
Three-Dimensional Pulp Volume Analysis in Lip and Palate Cleft Population

 ,
,  ,
,  , , ,
, , ,  ,
, 
Abstract
1. Introduction
- (1)
- Radiocarbon dating [12]: radiocarbon dating is a technique used to determine the age of organic materials by measuring the amount of carbon-14 present;
- (2)
- Dental analysis [13]: dental analysis is a method of determining age by examining the development and wear of teeth. The teeth develop in a predictable pattern, and the amount of wear on the teeth can give an indication of the person’s age;
- (3)
- Bone analysis [14]: the bones of the body develop and fuse at different ages, and by examining the bones, the age of the individual can be estimated;
- (4)
- Radiographic analysis [15]: radiographic analysis is a technique used to examine the internal structure of the body. By examining X-rays or other imaging techniques, the age of the individual can be estimated based on the development of certain bones or the presence of certain features;
- (5)
- Hormone analysis [16]: Hormone levels change as a person ages, and by examining the levels of certain hormones, the age of the individual can be estimated.
2. Materials and Methods
2.1. Study Design
2.2. Selection Criteria
2.3. Image Acquisition and Segmentation
2.4. Inter- and Intra-Observer Agreement
2.5. Statistical Analysis
3. Results
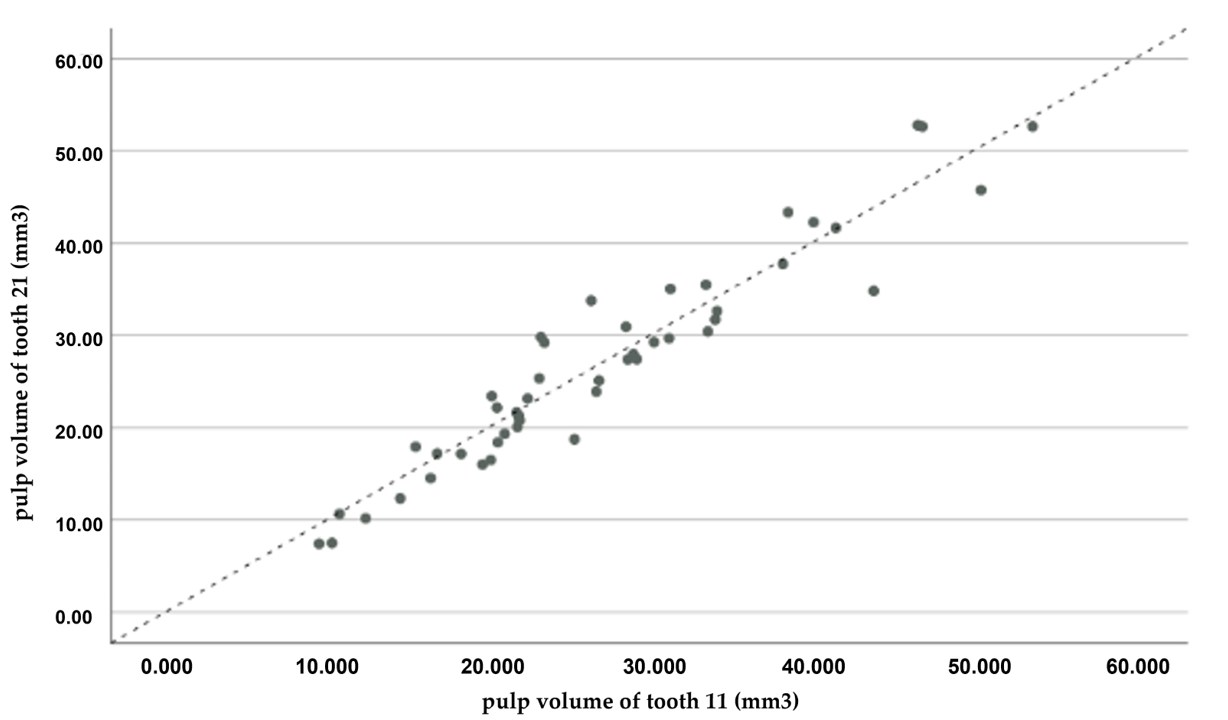
3.1. Interobserver Agreement
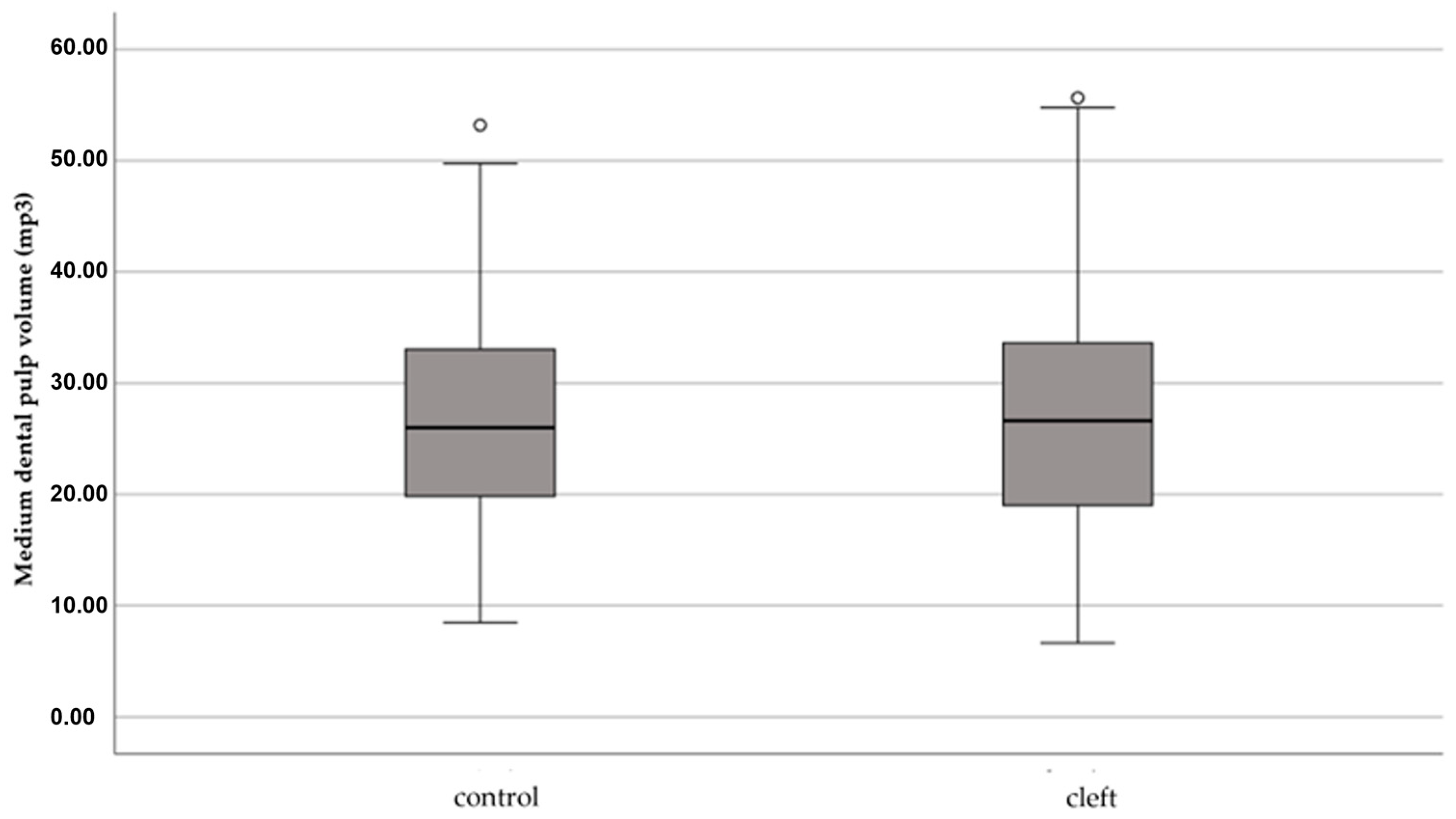
3.2. Pulp Volume Comparison between Patients with and without CLP
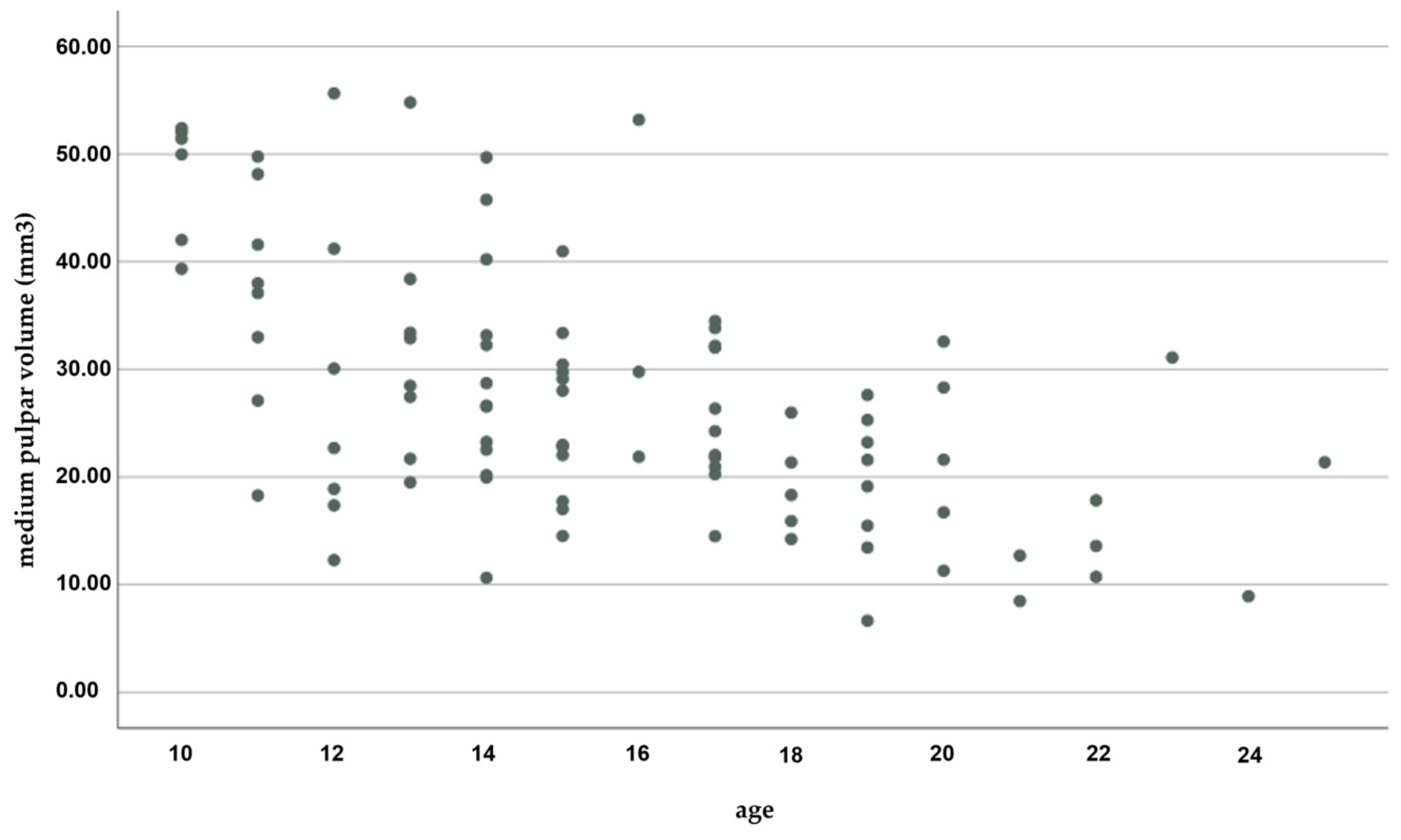
3.3. Comparison of Pulp Volume Regarding Sex and Age
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gustafson, G.; Malmö, D.O. Age Determinations on Teeth. J. Am. Dent. Assoc. 1950, 41, 45–54. [Google Scholar] [CrossRef] [PubMed]
- Arora, J.; Talwar, I.; Sahni, D.; Rattan, V. Secondary Dentine as a Sole Parameter for Age Estimation: Comparison and Reliability of Qualitative and Quantitative Methods among North Western Adult Indians. Egypt. J. Forensic Sci. 2016, 6, 170–178. [Google Scholar] [CrossRef]
- Maples, W.R. An Improved Technique Using Dental Histology for Estimation of Adult Age. J. Forensic Sci. 1978, 23, 764–770. [Google Scholar] [CrossRef] [PubMed]
- Solheim, T. A New Method for Dental Age Estimation in Adults. Forensic Sci. Int. 1993, 59, 137–147. [Google Scholar] [CrossRef] [PubMed]
- Agematsu, H.; Someda, H.; Hashimoto, M.; Matsunaga, S.; Abe, S.; Kim, H.-J.; Koyama, T.; Naito, H.; Ishida, R.; Ide, Y. Three-Dimensional Observation of Decrease in Pulp Cavity Volume Using Micro-CT: Age-Related Change. Bull. Tokyo Dent. Coll. 2010, 51, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Gupta, P. Human Age Estimation from Tooth Cementum and Dentin. J. Clin. Diagn. Res. 2014, 8, ZC07. [Google Scholar] [CrossRef] [PubMed]
- Kvaal, S.I.; Kolltveit, K.M.; Thomsen, I.O.; Solheim, T. Age Estimation of Adults from Dental Radiographs. Forensic Sci. Int. 1995, 74, 175–185. [Google Scholar] [CrossRef]
- Agarwal, N.; Ahuja, P.; Sinha, A.; Singh, A. Age Estimation Using Maxillary Central Incisors: A Radiographic Study. J. Forensic Dent. Sci. 2012, 4, 97. [Google Scholar] [CrossRef]
- Andrade, V.M.; Fontenele, R.C.; de Souza, A.C.; de Almeida, C.A.; Vieira, A.C.; Groppo, F.C.; Freitas, D.Q.; Junior, E.D. Age and Sex Estimation Based on Pulp Cavity Volume Using Cone Beam Computed Tomography: Development and Validation of Formulas in a Brazilian Sample. Dentomaxillofac. Radiol. 2019, 48, 20190053. [Google Scholar] [CrossRef]
- Lee, S.-M.; Oh, S.; Kim, J.; Kim, Y.-M.; Choi, Y.-K.; Kwak, H.H.; Kim, Y.-I. Age Estimation Using the Maxillary Canine Pulp/Tooth Ratio in Korean Adults: A CBCT Buccolingual and Horizontal Section Image Analysis. J. Forensic Radiol. Imaging 2017, 9, 1–5. [Google Scholar] [CrossRef]
- Ge, Z.; Yang, P.; Li, G.; Zhang, J.; Ma, X. Age Estimation Based on Pulp Cavity/Chamber Volume of 13 Types of Tooth from Cone Beam Computed Tomography Images. Int. J. Leg. Med. 2016, 130, 1159–1167. [Google Scholar] [CrossRef]
- Ubelaker, D.H. Radiocarbon Analysis of Human Remains: A Review of Forensic Applications. J. Forensic Sci. 2014, 59, 1466–1472. [Google Scholar] [CrossRef] [PubMed]
- Hillson, S. Dental Pathology. In Biological Anthropology of the Human Skeleton; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2018; pp. 293–333. [Google Scholar]
- Buikstra, J.E.; Ubelaker, D.H. Standards for Data Collection from Human Skeletal Remains; Arkansas Archeological Survey Research Series; University of Arkansas: Fayetteville, AR, USA, 2012; Volume 44. [Google Scholar]
- Manini, A.; Savino, G.; Calliada, F. Radiographic Anatomy; Springer: Berlin/Heidelberg, Germany, 2020. [Google Scholar]
- Vermeulen, A.; Kaufman, J.M. Ageing of the Hypothalamo-Pituitary-Testicular Axis in Men. Horm. Res. 1995, 43, 25–28. [Google Scholar] [CrossRef] [PubMed]
- Corral, C.; García, F.; García, J.; León, P.; Herrera, A.; Martínez, C.; Moreno, F. Chronological versus Dental Age in Subjects from 5 to 19 Years: A Comparative Study with Forensic Implications. Colomb. Médica 2010, 41, 215–223. [Google Scholar] [CrossRef]
- Vodanović, M.; Dumančić, J.; Galić, I.; Savić Pavičin, I.; Petrovečki, M.; Cameriere, R.; Brkić, H. Age Estimation in Archaeological Skeletal Remains: Evaluation of Four Non-Destructive Age Calculation Methods. J. Forensic Odontostomatol. 2011, 29, 14–21. [Google Scholar] [PubMed]
- Pereira, C.P.; Caldas, R.; Pestana, D. Legal Medical Age Estimation in Portuguese Adult Cadavers: Evaluation of the Accuracy of Forensic Dental Invasive and Non-Invasive Methods. J. Forensic Sci. Criminol. 2013, 1, 1. [Google Scholar] [CrossRef]
- Afify, M.M. Age Estimation from Pulp/Tooth Area Ratio in Three Mandibular Teeth by Panoramic Radiographs: Study of an Egyptian Sample. J. Forensic Res. 2014, 5, 2. [Google Scholar] [CrossRef]
- Ge, Z.; Ma, R.; Li, G.; Zhang, J.; Ma, X. Age Estimation Based on Pulp Chamber Volume of First Molars from Cone-Beam Computed Tomography Images. Forensic Sci. Int. 2015, 253, 133.e1–133.e7. [Google Scholar] [CrossRef]
- Tannure, P.N.; Oliveira, C.A.G.R.; Maia, L.C.; Vieira, A.R.; Granjeiro, J.M.; de Castro Costa, M. Prevalence of Dental Anomalies in Nonsyndromic Individuals with Cleft Lip and Palate: A Systematic Review and Meta-Analysis. Cleft Palate-Craniofacial J. 2012, 49, 194–200. [Google Scholar] [CrossRef]
- de Assis, I.O.; de Lavôr, J.R.; Cavalcante, B.G.N.; Lacerda, R.H.W.; Vieira, A.R. Pulp Enlargement in Individuals Born with Cleft Lip and Palate Pulp, a Radiographic Study from the Cleft Lip and Palate Service of Paraiba, Brazil. Eur. Arch. Paediatr. Dent. 2021, 22, 1101–1106. [Google Scholar] [CrossRef]
- Küchler, E.C.; da Motta, L.G.; Vieira, A.R.; Granjeiro, J.M. Side of Dental Anomalies and Taurodontism as Potential Clinical Markers for Cleft Subphenotypes. Cleft Palate-Craniofacial J. 2011, 48, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Jamal, G.A.A.; Hazza’a, A.M.; Rawashdeh, M.A. Prevalence of Dental Anomalies in a Population of Cleft Lip and Palate Patients. Cleft Palate-Craniofacial J. 2010, 47, 413–420. [Google Scholar] [CrossRef]
- Cassolato, S.F.; Ross, B.; Daskalogiannakis, J.; Noble, J.; Tompson, B. Treatment of Dental Anomalies in Children with Complete Unilateral Cleft Lip and Palate at Sickkids Hospital, Toronto. Cleft Palate-Craniofacial J. 2009, 46, 166–172. [Google Scholar] [CrossRef] [PubMed]
- Smith, B.G.; Knight, J.K. An Index for Measuring the Wear of Teeth. Br. Dent. J. 1984, 156, 435–438. [Google Scholar] [CrossRef] [PubMed]
- Biuki, N.; Razi, T.; Faramarzi, M. Relationship between Pulp-Tooth Volume Ratios and Chronological Age in Different Anterior Teeth on CBCT. J. Clin. Exp. Dent. 2017, 9, e688–e693. [Google Scholar] [CrossRef]
- Alvesalo, L.; Tammisalo, E.; Townsend, G. Upper Central Incisor and Canine Tooth Crown Size in 47,XXY Males. J. Dent. Res. 1991, 70, 1057–1060. [Google Scholar] [CrossRef] [PubMed]
- de Angelis, D.; Gibelli, D.; Gaudio, D.; Cipriani Noce, F.; Guercini, N.; Varvara, G.; Sguazza, E.; Sforza, C.; Cattaneo, C. Sexual Dimorphism of Canine Volume: A Pilot Study. Leg. Med. 2015, 17, 163–166. [Google Scholar] [CrossRef]
- Eslami, N.; Majidi, M.R.; Aliakbarian, M.; Hasanzadeh, N. Prevalence of Dental Anomalies in Patients with Cleft Lip and Palate. J. Craniofacial Surg. 2013, 24, 1695–1698. [Google Scholar] [CrossRef]
- Konstantonis, D.; Alexandropoulos, A.; Konstantoni, N.; Nassika, M. A Cross-Sectional Analysis of the Prevalence of Tooth Agenesis and Structural Dental Anomalies in Association with Cleft Type in Non-Syndromic Oral Cleft Patients. Prog. Orthod. 2017, 18, 20. [Google Scholar] [CrossRef]
- Tsai, T.-P.; Huang, C.-S.; Huang, C.-C.; See, L.-C. Distribution Patterns of Primary and Permanent Dentition in Children with Unilateral Complete Cleft Lip and Palate. Cleft Palate-Craniofacial J. 1998, 35, 154–160. [Google Scholar] [CrossRef]
- Akcam, M.O.; Evirgen, S.; Uslu, O.; Memikoglu, U.T. Dental Anomalies in Individuals with Cleft Lip and/or Palate. Eur. J. Orthod. 2010, 32, 207–213. [Google Scholar] [CrossRef] [PubMed]
- Guler, A.Y.; Isik, B.K.; Esen, A.; Menziletoglu, D. Assessment of Pulp Volume Changes after Surgically Assisted Rapid Palatal Expansion. J. Stomatol. Oral Maxillofac. Surg. 2021, 122, 263–266. [Google Scholar] [CrossRef] [PubMed]
- Popp, T.W.; Årtun, J.; Linge, L. Pulpal Response to Orthodontic Tooth Movement in Adolescents: A Radiographic Study. Am. J. Orthod. Dentofac. Orthop. 1992, 101, 228–233. [Google Scholar] [CrossRef] [PubMed]
- Venkatesh, S.; Ajmera, S.; Ganeshkar, S.V. Volumetric Pulp Changes after Orthodontic Treatment Determined by Cone-Beam Computed Tomography. J. Endod. 2014, 40, 1758–1763. [Google Scholar] [CrossRef]
- Terlemez, A.; Alan, R.; Gezgin, O. Evaluation of the Periodontal Disease Effect on Pulp Volume. J. Endod. 2018, 44, 111–114. [Google Scholar] [CrossRef]
- Gaggl, A.; Schultes, G.; Kärcher, H.; Mossböck, R. Periodontal Disease in Patients with Cleft Palate and Patients with Unilateral and Bilateral Clefts of Lip, Palate, and Alveolus. J. Periodontol. 1999, 70, 171–178. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| α = 0.01 | α = 0.05 | α = 0.10 | |
|---|---|---|---|
| 1 − β = 0.80 | 10 | 7 | 6 |
| 1 − β = 0.85 | 11 | 8 | 6 |
| 1 − β = 0.90 | 13 | 9 | 7 |
| β = 0.80 | |||
| β = 0.85 | |||
| β = 0.90 |
| Control (47) | CLP (47) | p | |
|---|---|---|---|
| sex (M/F) | 31/16 (66.0%/34.0%) | 31/16 (66.0%/34.0%) | 1.000 £ |
| Age | 16.1; 16 (3.6) 13.0/19.0 | 14.8; 14 (3.5) 12.0/17.0 | 0.065 § |
| Masculine (61) | Feminine (33) | p | |
|---|---|---|---|
| Volume (mm3) | 30.8; 29 (11.3) 22.5/37.1 | 21.4; 19 (10.6) 14.4/22.9 | <0.001 £ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Francisco, I.; Travassos, R.; Marques, F.; Ribeiro, M.P.; Rodrigues, M.; Quaresma, P.; Caramelo, F.; Marto, C.M.; Paula, A.B.; Nunes, C.; et al. Three-Dimensional Pulp Volume Analysis in Lip and Palate Cleft Population. Appl. Sci. 2023, 13, 3728. https://doi.org/10.3390/app13063728
Francisco I, Travassos R, Marques F, Ribeiro MP, Rodrigues M, Quaresma P, Caramelo F, Marto CM, Paula AB, Nunes C, et al. Three-Dimensional Pulp Volume Analysis in Lip and Palate Cleft Population. Applied Sciences. 2023; 13(6):3728. https://doi.org/10.3390/app13063728
Chicago/Turabian StyleFrancisco, Inês, Raquel Travassos, Filipa Marques, Madalena Prata Ribeiro, Mariana Rodrigues, Patrícia Quaresma, Francisco Caramelo, Carlos Miguel Marto, Anabela Baptista Paula, Catarina Nunes, and et al. 2023. "Three-Dimensional Pulp Volume Analysis in Lip and Palate Cleft Population" Applied Sciences 13, no. 6: 3728. https://doi.org/10.3390/app13063728
APA StyleFrancisco, I., Travassos, R., Marques, F., Ribeiro, M. P., Rodrigues, M., Quaresma, P., Caramelo, F., Marto, C. M., Paula, A. B., Nunes, C., & Vale, F. (2023). Three-Dimensional Pulp Volume Analysis in Lip and Palate Cleft Population. Applied Sciences, 13(6), 3728. https://doi.org/10.3390/app13063728