
Evaluation of Removable Partial Denture Metal Frameworks Produced by Digital Methods—A Systematic Review


Abstract
:1. Introduction
2. Materials and Methods
3. Results
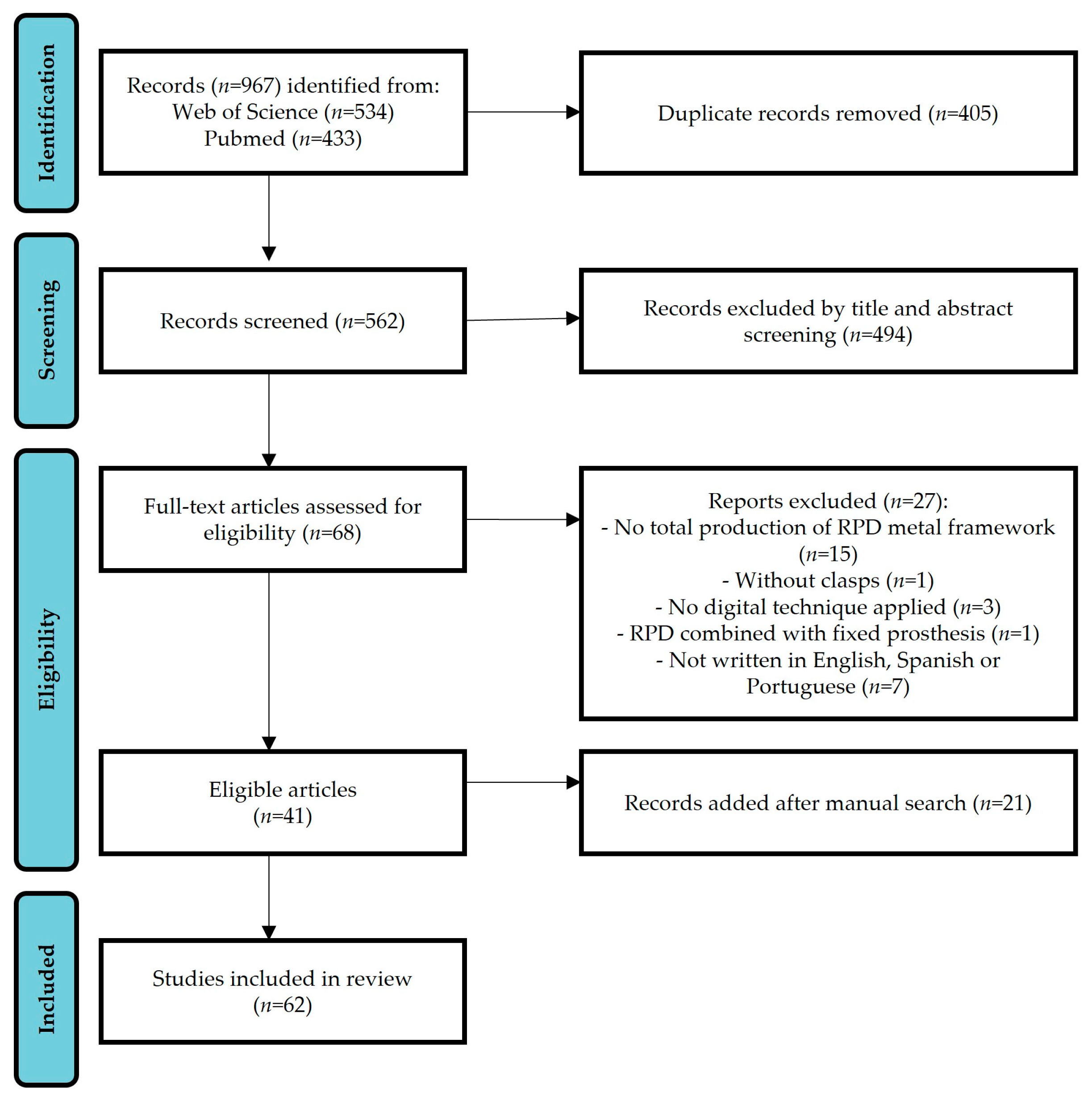
3.1. Search Results
3.2. Main Characteristics of the Studies
3.3. Fit Assessment Outcomes
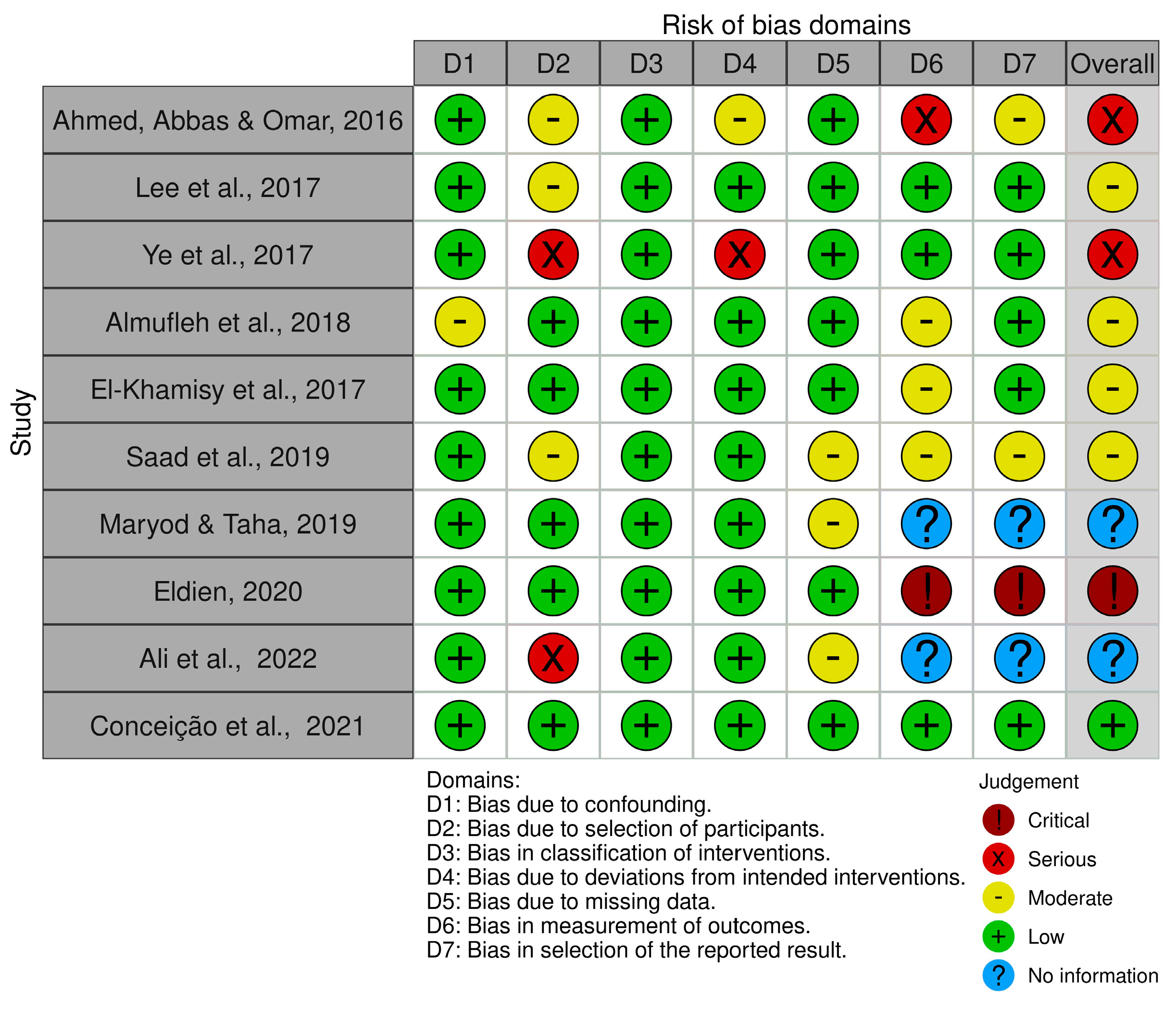
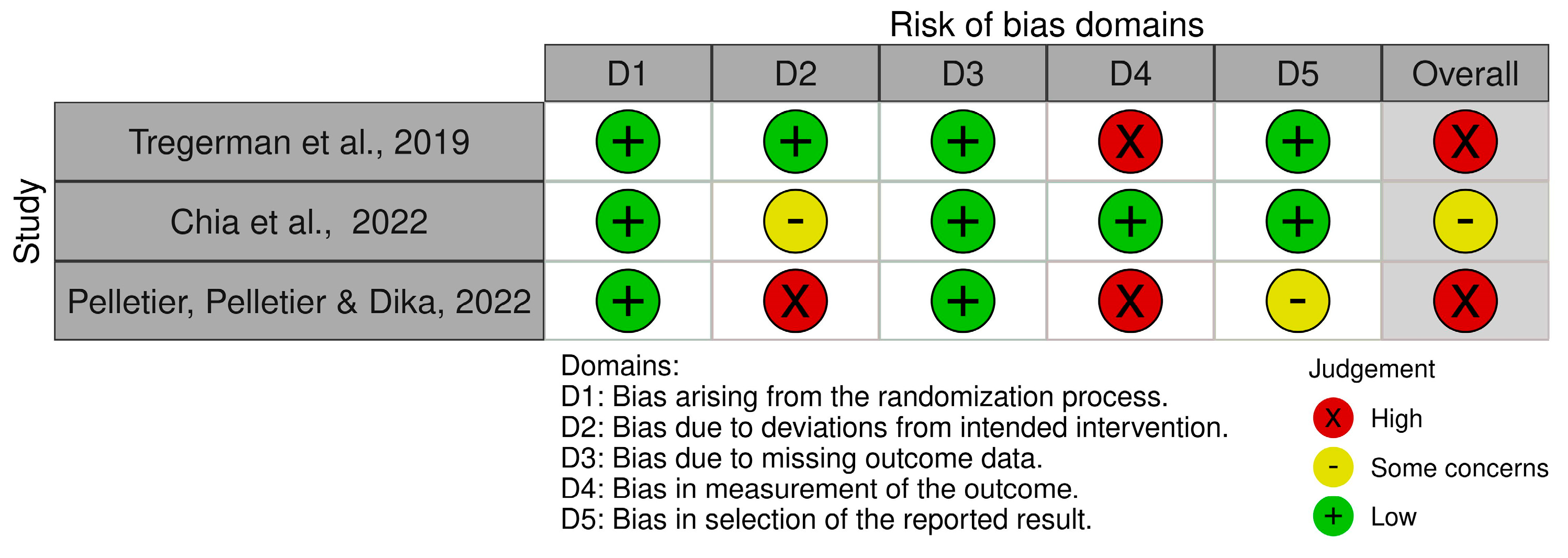
3.4. Risk of Bias
4. Discussion
4.1. Production Protocols Used in the Studies
4.2. Fit Assessment Evaluation
4.3. Future Approaches
5. Conclusions
- -
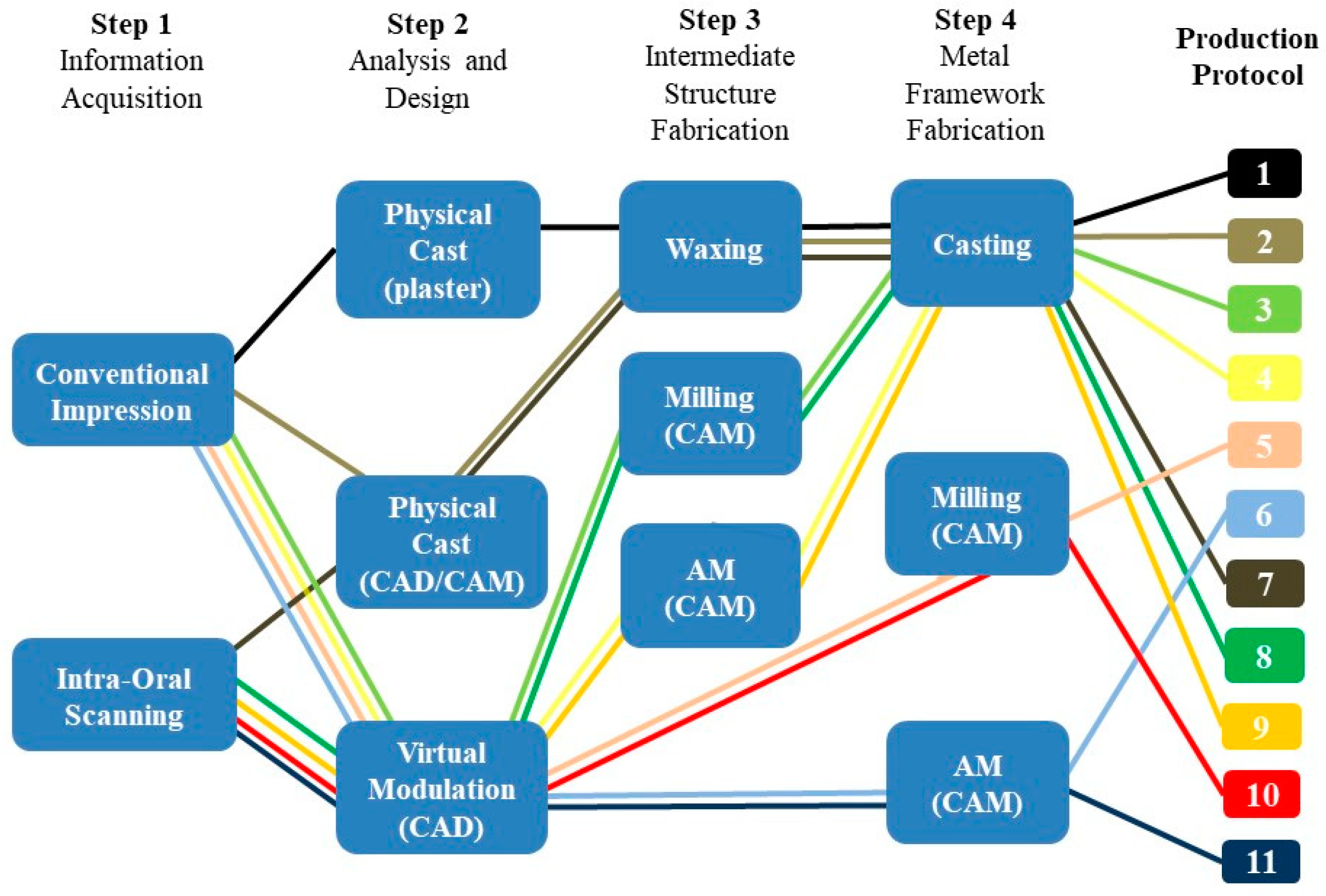
- Eleven protocols of different combinations of digital and conventional techniques to produce an RPD metal framework can be described;
- -
- All studied protocols with digital techniques exhibit fit accuracy within the acceptable clinical range for RPDs;
- -
- The protocol that combines direct metal additive manufacturing with the conventional impression (protocol 6) was the most frequently used in the literature and presented better qualitative and quantitative fit accuracy outcomes in comparison with the other digital protocols;
- -
- Considering the number of studies and the fit accuracy outcomes, protocol 6 seems to be the best alternative to the conventional protocol, ensuring a good fit within a reasonable cost and time investment. However, more studies are needed to support these conclusions since the low scientific evidence quality and the significant heterogeneity of the methodologies applied in the included papers show that there is still much room for improvement.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kreyer, R. Digital partial design and manufacturing: Using 3D printing technology to fabricate removable partial denture frameworks. Inside Dent. Technol. 2012, 3, 2–5. Available online: https://www.aegisdentalnetwork.com/idt/2012/08/digital-partial-design-and-manufacturing (accessed on 13 May 2022).
- Campbell, S.D.; Cooper, L.; Craddock, H.; Hyde, T.P.; Nattress, B.; Pavitt, S.H.; Seymour, D.W. Removable partial dentures: The clinical need for innovation. J. Prosthet. Dent. 2017, 118, 273–280. [Google Scholar] [CrossRef]
- Lima, J.M.; Anami, L.C.; Araujo, R.M.; Pavanelli, C.A. Removable partial dentures: Use of rapid prototyping. J. Prosthodont. 2014, 23, 588–591. [Google Scholar] [CrossRef]
- Almufleh, B.; Emami, E.; Alageel, O.; de Melo, F.; Seng, F.; Caron, E.; Nader, S.A.; Al-Hashedi, A.; Albuquerque, R.; Feine, J.; et al. Patient satisfaction with laser-sintered removable partial dentures: A crossover pilot clinical trial. J. Prosthethic Dent. 2018, 119, 560–567.e1. [Google Scholar] [CrossRef]
- Kim, J.J. Revisiting the removable partial denture. Dent. Clin. North Am. 2019, 63, 263–278. [Google Scholar] [CrossRef]
- Batisse, C.; Bonnet, G.; Nongert, P.; Gourrier, Y.; Bessadet, M.; Veyrune, J.L.; Nicolas, E. Optical impression and removable partial denture: An accurate and actual solution? J. Dent. Oral Health 2017, 3, 78. Available online: https://www.scientonline.org/open-access/optical-impression-and-removable-partial-denture-an-accurate-and-actual-solution.pdf (accessed on 13 May 2022).
- Yager, S.; Ma, J.; Ozcan, H.; Kilinc, H.I.; Elwany, A.H.; Karaman, I. Mechanical properties and microstructure of removable partial denture clasps manufactured using selective laser melting. Addit. Manuf. 2015, 8, 117–123. [Google Scholar] [CrossRef]
- Husain, N.A.-H.; Ozcan, M.; Shimmel, M.; Abou-Ayash, S. A digital cast-free clinical workflow for oral rehabilitation with removable partial dentures: A dental technique. J. Prosthethic Dent. 2020, 123, 680–685. [Google Scholar] [CrossRef]
- Anes, V.; Neves, C.B.; Bostan, V.; Gonçalves, S.; Reis, L. Evaluation of the retentive forces from removable partial denture clasps manufactured by the digital method. Appl. Sci. 2023, 13, 8072. [Google Scholar] [CrossRef]
- Puskar, T.; Jevremovic, D.; Williams, R.J.; Eggbeer, D.; Vukelic, D.; Budak, I. A Comparative Analysis of the Corrosive Effect of Artificial Saliva of Variable pH on DMLS and Cast Co-Cr-Mo Dental Alloy. Materials 2014, 7, 6486–6501. [Google Scholar] [CrossRef]
- Dikova, T. Properties of Co-Cr Dental Alloys Fabricated Using Additive Technologies. In Biomaterials in Regenerative Medicine; Dobrzanski, L.A., Ed.; IntechOpen: London, UK, 2017; Available online: https://www.intechopen.com/chapters/56100 (accessed on 4 September 2022).
- Lee, W.-T.; Chen, Y.-C. Digitally fabricated dentures for full mouth rehabilitation with zirconia, polyetheretherketone and selective laser melted Ti-6Al-4V material. Int. J. Environ. Res. Public Health 2022, 19, 3021. [Google Scholar] [CrossRef]
- Neves, C.B.; Costa, J.; Nepomuceno, L.; Madeira, A.; Portugal, J.; Bettencourt, A. Microhardness and Flexural Strength after Chemical Aging of chlorhexidine delivery systems based on acrylic resin. Rev. Port. Estomatol. Med. Dentária E Cir. Maxilofac. 2019, 60, 104–110. [Google Scholar] [CrossRef]
- Ohkubu, C.; Sato, Y.; Nishiyama, Y.; Suzuki, Y. Titanium removable denture based on a one-metal rehabilitation concept. Dent. Mater. J. 2017, 36, 517–523. [Google Scholar] [CrossRef]
- Tan, F.B.; Song, J.L.; Wang, C.; Fan, Y.B.; Dai, H.W. Titanium clasp fabricated by selective laser melting, CNC milling, and conventional casting: A comparative in vitro in vitro study. J. Prosthodont. Res. 2019, 63, 58–65. [Google Scholar] [CrossRef]
- Alageel, O.; Abdallah, M.N.; Alsheghri, A.; Song, J.; Caron, E.; Tamimi, F. Removable partial denture alloys processed by laser-sintering technique. J. Biomed. Mater. Res. B Appl. Biomater. 2018, 106, 1174–1185. [Google Scholar] [CrossRef]
- Arafa, K.A. Assessment of the fit of removable partial denture fabricated by computer-aided designing/computer aided manufacturing technology. Saudi Med. J. 2018, 39, 17–22. [Google Scholar] [CrossRef]
- Stern, M.A.; Brudvik, J.S.; Frank, R.P. Clinical evaluation of removable partial denture rest seat adaptation. J. Prosthet. Dent. 1985, 53, 658–662. [Google Scholar] [CrossRef]
- Bibb, R.J.; Eggbeer, D.; Williams, R.J.; Woodward, A. Trial fitting of a removable partial denture framework made using computer-aided design and rapid prototyping techniques. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2006, 220, 793–797. [Google Scholar] [CrossRef]
- Rudd, R.W.; Rudd, K.D. A review of 243 errors possible during the fabrication of a removable partial denture: Part I. J. Prosthethic Dent. 2001, 86, 251–261. [Google Scholar] [CrossRef]
- Frank, R.P.; Brudvik, J.S.; Leroux, B.; Milgrom, P.; Hawkins, N. Relationship between the standards of removable partial denture construction, clinical acceptability, and patient satisfaction. J. Prosthet. Dent. 2000, 83, 521–527. [Google Scholar] [CrossRef]
- Keltjens, H.M.; Mulder, J.; Käyser, A.F.; Creugers, N.H. Fit of direct retainers in removable partial dentures after 8 years of use. J. Oral Rehabil. 1997, 24, 138–142. [Google Scholar] [CrossRef]
- Dunham, D.; Brudvik, J.S.; Morris, W.J.; Plummer, K.D.; Cameron, S.M. A clinical investigation of the fit of removable partial dental prosthesis clasp assemblies. J. Prosthet. Dent. 2006, 95, 323–326. [Google Scholar] [CrossRef]
- Bettencourt, A.; Florindo, H.F.; Ferreira, I.F.S.; Matos, A.; Monteiro, J.; Neves, C.; Lopes, L.P.; Calado, A.; Castro, M.; Almeida, A.J. Incorporation of tocopherol acetate-containing particles in acrylic bone cement. J. Microencapsul. 2010, 27, 533–541. [Google Scholar] [CrossRef]
- Abduo, J.; Lyons, K.; Bennamoun, M. Trends in computer-aided manufacturing in prosthodontics: A review of the available streams. Int. J. Dent. 2014, 2014, 783948. [Google Scholar] [CrossRef]
- Lang, L.A.; Tulunoglu, I. A critically appraised topic review of computer-aided design/computer-aided machining of removable partial denture frameworks. Dent. Clin. North Am. 2014, 58, 247–255. [Google Scholar] [CrossRef]
- Schweiger, J.; Güth, J.F.; Erdelt, K.J.; Edelhoff, D.; Schubert, O. Internal porosities, retentive force, and survival of cobalt–chromium alloy clasps fabricated by selective laser-sintering. J. Prosthodont. Res. 2020, 64, 210–216. [Google Scholar] [CrossRef]
- Sun, J.; Zhang, F.Q. The application of rapid prototyping in prosthodontics. J. Prosthodont. 2012, 21, 641–644. [Google Scholar] [CrossRef]
- Ye, H.; Ning, J.; Li, M.; Niu, L.; Yang, J.; Sun, Y.; Zhou, Y. Preliminary clinical application of removable partial denture frameworks fabricated using computer aided design and rapid prototyping techniques. Int. J. Prosthodont. 2017, 30, 348–353. [Google Scholar] [CrossRef]
- Tregerman, I.; Renne, W.; Kelly, A.; Wilson, D. Evaluation of removable partial denture frameworks fabricated using 3 different techniques. J. Prosthet. Dent. 2019, 122, 390–395. [Google Scholar] [CrossRef]
- Conceição, P.; Portugal, J.; Franco, M.; Alves, N.M.; Marques, D.; Neves, C.B. Comparison between digital superimposition and microcomputed tomography methods of fit assessment of removable partial denture frameworks. J. Prosthet. Dent. 2023, in press. [Google Scholar] [CrossRef]
- Pereira, A.L.C.; Medeiros, A.K.B.; Santos, K.S.; Almeida, E.O.; Barbosa, G.A.S.; Carreiro, A.F.P. Accuracy of CAD-CAM systems for removable partial denture framework fabrication: A systematic review. J. Prosthet. Dent. 2021, 125, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and Meta-Analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 88, 105906. [Google Scholar] [CrossRef]
- OCEBM Levels of Evidence Working Group. The Oxford 2011 Levels of Evidence; Oxford Centre for Evidence-Based Medicine: Oxford, UK, 2011; Available online: http://www.cebm.net/index.aspx?o=5 (accessed on 5 March 2022).
- Williams, R.J.; Bibb, R.; Rafik, T. A technique for fabricating patterns for fabricating patterns for removable partial denture frameworks using digitized casts and electronic surveying. J. Prosthet. Dent. 2004, 91, 85–88. [Google Scholar] [CrossRef]
- Eggbeer, D.; Bibb, R.J.; Williams, R.J. The computer-aided design and rapid prototyping fabrication of removable partial denture frameworks. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2005, 219, 195–202. [Google Scholar] [CrossRef]
- Bibb, R.; Eggbeer, D.; Williams, R. Rapid manufacture of removable partial denture frameworks. Rapid Prototyp. J. 2006, 12, 95–99. [Google Scholar] [CrossRef]
- Williams, R.J.; Bibb, R.; Eggbeer, D.; Collis, J. Use of CAD/CAM technology to fabricate a removable partial denture framework. J. Prosthet. Dent. 2006, 96, 96–99. [Google Scholar] [CrossRef]
- Yan, G.-d.; Liao, W.-H.; Dai, N.; Yang, L.; Gao, Y.-G.; Zhu, S.-Y.; Cai, Y.-H. The Computer-Aided Design and Rapid Prototyping Fabrication of Removable Partial Denture Framework. In Proceedings of the 2nd IEEE International Conference on Computer Science and Information Technology, Beijing, China, 8–11 August 2009; pp. 266–268. [Google Scholar] [CrossRef]
- Han, J.; Wang, Y.; Lü, P. A preliminary report of designing removable partial denture framework using a specifically developed software package. Int. J. Prosthodont. 2010, 23, 370–375. [Google Scholar]
- Chen, G.; Zen, X.Y.; Wang, Z.; Guan, K.; Peng, C.W. Fabrication of removable partial framework by selective laser melting. Adv. Mater. Res. 2011, 317, 174–178. [Google Scholar] [CrossRef]
- Wu, J.; Wang, X.; Zhao, X.; Zhang, C.; Gao, B. A study on the fabrication method of removable partial denture framework by computer-aided design and rapid prototyping. Rapid Prototyp. J. 2012, 18, 318–323. [Google Scholar] [CrossRef]
- Kattadiyil, M.T.; Mursic, Z.; AlRumaih, H.; Goodacre, C.J. Intraoral scanning of hard and soft tissues for partial removable dental prosthesis fabrication. J. Prosthet. Dent. 2014, 112, 444–448. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.-S.; Lee, J.-Y.; Shin, S.-W. Fabricating an obturator using rapid prototyping to design the framework: A case report. Int. J. Prosthodont. 2014, 27, 439–441. [Google Scholar] [CrossRef]
- Lee, J.-H.; Lee, C.-H. A stereolithographic resin pattern for evaluating the framework, altered cast partial removable dental prosthesis impression, and maxillomandibual relationship record in a single appointment. J. Prosthet. Dent. 2015, 114, 625–626. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, F.A.; Faten, S.A.; Samia, S.O. Clinical and cytological evaluation of removable partial denture fabricated by selective laser sintering additive prototyping technique. Alex. Dent. J. 2016, 41, 42–49. [Google Scholar] [CrossRef]
- Arnold, C.; Hey, J.; Schweyen, R.; Setz, J.M. Accuracy of CAD-CAM-fabricated removable partial dentures. J. Prosthet. Dent. 2018, 119, 586–592. [Google Scholar] [CrossRef]
- Mansour, M.; Sanchez, E.; Machado, C. The use of digital impressions to fabricate tooth-supported partial removable dental prostheses: A clinical report. J. Prosthodont. 2016, 25, 495–497. [Google Scholar] [CrossRef]
- Hu, F.; Pei, Z.; Wen, Y. Using intraoral scanning technology for three-dimensional printing of Kennedy class I removable partial denture metal framework: A clinical report. J. Prosthodont. 2019, 28, e473–e476. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.-W.; Park, J.M.; Park, E.J.; Heo, S.J.; Koak, J.Y.; Kim, S.K. Accuracy of a digital removable partial denture fabricated by casting a rapid prototyped pattern: A clinical study. J. Prosthet. Dent. 2017, 118, 468–474. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Li, Y.; Zhang, Y. Use of intraoral scanning and 3-dimensional printing in the fabrication of a removable partial denture for a patient with a limited mouth opening. J. Am. Dent. Assoc. 2017, 148, 338–341. [Google Scholar] [CrossRef]
- Soltanzadeh, P.; Suprono, M.S.; Kattadiyil, M.T.; Goodacre, C.; Gregorius, W. An in vitro investigation of accuracy and fit of conventional and CAD/CAM removable partial denture frameworks. J. Prosthodont. 2019, 28, 547–555. [Google Scholar] [CrossRef]
- Bajunaid, S.O.; Altwaim, B.; Alhassan, M.; Alammari, R. The Fit Accuracy of Removable Partial Denture Metal Frameworks Using Conventional and 3D Printed Techniques: An In Vitro Study. J. Contemp. Dent. Pract. 2019, 20, 476–481. [Google Scholar]
- Chen, H.; Li, H.; Zhao, Y.; Zhang, X.; Wang, Y.; Lyu, P. Adaptation of removable partial denture frameworks fabricated by selective laser melting. J. Prosthet. Dent. 2019, 122, 316–324. [Google Scholar] [CrossRef] [PubMed]
- Mendes, T.A.; Marques, D.; Lopes, L.P.; Caramês, J. Total digital workflow in the fabrication of a partial removable dental prostheses: A case report. SAGE Open Med. Case Rep. 2019, 7, 2050313X19871131. [Google Scholar] [CrossRef] [PubMed]
- Tasaka, A.; Shimizu, T.; Kato, Y.; Okano, H.; Ida, Y.; Higuchi, S.; Yamashita, S. Accuracy of removable partial denture framework fabricated by casting with a 3D printed pattern and selective laser sintering. J. Prosthodont. Res. 2020, 64, 224–230. [Google Scholar] [CrossRef]
- Pereira, A.L.C.; Aquino, L.M.M.; Freitas, R.F.C.P.; Tôrres, A.C.S.P.; Carreiro, A.F.P. CAD/CAM-fabricated removable partial denture: A case report. Int. J. Comput. Dent. 2019, 22, 317–379. [Google Scholar]
- Peng, P.-W.; Hsu, C.Y.; Huang, H.Y.; Chao, J.C.; Lee, W.F. Trueness of removable partial denture frameworks additively manufactured wit selective laser melting. J. Prosthet. Dent. 2020, 127, 122–127. [Google Scholar] [CrossRef]
- Wu, J.; Cheng, Y.; Gao, B.; Yu, H. A novel digital cast impression technique for fabrication a removable partial denture with a distal extension. J. Am. Dent. Assoc. 2020, 151, 297–302. [Google Scholar] [CrossRef]
- Tasaka, A.; Okano, H.; Shimizu, T.; Kato, Y.; Higuchi, S.; Yamashita, S. Influence of reinforcement bar on accuracy of removable partial denture framework fabricated by casting with a 3D-printed pattern and selective laser sintering. J. Prosthodont. Res. 2021, 65, 213–218. [Google Scholar] [CrossRef]
- Rist, K.; Cimic, S. Selective laser melting in fabrication of partial denture metal framework. Res. J. Pharm. Biol. Chem. Sci. 2016, 7, 2039–2043. Available online: https://www.rjpbcs.com/pdf/2016_7(3)/[248].pdf (accessed on 23 June 2022).
- Lee, W.-F.; Wang, J.-C.; Hsu, C.-Y.; Peng, P.-W. Microstructure, mechanical properties, and retentive forces of cobalt-chromium removable partial denture frameworks fabricated by selective laser melting followed by heat treatment. J. Prosthethic Dent. 2022, 127, 115–121. [Google Scholar] [CrossRef]
- El-Khamisy, N.E.; Habib, A.H.; El-Mekawy, N.E.; Emera, R.M. Digital versus conventional design for mandibular distal extension RPD: A study of passivity of RPD components and principal abutment alveolar bone height changes. Mansoura J. Dent. 2017, 4, 6–13. Available online: https://www.academia.edu/36180078/Digital_Versus_Conventional_Design_For_Mandibular_Distal_Extension_RPD_A_Study_of_Passivity_of_RPD_Components_and_Principal_Abutment_Alveolar_Bone_Height_Changes (accessed on 23 June 2022).
- Malara, P.; Dobrzanski, L.B.; Dobrzanska, J. Computer-aided designing and manufacturing of partial removable dentures. J. Achiev. Mater. Manuf. Eng. 2015, 73, 157–164. [Google Scholar]
- Saad, A.S.; Abbas, F.S.; Elgharabawy, S.H. Clinical evaluation of removable partial denture constructed from 3D printed resin pattern designs using CAD CAM technology. Alex. Dent. J. 2019, 44, 1–7. [Google Scholar] [CrossRef]
- Carreiro, A.F.P.; Pereira, A.L.; Paz, C.O.; Cardoso, R.G.; Medeiros, C.R.P.; Medeiros, A.K.B.; Freitas, R.F.C.P. The computer-aided design and rapid prototyping fabrication of removable partial denture framework for occlusal rehabilitation: Clinical report. Res. Soc. Dev. 2020, 9, e9891210692. [Google Scholar] [CrossRef]
- Hwang, S.; An, S.; Robles, U.; Rumpf, R.C. Process parameter optimization for removable partial denture frameworks manufactured by selective laser melting. J. Prosthet. Dent. 2023, 129, 191–198. [Google Scholar] [CrossRef]
- Cabrita, J.P.; Mendes, T.A.; Martins, J.P.; Lopes, L. Removable partial denture metal framework manufactured by selective laser melting technology—A clinical report. Rev. Port. Estomatol. Med. Dentária E Cir. Maxilofac. 2021, 62, 109–113. [Google Scholar] [CrossRef]
- Maryod, W.H.; Taha, E.R. Comparison of the retention of conventional versus digitally fabricated removable partial dentures. A cross over study. Int. J. Dent. Oral Health 2019, 5, 13–19. Available online: https://www.biocoreopen.org/ijdoh/Comparison-of-the-retention-of-conventional-versus-digitally.php (accessed on 11 July 2022).
- Eldien, A.R. Polyetherether Ketone (PEEK) versus Metallic Kennedy Class III Removable Partial Dentures: Evaluation of Retention Force. Master’s Thesis, Mansoura University, Mansoura, Egypt, 2020. Available online: https://www.researchgate.net/profile/Mohammed-Fouad-3/publication/342701195_Polyetherether_Ketone_PEEK_versus_Metallic_Kennedy_Class_III_Removable_Partial_Dentures_Evaluation_of_Retention_Force/links/5f01d8ae92851c52d619c276/Polyetherether-Ketone-PEEK-versus-Metallic-Kennedy-Class-III-Removable-Partial-Dentures-Evaluation-of-Retention-Force.pdf (accessed on 12 July 2022).
- Kobayashi, H.; Tasaka, A.; Higuchi, S.; Yamashita, S. Influence of molding angle on the trueness and defects of removable partial denture frameworks fabricated by selective laser melting. J. Prosthodont. Res. 2021, 66, 589–599. [Google Scholar] [CrossRef]
- Muehlemann, E.; Ozcan, M. Accuracy of removable partial denture frameworks fabricated using conventional and digital technologies. Eur. J. Prosthodont. Restor. Dent. 2022, 30, 76–86. [Google Scholar] [CrossRef]
- Pugliese, A.; Cataneo, E.; Fortunato, L. Construction of a removable partial denture (RPD): Comparison between the analog procedure and the selective laser melting procedure. Prosthesis 2021, 3, 428–436. [Google Scholar] [CrossRef]
- Snosi, A.M.; Lotfy, S.M.; Thabet, Y.G.; Sabet, M.E.; Rizk, F.N. Subtractive versus additive indirect manufacturing techniques of digitally designed partial dentures. J. Adv. Prosthodont. 2021, 13, 327–332. [Google Scholar] [CrossRef]
- Suzuki, Y.; Harada, N.; Watanabe, K.I.; Maruo, R.; Shimpo, H.; Ohkubo, C. Clinical application of an intraoral scanner and CAD/CAM system for a Kennedy class I. J. Oral Sci. 2022, 64, 109–111. [Google Scholar] [CrossRef] [PubMed]
- Ali, Z.; Wood, D.; Elmougy, A.; Kelleher, P.; Martin, N. Laboratory evaluation of production efficiency for removable partial denture frameworks using in-house casting versus outsourced additive manufacturing techniques. Int. J. Prosthodont. 2023, 36, 338–342. [Google Scholar] [CrossRef]
- Oh, K.C.; Jeon, J.; Kim, J.-H. Top-down design and fabrication with digital technology of removable partial dentures incorporating custom abutments: A dental technique. J. Prosthet. Dent. 2022, in press. [Google Scholar] [CrossRef] [PubMed]
- Zhang, N.; Mao, B.; Yu, P.; Chen, S.; Chen, X.; Yu, H. Digital workflow for a scleroderma patient with microstomia: A clinical report. J. Prosthodont. 2021, 30, 376–383. [Google Scholar] [CrossRef] [PubMed]
- Conceição, P.; Franco, M.; Alves, N.; Portugal, J.; Neves, C.B. Fit accuracy of removable partial denture metal frameworks produced by CAD-CAM—A clinical study. Rev. Port. Estomatol. Med. Dentária E Cir. Maxilofac. 2021, 62, 194–200. [Google Scholar] [CrossRef]
- Maraka, N.; Salloum, A.; Al-Mohareb, M.; Shihabi, S. Evaluation of the fit Accuracy of removable partial denture frameworks fabricated using three different techniques: An in vitro study. Int. J. Dent. Oral Sci. 2021, 8, 4881–4886. Available online: https://www.researchgate.net/profile/Nariman-Maraka/publication/355890070_Evaluation_of_the_Fit_Accuracy_of_Removable_Partial_Denture_Frameworks_Fabricated_Using_Three_Different_Techniques_An_In_Vitro_Study/links/6182f2800be8ec17a96a1ae3/Evaluation-of-the-Fit-Accuracy-of-Removable-Partial-Denture-Frameworks-Fabricated-Using-Three-Different-Techniques-An-In-Vitro-Study.pdf (accessed on 23 July 2023). [CrossRef]
- Piao, X.-Y.; Jeon, J.; Shim, J.-S.; Park, J.-M. A digital workflow for the fabrication of a milled removable partial denture. Int. J. Environ. Res. Public Health 2022, 19, 8540. [Google Scholar] [CrossRef]
- Alabdullah, S.A.; Hannam, A.G.; Wyatt, C.C.; McCullagh, A.P.G.; Aleksejuniene, J.; Mostafa, N.Z. Comparison of digital and conventional methods of fit evaluation of partial removable dental prosthesis frameworks fabricated by selective laser melting. J. Prosthet. Dent. 2022, 127, 478.e1–478.e10. [Google Scholar] [CrossRef]
- Chia, V.A.P.; Toh, Y.L.S.; Quek, H.C.; Pokharkar, Y.; Yap, A.U.; Yu, N. Comparative clinical evaluation of removable partial denture frameworks fabricated traditionally or with selective laser melting: A randomized controlled trial. J. Prosthet. Dent. 2022, in press. [Google Scholar] [CrossRef]
- Rokhshad, R.; Tehrani, A.M.; Nahidi, R.; Zarbakhsh, A. Fit of removable partial denture frameworks fabricated from 3D-printed patterns versus the conventional method: An in vitro comparison. J. Prosthet. Dent. 2022, in press. [Google Scholar] [CrossRef]
- Cameron, A.B.; Evans, J.L.; Robb, N.D. A technical and clinical digital approach to the altered cast technique with an intraoral scanner and polyvinyl siloxane impression material. J. Prosthet. Dent. 2022, 15. in press. [Google Scholar] [CrossRef]
- Pelletier, S.; Pelletier, A.; Dika, A. Adaptation of removable partial denture rest seats in prostheses made with selective laser sintering or casting techniques: A randomized clinical trial. J. Prosthet. Dent. 2022, in press. [Google Scholar] [CrossRef]
- Oh, K.C.; Jeon, J.; Kim, J.H. Fabrication of a removable partial denture combining conventional and digital techniques. J. Prosthet. Dent. 2021, 125, 588–591. [Google Scholar] [CrossRef]
- Hamed, H.A.; Hebeshi, A.M.; Husseiny, E. Effect of palatal vault depth on the trueness of metal laser-sintered and cast cobalt-chromium removable partial denture frameworks. J. Prosthodont. 2022, 32, 353–360. [Google Scholar] [CrossRef]
- Liedke, G.S.; Spin-Neto, R.; Vizzotto, M.B.; da Silveira, P.F.; Wenzel, A.; da Silveira, H.E. Diagnostic accuracy of cone beam computed tomography sections with various thicknesses for detecting misfit between the tooth and restoration in metal-restored teeth. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2015, 120, 131–137. [Google Scholar] [CrossRef]
- Ye, H.; Li, X.; Wang, G.; Kang, J.; Liu, Y.; Sun, Y.; Zhou, Y. A novel computer-aided design/computer-assisted manufacture method for one-piece removable partial denture evaluation of fit. Int. J. Prosthodont. 2018, 31, 149–151. [Google Scholar] [CrossRef]
- Costa, J.; Matos, A.; Bettencourt, A.; Portugal, J.; Neves, C.B. Effect of Ethanol Solutions as Post-Polymerization Treatment on the Properties of Acrylic Reline Resins. Rev. Port. Estomatol. Med. Dentária E Cir. Maxilofac. 2016, 57, 215–222. [Google Scholar] [CrossRef]
- Duret, F.; Blouin, J.-L.; Duret, B. CAD-CAM in dentistry. J. Am. Dent. Assoc. 1988, 117, 715–720. [Google Scholar]
- Hayama, H.; Fueki, K.; Wadacho, J.; Wakabayashi, N. Trueness and precision of digital impressions obtained using an intraoral scanner with different head size in the partially edentulous mandible. J. Prosthodont. Res. 2018, 62, 347–352. [Google Scholar] [CrossRef]
- Gan, N.; Xiong, Y.; Jiao, T. Accuracy of intraoral digital impressions for whole upper jaws, including full dentitions and palatal soft tissues. PLoS ONE 2016, 11, e0158800. [Google Scholar] [CrossRef]
- Revilla-Léon, M.; Ozcan, M. Additive manufacturing technologies used for 3D metal printing in dentistry. Curr. Oral Health Rep. 2017, 4, 201–208. [Google Scholar] [CrossRef]
- Dobrzanski, L.A.; Borazanski, L.B. Dentistry 4.0 concept in the design and manufacturing of prosthetic dental restorations. Processes 2020, 8, 525–572. [Google Scholar] [CrossRef]
- Alharbi, N.; Wismeijer, D.; Osman, R.B. Additive Manufacturing Techniques in Prosthodontics: Where do we Currently Stand? A Critical Review. Int. J. Prosthodont. 2017, 30, 474–484. [Google Scholar] [CrossRef]
- Harb, I.E.; Abdel-Khalek, E.A.; Hegazy, S.A. CAD/CAM Constructed poly(etheretherketone) (PEEK) framework of Kennedy class I removable partial denture: A clinical report. Am. Coll. Prosthodont. 2019, 28, 595–598. [Google Scholar] [CrossRef]
- Negm, E.E.; Aboutaleb, F.A.; Alam-Eldein, A. Virtual evaluation of the accuracy of fit and trueness in maxillary poly(etheretherketone) removable partial denture frameworks fabricated by direct and indirect CAD/CAM techniques. J. Prosthodont. 2019, 28, 804–810. [Google Scholar] [CrossRef]
- Papathanasiou, I.; Kamposiora, P.; Papavasiliou, G.; Ferrari, M. The use of PEEK in digital prosthodontics: A narrative review. BMC Oral Health 2020, 20, 217. [Google Scholar]
- Laverty, D.P.; Thomas, M.B.; Clark, P.; Addy, L.D. The use of metal printing (direct metal laser sintering) in removable prosthodontics. Dent. Update 2016, 43, 826–835. [Google Scholar] [CrossRef]
- Kim, S.Y.; Shin, S.-Y.; Lee, J.H. Effect of cyclic bend loading on a cobalt-chromium clasp fabricated by direct metal laser sintering. J. Prosthet. Dent. 2018, 119, e1–e7. [Google Scholar] [CrossRef]
- Brudvik, J.S.; Reimers, D. The tooth-removable partial denture interface. J. Prosthet. Dent. 1992, 68, 924–927. [Google Scholar] [CrossRef]
- Nakata, T.; Shimpo, H.; Ohkubo, C. Clasp fabrication using one-process molding by repeated laser sintering and high-speed milling. J. Prosthodont. Res. 2017, 61, 276–282. [Google Scholar] [CrossRef] [PubMed]
- Torii, M.; Nakata, T.; Takahashi, K.; Kawamura, N.; Shimpo, H.; Ohkubo, C. Fitness and retentive force of cobalt-chromium alloy clasps fabricated with repeated laser sintering and milling. J. Prosthodont. Res. 2018, 62, 342–346. [Google Scholar] [CrossRef] [PubMed]
- Peng, T.Y.; Shimoe, S.; Tanoue, N.; Akebono, H.; Murayama, T.; Satoda, T. Fatigue resistance of yttria-stabilized tetragonal zirconia polycrystal clasps for removable partial dentures. Eur. J. Oral Sci. 2019, 127, 269–275. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Study Design | Sample Size | Level of Evidence | Information Acquisition (Equipment) | Analysis and Design (Software) | Intermediate Structure (Technique) | Framework Fabrication | Type of Metal (Brand) | Production Protocol |
|---|---|---|---|---|---|---|---|---|---|
| Williams, Bibb & Rafik, 2004 [36] | In vitro study | 2 | - | CImp+eOS (Comet 250) | CAD (Polyworks + Spyder + Matlab Surface Studio) | AM (SLA) | Casting | Co-Cr (Ndd) | 4 |
| Eggbeer, Bibb & Williams, 2005 [37] | In vitro study | 1 | - | CImp+eOS (Comet 250) | CAD (Polyworks + Spyder + FreeForm SensAble) | AM (SLA; JET) | Casting | Co-Cr (Nd) | 4 |
| Bibb et al., 2006 [19] | Case report | 1 | 4 | CImp+eOS (Comet 250) | CAD (Polyworks + Spyder + FreeForm SensAble) | AM (SLA) | Casting | Co-Cr (Nd) | 4 |
| Bibb & Eggbeer, 2006 [38] | Case report | 1 | 4 | CImp+eOS (Comet 250) | CAD (Polyworks + Spyder + FreeForm SensAble) | - | AM (SLM: Realizer 2) | Co-Cr (Nd) | 6 |
| Williams et al., 2006 [39] | Case report | 1 | 4 | CImp+eOS (Comet 250) | CAD (Polyworks + Spyder + FreeForm SensAble) | - | AM (SLM: Realizer 2) | Co-Cr (Nd) | 6 |
| Yan et al., 2009 [40] | Case report | 1 | 4 | CImp+eOS (Nd) | CAD (Nd) | AM (SLA) | Casting | Co-Cr (Nd) | 4 |
| Han, Wang & Lü, 2010 [41] | Case report | 2 | 4 | CImp+eOS (CXM-I) | CAD (Tang Long) | - | AM (SLM) | Nd | 6 |
| Chen et al., 2011 [42] | Case report | 2 | 4 | CImp+eOS (Not described) | CAD (Not described) | - | AM (SLM) | Ti (Nd) | 6 |
| Kreyer, 2012 [1] | Case report | 2 | 4 | CImp+eOS (3Shape D710) | CAD (3Shape DS) | AM (DLP; JET) | Casting | N dd | 4 |
| Wu et al., 2012 [43] | Case report | 1 | 4 | CImp+eOS (LSH600) | CAD (Geomagic Studio) | AM (SLA) | Casting | Co-Cr (Nd) | 4 |
| Kattadiyil et al., 2014 [44] | Case report | 1 | 4 | IntraS (Cadent iTero) | CAD (FreeForm SensAble) | AM (Nd) | Casting | Co-Cr (Nd) | 9 |
| Kim, Lee & Shin 2014 [45] | Case report | 1 | 4 | CImp+eOS (Nd) | CAD (FreeForm SensAble) | AM (Nd) | Casting | Nd | 4 |
| Lee & Lee, 2015 [46] | Case report | 1 | 4 | CImp+eOS (Nd | CAD (FreeForm SensAble) | AM (MJ) | Casting | Nd | 4 |
| Ahmed, Abbas & Omar, 2016 [47] | Clinical study | 6 | 2 | CImp+eOS (Nd) | CAD (3Shape DS) | - | AM (SLS: EOS M270 | Co-Cr (EOS SP2) | 6 |
| Arnold et al., 2018 [48] | In vitro study | 3 | - | CImp+eOS (3ShapeD900) | CAD (3Shape DS) | AM (Nd); MILL | Casting; AM (SLM: Concept Laser Mlab M1) | Co-Cr (Remanium Star CL) | 1, 3, 4, 6 |
| Mansour, Sanchez & Machado, 2016 [49] | Case report | 2 | 4 | IntraS (LAVA COS 3M) | Physical cast (Resin) | Waxing | Casting | Co-Cr (Nd) | 7 |
| Batisse et al., 2017 | Case report | 1 | 4 | IntraS (3Shape Trios) | CAD (3Shape DS) | - | AM (SLM: ProX DMP 200) | Co-Cr (Nd) | 11 |
| Hu, Pei& Wen, 2019 [50] | Case report | 1 | 4 | IntraS (3Shape Trios) | CAD (3Shape DS) | - | AM (SLM: EOS M280) | Ti (Nissin) | 11 |
| Lee et al., 2017 [51] | Clinical study | 10 | 2 | CImp+eOS (Activity 101) | CAD (FreeForm SensAble) | AM (MJ) | Casting | Nd | 4 |
| Wu, Li& Zhan, 2017 [52] | Case report | 1 | 4 | IntraS (CEREC Omnicam) | CAD (3Shape DS) | - | AM (SLM: BLT S200) | Ti (Nd) | 11 |
| Ye et al., 2017 [29] | Clinical study | 15 | 2 | CImp+eOS (3Shape D800) | CAD (3Shape DS) | - | AM (Nd: EOS M270) | Co-Cr (Wirebond C+) | 1, 6 |
| Almufleh et al., 2018 [4] | Clinical study | 12 | 2 | CImp+eOS (Dental wings 3) | CAD (3Shape DS) | - | AM (SLS: Phenix PM100) | Co-Cr (Sint-Tech) | 1, 6 |
| Soltanzadeh et al., 2019 [53] | In vitro study | 10 | - | CImp+eOS (3Shape D900) | Physical cast (Resin), CAD (3Shape DS) | Waxing | Casting; AM (SLM: 3DRPD) | Co-Cr (Si-Tech ST2724G-A) | 1, 2, 6 |
| Husain et al., 2020 [8] | Case report | 1 | 4 | IntraS (3Shape Trios) | CAD (3Shape DS) | - | AM (SLM: EOS M270) | Co-Cr (Starbond Easy) | 11 |
| Bajunaid et al., 2019 [54] | In vitro study | 15 | - | ExtraS (Zirkonzahn S600) | CAD (3Shape DS) | - | AM (SLM: Concept laser Mlab) | Co-Cr (Remanium CL) | 1, 6 |
| Chen et al., 2019 [55] | In vitro study | 3 | - | CImp+eOS (IScan D104i) | CAD (3Shape DS) | - | AM (SLM: Concept laser Mlab) | Co-Cr (Remanium CL) | 1, 6 |
| Mendes et al., 2019 [56] | Case report | 1 | 4 | IntraS (3Shape Trios) | CAD (3Shape DS) | - | AM (SLM: EOS—Phibo) | Co-Cr (Nd) | 11 |
| Tasaka et al., 2020 [57] | In vitro study | 5 | - | CImp+eOS (Smart Big) | CAD (Digistell) | AM (MJ) | Casting; AM (DMLS: EOS M270) | Co-Cr (Nd) | 4, 6 |
| Tregerman et al., 2019 [30] | Clinical study (R) | 9 | 2 | CImp+eOS (3Shape D800) + IntraS (3Shape Trios) | CAD (3Shape DS) | - | AM (SLM) | Co-Cr (EOS SP2) | 1, 6, 11 |
| Pereira et al., 2019 [58] | Case report | 1 | 4 | IntraS (3Shape Trios) | CAD (Dental Wings) | AM (SLA) | Casting | Co-Cr (Remanium GM 280) | 9 |
| Peng et al., 2020 [59] | In vitro study | 6 | - | ExtraS (3 Shape D900) | CAD (3 Shape DS) | AM (SLA) | Casting; AM (SLM: Concept Laser Mlab Cusing) | Co-Cr (Wironit; Remanium; Ti (Rematitan) | 4, 6 |
| Wu et al., 2020 [60] | Case report | 1 | 4 | CImp+eOS (3Shape D850) | CAD (3Shape DS) | AM (SLM: Concept Laser M2) | Ti (Ti6Al4V) | 6 | |
| Tasaka et al., 2021 [61] | In vitro study | 5 | - | ExtraS (Smart Big) | CAD (Digistell) | AM (MJ) | Casting; AM (DMLS: EOSINT M270) | Co-Cr (EOS SP2) | 4, 6 |
| Rist & Cimic, 2016 [62] | Case report | 1 | 4 | CImp+eOS (Nd) | CAD (Nd) | AM (SLM: Nd) | Nd | 6 | |
| Lee et al., 2022 [63] | In vitro study | 5 | - | ExtraS (3Shape D900) | CAD (3Shape DS) | AM (SLA) | Casting; AM (SLM: ITRI AM System) | Co-Cr (Neoloy Denture) | 4, 6 |
| El-Khamisy et al., 2017 [64] | Clinical study | 6 | 2 | CImp+eOS (Shera eco-Scann7) | CAD (Nd) | - | MILL (Shera eco-mill 5x) | Co-Cr (Nd)) | 1, 5 |
| Malara et al., 2015 [65] | Case report | 1 | 4 | CImp+eOS (Nd) | CAD (Nd) | - | MILL (Nd) | Co-Cr (Nd) | 5 |
| Saad et al., 2019 [66] | Clinical study | 7 | 2 | CImp+eOS (3Shape D900) | CAD (3Shape DS) | AM (Nd) | Casting | Co-Cr (Nd) | 1, 4 |
| Carreiro et al., 2020 [67] | Case report | 2 | 4 | IntraS (3Shape Trios) | CAD (Dental Wings) | - | Casting | Co-Cr (Nd) | 9 |
| Hwang et al., 2021 [68] | In vitro study | 3 | - | ExtraS (3Shape E2) | CAD (Exocad Partial CAD) | - | AM (SLM: Dentium Metal Printer) | Ti (Nd) | 6 |
| Cabrita et al., 2021 [69] | Case report | 1 | 4 | CImp+eOS (3Shape D700) | CAD (3Shape DS) | - | AM (SLM: EOS Phibo) | Co-Cr (Nd) | 6 |
| Maryod & Taha, 2019 [70] | Clinical study | 20 | 2 | IntraS (3Shape Trios) | CAD (3Shape DS) | AM (DLP) | Casting | Co-Cr (Nd) | 1, 4 |
| Eldien, 2020 [71] | Clinical study | 10 | 2 | CImp+eOS (Ceramill map400) | CAD (Nd) | AM (Nd) | Casting | Co-Cr (Ticonium Premium 100) | 4 |
| Kobayashi et al., 2021 [72] | In vitro study | 10 | - | ExtraS (Smart Big) | CAD (Digistell) | - | AM (SLM: EOSINT M270) | Co-Cr (EOS SP2) | 6 |
| Muheleman&Ozcan, 2022 [73] | In vitro study | 3 | - | ExtraS (Nd) | CAD (Siladent SilaPart) | MILL; AM (MJ) | Casting; AM (SLM: Concept Laser; DMLS:ProX DMP 100) | Co-Cr (Siladent V); Co-Cr (Dentaurum Remanium star CL) | 1, 3, 4, 6 |
| Pugliese, Cataneo &Fortunato, 2021 [74] | Case report | 1 | 4 | CImp+eOS (Neway Open Tech 3D) | CAD (Nd) | - | AM (SLM: Nd) | Co-Cr (Nd) | 1, 6 |
| Snosi et al., 2021 [75] | In vitro study | 6 | - | ExtraS (3Shape D850) | CAD (3Shape DS) | MILL; AM (DLP) | Casting | Co-Cr (Bego Wirinium) | 3, 4 |
| Suzuki et al., 2022 [76] | Case report | 1 | 4 | IntraS (3Shape Trios) | CAD (Dental Wings) | - | AM (Nd: GE Concept Laser M2) | Ti (Ti-6Al-4V AP&C) | 11 |
| Ali et al., 2022 [77] | Clinical study | 25 | 2 | CImp+eOS | CAD (Nd) | - | Casting; AM (SLS: Nd) | Co-Cr (Nd) | 1, 6 |
| Oh, Jeon & Kim 2022 [78] | In vitro study | 10 | - | ExtraS (Medit Co. T500) | CAD (3Shape DS) | AM (DLP) | Casting; AM (Nd:Concept Laser Cusing 200R) | Co-Cr (Degudent Biosil F, Dentaurum Remanium star CL | 1, 4, 6 |
| Zhang et al., 2021 [79] | Case report | 2 | 4 | ExtraS (3Shape D2000) | CAD (Exocad Partial CAD) | - | AM (Nd) | Co-Cr (Nobilium Nobil Star Ultra) | 6 |
| Conceição et al., 2021 [80] | Clinical Study | 20 | 2 | ExtraS (Zirkonzahn S600 Arti) | CAD (Zirkonzahn Partial Planner) | - | AM (DMLS: EOSINT M270) | Co-Cr (EOS SP2) | 6 |
| Maraka et al., 2021 [81] | In vitro study | 5 | - | CImp+eOS (CS Ultra Pro) | CAD (Exocad Partial CAD) | - | AM (SLM: Sisma Mysint) | Co-Cr (Scheftner) | 1, 6 |
| Piao et al., 2022 [82] | Case report | 1 | 4 | CImp+eOS (Medit T500) | CAD (Exocad Partial CAD) | MILL | Casting | Nd | 3 |
| Alabdullah et al., 2022 [83] | In vitro study | 12 | - | CImp+eOS (Dentisply Sirona inEos X5) | CAD (3Shape DS) | - | AM (SLM: 3DRPD Co Lab) | Co-Cr (Nd) | 6 |
| Chia et al., 2022 [84] | Clinical Study (R) | 29 | 2 | CImp+eOS (3Shape D800) | CAD (3Shape DS) | - | AM (SLM: EOS M270) | Co-Cr (EOS SP2) | 1, 6 |
| Lee & Chen, 2022 [82] | Case report | 1 | 4 | CImp+eOS (3Shape E4) | CAD (Exocad Partial CAD) | - | AM (SLM: Nd) | Ti (Ti-6Al-4V) | 6 |
| Rockshad et al., 2022 [85] | In vitro study | 9 | - | ExtraS (3Shape E4) | CAD (3Shape DS) | AM (DLP) | Casting | Co-Cr (Nd) | 1, 4 |
| Cameron, Evans & Robb, 2022 [86] | Case report | 1 | 4 | IntraS (3Shape Trios 4) | CAD (Nd) | - | AM (SLS: Renishaw AM 400) | Co-Cr (Nd) | 11 |
| Pelletier, Pelletier & Dika, 2022 [87] | Clinical Study (R) | 24 | 2 | CImp+eOS (Nd) | CAD (Nd) | - | AM (SLS: 3DRPD Co Lab) | Nd | 1, 6 |
| Oh, Jeon & Kim, 2021 [88] | Case report | 1 | 4 | CImp+eOS (Nd) | CAD (3Shape DS) | - | AM (Nd: ChamplionM2150X) | Nd | 6 |
| Hamed, Hebeshi & Husseiny 2022 [89] | In vitro study | 10 | - | CImp+eOS (CAD Star CS.NEO) | CAD (Exocad Partial CAD) | AM (DLP) | Casting; AM (SLS: Vulcan Tech VM120) | Co-Cr (Sheftner Starbondeasy Pulver 30) | 4, 6 |
| Study | Fit Assessment Method (Technique) | Fit Qualitative Constructed Outcome (Outcome Used) | Fit Assessment Location | Fit Quantitative Outcome (Thickness µm) | Protocols Studied and Fit Results |
|---|---|---|---|---|---|
| Williams, Bibb & Rafik, 2004 [36] | Ql (Visual inspection) | Nd | - | - | PT4 |
| Eggbeer, Bibb & Williams, 2005 [37] | Ql (Visual inspection) | Good (Satisfactory) | - | - | PT4 |
| Bibb et al., 2006 [19] | Ql (Visual inspection) | Good (Good) | - | - | PT4 |
| Bibb & Eggbeer, 2006 [38] | Ql (Visual inspection) | Excellent (Excellent) | - | - | PT6 |
| Williams et al., 2006 [39] | Ql (Nd) | Good (Good) | - | - | PT6 |
| Yan et al., 2009 [40] | Ql (Visual inspection) | Good (Good) | - | - | PT4 |
| Han, Wang & Lü, 2010 [41] | Nd | - | - | - | - |
| Chen et al., 2011 [42] | Ql+QT (Superimposition of entire framework to STL, analysis by CAE) | Good (Well) | EF | PT6 (+/− 172 µm) | PT6 |
| Kreyer, 2012 [1] | Nd | - | - | - | - |
| Wu et al., 2012 [43] | Ql (Visual inspection) | Good (Satisfactory) | - | - | PT4 |
| Kattadiyil et al., 2014 [44] | Ql (Visual inspection) | Excellent (Excellent) | - | - | PT9 |
| Kim, Lee & Shin 2014 [45] | Ql (Visual inspection) | Good (Good) | - | - | PT4 |
| Lee & Lee, 2015 [46] | Nd | - | - | - | - |
| Ahmed, Abbas & Omar, 2016 [47] | Ql (Citology, Tissue inflamation) | Good (Accurate) | - | - | PT6 |
| Arnold et al., 2018 [48] | Ql+QT (Visual inspection, Pressing test, Silicone specimen: Light microscope) | PT4 and PT6: Bad (imperfections and reduced stability) | OcR | PT3 (117 ± 34 µm) PT4 (323 ± 188 µm) PT6 (365 ± 205 µm) PT1 (133 ± 59 µm) | PT3 ≈ PT1 ≈ PT4 > PT6 |
| Mansour, Sanchez & Machado, 2016 [49] | Ql (Visual inspection; Pressing test) | Good (Properly) | - | - | PT7 |
| Batisse et al., 2017 [6] | Ql (Patient satisfaction) | Good (Good) | - | - | PT11 |
| Hu, Pei& Wen, 2019 [50] | Ql (Visual inspection; Patient satisfaction) | Good (Properly) | - | - | PT11 |
| Lee et al., 2017 [51] | QT (Silicone specimens: Stereo microscope) | - | EF, OcR, MC, OtC | EF (228 ± 173 µm) OcR (249 ± 135 µm) | PT4 |
| Wu, Li& Zhan, 2017 [52] | Nd | - | - | - | - |
| Ye et al., 2017 [29] | Ql+QT (Visual inspection; Pressing test; Stereo microscope) | PT6: Good (Well) | OcR | PT6 (174 ± 117 µm) PT1 (108 ± 84 µm) | PT1 > PT6 |
| Almufleh et al., 2018 [4] | Ql (Patient satisfaction) | - | - | . | PT6 > PT1 |
| Soltanzadeh et al., 2019 [53] | QT (Superimposition to STL design and to master cast; analysis by CAE) | - | EF | PT2 (5 ± 30 µm), PT6 (160 ± 20 µm) PT1 (27 ± 40 µm) | PT1 ≈ PT2 > PT6 |
| Husain et al., 2020 [8] | Ql (Visual inspection) | Good (Similar to PT1) | - | - | PT11 |
| Bajunaid et al., 2019 [54] | QT (Silicone specimens: Digital microscope) | - | OcR | PT6 (272.16 ± 173.55) PT1 (279.61 ± 175.21) | PT1 ≈ PT6 |
| Chen et al., 2019 [55] | QT (Silicone specimens: CAE Superimposition) | - | EF | PT6 (150–330 µm) PT1 (140–280 µm) | PT1 ≈ PT6 |
| Mendes et al., 2019 [56] | Ql (Superimposition to the STL design: Color difference map by CAE) | Good (Good) | - | - | PT11 |
| Tasaka et al., 2020 [57] | QT (Superimposition to STL design and to master cast: Color difference map by CAE) | - | EF, OcR, MC, OtC | PT6 (various individual results) | PT6 > PT4 |
| Tregerman et al., 2019 [30] | Ql (Visual Inspection) | - | - | - | PT11 > PT1 > PT6 |
| Pereira et al., 2019 [58] | Ql (Visual inspection, fit checker paste) | Good (Adequate) | - | - | PT9 |
| Peng et al., 2020 [59] | Ql+QT (Superimposition to STL design: Color difference map by CAE) | PT6: Good (Good); PT4: Nd | EF | PT4 (513 µm) PT6.CoCr (350 µm) PT6.Ti (344 µm) | PT6 > PT4 |
| Wu et al., 2020 [60] | Ql (Visual inspection, fit checker paste) | Good (Good) | - | PT6 | |
| Tasaka et al., 2021 [61] | QT (Superimposition to STL design: Color difference map by CAE) | - | EF, OcR, MC | PT6 (various individual results) | PT6 > PT4 |
| Rist & Cimic, 2016 [62] | Ql (Visual inspection; Patient satisfaction) | Good (Satisfactory) | - | - | PT6 |
| Lee et al., 2020 [63] | Nd | - | - | - | - |
| El-Khamisy et al., 2017 [64] | QT (Silicone specimens: Digital gauge, Contact, Visual score by CAE) | - | MC, OtC | PT5 (Guidding plates: 30 µm, MC:50 µm, Lingual bar: 70 µm); PT1 (Guidding plates: 140 µm, MC: 290 µm, Lingual bar: 530 µm | PT5 > PT1 |
| Malara et al., 2015 [65] | Nd | - | - | - | - |
| Saad et al., 2019 [66] | QT (Silicone and acrylic specimens: Caliper) | - | OcR, MC | PT4 (300 ± 40 µm) PT1 (390 ± 60 µm) | PT4 > PT1 |
| Carreiro et al., 2020 [67] | Ql (Visual inspection, fit checker paste) | Good (Good) | - | - | PT9 |
| Hwang et al., 2023 [68] | QT (Superimposition to the STL design; analysis by CAE softwares | - | EF | PT6 (124 ± 110 µm) | PT6 |
| Cabrita et al., 2021 [69] | Ql: Visual inspection | Good (Good) | - | - | PT6 |
| Maryod & Taha, 2019 [70] | Nd | - | - | - | ------ |
| Eldien, 2020 [71] | Ql: Visual inspection | Good (Improved) | - | - | PT4 |
| Kobayashi et al., 2021 [72] | QT (Superimposition to STL design) | - | EF, OcR, MC, OtC | PT6 (140 µm) | PT6 |
| Muheleman&Ozcan, 2022 [73] | QT (Silicone specimens: Digital microscope) | - | EF, OcR, MC, OtC | PT3 (206 µm), PT4 (211 µm), PT6 (249 µm), PT1 (286 µm) | PT3 ≈ PT4 ≈ PT6 > PT1 |
| Pugliese, Cataneo &Fortunato,2021 [74] | Ql (Visual inspection; Pressing test; Patient satisfaction) | Excellent (Extremely accuracy and satisfaction) | - | - | PT6 ≈ PT1 |
| Snosi et al., 2021 [75] | QT (Superimposition to STL desig,; analysis by CAE softwares) | - | EF, OcR | PT3 (EF: 150 ± 20 µm; OcR: 142 ± 22 µm), PT4 (EF: 179 ± 14 µm; OcR: 235 ± 22 µm) | PT3 > PT4 |
| Suzuki et al., 2022 [76] | QT (Silicone specimens: Profile projector) | - | MC | 200–500 µm | PT11 |
| Ali et al., 2022 [77] | Nd | - | - | - | - |
| Oh, Jeon & Kim 2022 [78] | QT (Silicone specimens: CAE by superimposition) | - | EF, OcR, MC | PT1 (EF: 280 ± 95 µm OcR: 240 ± 65 µm; MC 292 ± 110 µm), PT4 (EF: 332 ± 34 µm; OcR 260 ± 45 µm; MC 356 ± 34 µm), PT6 (EF: 241 ± 14 µm; OcR: 212 ± 17 µm; MC: 251 ± 16 µm) | PT1 ≈ PT4 ≈ PT6 |
| Zhang et al., 2021 [79] | Ql (Visual inspection; Patient satisfaction) | Good (Good) | - | - | PT6 |
| Conceição et al., 2021 [80] | QT (Silicone specimens: Micro-CT + DataViewer + CTAn) | - | OcR | PT1 (310 ± 113 µm), PT6 (333 ± 115 µm) | PT6 ≈ PT1 |
| Maraka et al., 2021 [81] | QT (Silicone specimens: Weight) | - | MC | PT1 (0.154 g), PT6 (0.215 g) | PT1 > PT6 |
| Piao et al., 2022 [82] | Nd | - | - | - | - |
| Alabdullah et al., 2022 [83] | QT (Silicone specimens: Digital Gauge, Superimposition) | - | OcR, MC, OtC | Silicone specimens OtC: 14 µm) (Superimposition OtC: 65 ± 24 µm; OcR: 82 ± 22 µm) | PT6 |
| Chia et al., 2022 [84] | Ql+QT (Visual inspection; Silicone specimens: Digital icroscope) | Good (Good) | OcR | PT1 (242 ± 45 µm) PT6 (274 ± 45 µm) | PT6 ≈ PT1 |
| Lee & Chen, 2022 [82] | Ql (Patient satisfaction) | Good (Satisfied) | - | - | - |
| Rockshad et al., 2022 [85] | QT (Superimposition) | - | OcR, MC, OtC | PT1 (103 ± 18 µm) PT4 (109 ± 21 µm) | PT4 ≈ PT1 |
| Cameron, Evans & Robb, 2022 [86] | Nd | - | - | - | - |
| Pelletier, Pelletier & Dika, 2022 [87] | QT (Silicone specimens: Scanning electron microscope) | - | OcR | PT1 (170 ± 92 µm) PT6 (390 ± 227 µm) | PT1 > PT6 |
| Oh, Jeon & Kim, 2021 [88] | Nd | - | - | - | - |
| Hamed, Hebeshi & Husseiny 2022 [89] | QT (Superimposition to STL: CAD analysis) | - | OcR, MC, OtC | PT4 (319 ± 8 µm) PT6 (160 ± 11 µm) | PT6 > PT4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Conceição, P.; Portugal, J.; Neves, C.B. Evaluation of Removable Partial Denture Metal Frameworks Produced by Digital Methods—A Systematic Review. Appl. Sci. 2023, 13, 10824. https://doi.org/10.3390/app131910824
Conceição P, Portugal J, Neves CB. Evaluation of Removable Partial Denture Metal Frameworks Produced by Digital Methods—A Systematic Review. Applied Sciences. 2023; 13(19):10824. https://doi.org/10.3390/app131910824
Chicago/Turabian StyleConceição, Pedro, Jaime Portugal, and Cristina Bettencourt Neves. 2023. "Evaluation of Removable Partial Denture Metal Frameworks Produced by Digital Methods—A Systematic Review" Applied Sciences 13, no. 19: 10824. https://doi.org/10.3390/app131910824
APA StyleConceição, P., Portugal, J., & Neves, C. B. (2023). Evaluation of Removable Partial Denture Metal Frameworks Produced by Digital Methods—A Systematic Review. Applied Sciences, 13(19), 10824. https://doi.org/10.3390/app131910824