
Difference of Two Antiseptic Gels for the Treatment of Peri-Implant Mucositis on Plaque Index and Bleeding Score: A Randomized Controlled Clinical Study


 , ,
, ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients Recruiting
- -
- Patients aged over 18 years;
- -
- At least one dental implant with mucositis (clinical signs of inflammation with bleeding at probing and probing depth > 4 mm);
- -
- No exclusion criteria present;
- -
- Signing of informed consent.
- -
- Suppuration;
- -
- RX evidence of bone lesion with a depth > of 2 mm;
- -
- Peri-implantitis;
- -
- Physical or mental disabilities that affect correct domiciliary oral hygiene operations;
- -
- Abuse of alcohol or drugs;
- -
- Conditions or circumstances that prevent study participation completion or interfere with the analysis of study results.
2.2. Sample Dimension
2.3. Initial Preparation and Randomization
2.4. Test and Control Treatment
2.5. Control and Follow-Up Visits
2.6. Outcomes
2.7. Measurements
2.8. Methodological Aspects
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rizzo, S.; Zampetti, P.; Rodriguez, Y.; Baena, R.; Svanosio, D.; Lupi, S.M. Retrospective Analysis of 521 Endosseous Implants Placed under Antibiotic Prophylaxis and Review of Literature. Minerva Stomatol. 2010, 59, 75–88. [Google Scholar]
- Lupi, S.M.; Redoglia, L.; Rodriguez, Y.; Baena, A.; Garbelli, G.; Rodriguez, Y.; Baena, R. Detection of Peri-Implant Inflammation by the Use of a Matrix Metalloproteinase-8 Chair-Side Test. Minerva Stomatol. 2019, 68, 168–176. [Google Scholar] [CrossRef] [PubMed]
- Lupi, S.; Granati, M.; Butera, A.; Collesano, V.; Rodriguez, Y.; Baena, R. Air-Abrasive Debridement with Glycine Powder versus Manual Debridement and Chlorhexidine Administration for the Maintenance of Peri-Implant Health Status: A Six-Month Randomized Clinical Trial. Int. J. Dent. Hyg. 2017, 15, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Lupi, S.; Zaffe, D.; Baena, R.R.Y.; Rizzo, S.; Botticelli, A. Cytopathological and Chemico-Physical Analyses of Smears of Mucosa Surrounding Oral Piercing. Oral Dis. 2010, 16, 160–166. [Google Scholar] [CrossRef] [PubMed]
- Berglundh, T.; Armitage, G.; Araujo, M.G.; Avila-Ortiz, G.; Blanco, J.; Camargo, P.M.; Chen, S.; Cochran, D.; Derks, J.; Figuero, E.; et al. Peri-Implant Diseases and Conditions: Consensus Report of Workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Clin. Periodontol. 2018, 45, S286–S291. [Google Scholar] [CrossRef]
- Romeo, E.; Lops, D.; Margutti, E.; Ghisolfi, M.; Chiapasco, M.; Vogel, G. Long-Term Survival and Success of Oral Implants in the Treatment of Full and Partial Arches: A 7-Year Prospective Study with the ITI Dental Implant System. Int. J. Oral Maxillofac. Implants 2004, 19, 247–259. [Google Scholar]
- Tonetti, M.S.; Schmid, J. Pathogenesis of Implant Failures. Periodontol. 2000 1994, 4, 127–138. [Google Scholar] [CrossRef]
- Esposito, M.; Hirsch, J.; Lekholm, U.; Thomsen, P. Differential Diagnosis and Treatment Strategies for Biologic Complications and Failing Oral Implants: A Review of the Literature. Int. J. Oral Maxillofac. Implants 1999, 14, 473–490. [Google Scholar]
- Máximo, M.B.; de Mendonça, A.C.; Renata Santos, V.; Figueiredo, L.C.; Feres, M.; Duarte, P.M. Short-Term Clinical and Microbiological Evaluations of Peri-Implant Diseases before and after Mechanical Anti-Infective Therapies. Clin. Oral Implants Res. 2009, 20, 99–108. [Google Scholar] [CrossRef]
- Thöne-Mühling, M.; Swierkot, K.; Nonnenmacher, C.; Mutters, R.; Flores-de-Jacoby, L.; Mengel, R. Comparison of Two Full-Mouth Approaches in the Treatment of Peri-Implant Mucositis: A Pilot Study. Clin. Oral Implants Res. 2010, 21, 504–512. [Google Scholar] [CrossRef]
- Trejo, P.M.; Bonaventura, G.; Weng, D.; Caffesse, R.G.; Bragger, U.; Lang, N.P. Effect of Mechanical and Antiseptic Therapy on Peri-Implant Mucositis: An Experimental Study in Monkeys. Clin. Oral Implants Res. 2006, 17, 294–304. [Google Scholar] [CrossRef] [PubMed]
- Albrektsson, T.; Isidor, F.; Lang, N.P.; Karring, T. Consensus Report of Session IV. In Proceedings of the First European Workshop on Periodontology; Quintessence Publishing: London, UK, 2014; pp. 365–369. ISBN 9781119130536. [Google Scholar]
- Butera, A.; Maiorani, C.; Gallo, S.; Pascadopoli, M.; Venugopal, A.; Marya, A.; Scribante, A. Evaluation of Adjuvant Systems in Non-Surgical Peri-Implant Treatment: A Literature Review. Healthcare 2022, 10, 886. [Google Scholar] [CrossRef] [PubMed]
- Lang, N.; Hase, J.; Grassi, M.; Hämmerle, C.; Weigel, C.; Kelty, E.; Frutig, F. Plaque Formation and Gingivitis after Supervised Mouthrinsing with 0.2% Delmopinol Hydrochloride, 0.2% Chlorhexidine Digluconate and Placebo for 6 Months. Oral Dis. 2008, 4, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Ouhayoun, J.-P. Penetrating the Plaque Biofilm: Impact of Essential Oil Mouthwash. J. Clin. Periodontol. 2003, 30, 10–12. [Google Scholar] [CrossRef]
- Mandel, I.D. Chemotherapeutic Agents for Controlling Plaque and Gingivitis. J. Clin. Periodontol. 1988, 15, 488–498. [Google Scholar] [CrossRef]
- Costa, X.; Laguna, E.; Herrera, D.; Serrano, J.; Alonso, B.; Sanz, M. Efficacy of a New Mouth Rinse Formulation Based on 0.07% Cetylpyridinium Chloride in the Control of Plaque and Gingivitis: A 6-Month Randomized Clinical Trial. J. Clin. Periodontol. 2013, 40, 1007–1015. [Google Scholar] [CrossRef] [PubMed]
- Mor-Reinoso, C.; Pascual, A.; Nart, J.; Quirynen, M. Inhibition of de Novo Plaque Growth by a New 0.03 % Chlorhexidine Mouth Rinse Formulation Applying a Non-Brushing Model: A Randomized, Double Blind Clinical Trial. Clin. Oral Investig. 2016, 20, 1459–1467. [Google Scholar] [CrossRef]
- Becker, K.; Brunello, G.; Scotti, L.; Drescher, D.; John, G. Efficacy of 0.05% Chlorhexidine and 0.05% Cetylpyridinium Chloride Mouthwash to Eliminate Living Bacteria on In Situ Collected Biofilms: An In Vitro Study. Antibiotics 2021, 10, 730. [Google Scholar] [CrossRef]
- Silness, J.; Löe, H. Periodontal Disease in Pregnancy II. Correlation Between Oral Hygiene and Periodontal Condition. Acta Odontol. Scand. 1964, 22, 121–135. [Google Scholar] [CrossRef]
- Mombelli, A.; Marxer, M.; Gaberthüel, T.; Grander, U.; Lang, N.P. The Microbiota of Osseointegrated Implants in Patients with a History of Periodontal Disease. J. Clin. Periodontol. 1995, 22, 124–130. [Google Scholar] [CrossRef]
- Jepsen, S.; Berglundh, T.; Genco, R.; Aass, A.M.; Demirel, K.; Derks, J.; Figuero, E.; Giovannoli, J.L.; Goldstein, M.; Lambert, F.; et al. Primary Prevention of Peri-Implantitis: Managing Peri-Implant Mucositis. J. Clin. Periodontol. 2015, 42, S152–S157. [Google Scholar] [CrossRef] [PubMed]
- Derks, J.; Tomasi, C. Peri-Implant Health and Disease. A Systematic Review of Current Epidemiology. J. Clin. Periodontol. 2015, 42, S158–S171. [Google Scholar] [CrossRef] [PubMed]
- Gurgel, B.C.D.V.; Montenegro, S.C.L.; Dantas, P.M.C.; Pascoal, A.L.D.B.; Lima, K.C.; Calderon, P.D.S. Frequency of Peri-Implant Diseases and Associated Factors. Clin. Oral Implants Res. 2017, 28, 1211–1217. [Google Scholar] [CrossRef] [PubMed]
- Costa, F.O.; Takenaka-Martinez, S.; Cota, L.O.M.; Ferreira, S.D.; Silva, G.L.M.; Costa, J.E. Peri-Implant Disease in Subjects with and without Preventive Maintenance: A 5-Year Follow-Up. J. Clin. Periodontol. 2012, 39, 173–181. [Google Scholar] [CrossRef]
- Esposito, M.; Grusovin, M.G.; Worthington, H.V. Treatment of Peri-Implantitis: What Interventions Are Effective? A Cochrane Systematic Review. Eur. J. Oral Implantol. 2012, 5, S21–S41. [Google Scholar] [PubMed]
- Berglundh, T.; Wennström, J.L.; Lindhe, J. Long-Term Outcome of Surgical Treatment of Peri-Implantitis. A 2-11-Year Retrospective Study. Clin. Oral Implants Res. 2018, 29, 404–410. [Google Scholar] [CrossRef]
- Büchter, A.; Meyer, U.; Kruse-Lösler, B.; Joos, U.; Kleinheinz, J. Sustained Release of Doxycycline for the Treatment of Peri-Implantitis: Randomised Controlled Trial. Br. J. Oral Maxillofac. Surg. 2004, 42, 439–444. [Google Scholar] [CrossRef]
- Renvert, S.; Polyzois, I. Risk Indicators for Peri-Implant Mucositis: A Systematic Literature Review. J. Clin. Periodontol. 2015, 42, S172–S186. [Google Scholar] [CrossRef]
- Golub, L.M.; Sorsa, T.; Lee, H.-M.; Ciancio, S.; Sorbi, D.; Ramamurthy, N.S.; Gruber, B.; Salo, T.; Konttinen, Y.T. Doxycycline Inhibits Neutrophil (PMN)-Type Matrix Metalloproteinases in Human Adult Periodontitis Gingiva. J. Clin. Periodontol. 2005, 22, 100–109. [Google Scholar] [CrossRef]
- Felo, A.; Shibly, O.; Ciancio, S.G.; Lauciello, F.R.; Ho, A. Effects of Subgingival Chlorhexidine Irrigation on Peri-Implant Maintenance. Am. J. Dent. 1997, 10, 107–110. [Google Scholar]
- Peres Pimentel, S.; Vieira Ribeiro, F.; Correa Casarin, R.; Ribeiro Cirano, F.; Haguihara Luchesi, V.; Gallego Arias Pecorari, V.; Zaffalon Casati, M. Triclosan-Containing Fluoride Toothpaste on Clinical Parameters and Osteo-Inflammatory Mediators When Applied in a Stent during Experimental Peri-Implant Mucositis in Smokers. Clin. Oral Implants Res. 2019, 30, 187–195. [Google Scholar] [CrossRef] [PubMed]
- Machtei, E.E.; Romanos, G.; Kang, P.; Travan, S.; Schmidt, S.; Papathanasiou, E.; Tatarakis, N.; Tandlich, M.; Liberman, L.H.; Horwitz, J.; et al. Repeated Delivery of Chlorhexidine Chips for the Treatment of Peri-implantitis: A Multicenter, Randomized, Comparative Clinical Trial. J. Periodontol. 2021, 92, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Heitz-Mayfield, L.J.A.; Salvi, G.E.; Botticelli, D.; Mombelli, A.; Faddy, M.; Lang, N.P. Anti-Infective Treatment of Peri-Implant Mucositis: A Randomised Controlled Clinical Trial. Clin. Oral Implants Res. 2011, 22, 237–241. [Google Scholar] [CrossRef] [PubMed]
- Salvi, G.E.; Ramseier, C.A. Efficacy of Patient-Administered Mechanical and/or Chemical Plaque Control Protocols in the Management of Peri-Implant Mucositis. A Systematic Review. J. Clin. Periodontol. 2015, 42, S187–S201. [Google Scholar] [CrossRef]
- Schwarz, F.; Becker, K.; Sager, M. Efficacy of Professionally Administered Plaque Removal with or without Adjunctive Measures for the Treatment of Peri-Implant Mucositis. A Systematic Review and Meta-Analysis. J. Clin. Periodontol. 2015, 42, S202–S213. [Google Scholar] [CrossRef]
- Sanz, M.; Chapple, I.L. Clinical Research on Peri-Implant Diseases: Consensus Report of Working Group 4. J. Clin. Periodontol. 2012, 39, 202–206. [Google Scholar] [CrossRef]
- Pałka, Ł.; Nowakowska-Toporowska, A.; Dalewski, B. Is Chlorhexidine in Dentistry an Ally or a Foe? A Narrative Review. Healthcare 2022, 10, 764. [Google Scholar] [CrossRef]
- Jones, C.G. Chlorhexidine: Is It Still the Gold Standard? Periodontol. 2000 1997, 15, 55–62. [Google Scholar] [CrossRef]
- Slot, D.; Berchier, C.; Addy, M.; Van der Velden, U.; Van der Weijden, G. The Efficacy of Chlorhexidine Dentifrice or Gel on Plaque, Clinical Parameters of Gingival Inflammation and Tooth Discoloration: A Systematic Review. Int. J. Dent. Hyg. 2014, 12, 25–35. [Google Scholar] [CrossRef]
- Pulcini, A.; Bollaín, J.; Sanz-Sánchez, I.; Figuero, E.; Alonso, B.; Sanz, M.; Herrera, D. Clinical Effects of the Adjunctive Use of a 0.03% Chlorhexidine and 0.05% Cetylpyridinium Chloride Mouth Rinse in the Management of Peri-Implant Diseases: A Randomized Clinical Trial. J. Clin. Periodontol. 2019, 46, 342–353. [Google Scholar] [CrossRef]
- Carinci, F.; Lauritano, D.; Bignozzi, C.A.; Pazzi, D.; Candotto, V.; Santos de Oliveira, P.; Scarano, A. A New Strategy Against Peri-Implantitis: Antibacterial Internal Coating. Int. J. Mol. Sci. 2019, 20, 3897. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Scores | Plaque Index (PI) | Modified Bleeding Index (mBI) |
|---|---|---|
| 0 | Absence of plaque | No bleeding |
| 1 | Plaques with the probing | Isolated point bleeding |
| 2 | Visible plaque | Linear bleeding |
| 3 | Abundant plaque | Profuse bleeding |
| Test Group | Control Group | |
|---|---|---|
| Male | 4 | 5 |
| Female | 6 | 3 |
| Total | 10 | 8 |
| Smoker | 5 | 2 |
| Prosthetic rehabilitation | ||
| Crowns | 5 | 2 |
| Overdenture/Toronto Bridges | 2 | 3 |
| Overdenture | 0 | 1 |
| Overdentures/Crowns | 0 | 1 |
| Toronto | 2 | 1 |
| Crowns/Toronto Bridges | 1 | 0 |
| Control Group | Test Group | Difference | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Total | Mean | Total | Mean | ||||||
| Implants (n) | 43 | 5.38 | ± | 2.13 | 53 | 5.30 | ± | 3.62 | |
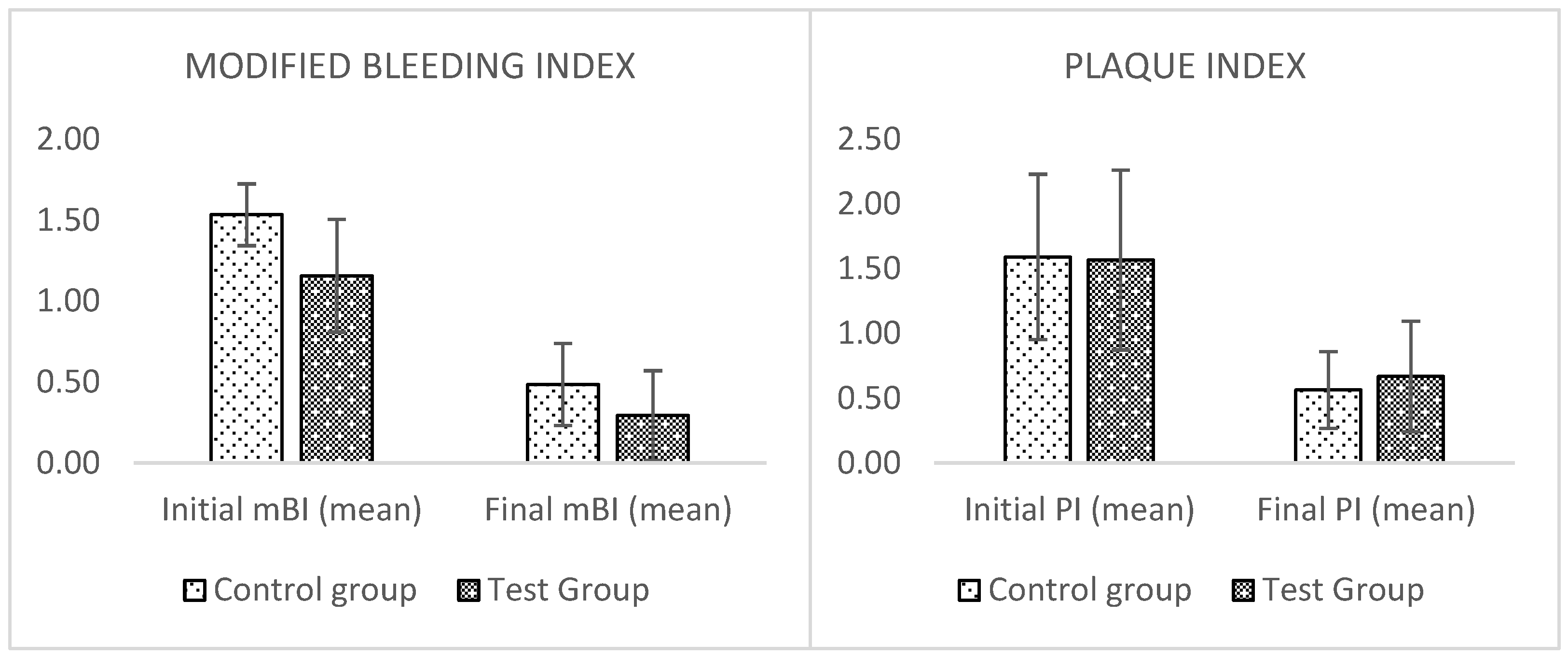
| Initial mBI | 1.53 | ± | 0.19 | 1.16 | ± | 0.35 | 0.0251 * | ||
| Final mBI | 0.49 | ± | 0.25 | 0.29 | ± | 0.28 | NS * | ||
| Improvement (%) | 68.23 | ± | 17.38 | 71.01 | ± | 32.62 | NS * | ||
| Initial PI | 1.59 | ± | 0.64 | 1.57 | ± | 0.69 | NS * | ||
| Final PI | 0.56 | ± | 0.30 | 0.67 | ± | 0.43 | NS * | ||
| Improvement (%) | 64.13 | ± | 18.04 | 58.41 | ± | 28.04 | NS * | ||
| Implants healed | 28 | 3.50 | ± | 1.41 | 36 | 3.60 | ± | 1.90 | NS ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Storelli, S.; Palandrani, G.; Manfredi, B.; Romeo, E.; De Martis, D.; Todaro, C.; Rodriguez y Baena, R.; Lupi, S.M. Difference of Two Antiseptic Gels for the Treatment of Peri-Implant Mucositis on Plaque Index and Bleeding Score: A Randomized Controlled Clinical Study. Appl. Sci. 2023, 13, 1288. https://doi.org/10.3390/app13031288
Storelli S, Palandrani G, Manfredi B, Romeo E, De Martis D, Todaro C, Rodriguez y Baena R, Lupi SM. Difference of Two Antiseptic Gels for the Treatment of Peri-Implant Mucositis on Plaque Index and Bleeding Score: A Randomized Controlled Clinical Study. Applied Sciences. 2023; 13(3):1288. https://doi.org/10.3390/app13031288
Chicago/Turabian StyleStorelli, Stefano, Giulia Palandrani, Barbara Manfredi, Eugenio Romeo, Dario De Martis, Claudia Todaro, Ruggero Rodriguez y Baena, and Saturnino Marco Lupi. 2023. "Difference of Two Antiseptic Gels for the Treatment of Peri-Implant Mucositis on Plaque Index and Bleeding Score: A Randomized Controlled Clinical Study" Applied Sciences 13, no. 3: 1288. https://doi.org/10.3390/app13031288
APA StyleStorelli, S., Palandrani, G., Manfredi, B., Romeo, E., De Martis, D., Todaro, C., Rodriguez y Baena, R., & Lupi, S. M. (2023). Difference of Two Antiseptic Gels for the Treatment of Peri-Implant Mucositis on Plaque Index and Bleeding Score: A Randomized Controlled Clinical Study. Applied Sciences, 13(3), 1288. https://doi.org/10.3390/app13031288