

Assessment of Individualized and Group Physical Exercise Programs in Patients with Parkinson’s Disease: A Pilot Study



Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
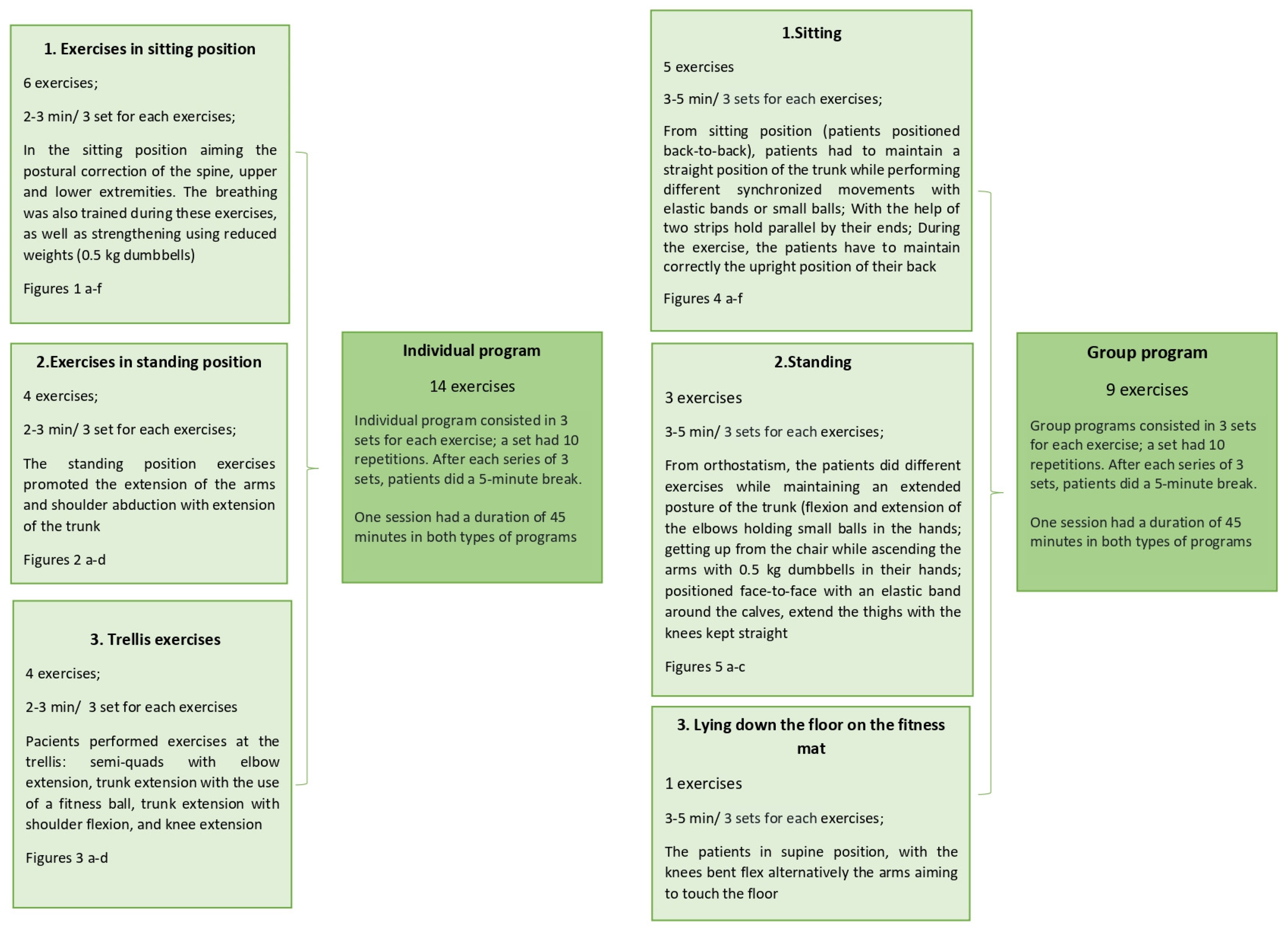
2.2. Physical Exercise Programs
2.3. Assessment
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jagadeesan, A.J.; Murugesan, R. Currents trends in etiology, prognosis and therapeutic aspects of Parkinson’s disease: A review. Acta Bio Medica Atenei Parm. 2017, 88, 249–262. [Google Scholar]
- Zippenfening, H.A.; Alexoi, I. Kinetoterapie și Nutriție Destinată Bolii Parkinson GHID; Mirton: Timișoara, Romania, 2021; pp. 13–15. [Google Scholar]
- The Michael, J. Fox Foundation for Parkinson’s Research. Available online: https://www.michaeljfox.org/parkinsons-101 (accessed on 15 March 2023).
- Foster, E.R.; Carson, L.G.; Archer, J.; Hunter, E.G. Occupational Therapy Interventions for Instrumental Activities of Daily Living for Adults with Parkinson’s Disease: A Systematic Review. Am. J. Occup. Ther. 2021, 75, 7503190030. [Google Scholar] [CrossRef] [PubMed]
- Zippenfening, H.A.; Răican, D. Broșură—Recomandări Pentru cei Apropiați Persoanelor cu Boala Parkinson; Asociația de Parkinson: București, Romania, 2015; pp. 15–20. [Google Scholar]
- Durner, J.; Fickert, G.; Kröner, W.; Stadler, B. Training fȕr das Leben im Alltag—Physio-und ergotherapeutische Anleitng zum Eigentraining fȕr Parkinson-Patienten; Fachklinik: Ichenhausen, Germany, 1998; pp. 40–61. [Google Scholar]
- Varadi, C. Clinical Features of Parkinson’s Disease: The Evolution of Critical Symptoms. Biology 2020, 9, 103. [Google Scholar] [CrossRef] [PubMed]
- Iordan, D.A.; Munteanu, C.; Constantin, G.B.; Onu, I.; Nechifor, A. Age-Related Sport-Specific Dysfunctions of the Shoulder and Pelvic Girdle in Athletes Table Tennis Players. Observational Study. Balneo PRM Res. J. 2021, 12, 337–344. [Google Scholar] [CrossRef]
- Etoom, M.; Alwardat, M.; Aburub, A.S.; Lena, F.; Fabbrizo, R.; Modugno, N.; Centonze, D. Therapeutic interventions for Pisa syndrome in idiopathic Parkinson’s disease. A Scoping Systematic Review. Clin. Neurol. Neurosurg. 2020, 198, 106242. [Google Scholar] [CrossRef] [PubMed]
- Ninomiya, S.; Morita, A.; Teramoto, H.; Akimoto, T.; Shiota, H.; Kamei, S. Relationship between Postural Deformities and Frontal Function in Parkinson’s Disease. Park. Dis. 2015, 2015, 462143. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Warburton, D.E.; Nicol, C.W.; Bredin, S.S. Health benefits of physical activity: The evidence. CMAJ 2006, 174, 801–809. [Google Scholar] [CrossRef] [PubMed]
- López-Liria, R.; Vega-Tirado, S.; Valverde-Martínez, M.Á.; Calvache-Mateo, A.; Martínez-Martínez, A.M.; Rocamora-Pérez, P. Efficacy of Specific Trunk Exercises in the Balance Dysfunction of Patients with Parkinson’s Disease: A Systematic Review and Meta-Analysis. Sensors 2023, 23, 1817. [Google Scholar] [CrossRef] [PubMed]
- Gandolfi, M.; Tinazzi, M.; Magrinelli, F.; Busselli, G.; Dimitrova, E.; Polo, N.; Manganotti, P.; Fasano, A.; Smania, N.; Geroin, C. Four-week trunk-specific exercise program decreases forward trunk flexion in Parkinson’s disease: A single-blinded, randomized controlled trial. Park. Relat. Disord. 2019, 64, 268–274. [Google Scholar] [CrossRef]
- Yitayeh, A.; Teshome, A. The effectiveness of physiotherapy treatment on balance dysfunction and postural instability in persons with Parkinson’s disease: A systematic review and meta-analysis. BMC Sports Sci. Med. Rehabil. 2016, 8, 17. [Google Scholar] [CrossRef] [PubMed]
- Opara, J.; Małecki, A.; Małecka, E.; Socha, T. Motor assessment in Parkinson’ s disease. Ann. Agric. Environ. Med. 2017, 24, 411–415. [Google Scholar] [CrossRef] [PubMed]
- MDS-UPDRS. The MDS-Sponsored Revision of the Unified Parkinson’s Disease Rating Scale. Official MDS Romanian Translation. 2018 International Parkinson and Movement Disorder Society. Available online: https://www.movementdisorders.org/MDS-Files1/PDFs/MDS-UPDRS-Rating-Scales/MDS_UPDRS_Romanian_OfficialTranslation_FINAL.pdf (accessed on 6 June 2022).
- Cocks, K.; Torgerson, D.J. Sample size calculations for pilot randomized trials: A confidence interval approach. J. Clin. Epidemiol. 2013, 66, 197–201. [Google Scholar] [CrossRef] [PubMed]
- Borrero, L.; Miller, S.A.; Hoffman, E. The meaning of regular participation in vigorous-intensity exercise among men with Parkinson’s disease. Disabil. Rehabil. 2022, 44, 2385–2391. [Google Scholar] [CrossRef] [PubMed]
- van der Kolk, N.M.; de Vries, N.M.; Kessels, R.P.C.; Joosten, H.; Zwinderman, A.H.; Post, B.; Bloem, B.R. Effectiveness of home-based and remotely supervised aerobic exercise in Parkinson’s disease: A double-blind, randomised controlled trial. Lancet Neurol. 2019, 18, 998–1008. [Google Scholar] [CrossRef] [PubMed]
- Schenkman, M.; Moore, C.G.; Kohrt, W.M.; Hall, D.A.; Delitto, A.; Comella, C.L.; Josbeno, D.A.; Christiansen, C.L.; Berman, B.D.; Kluger, B.M.; et al. Effect of high-intensity treadmill exercise on motor symptoms in patients with de novo Parkinson disease: A phase 2 randomized clinical trial. JAMA Neurol. 2018, 75, 219–226. [Google Scholar] [CrossRef]
- Schootemeijer, S.; van der Kolk, N.M.; Ellis, T.; Mirelman, A.; Nieuwboer, A.; Nieuwhof, F.; Schwarzschild, M.A.; de Vries, N.M.; Bloem, B.R. Barriers and Motivators to Engage in Exercise for Persons with Parkinson’s Disease. J. Park. Dis. 2020, 10, 1293–1299. [Google Scholar] [CrossRef] [PubMed]
- David, Z.; Russel, J. Delay the Disease—Exercises and Parkinson’s Disease, 2nd ed.; OhioHealth: Columbus, OH, USA, 2017. [Google Scholar]
- Falup-Pecurariu, C. Boala Parkinson și alte Tulburări de Mișcare- de la Diagnostic la Tratament. Habilitation Thesis, Universitatea Transylvania University of Brasov, Brasov, Romania, 2021. [Google Scholar]
- Sangarapillai, K.; Norman, B.M.; Almeida, Q.J. An equation to calculate UPDRS motor severity for online rural assessments of Parkinson’s. Park. Relat. Disord. 2022, 94, 96–98. [Google Scholar] [CrossRef] [PubMed]
- Lo, C.; Arora, S.; Lawton, M.; Barber, T.; Quinnell, T.; Dennis, G.J.; Ben-Shlomo, Y.; Hu, M.T. A composite clinical motor score as a comprehensive and sensitive outcome measure for Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 2022, 93, 617–624. [Google Scholar] [CrossRef] [PubMed]
- Mak, M.K.; Wong-Yu, I.S.; Shen, X.; Chung, C.L. Long-term effects of exercise and physical therapy in people with Parkinson disease. Nat. Rev. Neurol. 2017, 13, 689–703. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Range | |
|---|---|---|
| Age (years) (mean (SD)) | 66.24 (6.53) | 52–76 |
| Height (cm) (mean (SD)) | 170 (10.33) | 156–179 |
| Weight (kg) (mean (SD)) | 77.72 (14.52) | 55–110 |
| BMI (kg/m2) (mean (SD)) | 26.87 (4.48) | 18.10–36.40 |
| Medical treatment | ||
| Dopamine agonist (N%) | 15 (52%) | |
| Monoamine oxidase inhibitors (N%) | 9 (31%) | |
| Levodopa–carbidopa (N%) | 19 (65.5%) | |
| Dopaminergic agents (N%) | 4 (14%) | |
| Decarboxydase inhibitors (N%) | 5 (17%) |
| Question | N (%) |
|---|---|
| Information about the type of exercises | |
| Yes | 24 (83%) |
| No | 5 (17%) |
| Difficulty level of the physical exercise program | |
| No difficulty | 7 (24%) |
| Mild difficulty | 9 (31%) |
| Some exercises were difficult, patient completed the program | 9 (31%) |
| Exercises were difficult, patient did not complete the program | 4 (14%) |
| Mental status during the physical exercise program | |
| Very good | 19 (65%) |
| Good | 10 (35%) |
| No change | 0 |
| Worse | 0 |
| Physical status during the physical exercise program | |
| Very good | 24 (83%) |
| Good | 5 (17%) |
| No change | 0 |
| Worse | 0 |
| If the patient followed the instructions of the physical therapist during the physical exercise program | |
| Always | 25 (86%) |
| Sometimes | 4 (14%) |
| No | 0 |
| If the physical status improvement through physical exercise program helps boosting the self-esteem | |
| Yes | 25 (86%) |
| No | 1 (4%) |
| No connection between physical exercise and self-esteem | 3 (10%) |
| Persistence in performing the exercises at home | |
| Yes | 9 (31%) |
| No | 13 (45%) |
| Occasionally | 7 (24%) |
| Improvement in the quality of life after physical exercise program | |
| Significant improvement | 18 (62%) |
| Insignificant improvement | 10 (34%) |
| No improvement | 1 (4%) |
| Worsening | 0 |
| Satisfaction with the physical exercise program | |
| Very satisfied | 24 (83%) |
| Satisfied | 5 (17%) |
| Unsatisfied | 0 |
| Type of therapy most appropriate for patient | |
| Individual therapy | 12 (41%) |
| Group therapy | 17 (59%) |
| Benefits after the physical exercise program for the health status | |
| Yes | 29 (100%) |
| No | 0 |
| If the patient continued the recommended physical exercise program at home | |
| Yes | 13 (45%) |
| No | 16 (55%) |
| Questionnaire Items | Individual Therapy (N = 12) | Group Therapy (N = 17) | p |
|---|---|---|---|
| Mental status during the physical exercise program a | 2.58 ± 0.51 | 2.71 ± 0.47 | 0.25 |
| Physical status during the physical exercise program a | 2.83 ± 0.39 | 2.82 ± 0.39 | 0.47 |
| Improvement in the quality of life after physical exercise program b | 2.58 ± 0.51 | 2.59 ± 0.62 | 0.49 |
| MDS-UPDRS Items | First Assessment | 6 Month Assessment |
|---|---|---|
| Pain and other sensations | 2.6 ± 0.99 | 2.14 ± 1 |
| Fatigue | 2.85 ± 1.04 | 2.21 ± 0.87 |
| Hygiene | 2.25 ± 1.07 | 2.03 ± 1.1 |
| Performing hobbies and other activities | 2.28 ± 0.76 | 2.17 ± 0.86 |
| Getting out of bed, a car, or a deep chair | 1.64 ± 0.98 | 1.35 ± 0.95 |
| Walking and balance | 1.75 ± 1.32 | 1.67 ± 1.12 |
| Postural stability | 1.82 ± 1.44 | 1.46 ± 1.26 |
| MDS-UPDRS (combined score) | 2.20 ± 1.01 | 1.83 ± 0.92 |
| Individual Therapy (N = 12) | Group Therapy (N = 17) | |||||
|---|---|---|---|---|---|---|
| First Assessment | 6 Month Assessment | p | First Assessment | 6 Month Assessment | p | |
| MDS-UPDRS (combined score) | 2.30 ± 1.04 | 1.90 ± 1.05 | 0.001 | 2.13 ± 1.02 | 1.79 ± 0.85 | 0.005 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zippenfening, H.A.; Amaricai, E.; Raducan, M.R. Assessment of Individualized and Group Physical Exercise Programs in Patients with Parkinson’s Disease: A Pilot Study. Appl. Sci. 2023, 13, 8962. https://doi.org/10.3390/app13158962
Zippenfening HA, Amaricai E, Raducan MR. Assessment of Individualized and Group Physical Exercise Programs in Patients with Parkinson’s Disease: A Pilot Study. Applied Sciences. 2023; 13(15):8962. https://doi.org/10.3390/app13158962
Chicago/Turabian StyleZippenfening, Himena Adela, Elena Amaricai, and Maria Raluca Raducan. 2023. "Assessment of Individualized and Group Physical Exercise Programs in Patients with Parkinson’s Disease: A Pilot Study" Applied Sciences 13, no. 15: 8962. https://doi.org/10.3390/app13158962
APA StyleZippenfening, H. A., Amaricai, E., & Raducan, M. R. (2023). Assessment of Individualized and Group Physical Exercise Programs in Patients with Parkinson’s Disease: A Pilot Study. Applied Sciences, 13(15), 8962. https://doi.org/10.3390/app13158962