Abstract
Modern implant designs should allow for adequate primary stability but limit mechanical stress on buccal bone in order to prevent initial marginal bone loss. A dental implant characterized by a shift in core diameter and thread geometry was evaluated. Polyurethane foam was used as bone surrogate material and implant placement was performed measuring insertion torque and strain development on buccal bone using strain gauges as well as primary stability by using damping capacity assessments. An existing tapered bone-level implant was used as a control while the novel experimental implant described above (n = 10) was used in the test group. Statistical analysis was based on t-tests (α = 0.05). Both the maximum insertion torque (p = 0.0016) and maximum strain development in buccal bone (p = 0.1069) were greater in control implants as compared to the novel implant design. Moreover, in the control group, these were reached at a significantly later timepoint of the insertion process, i.e., when the implant was almost fully seated (maximum insertion torque p = 0.0001, maximum strain development p < 0.00001). The final insertion torque (p < 0.00001) and final strain development (p = 0.0137) were significantly lower in the novel implant design while the primary stability of both implant types did not differ significantly (p = 0.219). The novel implant design allowed for a greater undersizing of osteotomies while not mechanically overstressing buccal bone. Comparable primary stability was obtained from trabecular bone instead of compressing cortical bone as occurs in conventional, existing tapered implant designs.
1. Introduction
Achieving adequate primary stability still is one of the major goals in dental implant surgery and is governed by several parameters including bone quality [1], surgical protocol and implant design [2,3,4]. Host factors such as diabetes and osteoporosis are difficult to control for dentists but have been shown to also affect osseointegration [5,6]. Consequently, implant manufacturers advocate drilling protocols [7] with varying levels of undersizing depending on the bone quality present in a specific implant site [8]. As a general trend, undersizing an osteotomy and the use of tapered implant macrodesigns compressing cortical layers of alveolar bone [9] increases primary stability [3,10,11,12].
Using both clinical and animal research designs, several authors have meanwhile reconsidered the concept of high initial implant stability being a desirable goal [13]. A retrospective clinical study showed that excessive insertion torque in dense bone can cause negative marginal bone responses [7] thereby confirming data from a randomized clinical trial recording more peri-implant bone remodeling and buccal soft tissue recession in implants inserted with high insertion torque [14]. While still concluding that high insertion torque would not have a negative effect, De Santis and coworkers found a three-year survival rate of only 98.6% and a considerable bone loss of up to 2.5 mm for implants placed with high insertion torque [15]. On the other end of the spectrum, a clinical study proved that lower insertion torques may yield favorable implant survival rates with optimal marginal bone levels [16]. In this context, it might be anticipated that less stress is induced in maxillary sites as compared to mandibular sites due to their lower percentage of stiff cortical bone. While this question certainly cannot be addressed in a clinical study, a recent meta-analysis indeed showed greater risk for implant loss in the maxilla [17].
A clear trend depicting the negative effects of high insertion torques on alveolar bone can be derived from animal studies. It was pointed out that underpreparation of the implant socket compromised osseointegration of immediately loaded bone-level tapered implants [18] and reduces crestal bone-to-implant contact at early healing stages [11]. In addition, it has been shown that the speed of new bone formation was relatively slow while the speed of marginal bone loss was relatively fast when the final drill was excessively smaller than the implant to be placed [19]. Two animal studies showed a correlation between microcracks induced during implant placement and bone resorption [20,21]. Knowledge on how immediate vs. conventional implant loading might affect bone in this context is sparse [22]. However, similar amounts of osseointegration have been described irrespective of the implant insertion torque applied [23]. Using various analyzing techniques up to molecular levels, it has recently been proven that placing implants with high insertion torque leads to a zone of dead and dying osteocytes, resulting in microfractures of bone increasing bone resorption but decreasing new bone formation [24,25]. Insertion torque may be seen as a common denominator for assessing implant stability [13,26] and has been correlated with resonance frequency analysis [26] and damping capacity assessments [27].
While a certain level of peri-implant marginal bone loss during healing is widely accepted [28,29], it may be argued that this phenomenon results from overstressing of alveolar bone during implant installation. In response to that and as a potential alternative to common tapered bone-level implants (Figure 1a), a novel implant macrodesign characterized by an increase in the core diameter of the implant in the middle portion was fabricated (Figure 1b). The change in core diameter coincided with a continuous change in thread geometry starting with sharp threads in the apical region, dull, condensing threads in the middle portion and sharp threads in the cervical portion.

Figure 1.
Bone-level implant types used in this study comprising Straumann BLT 4.1 × 10 mm (a) and AlfaGate 4.3 × 10 mm (b).
Using a previously established study design [30,31,32], it was the goal of this in vitro experiment to gain insight into the insertion characteristics of this novel implant design with respect to insertion torque, bone strain and primary stability as compared to a well-documented bone-level implant system.
2. Materials and Methods
Polyurethane foam material [3,4,8,9,33,34,35,36] consisting of a low-density trabecular portion covered by a cortical layer with a thickness of 3 mm (Solid Rigid polyurethane foam 10 pcf/40 pcf, Sawbones Europe AB, Malmö, Sweden) was used as bone surrogate material [8,9]. Strain gauges [10] were positioned on the buccal surface of the cortical layer next to the osteotomy positions with the sensing elements oriented in the horizontal plane (Figure 2). Using a measurement amplifier (Quantum X, Hottinger Baldwin, Darmstadt, Germany) and analyzing software (jBEAM, AMS GmbH, Chemnitz, Germany) allowed for the recording of strain development during implant insertion [30,31,32].
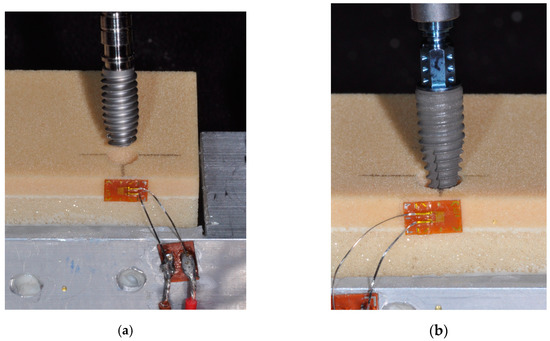
Figure 2.
Insertion of a novel design AlfaGate implant (a) and a Straumann BLT implant (b) into osteotomies created in laminated polyurethane foam simulating alveolar bone. Strain gauges were positioned on the buccal aspect of the bone with the sensing elements oriented in the horizontal direction for recording deformation of the material.
The osteotomies were prepared adhering to the manufacturer-recommended protocols and involved the steps detailed in Table 1. All implants (sample size per group: n = 10) were placed with a final thickness of buccal bone of 2 mm extending from the implant shoulder. Implant insertion was carried out by one experienced clinician using a surgical motor capable of recording actual torque over time and which was set at 25 rpm (iChiropro, BienAir, Biel, Switzerland). Following implant placement, gingiva formers 4 mm in height were attached to the implants and damping capacity measurements (Periotest M, Medizintechnik Gulden, Modautal, Germany) were performed twice, horizontally applying the probe to the gingiva former at a distance of 1 mm.

Table 1.
Description of the implant systems used in this study and the sequence of drills as recommended in the manufacturer-specific guidelines for class III bone. All drills were inserted until a depth of 10 mm was reached unless otherwise specified. All implants were inserted with the surgical motor set at 25 rpm.
For statistical analysis, the mean values of Periotest measurements were calculated and mean maximum values, position of mean maximum values and final values were derived from the curves recorded for torque and strain development during the insertion process. For comparisons between the two implant types, t-tests were applied (α = 0.05) as the mean values could be assumed to be normally distributed according to the central limit theorem.
3. Results
The insertion process of AlfaGate implants took approximately 30% more time as compared to BLT implants, requiring the normalization of data for statistical analysis by setting the duration of full insertion to 1 for each implant type independently. In BLT implants, three fractures of bone specimens occurred due to overstressing and consequently, these samples were excluded from comparative statistical analysis.
Torque and strain development during implant insertion was characteristic for both implant types used. In BLT implants a continuous increase in strain and torque development occurred during insertion reaching its maximum when the implant was fully seated. AlfaGate implants showed maximum torque and strain development when the bulky portion of the implant body passed the cortical layer followed by a drop in both parameters prior to the implants being fully seated (Figure 3 and Figure 4).

Figure 3.
Torque development over time during implant insertion for both groups investigated showing an overall torque increase with insertion depth for Straumann BLT while lower maximum torque was required in AlfaGate implants coinciding with the bulky central part of the implant passing the cortical plate.
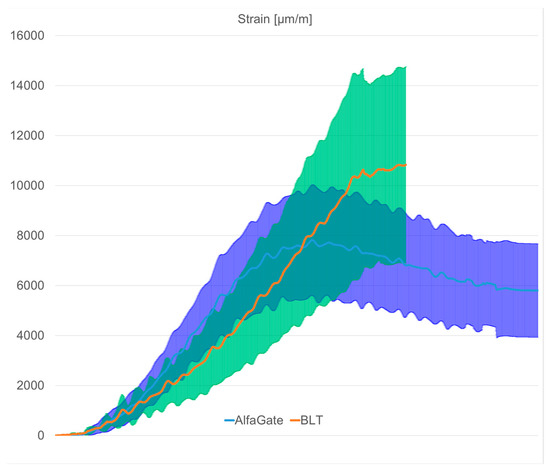
Figure 4.
Strain development over time during implant insertion for both groups investigated with continuously increasing strain levels for Straumann BLT. Lower maximum strain was seen in AlfaGate implants coinciding with the bulky central part of the implant passing the cortical plate.
The mean values and standard deviations for all parameters determined during the experiment are given in Table 2 as well as the results of the t-tests performed for comparing both groups of implants. The mean maximum insertion torque was significantly greater in BLT as compared to AlfaGate (p = 0.0016) and was reached at a significantly later timepoint of the insertion process, i.e., when the implant was almost fully seated (p = 0.0001). The final insertion torque was significantly lower in AlfaGate implants as compared to BLT implants (p < 0.00001).
Table 2.
Mean values and standard deviations recorded for all parameters for both implant types. Results of t-tests for comparisons between the two implant groups are given as p-values with significant differences (p < 0.05) written in bold.
The maximum strain development in buccal bone was greater in BLT implants showing high standard deviation in the range of 30% of absolute values resulting in a non-significant difference compared to AlfaGate implants (p = 0.1069). The maximum strain development in BLT occurred at a significantly later timepoint as compared to AlfaGate implants (p < 0.00001). The final strain development was almost twice as high in BLT implants as compared to AlfaGate implants (p = 0.0137). The primary stability of both implant types as measured with the Periotest device did not differ significantly (p = 0.219).
4. Discussion
Measuring insertion torque, primary implant stability and peri-implant strain, this experiment attempted to compare a novel implant design characterized by a change in core diameter (AlfaGate) to an existing, well-established tapered implant design (BLT). Of course, any other implant system could have been chosen as a control group and would certainly have led to a different but implant-specific insertion torque curve and strain curve. During the insertion of BLT implants, both, emerging strains and insertion torque continuously increased, indicating that primary stability mostly resulted from compressing cortical bone [9,12]. In AlfaGate implants, the maximum torque was measured when the middle portion coincided with the cortical layer indicating that primary stability was mostly obtained by compressing trabecular bone. With the implant types not differing with respect to primary stability, it appears that the tapered BLT implants derived stability from cortical bone while AlfaGate engaged the bony walls over the whole depth of the osteotomy. Given the comparable levels of primary stability achieved, AlfaGate implants should be applicable in the same indications as BLT implants.
Determining implant stability using the Periotest device may be considered as being old-fashioned but appeared to be only option as neither SmartPegs nor MultiPegs were available for the novel implant as a prerequisite for resonance frequency analysis. Akkoyun and coworkers [37] used an identical approach in studying individually fabricated implants.
In addition, both the maximum as well as final torque and strain values were lower in AlfaGate implants although a greater amount of undersizing of the osteotomy was realized here as compared to BLT implants with a conical outer shape, i.e., less bone had to be removed for inserting the implant. The slower insertion of AlfaGate implants may be attributed to the lower thread pitch realized here and to the osteotomy size relative to the implant size. In the BLT group, implants could be inserted into the osteotomy to a much greater extent prior to engaging bony walls as compared to AlfaGate implants (see Figure 2b). While it may be argued that longer insertion time is critical from a clinical perspective, it has to be kept in mind that potentially fewer drill steps will be required for placing the novel implant type. From a methodological point of view, the difference in insertion time hindered from directly comparing whole graphs but required the determination of specific torque and strain points for comparison.
In the past, high levels of insertion torque indicating high levels of primary implant stability as required for immediate loading protocols have been considered as being desirable [11,15]. However, newer literature meanwhile shows that comparably low levels of insertion torque may also result in the good long-term performance of dental implants [16,23]. In addition, recent research also applying molecular analysis has provided evidence that the compression of alveolar bone causes cell death in the surrounding of an osteotomy [18,24,25], which may have negative effects during osseointegration and may be a co-factor for bone loss frequently observed in the initial phase of implant healing [7,14,19]. Based on that, modern implant systems should not only minimize bone trauma during osteotomy preparation but should also minimize peri-implant strain development during insertion. Coinciding with these findings, implants with a triangular cross-section have been introduced not touching buccal bone walls upon final placement in order to avoid excessive stresses in esthetically relevant areas. As clinical studies did not find major benefits of such designs as compared to conventionally round implant shapes [38], the novel design investigated here may be seen as an alternative.
The methodology applied in this experiment followed comparable previous studies on round vs. triangular [31] and wedge-shaped [32] dental implants. In order to benefit from standardized conditions, polyurethane foam was used as a bone surrogate material instead of using cadaver bone [30], which would have also allowed for strain measurements. For future studies, the bone surrogate materials could be adapted in order to better reflect the anatomy of the maxilla and mandible, respectively. In addition to the limited sample size and obvious limitations in simulating the mechanical behavior of alveolar bone, the alignment of the sensing elements of the strain gauges parallel to the occlusal surface of the bone surrogate material as well as the positioning of the implants with a standardized buccal wall thickness have to be seen as limitations. Due to the sensitivity of the measurement technique applied with minor positional deviations having an impact on the absolute readings, strain values can only be used for comparisons on a relative scale. Moreover, all implants were placed by one surgeon and it might be expected that variation in measurement outcomes exists among practitioners.
5. Conclusions
A novel implant design characterized by a shift in its core diameter and a simultaneous change in thread geometry allows for greater undersizing of osteotomies while not mechanically overstressing buccal bone. Clinical studies will be required for verifying a potentially positive effect with respect to initial marginal bone-level changes.
Author Contributions
Conceptualization, M.K.; Formal Analysis, A.S., V.K. and T.G.-K.; Investigation, V.K.; Methodology, V.K.; Resources, T.G.-K.; Software, M.K.; Supervision, M.K.; Visualization, A.S.; Writing—Original Draft, T.G.-K. and M.K.; Writing—Review and Editing, A.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are available on request from the corresponding authors. The data are not publicly available for intellectual property reasons.
Acknowledgments
The authors wish to thank Friedrich Graef, Professor emeritus, Department of Mathematics, University of Erlangen-Nuremberg for statistical data analysis. Implants were kindly provided by Alfa Gate, Kfar Qara, Israel.
Conflicts of Interest
T.G-K. is the inventor of the novel implant design.
References
- Nicolielo, L.F.P.; Van Dessel, J.; Jacobs, R.; Quirino Silveira Soares, M.; Collaert, B. Relationship between trabecular bone architecture and early dental implant failure in the posterior region of the mandible. Clin. Oral Implant. Res. 2020, 31, 153–161. [Google Scholar]
- Karl, M.; Irastorza-Landa, A. Does implant design affect primary stability in extraction sites? Quintessence Int. 2017, 48, 219–224. [Google Scholar] [PubMed]
- Elias, C.N.; Rocha, F.; Nascimento, A.L.; Coelho, P.G. Influence of implant shape, surface morphology, surgical technique and bone quality on the primary stability of dental implants. J. Mech. Behav. Biomed. Mater. 2012, 16, 169–180. [Google Scholar] [CrossRef]
- Gehrke, S.A.; Pérez-Díaz, L.; Mazón, P.; De Aza, P.N. Biomechanical Effects of a New Macrogeometry Design of Dental Implants: An In Vitro Experimental Analysis. J. Funct. Biomater. 2019, 10, 47. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X.; Zhu, Y.; Liu, Z.; Tian, Z.; Zhu, S. Association between diabetes and dental implant complications: A systematic review and meta-analysis. Acta. Odontol. Scand. 2021, 79, 9–18. [Google Scholar] [CrossRef]
- Chen, H.; Liu, N.; Xu, X.; Qu, X.; Lu, E. Smoking, radiotherapy, diabetes and osteoporosis as risk factors for dental implant failure: A meta-analysis. PLoS ONE 2013, 8, e71955. [Google Scholar] [CrossRef]
- Toia, M.; Stocchero, M.; Cecchinato, F.; Corrà, E.; Jimbo, R.; Cecchinato, D. Clinical Considerations of Adapted Drilling Protocol by Bone Quality Perception. Int. J. Oral Maxillofac. Implant. 2017, 32, 1288–1295. [Google Scholar] [CrossRef]
- Dard, M.; Kuehne, S.; Obrecht, M.; Grandin, M.; Helfenstein, J.; Pippenger, B.E. Integrative Performance Analysis of a Novel Bone Level Tapered Implant. Adv. Dent. Res. 2016, 28, 28–33. [Google Scholar] [CrossRef]
- Wang, R.; Eppell, S.J.; Nguyen, C.; Morris, N. Relative Contribution of Trabecular and Cortical Bone to Primary Implant Stability: An In Vitro Model Study. J. Oral Implant. 2016, 42, 145–152. [Google Scholar] [CrossRef]
- Huang, H.L.; Chang, Y.Y.; Lin, D.J.; Li, Y.F.; Chen, K.; Hsu, J.T. Initial stability and bone strain evaluation of the immediately loaded dental implant: An in vitro model study. Clin. Oral Implant. Res. 2011, 22, 691–698. [Google Scholar]
- Cohen, O.; Ormianer, Z.; Tal, H.; Rothamel, D.; Weinreb, M.; Moses, O. Differences in crestal bone-to-implant contact following an under-drilling compared to an over-drilling protocol. A study in the rabbit tibia. Clin. Oral Investig. 2016, 20, 2475–2480. [Google Scholar] [CrossRef]
- Wilson, T.G., Jr.; Miller, R.J.; Trushkowsky, R.; Dard, M. Tapered Implants in Dentistry: Revitalizing Concepts with Technology: A Review. Adv. Dent. Res. 2016, 28, 4–9. [Google Scholar] [CrossRef]
- Ikar, M.; Grobecker-Karl, T.; Karl, M.; Steiner, C. Mechanical stress during implant surgery and its effects on marginal bone: A literature review. Quintessence Int. 2020, 51, 142–150. [Google Scholar] [PubMed]
- Barone, A.; Alfonsi, F.; Derchi, G.; Tonelli, P.; Toti, P.; Marchionni, S.; Covani, U. The Effect of Insertion Torque on the Clinical Outcome of Single Implants: A Randomized Clinical Trial. Clin. Implant. Dent. Relat. Res. 2016, 18, 588–600. [Google Scholar] [CrossRef]
- De Santis, D.; Cucchi, A.; Rigoni, G.; Longhi, C.; Nocini, P.F. Relationship Between Primary Stability and Crestal Bone Loss of Implants Placed with High Insertion Torque: A 3-Year Prospective Study. Int. J. Oral Maxillofac. Implant. 2016, 31, 1126–1134. [Google Scholar] [CrossRef] [PubMed]
- Norton, M.R. The Influence of Low Insertion Torque on Primary Stability, Implant Survival, and Maintenance of Marginal Bone Levels: A Closed-Cohort Prospective Study. Int. J. Oral Maxillofac. Implant. 2017, 32, 849–857. [Google Scholar] [CrossRef]
- Kern, J.S.; Kern, T.; Wolfart, S.; Heussen, N. A systematic review and meta-analysis of removable and fixed implant-supported prostheses in edentulous jaws: Post-loading implant loss. Clin. Oral. Implants. Res. 2016, 27, 174–195. [Google Scholar] [PubMed]
- Stavropoulos, A.; Cochran, D.; Obrecht, M.; Pippenger, B.E.; Dard, M. Effect of Osteotomy Preparation on Osseointegration of Immediately Loaded, Tapered Dental Implants. Adv. Dent. Res. 2016, 28, 34–41. [Google Scholar] [CrossRef]
- Eom, T.G.; Kim, H.W.; Jeon, G.R.; Yun, M.J.; Huh, J.B.; Jeong, C.M. Effects of Different Implant Osteotomy Preparation Sizes on Implant Stability and Bone Response in the Minipig Mandible. Int. J. Oral Maxillofac. Implant. 2016, 31, 997–1006. [Google Scholar] [CrossRef] [PubMed]
- Tian, Y.; Sadowsky, S.J.; Brunski, J.B.; Yuan, X.; Helms, J.A. Effects of masticatory loading on bone remodeling around teeth versus implants: Insights from a preclinical model. Clin. Oral. Implants. Res. 2022, 33, 342–352. [Google Scholar] [CrossRef]
- Abrahamsson, I.; Carcuac, O.; Berglundh, T. Influence of implant geometry and osteotomy design on early bone healing: A pre-clinical in vivo study. Clin. Oral. Implants. Res. 2021, 32, 1190–1199. [Google Scholar] [CrossRef]
- Mehl, C.; Becker, S.T.; Acil, Y.; Harder, S.; Wiltfang, J.; Dabbagh-Afrouz, A.A.; de Buhr, W.; Kern, M. Impact of vertical loading on the implant-bone interface. Clin. Oral. Implants. Res. 2013, 24, 949–956. [Google Scholar] [CrossRef]
- Rea, M.; Lang, N.P.; Ricci, S.; Mintrone, F.; González González, G.; Botticelli, D. Healing of implants installed in over- or under-prepared sites—An experimental study in dogs. Clin. Oral Implant. Res. 2015, 26, 442–446. [Google Scholar] [CrossRef]
- Cha, J.Y.; Pereira, M.D.; Smith, A.A.; Houschyar, K.S.; Yin, X.; Mouraret, S.; Brunski, J.B.; Helms, J.A. Multiscale analyses of the bone-implant interface. J. Dent. Res. 2015, 94, 482–490. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Wu, Y.; Perez, K.C.; Hyman, S.; Brunski, J.B.; Tulu, U.; Bao, C.; Salmon, B.; Helms, J.A. Effects of Condensation on Peri-implant Bone Density and Remodeling. J. Dent. Res. 2017, 96, 413–420. [Google Scholar] [CrossRef]
- Bandela, V.; Shetty, N.; Munagapati, B.; Basany, R.B.; Kanaparthi, S. Comparative Evaluation of Osseodensification Versus Conventional Osteotomy Technique on Dental Implant Primary Stability: An Ex Vivo Study. Cureus 2022, 14, e30843. [Google Scholar] [CrossRef] [PubMed]
- Winter, W.; Möhrle, S.; Holst, S.; Karl, M. Parameters of implant stability measurements based on resonance frequency and damping capacity: A comparative finite element analysis. Int. J. Oral. Maxillofac. Implants. 2010, 25, 532–539. [Google Scholar]
- Albrektsson, T.; Chrcanovic, B.; Östman, P.O.; Sennerby, L. Initial and long-term crestal bone responses to modern dental implants. Periodontology 2000 2017, 73, 41–50. [Google Scholar] [CrossRef]
- Friberg, B.; Ahmadzai, M. A prospective study on single tooth reconstructions using parallel walled implants with internal connection (Nobel Parallel CC) and abutments with angulated screw channels (ASC). Clin. Implant. Dent. Relat. Res. 2019, 21, 226–231. [Google Scholar] [CrossRef] [PubMed]
- Klär, V.; Karl, M.; Grobecker-Karl, T. Bone damage during dental implant insertion: A pilot study combining strain gauge and histologic analysis. Appl. Sci. 2022, 12, 291. [Google Scholar] [CrossRef]
- Steiner, C.; Karl, M.; Grobecker-Karl, T. Insertion and loading characteristics of three different bone-level implants. Int. J. Oral Maxillofac. Implant. 2020, 35, 560–565. [Google Scholar] [CrossRef]
- Steiner, C.; Karl, M.; Grobecker-Karl, T. Wedge shaped vs. round implants: Bone strain during the insertion process. J. Oral Implantol. 2022; accepted. [Google Scholar]
- Sierra-Rebolledo, A.; Allais-Leon, M.; Maurette-O’Brien, P.; Gay-Escoda, C. Primary Apical Stability of Tapered Implants Through Reduction of Final Drilling Dimensions in Different Bone Density Models: A Biomechanical Study. Implant. Dent. 2016, 25, 775–782. [Google Scholar] [CrossRef]
- Di Stefano, D.A.; Arosio, P.; Gastaldi, G.; Gherlone, E. The insertion torque-depth curve integral as a measure of implant primary stability: An in vitro study on polyurethane foam blocks. J. Prosthet. Dent. 2018, 120, 706–714. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.M.; Lee, M.S.; Wang, J.S.; Lin, L.D. The effect of implant design and bone quality on insertion torque, resonance frequency analysis, and insertion energy during implant placement in low or low- to medium-density bone. Int. J. Prosthodont. 2015, 28, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Ueno, D.; Nakamura, K.; Kojima, K.; Toyoshima, T.; Tanaka, H.; Ueda, K.; Koyano, K.; Kodama, T. A stepwise under-prepared osteotomy technique improves primary stability in shallow-placed implants: A preliminary study for simultaneous vertical ridge augmentation. Odontology 2018, 106, 187–193. [Google Scholar] [CrossRef]
- Akkoyun, E.F.; Demirbaş, A.E.; Gümüş, H.Ö.; Alkan, B.A.; Alkan, A. Custom-Made Root Analog Immediate Dental Implants: A Prospective Clinical Study with 1-Year Follow-up. Int. J. Oral. Maxillofac. Implants. 2022, 37, 1223–1231. [Google Scholar] [CrossRef]
- Li Manni, L.; Lecloux, G.; Rompen, E.; Aouini, W.; Shapira, L.; Lambert, F. Clinical and radiographic assessment of circular versus triangular cross-section neck Implants in the posterior maxilla: A 1-year randomized controlled trial. Clin. Oral Implant. Res. 2020, 31, 814–824. [Google Scholar] [CrossRef] [PubMed]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).