1. Introduction
Bacterial plaque begins to form immediately after food intake and, if not removed, it can cause phenomena that lead to the development of oral and dental disorders. Thus, good oral hygiene, using appropriate products, is essential for the health of the entire body [
1]. Bacterial plaque can be removed by mechanical and chemical means. The most important way of removing plaque is brushing the teeth, but it can be optimized by adding chemicals that prevent, relieve, or treat an existing condition while also inhibiting the formation of bacterial plaque or not allowing its adhesion to dental structures [
1,
2].
Currently, fluoride-based chemical compounds, such as sodium fluoride (NaF), are the main elements used as chemical adjuvants in the removal of plaque, included in toothpaste, mouthwash, dental floss, etc. [
2]. However, many manufacturers also add to their product other natural ingredients, such as sodium bicarbonate, peppermint, eucalyptus, etc. The existence of fluoride ions in dental hygiene products causes the degradation of carbohydrates followed by a decrease in acid production, a decrease in surface tension, and the prevention of microbial adhesion to tooth enamel. It also diminishes the formation of polysaccharides on a cellular level, having an antibacterial effect; also, the ions can lead to the remineralization of tooth enamel by increasing the precipitation tendency of inorganic components [
2,
3,
4,
5].
There are many chemicals in the diet that help to maintain good oral health, and there are many studies that show that the diets of our ancestors, rich in fats and proteins, favored good oral health, while the consumption of semi-prepared foods, canned food, and sweets has caused an increase in the index of caries in today’s population [
3,
5,
6,
7,
8,
9]. Dietary food compounds can promote good oral health; for instance, sodium bicarbonate creates an alkaline oral environment. It is known that an acidic environment, which actually produces demineralization of tooth enamel, favors the occurrence of tooth decay. Since tooth decay does not progress without the bacteria present in dental plaques, daily removal of plaque by brushing, flossing, and rinsing is one of the best ways to prevent tooth decay and periodontal disease. Proper methods of brushing and flossing can be taught in the dental office during routine check-ups [
5,
6].
Fluoride prevents tooth decay by inhibiting the demineralization of crystalline structures inside the tooth and improving remineralization. The remineralized surface is resistant to acid attack. In addition, fluoride inhibits bacterial enzymes. Methods of fluoride application include the fluoridation of water, fluoride toothpaste, mouth rinse with fluoride, dietary fluoride supplements, and professionally applied fluorinated compounds such as gels and varnishes. The use of antiplatelet agents such as chlorhexidine, delmopinol chloride, hexetidine, extracts of
Sanguinaria, triclosan, and phosphopeptide calcium phosphate (CCP-ACP) has been proven to be effective in reversing incipient caries [
4].
An overall improvement in oral health has been observed in our societies over the past thirty years. Improved hygiene (brushing quality and regular use of fluorides) and the ease of access to dental care, as well as the establishment of systems to promote oral health [
7], could explain this.
The eating habits of different populations have evolved. We have moved from eating fresh produce grown in gardens to processed products that generally affect the state of health. Presently, there is a tendency to adopt a diet rich in sugars and fats, with a decline in physical activity [
5]. The evolution of lifestyle, the lack of time, and a disorganized meal program lead to the consumption of snacks and sugar-rich drinks. However, the frequency of consumption remains the most important factor for the onset of degradation. The carious process can be stopped or reversed in the early stages of development, but most of the time it gradually expands, and, without proper hygiene, it progresses to the destruction of the dental organ [
5,
6].
Although all age groups are affected in different clinical forms, students tend to be in the category most at risk due to a more imbalanced lifestyle. The risk of caries is increased by sweet snacks consumed throughout the day, especially those consumed between meals. However, there are very few studies on the prevalence of tooth decay among students concerned about the impact of eating habits on oral health. In this context, a study was conducted with the specific objectives of studying the influence of students’ eating habits, hygiene, and dental care practices on the prevalence of caries [
5,
6,
7,
8,
9].
The literature shows that certain foods decrease the rate of caries; thus, fats in the diet create a film on the surface of the tooth enamel. This forms a protective barrier on the tooth and also includes products from hydrocarbons, reducing the release time and enzymatic degradation, and acts on the membrane of microorganisms in the bacterial plaque [
8].
2. Materials and Methods
For good oral health, in addition to eating habits, we can talk about the mechanical and chemical means of removing plaque. Mechanical means are most effective and, if supplemented by chemical ones, they have an optimal effect on oral health. It is well known that brushing the teeth is the most effective technique for plaque removal, and toothpaste complements it by acting as a detergent and amplifying the effect on the plaque. Currently, on the market there is a wide variety of toothpastes, which have in their composition basic ingredients, which are found in all toothpastes, but also ingredients that give them special properties. Certain toothpastes contain baking soda, peppermint, cinnamon, etc. Certain ingredients in toothpastes are not to be swallowed, as they can negatively affect general health [
10,
11,
12,
13,
14,
15,
16,
17,
18,
19,
20,
21,
22,
23].
The present study focuses on a comparison between toothpastes containing natural ingredients, in terms of their effectiveness in removing plaque. Thus, several ingredients were selected to be included in the composition of these toothpastes. The ingredients are: baking soda, coconut oil, flavor (such as mint, eucalyptus, lavender, turmeric), and charcoal (medicinal). Sodium bicarbonate is a white solid compound, often available as a fine powder. It has a slightly salty, alkaline taste. It helps to remove stains from the teeth, especially due to its abrasive properties, and it is also very good for maintenance of dentures and other dental appliances, as the odors are neutralized [
24,
25,
26].
Coconut oil was chosen as a vehicle for toothpaste, but also due to its antibacterial properties, as shown by a study conducted at the Athlone Institute of Technology, in which Dr. Damien Brady stated: “Adding enzymatically modified coconut oil to dental hygiene products can be a much more attractive alternative to chemical additives, especially when using very low concentrations” [
27].
When selecting flavors that were added to the toothpaste, their curative properties were taken into account. Thus, turmeric and lavender were selected. Turmeric has an antiseptic, antibacterial, and anti-inflammatory role. Turmeric root contains volatile oils, sesquiterpenes, monoterpenes, curcumin (yellow dye), mineral salts, water-soluble peptides, and polysaccharides [
28]. The active substances in lavender provide antiseptic, antidepressant, antispasmodic, and carminative properties. Lavender flowers contain volatile oils (linalool), geraniol, nerol, lavandulol, borneol, tannin, coumarins, bitter principles, resins, and pectins [
29].
Last but not least, activated charcoal (medicinal) was selected, which is a material with a porous structure, in the form of a black powder. This was chosen because it also has an abrasive effect, being able to remove stains from the teeth, but also because of its property to absorb the tannins present in the composition of certain fruits, tea, coffee, or wine [
30].
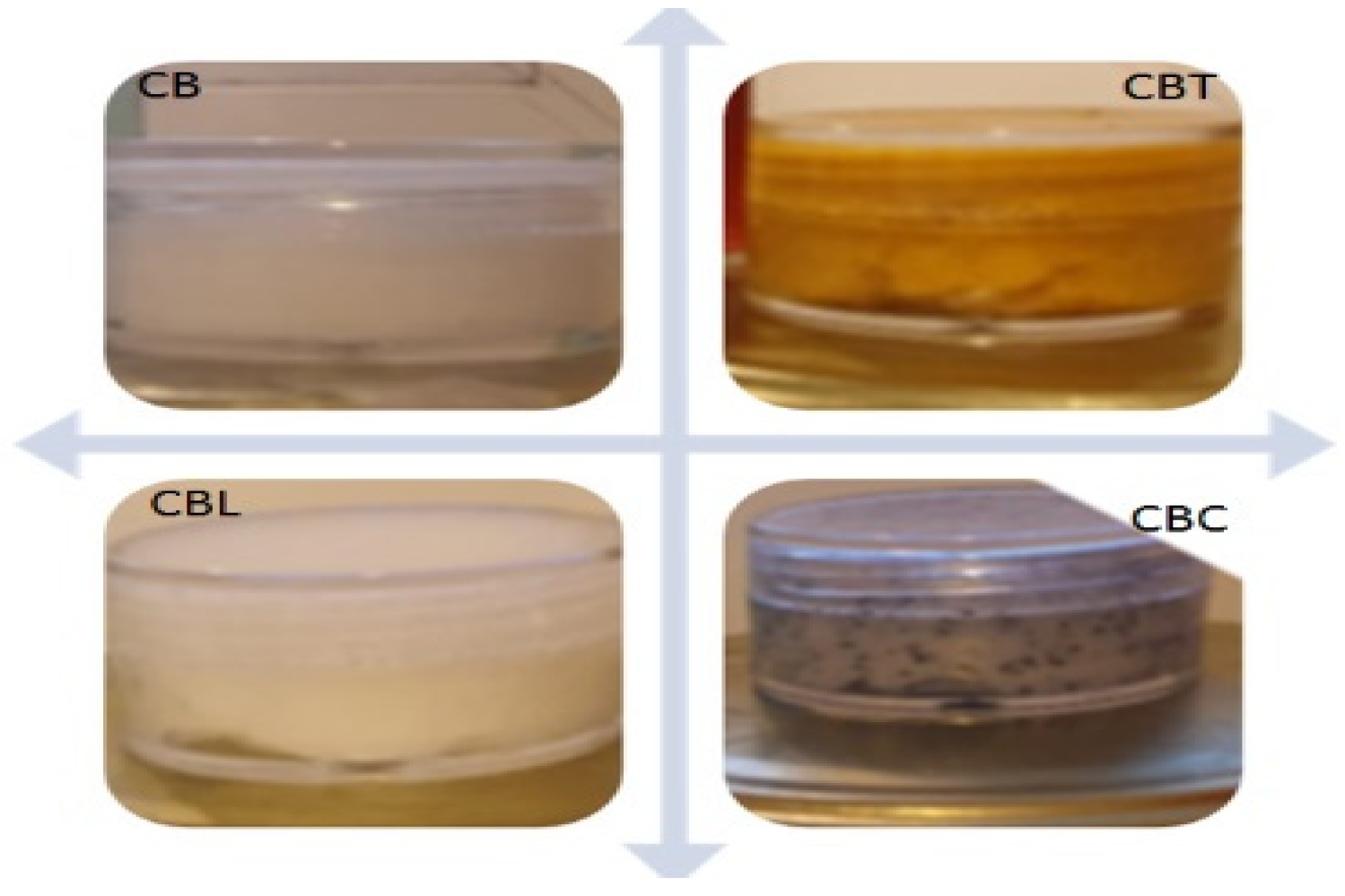
After selecting the components, the toothpaste was made in four versions (
Figure 1). The first version of the toothpaste was made by mixing 25 g of coconut butter with 10 g of baking soda, obtaining a homogeneous oily paste, and it was called CB. The first version was a basic version and included the selected flavors to obtain other forms of toothpaste. The second version was obtained by adding 5 g of turmeric to the basic version and was called CBT. For the third version, we added lavender essential oil to the base, denoted as CBL. For the last version, natural charcoal was used due to its abrasive effect, denoted as CBC.
In our study, all participants, without exception, were provided with toothpaste that was meticulously mixed. This was done to ensure that the best and most visible results could be obtained for the benefit of our participants.
The cohort of individuals considered in this study comprised individuals with an age range spanning from 14 to 49 years. The participants included in this study met the criteria of having no preexisting medical conditions and no allergies, and a total of 80 participants were included. Each participant was examined individually. Thus, the study included a cohort of 42 female participants, accounting for 52.5% of the total sample, complemented by 16 male participants, representing 20% of the total sample, and 22 individuals with an age range between 14 and 18 years, comprising both genders, were included in the study, constituting 27.5% of the total sample (
Figure 2).
The study was conducted over a period of eighteen months. The participants underwent an initial session of expert oral cleansing. They were informed about the content of the study, including the possible adverse effects, and signed an informed consent. All participants were informed regarding the requirements for good oral health and were taught the Bass brushing technique, knowing that this is one of the most effective techniques for removing dental plaque.
This study involved the categorization of participants into four distinct groups, namely G1, G2, G3, and G4, and the groups were differentiated based on the age of the participants. The groups G1, G2, and G3 comprised 58 adult participants each, while G4 contained 22 child participants. The age groups under consideration in this study are those between the ages of 18 and 29, 30 and 39, 40 and 49, and 14 and 18. The male population within the sample size for this study is represented by 11 participants in the age range of 18–29, 4 participants in the age range of 30–39, 1 participant in the age range of 40–49, and 10 participants in the age range of 14–18. The female population within the sample size for the study is represented by 18 participants in the age range of 18–29, 14 participants in the age range of 30–39, 10 participants in the age range of 40–49, and 12 participants in the age range of 14–18 (
Figure 3).
All participants were informed on the requirements for good oral health and were taught the Bass brushing technique, knowing that this is one of the most effective techniques for removing dental plaque.
Prior to performing tooth brushing using the acquired methodology, every participant underwent a consultation session, during which the Silness–Löe plaque index was used to assess the bacterial plaque.
Following the examination, we noted that 4 participants exhibited an index score of ISL 0 (representing a percentage of 13%), 18 participants exhibited ISL 1 (22.25%), 57 participants exhibited ISL 2 (71.25%) and 1 participant exhibited ISL 3. Most of the participants who were included in this study had an ISL index of 2 (
Figure 4).
From the graphic above, it can be observed that in each group there were participants who had ISL 0, ISL 1, and ISL 2. ISL 3 was found in a single participant, belonging to Group 4 (G4) (
Figure 5).
After the consultation, each participant was asked to brush their teeth according to the previously learned Bass brushing technique. Participants included in the G1 were directed to brush their teeth with CB, the basic toothpaste, containing only coconut oil and baking soda.
The G2 participants brushed their teeth with CBT, the paste containing coconut oil, baking soda, and turmeric.
The G3 group brush their teeth with the paste containing the essential oil of lavender in addition to coconut oil and baking soda.
The last group, G4, used as an auxiliary means for brushing teeth with toothpaste that contains medicinal charcoal (active) included in the base paste.
3. Results and Discussion
The participants who entered the study had a caries prevalence of 66%. Each of the respondents had at least one case of tooth decay. This prevalence varied depending on gender and was higher for women and girls (37%) than for men or boys (29%). In total, 18% of the participants who entered the study had a missing tooth, 8% two missing teeth, 3% three missing teeth, and 1% four missing teeth (
Figure 6).
Only 6% of the participants wore braces, with 81.7% of them being consistent in their daily cleaning routines, while the remaining 18.3% were occasionally negligent in their oral hygiene practices.
A distinction was drawn between individuals who exhibited regularity in utilizing toothpaste and a toothbrush as compared to those who substitute dental brushing with alternate methods such as rinsing, flossing, and chewing gum. As per the report, 92% of the participants confirmed their usage of toothpaste and toothbrush for teeth cleaning purposes. Furthermore, 78% of the individuals employed a paste containing fluoride, while 10% opted for a different variant of toothpaste.
During this study, we observed that 41% of the participants who used a toothbrush were brushing twice a day. Conversely, a smaller proportion of 35% of the participants engaged in brushing only once, while 11.2% brushed their teeth three times daily. Moreover, an additional 4.8% of the participants brushed more than three times daily. Further scrutiny revealed that 21% of the participants brushed their teeth for a duration of 3 min, while 34% brushed for 2 min, and 45% brushed for 1 min. Additionally, 53% of the participants brushed their teeth less than half an hour after eating, while 17% brushed more than half an hour later. Finally, it was discovered that the remaining 22% of the participants did not give any importance to the time interval between the end of the meal and brushing (
Figure 7).
When the respondents are unable to perform dental hygiene, 36% of them choose to rinse their mouth with water, while 29% prefer to utilize sugar-free chewing gum. An additional 16% of respondents opt for chewing gum containing sugar, while 12% choose to take no action to replace brushing.
After brushing with the toothpaste selected for each group, the plaque index value was reassessed for each group.
In G1, the group who brushed their teeth with coconut oil base paste and baking soda, it was found that the dental plaque was removed by observing an improvement in the ISL values. Initially, only one participant had the value of zero; after brushing, five participants had a score of ISL 0, which represents the lack of plaque on the dental surfaces (
Figure 8 and
Figure 9).
In the G2 group that used toothpaste consisting of coconut oil, baking soda, and turmeric, an improvement was also observed in the state of oral hygiene—the number of participants with ISL 0 being much higher at the end of the brushing than at the beginning. However, two participants presented as ISL 1 and one participant presented as ISL 2 (
Figure 10).
The toothpaste composed of coconut oil, baking soda, and lavender oil also had beneficial effects on oral hygiene, finding that three participants, in addition to the initial one, reached a score of ISL 0, which means that there were no bacterial plaques. Only two of the other participants who had a score of ISL 2 managed to reach ISL 0. Overall, for each participant in this group, the ISL score was reduced meaning that they improved their oral health, managing to reduce the amount of dental plaque found in dental–periodontal structures (
Figure 11).
The participants who belonged to the G4 group and who used toothpaste containing medicinal charcoal in addition to coconut oil and baking soda, obtained the complete removal of the bacterial plaque, i.e., ISL 0, in 75% of the participants; this meant that 15 participants had a score of ISL 0. ISL 1 (film adhering to the gingival edge) was exhibited by the remaining participants. No participant in this group, after brushing, presented scores of ISL 2 or ISL 3 (
Figure 12).
When evaluating the Silness and Löe plaque index in the entire group of participants, analyzing the effectiveness of all toothpastes used in this study, we found that 63% of the participants obtained a score of ISL 0, managing to completely remove the bacterial plaque (
Figure 13). In total, 24% of the participants exhibited ISL 1; they managed to remove most of the bacterial plaque, but a film remained adhering to the free gingival margin. In a small number of participants (13%), we still observed the presence of plaque on the teeth and periodontal structures, including in one participant who initially exhibited ISL 3 and therefore showed an improvement in the removal of bacterial plaque. The other participants did not obtain any improvements in the removal of the dental plaque for several reasons: either the dental plaque was old and transformed into tartar, or they did not manage to learn the brushing technique sufficiently, or did not have good brushing skills, etc. (
Figure 14).
4. Discussion
Recently, there has been a growing trend in dental research to explore innovative approaches for eliminating dental biofilms. Similar studies have shown that using organic products can eliminate bacterial biofilms in the oral cavity, that various forms of chlorhexidine in mouthwashes are effective, that fluoride-free toothpaste has benefits, as does toothpaste containing fluoride and fluoride varnish, and that the incorporation of sodium bicarbonate into oral hygiene products and its application is significant [
27,
28,
29]. The benefits of sodium bicarbonate are described in many dental studies. Although not a universal remedy for dental ailments, the properties of sodium bicarbonate, including its ingestion safety, low abrasiveness, cost-effectiveness, and synergy with fluoride, make it an excellent ingredient in dental hygiene products [
30,
31,
32,
33,
34,
35,
36]. Moreover, recently introduced compounds have been shown to have a significant impact on the oral environment [
37]. A turmeric toothpaste capable of keeping oral cavity warm and improving tooth cold, dental ulcers, and stomach stench is a patented invention that comprises sorbitol, water, silicon dioxide hydrate, polyethylene glycol-8, sodium lauryl sulfate, essence, cellulose gum, xanthan gum, sodium saccharin, sodium benzoate, tetrasodium pyrophosphate, and turmeric extract [
38]. A Chinese herbal medicine toothpaste offers the same tooth cleaning and oral health protective functions as common toothpaste and it is fortified with lavender herbal extract to provide fragrance and antibacterial effects [
39]. Another study aimed to assess the impact of activated charcoal toothpastes on enamel and dentin erosive wear, utilizing an optical profilometer. The results indicate that there is no increase in erosive tooth wear when using activated charcoal toothpastes. Furthermore, it was observed that certain charcoal toothpastes, as well as a reference toothpaste, offer protection against surface loss, and the results also suggested that the concentration of fluoride in the slurries for enamel has a strong negative correlation with surface loss, concluding that the use of activated charcoal toothpastes does not lead to an increase in tooth wear, and certain products may even provide additional protection against surface loss [
40].
In the present study, a comparative analysis was conducted on toothpastes formulated with organic components including sodium bicarbonate compounds, coconut oil, turmeric, lavender, and medicinal charcoal that do not cause insults to the body. The findings indicated that all four toothpastes, namely CB, CBT, CBL, and CBC, led to a reduction in the ISL score. Notably, the toothpaste containing medicinal charcoal was the most efficacious in this respect.
The utilization of sodium bicarbonate [
30,
31,
32,
33,
34,
35,
36], turmeric [
38], lavender [
39], and charcoal [
40,
41] has a notable impact on reducing the ISL value, and subsequently, has the potential to positively impact oral health by effectively decreasing the bacterial plaque film on teeth, thereby promoting optimal oral hygiene. Therefore, these products should be regarded as toothbrushing adjuvants in future studies.
This study details certain constraints, such as a narrow selection of naturally occurring constituents used in the toothpaste formulation, and the exclusion of fluoride, which decreases the caries index but may cause detrimental effects on human physiology. Nevertheless, this study is the first to compare four types of toothpaste with natural ingredients: CB, CBT, CBL, and CBC.


 ,
, 



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}













