
Recent Advances in Artificial Intelligence-Assisted Ultrasound Scanning

 , , and
, , and 
Abstract
1. Introduction
1.1. Current Challenges of Ultrasound Imaging
- Operator dependency. As US imaging depends on the ability of the operator to position the transducer and interpret the images correctly, it can be difficult to obtain consistent and reliable results from different operators, requiring long and specialized training.
- Subjectivity in image interpretation. The interpretation of the US images is quite subjective. Unlike other imaging modalities, which produce objective, quantitative data, the interpretation of US images depends heavily on the experience and skills of the person performing the scan. This can lead to variability in the accuracy and reliability of the images, particularly when they are used for diagnostic purposes.
- Limited penetration depth, which limits its use for imaging deep structures in the body, and an inability to penetrate certain tissues or structures, such as bone and air-filled cavities.
- Limited quality of US images. Ultrasound images are typically less detailed than those produced by other modalities. This can make it difficult to accurately diagnose certain conditions, particularly when the structures being imaged are small or located deep within the body.
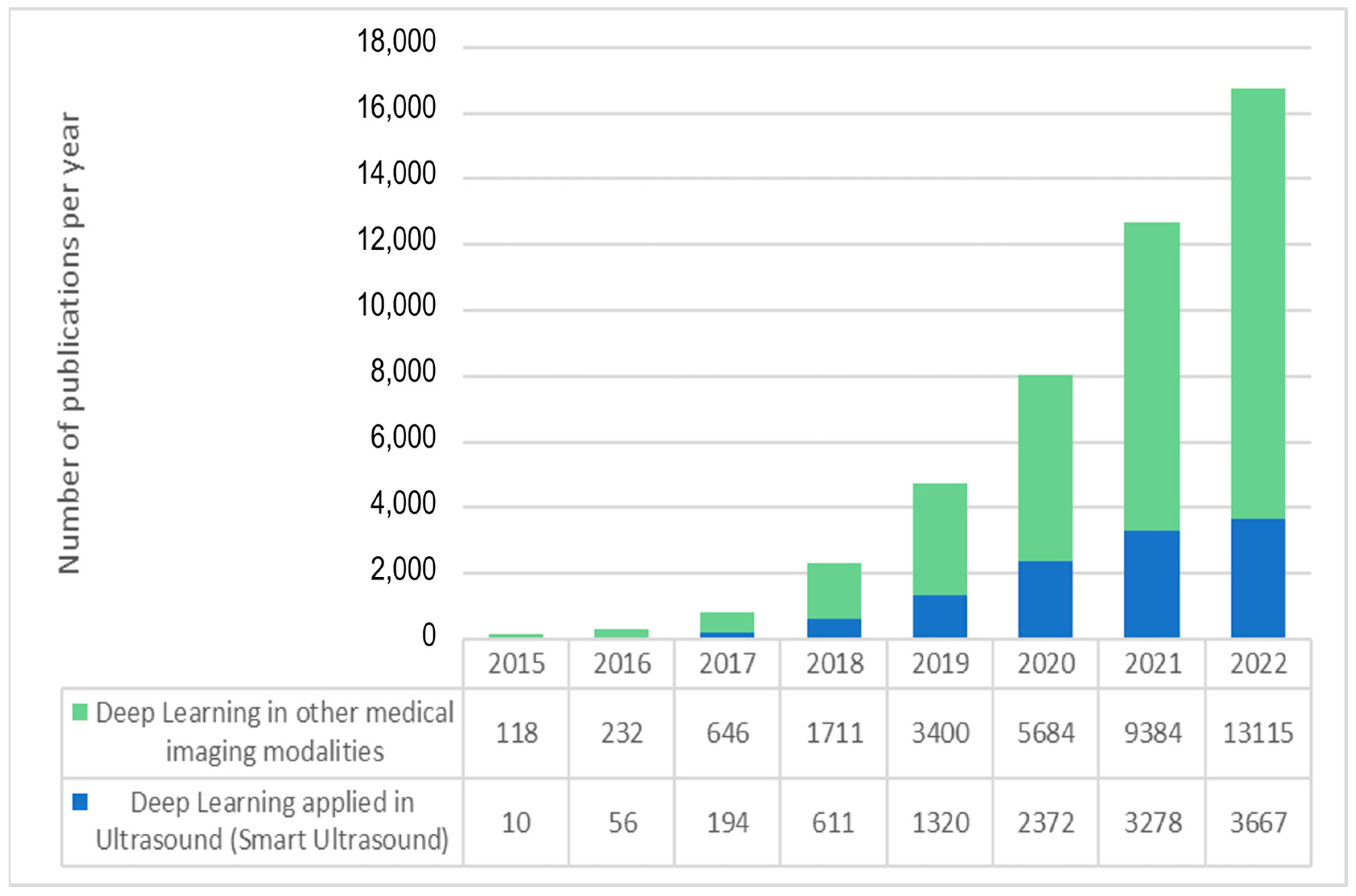
1.2. The Deep-Learning Revolution in Ultrasound Imaging
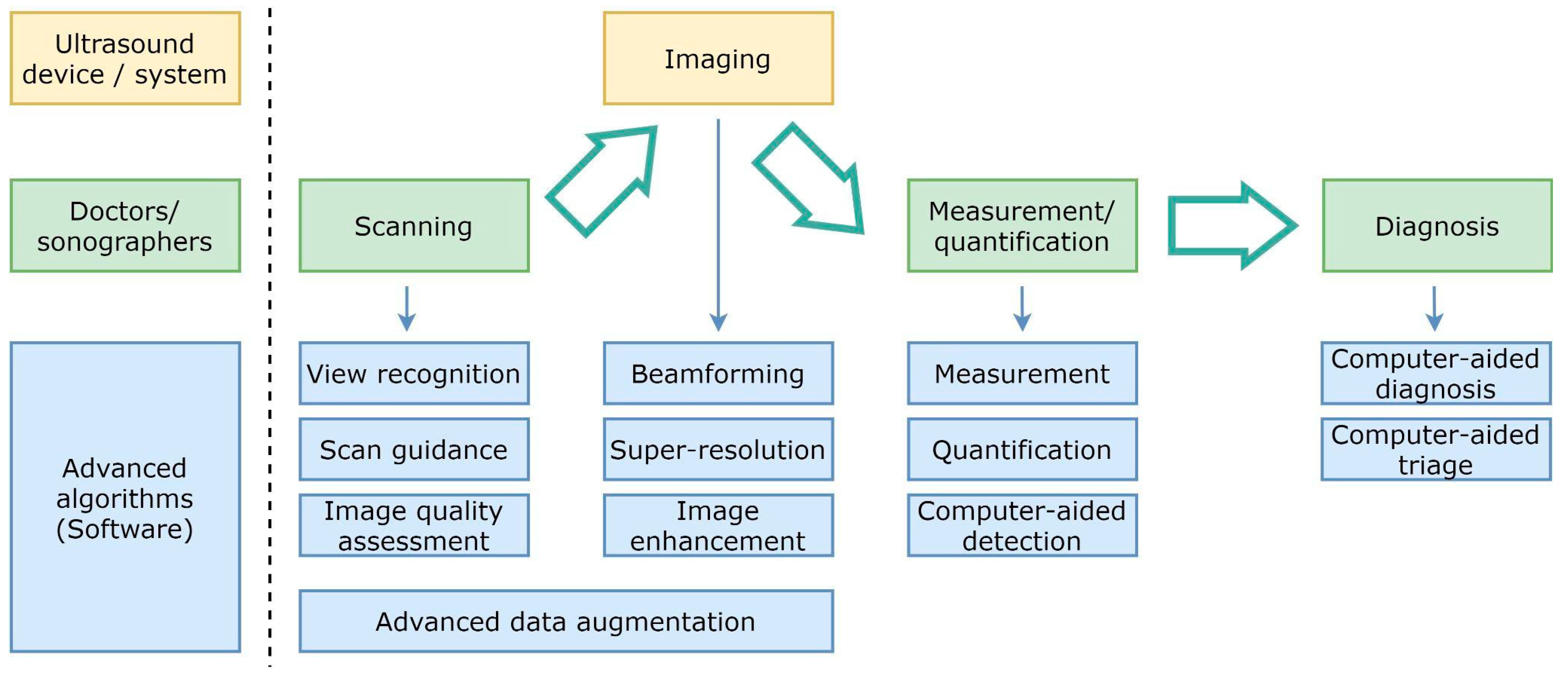
1.3. Main Applications of AI in US Imaging
- The application of machine learning techniques to ultrasound image formation has a large margin of improvement to provide less blurry and more significant images, even by creating new ultrasound medical imaging modalities [11]. New approaches in beamforming, super-resolution, and image enhancement require modifications to hardware elements, which are usually more ambitious than more straightforward software post-processing approaches. In spite of the more difficult adoption, many research advances are overcoming traditional and simple reconstruction algorithms, which translate physical measurements of ultrasound waves into images in the display. The more computational power available in medical devices, the more sophisticated real-time solutions may enrich the different ultrasound imaging modalities.
- AI algorithms can help to reduce the steep learning curve in ultrasound scanning by assisting physicians, nurses, and technicians to perform full examinations, as is shown in detail in the following sections.
- Image processing algorithms for measurement, quantification, and computer-aided detection have left behind traditional feature engineering, and the most competitive solutions in ultrasound imaging take advantage of deep learning-based approaches.
- Finally, computer-assisted diagnosis, triage, detection, and quantification have also attracted the research community’s attention because of their significant impact on reducing physicians’ workload.
1.4. Computer-Assisted Ultrasound Scanning
- The operator must place the transducer on the patient’s body surface at precise locations to allow the signal to reach the desired organ and bounce back to the sensor. Bones (such as the ribs) and certain organs (such as the lungs) are opaque to pressure waves, so they must be avoided to reach the target organ.
- Both the exact location of the acoustic windows and the force to be exerted with the probe slightly depend on the patient’s morphology.
- In conventional US imaging, the operator manually moves the transducer, obtaining a series of two-dimensional (2D) images of the target region. Then, he/she performs a mental 3D reconstruction of the underlying anatomy based on the content and the movement patterns used. Physicians have defined a set of protocols to obtain standard views that contain most of the relevant features in the 2D cutting plane of the organ. However, such views are not easy to locate for a person with limited training.
- Ultrasound images are noisy and are affected by signal dropout, attenuation, speckle, and acoustic shadows. So, the operator does not always perceive the anatomy as clearly as one would like. Moreover, a soft-textured image free of noise due to excessive filtering or incorrect gain settings is useless from a clinical point of view.
2. Standard Planes Recognition with AI
2.1. Scan Plane Detection

{kind=link}
{kind=link}
| Scan Plane Detection, Plane Classification, and Organ Identification | |||||
|---|---|---|---|---|---|
| Reference | Target Organ | # Cases | US System | AI Model | Results |
| R.-F. Chang et al. [14] | Breast | 250 images | ATL HDI 3000 | SVM | Accuracy 95.4% |
| C. P. Bridge et al. [15] | Heart | 91 videos from 12 subjects | GE Voluson E8 | RF | Classification error <20% |
| M. W. Attia et al. [16] | Kidney | 66 images | Several (Databases) | Multilayer ANN | Accuracy 97%. |
| H. Chen et al. [17] | Hrain, Stomach, Spine, Heart | 300 training 331 evaluation | Siemens Acuson Sequoia 512 US | RNN | AUC 0.94 |
| H. Chen et al. [18] | Fetal Abdomen | 20,660 images | Unknown | CNN | Accuracy 90.4% |
| D. Ni et al. [19] | Fetal Abdomen | 1664 images 100 videos | Siemens Acuson Sequoia 512 | AdaBoost, Selective Search (SSD/SSSD) | Accuracy 81% (SSSD) |
| D. Ni et al. [20] | Fetal Abdomen | 1995 images | Siemens Acuson Sequoia 512 | RF + SVM | Accuracy 85.6% AUC >0.98 |
| B. Rahmatullah et al. [21] | Fetal Abdomen | 2384 images | Philips HD9 | AdaBoost | Accuracy 80.7% |
| B. Rahmatullah et al. [22] | Fetal Abdomen | 8749 images | Philips HD9 | Local Phase Feature | AUC 0.88 |
| H. Wu et al. [23] | Heart | 270 videos | Philips CX50 | SVM | Accuracy 98.5% |
| D. Agarwal et al. [24] | Heart | 703 images | GE Vivid series | SVM | Accuracy 98% |
| R. Kumar et al. [25] | Heart | 113 videos (2470 frames) | Several (Database) | SVM | Recognition rate 81% |
| W.-C. Ye et al. [26] | Liver | 20 livers | frame grabber | SVM | Accuracy 91% |
| B. Lei et al. [27] | Fetal Brain | 1.735 images | Siemens Acuson Sequoia 512 | SVM Classifier | Accuracy 93.27% Precision 99.19% |
| R. Qu et al. [28] | Fetal Brain | 31,200 images | Hitachi ARIETTA 70 | CNN | AUC 0.90 |
| Y. Cai et al. [29] | Fetal Abdomen | 1292 images | Philips HD9 (V7-3) | CNN | Precision 96.5% |
| C. F Baumgartner et al. [30] | Fetal Anatomy | 1003 videos | GE Voluson E8 | CNN | Accuracy 66–90% |
| C. F. Baumgartner et al. [31] | Fetal Anatomy | 2694 videos | GE Voluson E8 | CNN | Accuracy 90.1% |
| Y. Chen et al. [32] | Lung and Liver | 23,000 images | Several (Database) | CNN | Accuracy 94.2% |
| Y. Gao et al. [33] | Fetal head | >30,000 frames | Konted GEN 1 C10R | CNN | Precision 86% |
| M. Yaqub et al. [34] | Fetal brain | 19,838 images (10,595 scans) | Several | CNN | Agreement 94.1% |
| X. P. Burgos-Artizzu et al. [35] | Fetus and Mother’s Cervix | 12,400 images (1792 patients) | Several (Database) | CNN (19 models) | Accuracy Classification 93.6% |
| C. P Bridge et al. [15] | Fetal Heart | 91 videos | GE Voluson E8 | RF | ClassificationError 18% |
| C. P Bridge et al. [36] | Fetal Heart | 63 videos | - | Fourier and SVM | Accuracy 88% |
- Manual feature extraction settings depend on subjective human choices.
- The number and type of extracted features are usually very limited.
- Feature extraction methods cannot be optimized in real-time, which may be helpful when there are changes in the datasets.
2.2. Scan Plane Classification
2.3. Organ Identification
2.4. Standard Clinical Plane Extraction from Volumetric (3D) Ultrasound Images
| Standard Clinical Plane Extraction from 3D Volume | |||||
|---|---|---|---|---|---|
| Reference | Target Organ | # Cases | US System | AI Model | Results |
| K. Chykeyuk et al. [37] | Heart | 25 3D cases | Philips iE33 | RF | Distance <6 mm, Angle <3.5° |
| C. Lorenz et al. [38] | Fetal Abdomen | 126 training 42 evaluation | Several | RF | Plane Offset Error 5.8 mm Circumference error 4.9% |
| Y.i Li et al. [39,40] | Fetal Brain | 72 volumes | - | CNN (ITN) | Translation error 3.5 mm Angular error 12.4 deg |
| H. Ryou et al. [41] | Fetal Brain | 19,838 images (10,595 scans) | Several | CNN | 96.9% Dice coefficient (Head Region Detection) |
| H. Dou et al. [42] | Fetal Brain | 430 | Mindray DC-9 US system | RNN recurrent neural network | |
| X. Yang et al. [43] | Uterus and Fetal Brain | 683 (Uterus) 432 (Fetal Brain) | - | RL, RNN, and DQN | Localization Accuracy Fetal Brain 1.19 mm |
| B. Jiang et al. [46] | Phantom | 6 volumes | Ultrasonix SonixTouch | RL, RNN, and DQN | Translation error 5.5 mm Angular error 2.2 deg |
| T.-F. Yu et al. [47] | Breast | 22,982,656 images (1 volume) | GE ABUS | CNN | Translation Prediction error (x/y) (0.14 mm/0.25 mm) |
| E Skelton et al. [48] | Fetal Brain | 551 images | Philips Healthcare EpiQ | CNN (ITN) | Translation error 3.4 mm Angular error 12.5 deg |
| Z. Baum et al. [49] | Prostate | 108 image pairs | Intraoperative TRUS | PointNet NN | Registration Error 4.4 mm |
2.5. Image Quality Assessment
3. Scanning Guidance with AI
3.1. Human-Operated Systems
| Scanning Guidance Human-Operated Systems | |||||
|---|---|---|---|---|---|
| Reference | Target Organ | # Cases | US System | AI Model | Results |
| P. Jarosik et al. [57] | Phantom | 4 runs 16 time steps | Simulation | Deep RL | Distance from the object’s center 0.2 cm |
| F. Milletari et al. [58] | Heart | 200k images | Unknown | RL + DQN | Correct guidance 86.1% |
| R. Droste et al. [59] | Fetus | 464 scans by 17 experts | GE Voluson E8 scanner | MNet CNN | Prediction accuracy: 88.8% goal, 90.9% action |
| A. Narang et al. [61] | Heart | 240 scans | Terason uSmart 3200t Plus | DL | Diagnostic Quality 98.8% |
3.2. Robot-Operated Systems
| Scanning Guidance Robot-Operated Systems | |||||
|---|---|---|---|---|---|
| Reference | Target Organ | # Cases | US System | AI Model | Results |
| G. Toporek et al. [62] | Fetal Phantom | 38,900 train 5400 test | Philips X5-1 EPIQ | CNN | Translational accuracy < 3 mm |
| A.S.B. Mustafa et al. [63] | Liver | Validation on 14 male subjects | Mitsubishi Electric MELFA RV-1 | Image Processing Methods | Localization Initial Posit. Success 94% |
| K Liang et al. [64] | Breast | 5 cyst biopsies | Duke/VMI 3-D scanner | Image Processing Methods | Distance error 1.15mm |
| H. Hase et al. [67] | Backbone | 34 volunteers | Zonare z.one ultra | RL + DQN | Correct Navigation 82.91% |
| Q. Huang et al. [68] | Phantom | - | Sonix RP Ultrasonic Medical Corp. | Point Cloud from Kinect | - |
4. Discussion
- Deep learning systems are only as good as the curated datasets applied in their training. The dependence on the operator creates a large variability in US-acquired images, which may limit the generalizability of DL-based systems [69]. AI results depend on how the target structure is represented and defined by the examiner in the captured image [70] and, furthermore, on whether the target is correctly identified and captured. Therefore, the data used for training AI systems must be acquired by examiners with some degree of competency and experience [70].
- Training data are usually taken by a group of physicians that share the same protocols and criteria to choose the right standard views. This may create considerable differences between the imaging data collected to train AI algorithms and the data from real-world practice. Normalization of scanning and image acquisition may be required to mitigate this problem, and it could be critical for the successful future application of AI in the US. In fact, this requirement of AI tools may promote the standardization and image quality verification of US examinations performed by humans.
- A lot of expert sonographer time is required to create datasets by sampling the body surface in all needed probe positions and orientations. Even in a simplified case, as the one presented in [71] for the parasternal long axis (Plax) acoustic window, it required more than 20 min per patient.
- Most of the proposed approaches for AI-based ultrasound guidance in this review paper require labeled data to train the algorithms. Labels may be obtained from external devices such as an IMU [59], an external optical tracking system in the probe [58], or by expert US practitioners. In both cases, labels are prone to errors, which limit the best achievable performance of the DL models trained with them.
- The development of these technologies requires collaboration between experts from multiple disciplines. Most of the successful ML applications in medicine arose from collaborations of computational scientists, signal-processing engineers, physics experts, and medical experts [7]. However, sometimes it is not straightforward to combine different perspectives, different data models, and different approaches to data analysis.
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Warner, H.R.; Gardner, R.M.; Toronto, A.F. Computer-Based Monitoring of Cardiovascular Functions in Postoperative Patients. Circulation 1968, 37, II68–II74. [Google Scholar] [CrossRef] [PubMed]
- Ambinder, E.P. A History of the Shift Toward Full Computerization of Medicine. J. Oncol. Pract. 2005, 1, 54–56. [Google Scholar] [CrossRef] [PubMed]
- Turing, A.M. Intelligent Machinery, 1948, 4. Reprinted in Mechanical Intelligence (Collected Works of AM Turing); North-Holland Publishing Co.: Amsterdam, The Netherlands, 1992. [Google Scholar]
- Keane, P.A.; Topol, E.J. With an Eye to AI and Autonomous Diagnosis. NPJ Digit. Med. 2018, 1, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Do, S.; Song, K.D.; Chung, J.W. Basics of Deep Learning: A Radiologist’s Guide to Understanding Published Radiology Articles on Deep Learning. Korean J. Radiol. 2020, 21, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Topol, E.J. High-Performance Medicine: The Convergence of Human and Artificial Intelligence. Nat. Med. 2019, 25, 44–56. [Google Scholar] [CrossRef]
- Littmann, M.; Selig, K.; Cohen-Lavi, L.; Frank, Y.; Hönigschmid, P.; Kataka, E.; Mösch, A.; Qian, K.; Ron, A.; Schmid, S. Validity of Machine Learning in Biology and Medicine Increased through Collaborations across Fields of Expertise. Nat. Mach. Intell. 2020, 2, 18–24. [Google Scholar] [CrossRef]
- Zhou, S.K.; Greenspan, H.; Davatzikos, C.; Duncan, J.S.; Van Ginneken, B.; Madabhushi, A.; Prince, J.L.; Rueckert, D.; Summers, R.M. A Review of Deep Learning in Medical Imaging: Imaging Traits, Technology Trends, Case Studies With Progress Highlights, and Future Promises. Proc. IEEE 2021, 109, 820–838. [Google Scholar] [CrossRef]
- Wang, Y.; Ge, X.; Ma, H.; Qi, S.; Zhang, G.; Yao, Y. Deep Learning in Medical Ultrasound Image Analysis: A Review. IEEE Access 2021, 9, 54310–54324. [Google Scholar] [CrossRef]
- Liu, S.; Wang, Y.; Yang, X.; Lei, B.; Liu, L.; Li, S.X.; Ni, D.; Wang, T. Deep Learning in Medical Ultrasound Analysis: A Review. Engineering 2019, 5, 261–275. [Google Scholar] [CrossRef]
- Deffieux, T.; Demené, C.; Tanter, M. Functional Ultrasound Imaging: A New Imaging Modality for Neuroscience. Neuroscience 2021, 474, 110–121. [Google Scholar] [CrossRef]
- Shah, S.; Bellows, B.A.; Adedipe, A.A.; Totten, J.E.; Backlund, B.H.; Sajed, D. Perceived Barriers in the Use of Ultrasound in Developing Countries. Crit. Ultrasound J. 2015, 7, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Maraci, M.A.; Napolitano, R.; Papageorghiou, A.; Noble, J.A. Searching for Structures of Interest in an Ultrasound Video Sequence; Springer: Berlin/Heidelberg, Germany, 2014; pp. 133–140. [Google Scholar]
- Chang, R.-F.; Wu, W.-J.; Moon, W.K.; Chen, D.-R. Improvement in Breast Tumor Discrimination by Support Vector Machines and Speckle-Emphasis Texture Analysis. Ultrasound Med. Biol. 2003, 29, 679–686. [Google Scholar] [CrossRef] [PubMed]
- Bridge, C.P.; Ioannou, C.; Noble, J.A. Automated Annotation and Quantitative Description of Ultrasound Videos of the Fetal Heart. Med. Image Anal. 2017, 36, 147–161. [Google Scholar] [CrossRef] [PubMed]
- Attia, M.W.; Abou-Chadi, F.; Moustafa, H.E.-D.; Mekky, N. Classification of Ultrasound Kidney Images Using PCA and Neural Networks. Int. J. Adv. Comput. Sci. Appl. 2015, 6, 53–57. [Google Scholar]
- Chen, H.; Dou, Q.; Ni, D.; Cheng, J.-Z.; Qin, J.; Li, S.; Heng, P.-A. Automatic Fetal Ultrasound Standard Plane Detection Using Knowledge Transferred Recurrent Neural Networks; Springer: Berlin/Heidelberg, Germany, 2015; pp. 507–514. [Google Scholar]
- Chen, H.; Ni, D.; Qin, J.; Li, S.; Yang, X.; Wang, T.; Heng, P.A. Standard Plane Localization in Fetal Ultrasound via Domain Transferred Deep Neural Networks. IEEE J. Biomed. Health Inform. 2015, 19, 1627–1636. [Google Scholar] [CrossRef]
- Ni, D.; Li, T.; Yang, X.; Qin, J.; Li, S.; Chin, C.-T.; Ouyang, S.; Wang, T.; Chen, S. Selective Search and Sequential Detection for Standard Plane Localization in Ultrasound; Springer: Berlin/Heidelberg, Germany, 2013; pp. 203–211. [Google Scholar]
- Ni, D.; Yang, X.; Chen, X.; Chin, C.-T.; Chen, S.; Heng, P.A.; Li, S.; Qin, J.; Wang, T. Standard Plane Localization in Ultrasound by Radial Component Model and Selective Search. Ultrasound Med. Biol. 2014, 40, 2728–2742. [Google Scholar] [CrossRef]
- Rahmatullah, B.; Sarris, I.; Papageorghiou, A.; Noble, J.A. Quality Control of Fetal Ultrasound Images: Detection of Abdomen Anatomical Landmarks Using AdaBoost; IEEE: Piscataway, NJ, USA, 2011; pp. 6–9. [Google Scholar]
- Rahmatullah, B.; Papageorghiou, A.T.; Noble, J.A. Integration of Local and Global Features for Anatomical Object Detection in Ultrasound; Springer: Berlin/Heidelberg, Germany, 2012; pp. 402–409. [Google Scholar]
- Wu, H.; Bowers, D.M.; Huynh, T.T.; Souvenir, R. Echocardiogram View Classification Using Low-Level Features; IEEE: Piscataway, NJ, USA, 2013; pp. 752–755. [Google Scholar]
- Agarwal, D.; Shriram, K.; Subramanian, N. Automatic View Classification of Echocardiograms Using Histogram of Oriented Gradients; IEEE: Piscataway, NJ, USA, 2013; pp. 1368–1371. [Google Scholar]
- Kumar, R.; Wang, F.; Beymer, D.; Syeda-Mahmood, T. Echocardiogram View Classification Using Edge Filtered Scale-Invariant Motion Features. In Proceedings of the 2009 IEEE Conference on Computer Vision and Pattern Recognition, Miami, FL, USA, 20–25 June 2009; IEEE: Miami, FL, USA, 2009; pp. 723–730. [Google Scholar]
- Yeh, W.-C.; Huang, S.-W.; Li, P.-C. Liver Fibrosis Grade Classification with B-Mode Ultrasound. Ultrasound Med. Biol. 2003, 29, 1229–1235. [Google Scholar] [CrossRef]
- Lei, B.; Tan, E.-L.; Chen, S.; Zhuo, L.; Li, S.; Ni, D.; Wang, T. Automatic Recognition of Fetal Facial Standard Plane in Ultrasound Image via Fisher Vector. PloS ONE 2015, 10, e0121838. [Google Scholar] [CrossRef]
- Qu, R.; Xu, G.; Ding, C.; Jia, W.; Sun, M. Deep Learning-Based Methodology for Recognition of Fetal Brain Standard Scan Planes in 2D Ultrasound Images. IEEE Access 2019, 8, 44443–44451. [Google Scholar] [CrossRef]
- Cai, Y.; Sharma, H.; Chatelain, P.; Noble, J.A. SonoEyeNet: Standardized Fetal Ultrasound Plane Detection Informed by Eye Tracking; IEEE: Piscataway, NJ, USA, 2018; pp. 1475–1478. [Google Scholar]
- Baumgartner, C.F.; Kamnitsas, K.; Matthew, J.; Smith, S.; Kainz, B.; Rueckert, D. Real-Time Standard Scan Plane Detection and Localisation in Fetal Ultrasound Using Fully Convolutional Neural Networks; Springer: Berlin/Heidelberg, Germany, 2016; pp. 203–211. [Google Scholar]
- Baumgartner, C.F.; Kamnitsas, K.; Matthew, J.; Fletcher, T.P.; Smith, S.; Koch, L.M.; Kainz, B.; Rueckert, D. SonoNet: Real-Time Detection and Localisation of Fetal Standard Scan Planes in Freehand Ultrasound. IEEE Trans. Med. Imaging 2017, 36, 2204–2215. [Google Scholar] [CrossRef]
- Chen, Y.; Zhang, C.; Liu, L.; Feng, C.; Dong, C.; Luo, Y.; Wan, X. Effective Sample Pair Generation for Ultrasound Video Contrastive Representation Learning. arXiv 2020, arXiv:2011.13066. [Google Scholar]
- Gao, Y.; Beriwal, S.; Craik, R.; Papageorghiou, A.T.; Noble, J.A. Label Efficient Localization of Fetal Brain Biometry Planes in Ultrasound through Metric Learning. In Medical Ultrasound, and Preterm, Perinatal and Paediatric Image Analysis; Springer: Berlin/Heidelberg, Germany, 2020; pp. 126–135. [Google Scholar]
- Yaqub, M.; Kelly, B.; Papageorghiou, A.T.; Noble, J.A. A Deep Learning Solution for Automatic Fetal Neurosonographic Diagnostic Plane Verification Using Clinical Standard Constraints. Ultrasound Med. Biol. 2017, 43, 2925–2933. [Google Scholar] [CrossRef]
- Burgos-Artizzu, X.P.; Coronado-Gutiérrez, D.; Valenzuela-Alcaraz, B.; Bonet-Carne, E.; Eixarch, E.; Crispi, F.; Gratacós, E. Evaluation of Deep Convolutional Neural Networks for Automatic Classification of Common Maternal Fetal Ultrasound Planes. Sci. Rep. 2020, 10, 10200. [Google Scholar] [CrossRef]
- Bridge, C.P.; Noble, J.A. Object Localisation in Fetal Ultrasound Images Using Invariant Features; IEEE: Piscataway, NJ, USA, 2015; pp. 156–159. [Google Scholar]
- Chykeyuk, K.; Yaqub, M.; Alison Noble, J. Class-Specific Regression Random Forest for Accurate Extraction of Standard Planes from 3D Echocardiography; Springer: Berlin/Heidelberg, Germany, 2013; pp. 53–62. [Google Scholar]
- Lorenz, C.; Brosch, T.; Ciofolo-Veit, C.; Tobias, K.; Lefevre, T.; Salim, I.; Papageorghiou, A.T.; Raynaud, C.; Roundhill, D.; Rouet, L.; et al. Automated Abdominal Plane and Circumference Estimation in 3D US for Fetal Screening; SPIE: Bellingham, WA, USA, 2018. [Google Scholar]
- Li, Y.; Khanal, B.; Hou, B.; Alansary, A.; Cerrolaza, J.J.; Sinclair, M.; Matthew, J.; Gupta, C.; Knight, C.; Kainz, B. Standard Plane Detection in 3d Fetal Ultrasound Using an Iterative Transformation Network; Springer: Berlin/Heidelberg, Germany, 2018; pp. 392–400. [Google Scholar]
- Li, Y.; Cerrolaza, J.J.; Sinclair, M.; Hou, B.; Alansary, A.; Khanal, B.; Matthew, J.; Kainz, B.; Rueckert, D. Standard Plane Localisation in 3D Fetal Ultrasound Using Network with Geometric and Image Loss. 2018. Available online: https://openreview.net/forum?id=BykcN8siz (accessed on 9 March 2023).
- Ryou, H.; Yaqub, M.; Cavallaro, A.; Roseman, F.; Papageorghiou, A.; Noble, J.A. Automated 3D Ultrasound Biometry Planes Extraction for First Trimester Fetal Assessment; Springer: Berlin/Heidelberg, Germany, 2016; pp. 196–204. [Google Scholar]
- Dou, H.; Yang, X.; Qian, J.; Xue, W.; Qin, H.; Wang, X.; Yu, L.; Wang, S.; Xiong, Y.; Heng, P.-A. Agent with Warm Start and Active Termination for Plane Localization in 3D Ultrasound; Springer: Berlin/Heidelberg, Germany, 2019; pp. 290–298. [Google Scholar]
- Yang, X.; Huang, Y.; Huang, R.; Dou, H.; Li, R.; Qian, J.; Huang, X.; Shi, W.; Chen, C.; Zhang, Y. Searching Collaborative Agents for Multi-Plane Localization in 3d Ultrasound. Med. Image Anal. 2021, 72, 102119. [Google Scholar] [CrossRef] [PubMed]
- Ren, P.; Xiao, Y.; Chang, X.; Huang, P.-Y.; Li, Z.; Chen, X.; Wang, X. A Comprehensive Survey of Neural Architecture Search: Challenges and Solutions. ACM Comput. Surv. CSUR 2021, 54, 1–34. [Google Scholar] [CrossRef]
- Dong, X.; Yang, Y. Searching for a Robust Neural Architecture in Four Gpu Hours. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition, Long Beach, CA, USA, 15–20 June 2019; 2019; pp. 1761–1770. Available online: https://openaccess.thecvf.com/content_CVPR_2019/papers/Dong_Searching_for_a_Robust_Neural_Architecture_in_Four_GPU_Hours_CVPR_2019_paper.pdf (accessed on 9 March 2023).
- Jiang, B.; Xu, K.; Taylor, R.H.; Graham, E.; Unberath, M.; Boctor, E.M. Standard Plane Extraction From 3D Ultrasound With 6-DOF Deep Reinforcement Learning Agent; IEEE: Piscataway, NJ, USA, 2020; pp. 1–4. [Google Scholar]
- Yu, T.-F.; Liu, P.; Peng, Y.-L.; Liu, J.-Y.; Yin, H.; Liu, D.C. Slice Localization for Three-Dimensional Breast Ultrasound Volume Using Deep Learning. DEStech Trans. Eng. Technol. Res. 2019. [Google Scholar] [CrossRef] [PubMed]
- Skelton, E.; Matthew, J.; Li, Y.; Khanal, B.; Martinez, J.C.; Toussaint, N.; Gupta, C.; Knight, C.; Kainz, B.; Hajnal, J. Towards Automated Extraction of 2D Standard Fetal Head Planes from 3D Ultrasound Acquisitions: A Clinical Evaluation and Quality Assessment Comparison. Radiography 2021, 27, 519–526. [Google Scholar] [CrossRef] [PubMed]
- Baum, Z.; Hu, Y.; Barratt, D.C. Multimodality Biomedical Image Registration Using Free Point Transformer Networks. In Medical Ultrasound, and Preterm, Perinatal and Paediatric Image Analysis; Springer: Berlin/Heidelberg, Germany, 2020; pp. 116–125. [Google Scholar]
- Khan, S.; Huh, J.; Ye, J.C. Variational Formulation of Unsupervised Deep Learning for Ultrasound Image Artifact Removal. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2021, 68, 2086–2100. [Google Scholar] [CrossRef]
- Rindal, O.M.H.; Austeng, A.; Fatemi, A.; Rodriguez-Molares, A. The Effect of Dynamic Range Alterations in the Estimation of Contrast. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2019, 66, 1198–1208. [Google Scholar] [CrossRef]
- Rodriguez-Molares, A.; Rindal, O.M.H.; D’hooge, J.; Masoy, S.-E.; Austeng, A.; Lediju Bell, M.A.; Torp, H. The Generalized Contrast-to-Noise Ratio: A Formal Definition for Lesion Detectability. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2020, 67, 745–759. [Google Scholar] [CrossRef]
- Zhang, B.; Liu, H.; Luo, H.; Li, K. Automatic Quality Assessment for 2D Fetal Sonographic Standard Plane Based on Multitask Learning. Medicine 2021, 100, e24427. [Google Scholar] [CrossRef]
- Prevost, R.; Salehi, M.; Jagoda, S.; Kumar, N.; Sprung, J.; Ladikos, A.; Bauer, R.; Zettinig, O.; Wein, W. 3D Freehand Ultrasound without External Tracking Using Deep Learning. Med. Image Anal. 2018, 48, 187–202. [Google Scholar] [CrossRef] [PubMed]
- Guo, H.; Xu, S.; Wood, B.; Yan, P. Sensorless Freehand 3D Ultrasound Reconstruction via Deep Contextual Learning; Springer: Berlin/Heidelberg, Germany, 2020; pp. 463–472. [Google Scholar]
- Park, S.H. Artificial Intelligence for Ultrasonography: Unique Opportunities and Challenges. Ultrasonography 2021, 40, 3–6. [Google Scholar] [CrossRef] [PubMed]
- Jarosik, P.; Lewandowski, M. Automatic Ultrasound Guidance Based on Deep Reinforcement Learning; IEEE: Piscataway, NJ, USA, 2019. [Google Scholar]
- Milletari, F.; Birodkar, V.; Sofka, M. Straight to the Point: Reinforcement Learning for User Guidance in Ultrasound. In Smart Ultrasound Imaging and Perinatal, Preterm and Paediatric Image Analysis; Springer: Berlin/Heidelberg, Germany, 2019; pp. 3–10. [Google Scholar]
- Droste, R.; Drukker, L.; Papageorghiou, A.T.; Noble, J.A. Automatic Probe Movement Guidance for Freehand Obstetric Ultrasound; Springer: Berlin/Heidelberg, Germany, 2020; pp. 583–592. [Google Scholar]
- Pan, Y.; Cheng, C.-A.; Saigol, K.; Lee, K.; Yan, X.; Theodorou, E.; Boots, B. Agile Autonomous Driving Using End-to-End Deep Imitation Learning. arXiv 2017, arXiv:1709.07174 2017. [Google Scholar]
- Narang, A.; Bae, R.; Hong, H.; Thomas, Y.; Surette, S.; Cadieu, C.; Chaudhry, A.; Martin, R.P.; McCarthy, P.M.; Rubenson, D.S.; et al. Utility of a Deep-Learning Algorithm to Guide Novices to Acquire Echocardiograms for Limited Diagnostic Use. JAMA Cardiol. 2021, 6, 624. [Google Scholar] [CrossRef] [PubMed]
- Toporek, G.; Wang, H.; Balicki, M.; Xie, H. Autonomous Image-Based Ultrasound Probe Positioning via Deep Learning; EasyChair Preprint no. 119. 2018. Available online: https://easychair.org/publications/preprint/XmZ9 (accessed on 9 March 2023).
- Mustafa, A.S.B.; Ishii, T.; Matsunaga, Y.; Nakadate, R.; Ishii, H.; Ogawa, K.; Saito, A.; Sugawara, M.; Niki, K.; Takanishi, A. Development of Robotic System for Autonomous Liver Screening Using Ultrasound Scanning Device; IEEE: Piscataway, NJ, USA, 2013; pp. 804–809. [Google Scholar]
- Liang, K.; Rogers, A.J.; Light, E.D.; von Allmen, D.; Smith, S.W. Three-Dimensional Ultrasound Guidance of Autonomous Robotic Breast Biopsy: Feasibility Study. Ultrasound Med. Biol. 2010, 36, 173–177. [Google Scholar] [CrossRef] [PubMed]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the IEEE Computer Society Conference on Computer Vision and Pattern Recognition (CVPR), Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar] [CrossRef]
- Kendall, A.; Grimes, M.; Cipolla, R. Posenet: A convolutional network for real-time 6-dof camera relocalization. In Proceedings of the IEEE International Conference on Computer Vision, Santiago, Chile, 11–18 December 2015; pp. 2938–2946. [Google Scholar]
- Hase, H.; Azampour, M.F.; Tirindelli, M.; Paschali, M.; Simson, W.; Fatemizadeh, E.; Navab, N. Ultrasound-Guided Robotic Navigation with Deep Reinforcement Learning; IEEE: Piscataway, NJ, USA, 2020; pp. 5534–5541. [Google Scholar]
- Huang, Q.; Lan, J.; Li, X. Robotic Arm Based Automatic Ultrasound Scanning for Three-Dimensional Imaging. IEEE Trans. Ind. Inform. 2018, 15, 1173–1182. [Google Scholar] [CrossRef]
- Kelly, C.J.; Karthikesalingam, A.; Suleyman, M.; Corrado, G.; King, D. Key Challenges for Delivering Clinical Impact with Artificial Intelligence. BMC Med. 2019, 17, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Jeong, E.Y.; Kim, H.L.; Ha, E.J.; Park, S.Y.; Cho, Y.J.; Han, M. Computer-Aided Diagnosis System for Thyroid Nodules on Ultrasonography: Diagnostic Performance and Reproducibility Based on the Experience Level of Operators. Eur. Radiol. 2019, 29, 1978–1985. [Google Scholar] [CrossRef]
- Kennedy Hall, M.; Coffey, E.; Herbst, M.; Liu, R.; Pare, J.R.; Andrew Taylor, R.; Thomas, S.; Moore, C.L. The “5Es” of Emergency Physician–Performed Focused Cardiac Ultrasound: A Protocol for Rapid Identification of Effusion, Ejection, Equality, Exit, and Entrance. Acad. Emerg. Med. 2015, 22, 583–593. [Google Scholar] [CrossRef]
- FDA Authorizes Marketing of First Cardiac Ultrasound Software That Uses Artificial Intelligence to Guide User. Feb 2020. FDA news. Available online: https://www.fda.gov/news-events/press-announcements/fda-authorizes-marketing-first-cardiac-ultrasound-software-uses-artificial-intelligence-guide-user (accessed on 9 March 2023).


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tenajas, R.; Miraut, D.; Illana, C.I.; Alonso-Gonzalez, R.; Arias-Valcayo, F.; Herraiz, J.L. Recent Advances in Artificial Intelligence-Assisted Ultrasound Scanning. Appl. Sci. 2023, 13, 3693. https://doi.org/10.3390/app13063693
Tenajas R, Miraut D, Illana CI, Alonso-Gonzalez R, Arias-Valcayo F, Herraiz JL. Recent Advances in Artificial Intelligence-Assisted Ultrasound Scanning. Applied Sciences. 2023; 13(6):3693. https://doi.org/10.3390/app13063693
Chicago/Turabian StyleTenajas, Rebeca, David Miraut, Carlos I. Illana, Rodrigo Alonso-Gonzalez, Fernando Arias-Valcayo, and Joaquin L. Herraiz. 2023. "Recent Advances in Artificial Intelligence-Assisted Ultrasound Scanning" Applied Sciences 13, no. 6: 3693. https://doi.org/10.3390/app13063693
APA StyleTenajas, R., Miraut, D., Illana, C. I., Alonso-Gonzalez, R., Arias-Valcayo, F., & Herraiz, J. L. (2023). Recent Advances in Artificial Intelligence-Assisted Ultrasound Scanning. Applied Sciences, 13(6), 3693. https://doi.org/10.3390/app13063693