Talbott, J.A.; George, A.; Pugh, M. Effect of Tongkat Ali on stress hormones and psychological mood state in moderately stressed subjects. J. Int. Soc. Sports Nutr. 2013, 10, 28. [Google Scholar] [CrossRef]
- Leitao, A.E.; Vieira, M.C.S.; Pelegrini, A.; da Silva, E.L.; Guimaraes, A.C.A. A 6-month, double-blind, placebo-controlled, randomized trial to evaluate the effect of Eurycoma longifolia (Tongkat Ali) and concurrent training on erectile function and testosterone levels in androgen deficiency of aging males (ADAM). Maturitas 2021, 145, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.K.; Ooi, F.K.; Kasim, N.A.A.; Asari, M.A. Effects of Eurycoma longifolia Jack supplementation combined with resistance training on isokinetic muscular strength and power, anaerobic power, and urinary testosterone: Epitestosterone ratio in young males. Int. J. Prev. Med. 2019, 10, 118. [Google Scholar] [CrossRef]
- Evans, C.; Stull, C.; Sanders, G.; Ricci, A.; French, D.; Antonio, J.; Peacock, C.A. Weight cutting in female UFC fighters. J. Int. Soc. Sports Nutr. 2023, 20, 2247384. [Google Scholar] [CrossRef] [PubMed]
- Garcia, J.R.; Manimaleth, R.; Czartoryski, P.; Napolitano, P.; Watters, H.; Weber, C.; Alvarez-Beaton, A.; Nieto, A.C.; Patel, A.; Peacock, C. A comparative study of body composition assessment techniques: DXA and InBody 270. J. Exerc. Nutr. 2020, 3, 10. [Google Scholar]
- Czartoryski, P.; Garcia, J.; Manimaleth, R.; Napolitano, P.; Watters, H.; Weber, C.; Alvarez-Beaton, A.; Nieto, A.C.; Patel, A.; Peacock, C. Body composition assessment: A comparison of the DXA, Inbody 270, and Omron. J. Exerc. Nutr. 2020, 3, 1. [Google Scholar]
- Yoshihara, K.; Hiramoto, T.; Sudo, N.; Kubo, C. Profile of mood states and stress-related biochemical indices in long-term yoga practitioners. Biopsychosoc. Med. 2011, 5, 6. [Google Scholar] [CrossRef]
- Lasaite, L.; Ostrauskas, R.; Zalinkevicius, R.; Jurgeviciene, N.; Radzeviciene, L. Profile of mood states in adult type 1 diabetes mellitus men and women with disease onset in childhood and in adulthood. J. Pediatr. Endocrinol. Metab. 2015, 28, 279–285. [Google Scholar] [CrossRef] [PubMed]
- Antonio, J.; Curtis, J.M. No “jitters” but no energy from a commercially available energy drink. J. Sports Neurosci. 2023, 1, 14. [Google Scholar]
- Zitser, J.; Allen, I.E.; Falgas, N.; Le, M.M.; Neylan, T.C.; Kramer, J.H.; Walsh, C.M. Pittsburgh Sleep Quality Index (PSQI) responses are modulated by total sleep time and wake after sleep onset in healthy older adults. PLoS ONE 2022, 17, e0270095. [Google Scholar] [CrossRef] [PubMed]
- Tambi, M.I.B.M.; Imran, M.K.; Henkel, R.R. Standardised water-soluble extract of Eurycoma longifolia, Tongkat ali, as testosterone booster for managing men with late-onset hypogonadism? Andrologia 2012, 44, 226–230. [Google Scholar] [CrossRef] [PubMed]
- Zakaria, A.Z.; Washif, J.A.; Lim, B.H.; Nosaka, K. Effects of Eurycoma longifolia Jack supplementation on eccentric leg press exercise-induced muscle damage in rugby players. Biol. Sport 2023, 40, 691–697. [Google Scholar] [CrossRef] [PubMed]
- Chinnappan, S.M.; George, A.; Pandey, P.; Narke, G.; Choudhary, Y.K. Effect of Eurycoma longifolia standardised aqueous root extract—Physta® on testosterone levels and quality of life in ageing male subjects: A randomised, double-blind, placebo-controlled multicentre study. Food Nutr. Res. 2021, 65, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Chan, K.Q.; Stewart, C.; Chester, N.; Hamzah, S.H.; Yusof, A. The effect of Eurycoma Longifolia on the regulation of reproductive hormones in young males. Andrologia 2021, 53, e14001. [Google Scholar] [CrossRef] [PubMed]
- Chan, K. Effects of Eurycoma longifolia Supplementation: An Evaluation of Cell Growth, Exercise Performance and Wellbeing in Adult Males. Ph.D. Thesis, Liverpool John Moores University, Liverpool, UK, 2021. [Google Scholar]
- Ismail, S.B.; Wan Mohammad, W.M.Z.; George, A.; Nik Hussain, N.H.; Musthapa Kamal, Z.M.; Liske, E. Randomized clinical trial on the use of PHYSTA freeze-dried water extract of Eurycoma longifolia for the improvement of quality of life and sexual well-being in men. Evid.-Based Complement. Altern. Med. 2012, 2012, 429268. [Google Scholar] [CrossRef]
- Chen, C.K.; Mohamad, W.M.Z.W.; Ooi, F.K.; Ismail, S.B.; Abdullah, M.R.; George, A. Supplementation of Eurycoma longifolia Jack extract for 6 weeks does not affect urinary testosterone: Epitestosterone ratio, liver and renal functions in male recreational athletes. Int. J. Prev. Med. 2014, 5, 728. [Google Scholar] [PubMed] [PubMed Central]
- Leisegang, K.; Finelli, R.; Sikka, S.C.; Panner Selvam, M.K. Eurycoma longifolia (Jack) Improves Serum Total Testosterone in Men: A Systematic Review and Meta-Analysis of Clinical Trials. Medicina 2022, 58, 1047. [Google Scholar] [CrossRef]
- Ono, T.; Nishino, N.; Iwai, Y.; Iwai, Y.; Sakai, N.; Kuroki, Y.; Nishino, S. Eurycoma longifolia (Tongkat Ali) enhances wakefulness during active periods but facilitates sleep during resting periods in C57BL/6 mice. Eur. J. Neurosci. 2023, 58, 4298–4309. [Google Scholar] [CrossRef] [PubMed]
- Yusof, S.M.; Zakaria, Z.; Karim, A.A.H.; Aiman, S.; Kadir, Z. Enhancement Effects of Tongkat Ali (Eurycoma longifolia) Supplementation on Performance Functions Following Strength Training in Middle-Aged Women. In Proceedings of the 2nd International Colloquium on Sports Science, Exercise, Engineering and Technology (ICoSSEET 2015), Kota Kinabalu, Malaysia, 20–22 November 2015; pp. 3–13. [Google Scholar]
- Lazarev, A.; Bezuglov, E. Testosterone boosters intake in athletes: Current evidence and further directions. Endocrines 2021, 2, 109–120. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tongkat Ali | Placebo | p-Value | |
|---|---|---|---|
| Age, years | 37 ± 14 | 30 ± 12 | 0.1127 |
| Height, cm | 174 ± 8 | 170 ± 14 | 0.3844 |
| Total number of years of training | 19 ± 15 | 9 ± 9 | 0.0177 * |
| Average hours of aerobic exercise/week | 4 ± 3 | 3 ± 3 | 0.5244 |
| Average hours of resistance training/week | 4 ± 3 | 4 ± 3 | 0.6440 |
| Other exercise hours/week | 1 ± 2 | 1 ± 2 | 0.4224 |
| Tongkat Ali | Placebo | p-Value Delta | |||||
|---|---|---|---|---|---|---|---|
| Pre | Post | Delta | Pre | Post | Delta | ||
| BM, kg | 79.9 ± 13.1 | 78.9 ± 13.4 | −1.0 ± 2.3 | 75.7 ± 19.6 | 75.6 ± 19.2 | −0.1 ± 1.2 | 0.1585 |
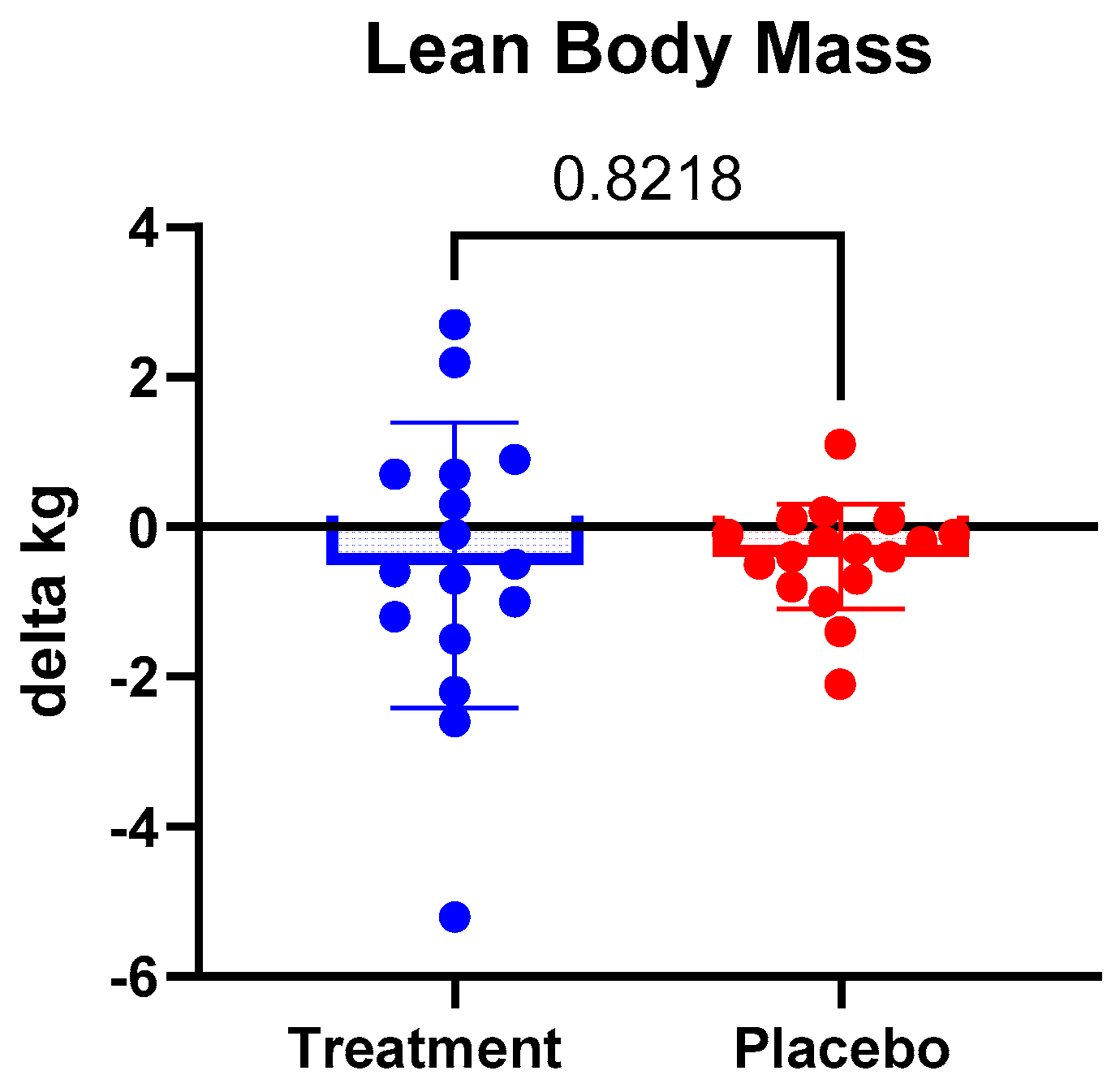
| LBM, kg | 63.9 ± 12.0 | 63.4 ± 12.5 | −0.5 ± 1.9 | 60.6 ± 15.5 | 60.2 ± 15.5 * | −0.4 ± 0.7 | 0.8218 |
| Fat mass, kg | 16.1 ± 5.2 | 15.5 ± 5.4 | −0.5 ± 1.6 | 15.1 ± 8.8 | 15.3 ± 8.6 | 0.3 ± 1.0 | 0.0956 |
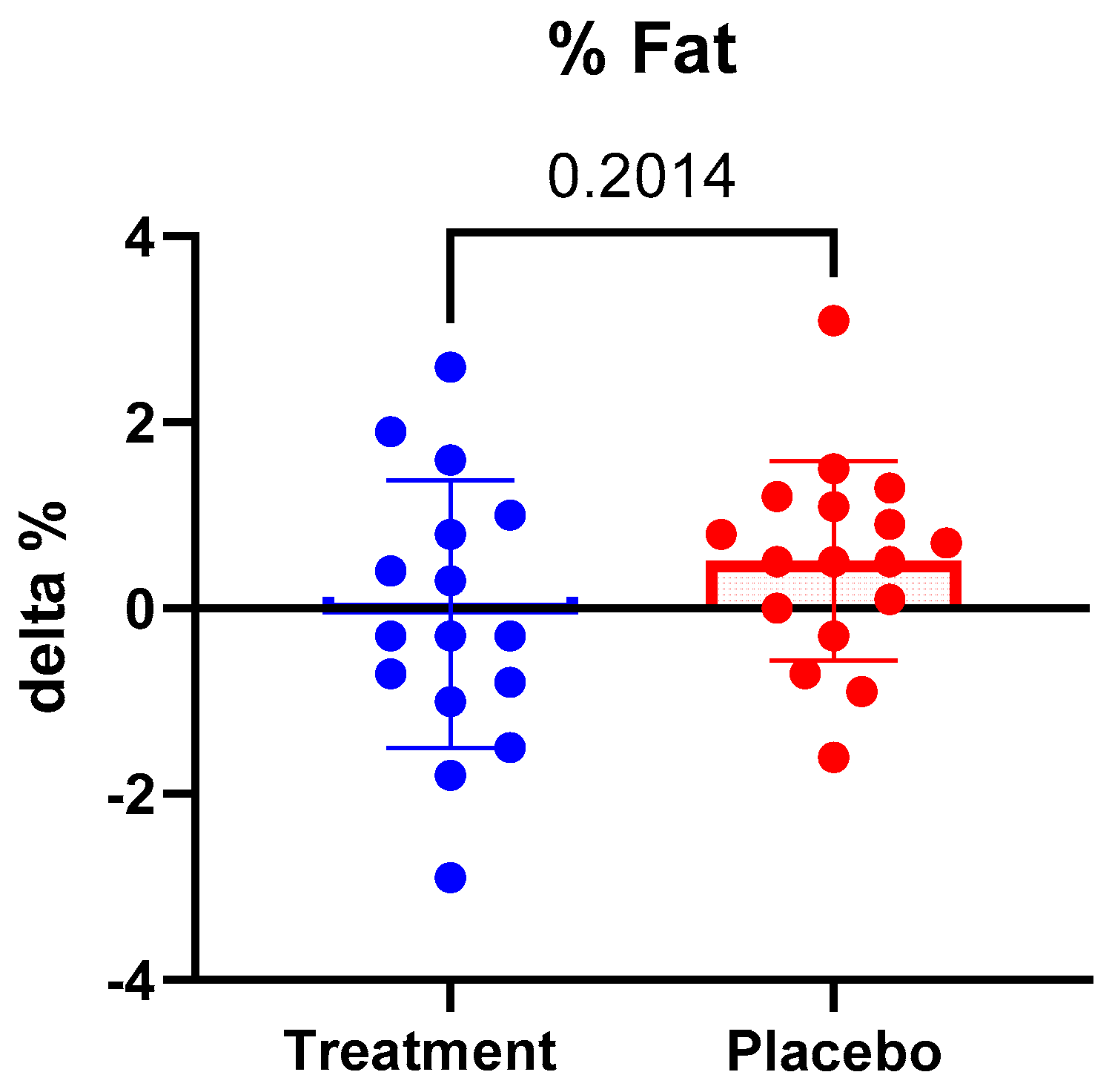
| % Body fat | 19.9 ± 5.6 | 19.8 ± 6.3 | −0.1 ± 1.4 | 19.7 ± 7.6 | 20.2 ± 7.7 * | 0.5 ± 1.1 | 0.2014 |
| TBW, L | 46.5 ± 9.0 | 46.4 ± 9.2 | −0.1 ± 1.1 | 43.0 ± 12.3 | 42.5 ± 11.0 | −0.5 ± 3.3 | 0.6969 |
| Tongkat Ali | Placebo | p-Value Delta | |||||
|---|---|---|---|---|---|---|---|
| Pre | Post | Delta | Pre | Post | Delta | ||
| TMDS | 29 ± 39 | 11 ± 23 | −18 ± 37 | 16 ± 23 | 6 ± 19 | −10 ± 24 | 0.4744 |
| PSQI | 6.1 ± 2.1 | 5.5 ± 2.2 | −0.6 ± 1.8 | 6.2 ± 2.5 | 5.5 ± 2.2 | −0.6 ± 1.7 | 0.8886 |
| Peak HG, kg | 48 ± 9 | 48 ± 11 | −1 ± 7 | 45 ± 15 | 45 ± 14 | 1 ± 2 | 0.5554 |
| Tongkat Ali | |||
|---|---|---|---|
| Pre | Post | Delta | |
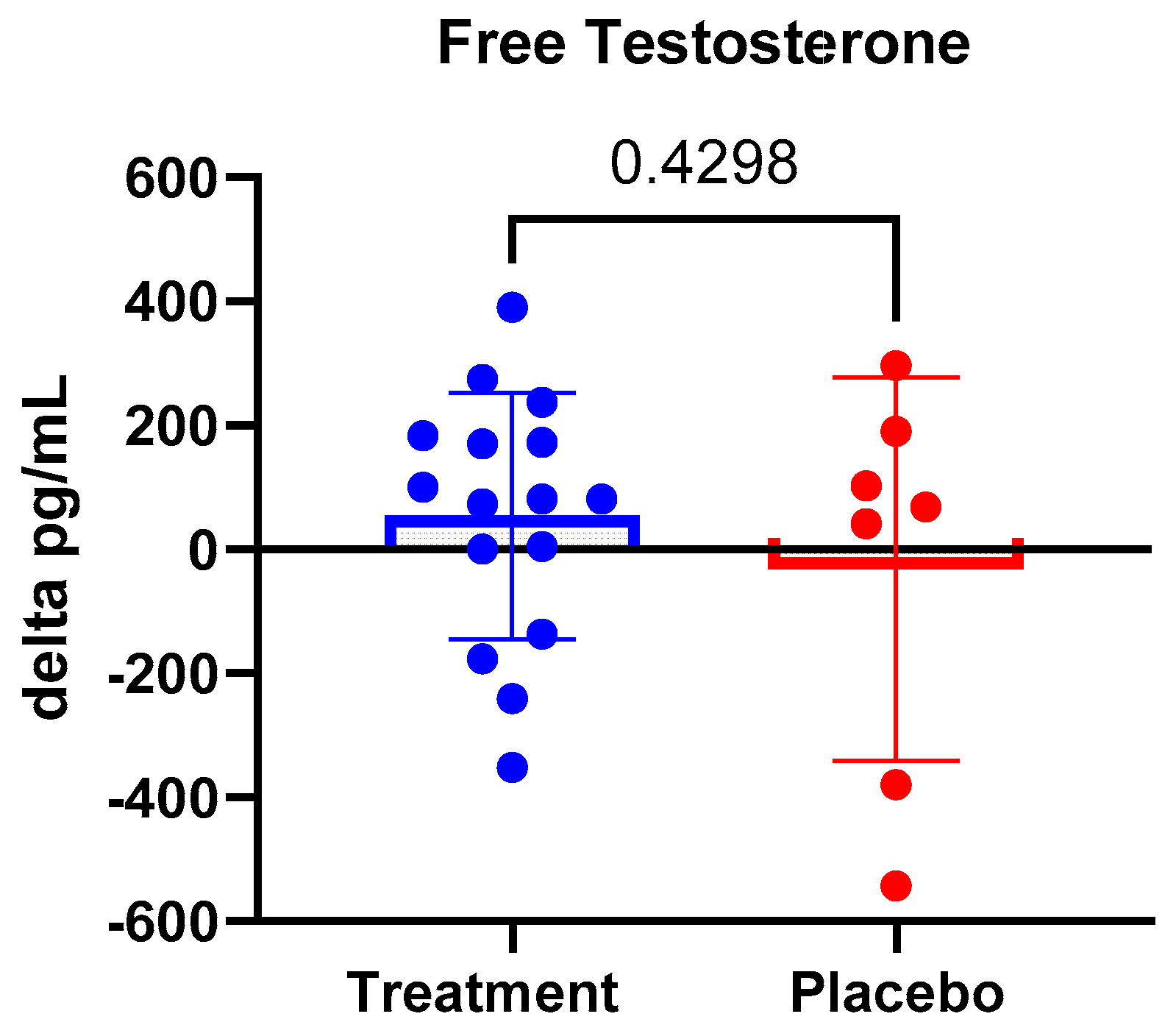
| Free testosterone, pg/mL | 247 ± 126 | 305 ± 180 | 58 ± 205 |
| Cortisol, mcg/dL | 0.206 ± 0.094 | 0.253 ± 0.167 | 0.047 ± 0.210 |
| Placebo | |||
| Pre | Post | Delta | |
| Free testosterone, pg/mL | 283 ± 262 | 251 ± 172 | −32 ± 309 |
| Cortisol, mcg/dL | 0.183 ± 0.033 | 0.225 ± 0.147 | 0.042 ± 0.162 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Antonio, J.; Evans, C.; Pereira, F.; Thakkar, H.; Miriyala, V.; Rocanelli, R.; Castillo, C.; Andal, A.; Rojas, J.; Santana, J.C.; et al. The Effect of Tongkat Ali Supplementation on Body Composition in Exercise-Trained Males and Females. Appl. Sci. 2024, 14, 4372. https://doi.org/10.3390/app14114372
Antonio J, Evans C, Pereira F, Thakkar H, Miriyala V, Rocanelli R, Castillo C, Andal A, Rojas J, Santana JC, et al. The Effect of Tongkat Ali Supplementation on Body Composition in Exercise-Trained Males and Females. Applied Sciences. 2024; 14(11):4372. https://doi.org/10.3390/app14114372
Chicago/Turabian StyleAntonio, Jose, Cassandra Evans, Flavia Pereira, Hena Thakkar, Viraaj Miriyala, Robert Rocanelli, Cesar Castillo, Alyana Andal, Jose Rojas, Juan Carlos Santana, and et al. 2024. "The Effect of Tongkat Ali Supplementation on Body Composition in Exercise-Trained Males and Females" Applied Sciences 14, no. 11: 4372. https://doi.org/10.3390/app14114372
APA StyleAntonio, J., Evans, C., Pereira, F., Thakkar, H., Miriyala, V., Rocanelli, R., Castillo, C., Andal, A., Rojas, J., Santana, J. C., Jiannine, L., Tartar, J., & Curtis, J. (2024). The Effect of Tongkat Ali Supplementation on Body Composition in Exercise-Trained Males and Females. Applied Sciences, 14(11), 4372. https://doi.org/10.3390/app14114372