
Effect of Rounded and Hunched Shoulder Postures on Myotonometric Measurements of Upper Body Muscles in Sedentary Workers


Abstract
1. Introduction
2. Methods
2.1. Study Participants
2.2. Outcome Measures
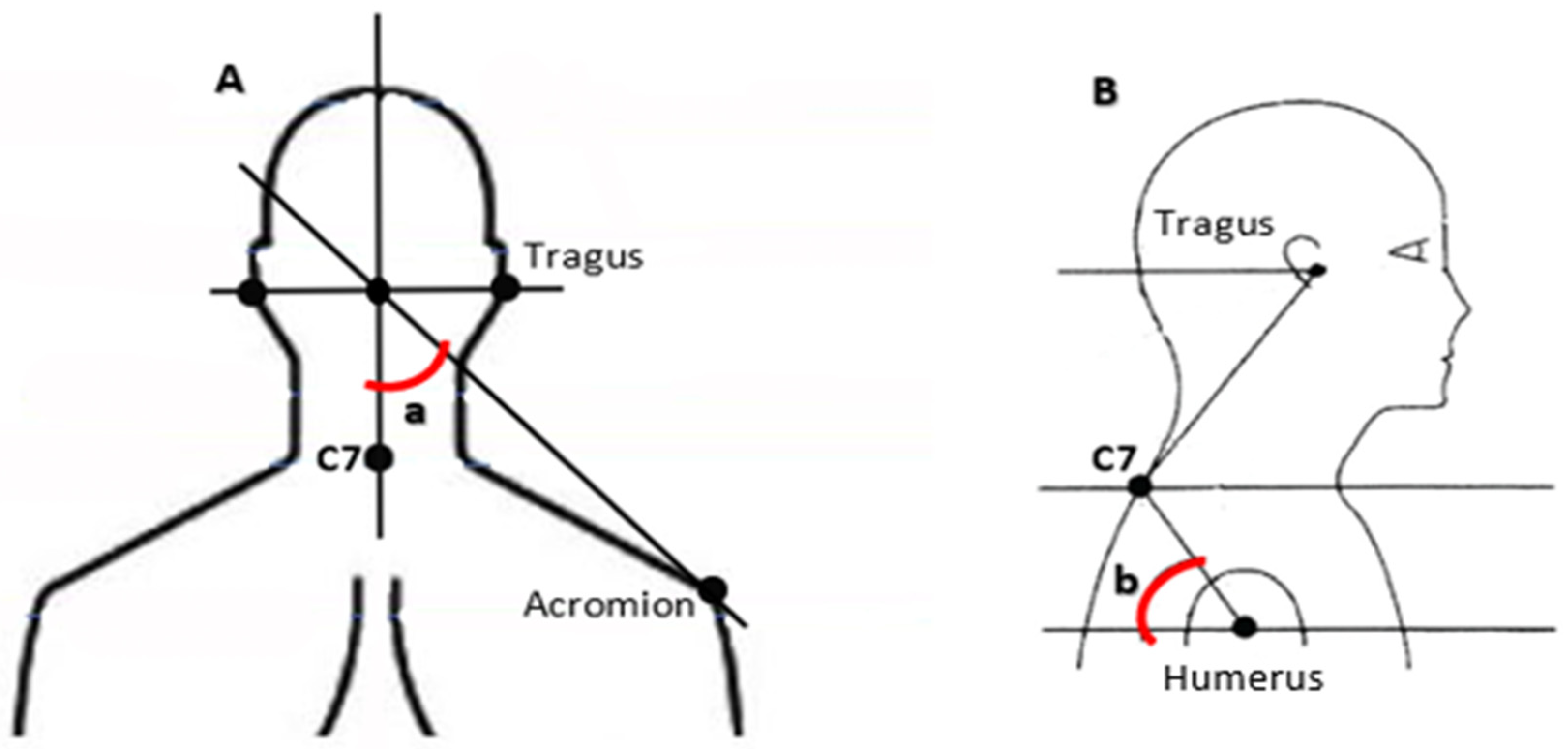
2.3. Measuring Angle
2.4. Procedure
2.5. Data Analysis
2.6. Statistical Analysis
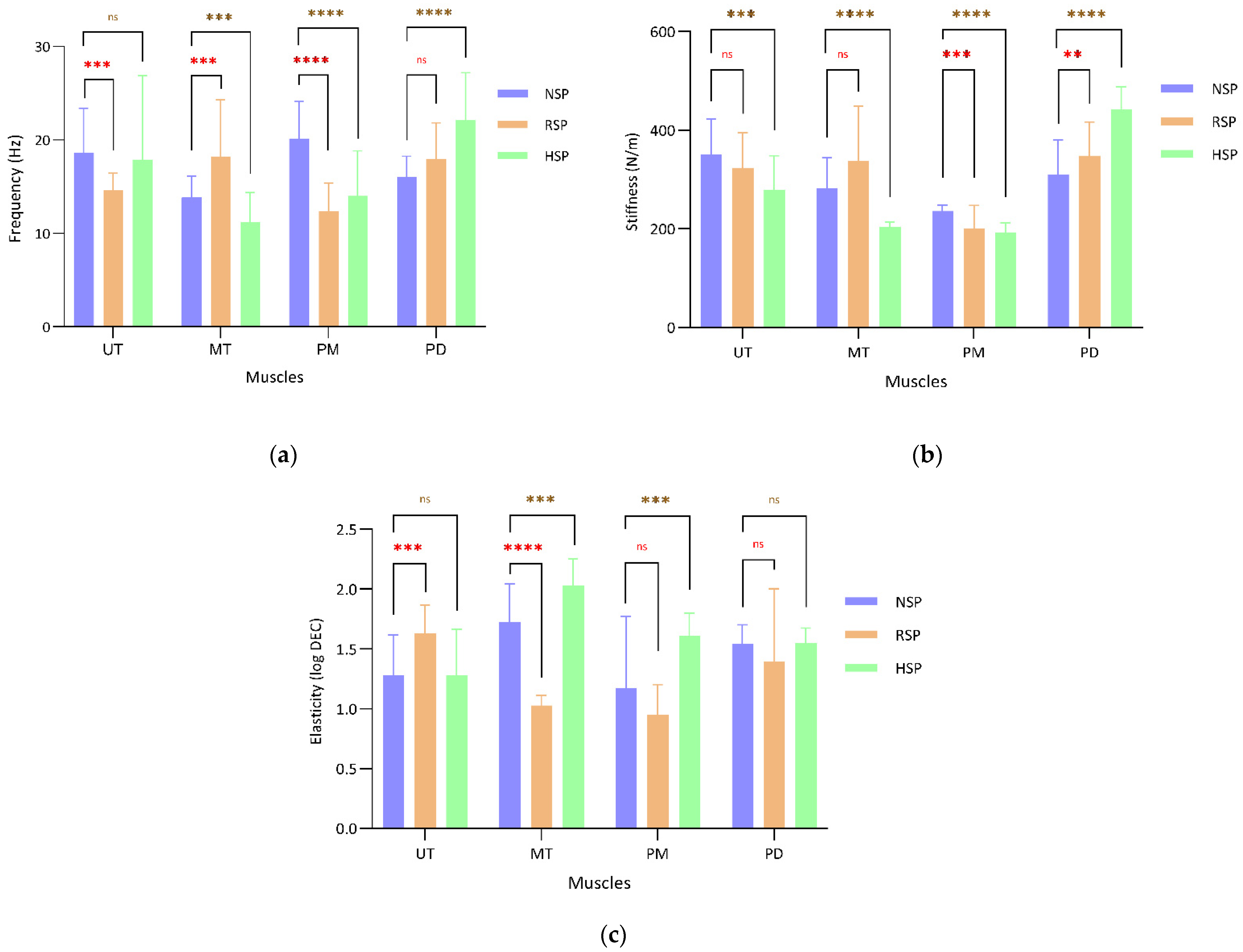
3. Results
4. Discussion
4.1. RSP and the Mechanical Characteristics
4.2. HSP and the Mechanical Characteristics
4.3. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| NSP | Normal shoulder posture |
| RSP | Rounded shoulder posture |
| HSP | Hunched shoulder posture |
| RSA | Rounded shoulder angle |
| HSA | Hunched shoulder angle |
| UT | Upper trapezius |
| MT | Middle trapezius |
| PM | Pectoralis major |
| PD | Posterior deltoid |
| BMI | Body mass index |
References
- Kang, J.-H.; Park, R.-Y.; Lee, S.-J.; Kim, J.-Y.; Yoon, S.-R.; Jung, K.-I. The Effect of The Forward Head Posture on Postural Balance in Long Time Computer Based Worker. Ann. Rehabil. Med. 2012, 36, 98–104. [Google Scholar] [CrossRef] [PubMed]
- Harrison, D.E.; Harrison, D.D.; Betz, J.J.; Janik, T.J.; Holland, B.; Colloca, C.J.; Haas, J.W. Increasing the cervical lordosis with chiropractic biophysics seated combined extension-compression and transverse load cervical traction with cervical manipulation: Nonrandomized clinical control trial. J. Manip. Physiol. Ther. 2003, 26, 139–151. [Google Scholar] [CrossRef]
- Kok, J.; De Vroonhof, P.; Snijders, J.; Roullis, G.; Clarke, M.; Peereboom, K.; Isusi, I. Work-Related MSDs: Prevalence, Costs and Demographics in the EU (European Risk Observatory Executive Summary); Publications Office of the European Union: Bilbao, Spain, 2019; pp. 1–18. [Google Scholar]
- Nguyen, M.T.; Dang, Q.K.; Kim, Y.; Chee, Y. A Measurement System for Rounded Shoulder Posture using a Wearable Stretch Sensor. J. Biomed. Eng. Res. 2018, 39, 10–15. [Google Scholar]
- Soares, F.A.; Andrade, M.M.; De Merletti, R. Automatic Tracking of Innervation Zones Using Image Processing Methods. In Proceedings of the ISSNIP Biosignals and Biorobotics Conference, Vitoria, Brazil, 4–6 January 2010; pp. 214–218. [Google Scholar]
- Mosaad, D.M.; Abdel-Aziem, A.A.; Mohamed, G.I.; Abd-Elaty, E.A.; Mohammed, K.S. Effect of forward head and rounded shoulder posture on hand grip strength in asymptomatic young adults: A cross-sectional study. Bull. Fac. Phys. Ther. 2020, 25, 1–8. [Google Scholar] [CrossRef]
- Tomita, Y.; Suzuki, Y.; Tanaka, Y.; Hasegawa, Y.; Yoshihara, Y.; Okura, K.; Matsuka, Y. Effects of sitting posture and jaw clenching on neck and trunk muscle activities during typing. J. Oral Rehabil. 2021, 48, 568–574. [Google Scholar] [CrossRef]
- Lukasiewicz, A.C.; McClure, P.; Michener, L.; Pratt, N.; Sennett, B.; Ludewig, P. Comparison of 3-Dimensional Scapular Position and Orientation Between Subjects With and Without Shoulder Impingement. J. Orthop. Sports Phys. Ther. 1999, 29, 574–586. [Google Scholar] [CrossRef]
- Lee, J.-H.; Kim, H.; Shin, W.-S. Characteristics of shoulder pain, muscle tone and isokinetic muscle function according to the scapular position of elite boxers. Phys. Ther. Rehabil. Sci. 2020, 9, 98–104. [Google Scholar] [CrossRef]
- Viir, R.; Virkus, A.; Laiho, K.; Rajaleid, K.; Selart, A.; Mikkelson, M. Trapezius muscle tone and viscoelastic properties in sitting and supine positions. Scand. J. Work Environ. Health Suppl. 2007, 33, 76–80. [Google Scholar]
- Naidoo, N.; Lazarus, L.; Van Tongel, A.; Osman, S.; Satyapal, K. Introduction of the angle of shoulder slope in a South African population. SA Orthop. J. 2017, 16, 40–43. [Google Scholar] [CrossRef]
- Ruivo, R.M.; Pezarat-Correia, P.; Carita, A.I. Cervical and shoulder postural assessment of adolescents between 15 and 17 years old and association with upper quadrant pain. Braz. J. Phys. Ther. 2014, 18, 364–371. [Google Scholar] [CrossRef]
- Kocur, P.; Wilski, M.; Goliwąs, M.; Lewandowski, J.; Łochyński, D. Influence of Forward Head Posture on Myotonometric Measurements of Superficial Neck Muscle Tone, Elasticity, and Stiffness in Asymptomatic Individuals With Sedentary Jobs. J. Manip. Physiol. Ther. 2019, 42, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Hibberd, E.E.; Laudner, K.; Berkoff, D.J.; Kucera, K.L.; Yu, B.; Myers, J.B. Comparison of Upper Extremity Physical Characteristics Between Adolescent Competitive Swimmers and Nonoverhead Athletes. J. Athl. Train. 2016, 51, 65–69. [Google Scholar] [CrossRef] [PubMed]
- Leong, H.T.; Hug, F.; Fu, A. Increased Upper Trapezius Muscle Stiffness in Overhead Athletes with Rotator Cuff Tendinopathy. PLoS ONE 2016, 11, e0155187. [Google Scholar] [CrossRef] [PubMed]
- Thigpen, C.A.; Padua, D.A.; Michener, L.A.; Guskiewicz, K.; Giuliani, C.; Keener, J.D.; Stergiou, N. Head and shoulder posture affect scapular mechanics and muscle activity in overhead tasks. J. Electromyogr. Kinesiol. 2010, 20, 701–709. [Google Scholar] [CrossRef] [PubMed]
- Brink, Y.; Crous, L.C.; Louw, Q.A.; Grimmer, K.; Schreve, K. The association between postural alignment and psychosocial factors to upper quadrant pain in high school students: A prospective study. Man. Ther. 2009, 14, 647–653. [Google Scholar] [CrossRef]
- Kim, T.-W.; An, D.-I.; Lee, H.-Y.; Jeong, H.-Y.; Kim, N.-H.; Sung, Y.-H. Effects of elastic band exercise on subjects with rounded shoulder posture and forward head posture. J. Phys. Ther. Sci. 2016, 28, 1733–1737. [Google Scholar] [CrossRef]
- Viir, R.; Laiho, K.; Kramarenko, J.; Mikkelsson, M. Repeatability of Trapezius Muscle Tone Assessment by a Myometric Method. J. Mech. Med. Biol. 2006, 6, 215–228. [Google Scholar] [CrossRef]
- Raine, S.; Twomey, L.T. Head and shoulder posture variations in 160 asymptomatic women and men. Arch. Phys. Med. Rehabil. 1997, 78, 1215–1223. [Google Scholar] [CrossRef]
- Mullix, J.; Warner, M.; Stokes, M. Testing muscle tone and mechanical properties of rectus femoris and biceps femoris using a novel hand held MyotonPRO device: Relative ratios and reliability. Work Pap. Heal. Sci. Internet. 2012, 2051–6266, 1–8. Available online: https://eprints.soton.ac.uk/345285/1/Testing_muscle_tone_and_mechanical_properties_of_rectus_.pdf (accessed on 6 February 2022).
- Kisilewicz, A.; Janusiak, M.; Szafraniec, R.; Smoter, M.; Ciszek, B.; Madeleine, P.; Fernández-De-Las-Peñas, C.; Kawczyński, A. Changes in Muscle Stiffness of the Trapezius Muscle after Application of Ischemic Compression into Myofascial Trigger Points in Professional Basketball Players. J. Hum. Kinet. 2018, 64, 35–45. [Google Scholar] [CrossRef]
- Singla, D.; Veqar, Z. Association Between Forward Head, Rounded Shoulders, and Increased Thoracic Kyphosis: A Review of the Literature. J. Chiropr. Med. 2017, 16, 220–229. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.T.; Moon, J.; Lee, S.H.; Cho, K.H.; Im, S.H.; Kim, M.; Min, K. Changes in Activation of Serratus Anterior, Trapezius and Latissimus Dorsi With Slouched Posture. Ann. Rehabil. Med. 2016, 40, 318–325. [Google Scholar] [CrossRef] [PubMed]
- Cools, A.M.; Declercq, G.A.; Cambier, D.C.; Mahieu, N.N.; Witvrouw, E.E. Trapezius activity and intramuscular balance during isokinetic exercise in overhead athletes with impingement symptoms. Scand. J. Med. Sci. Sports 2006, 17, 25–33. [Google Scholar] [CrossRef]
- Guney-Deniz, H.; Harput, G.; Toprak, U.; Duzgun, I. Relationship Between Middle Trapezius Muscle Activation and Acromiohumeral Distance Change During Shoulder Elevation With Scapular Retraction. J. Sport Rehabil. 2019, 28, 266–271. [Google Scholar] [CrossRef]
- Cheon, S.; Park, S. Changes in neck and upper trunk muscle activities according to the angle of movement of the neck in subjects with forward head posture. J. Phys. Ther. Sci. 2017, 29, 191–193. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Felix, D. Posture and Fitness (Part 1): Kyphosis (Rounded Shoulders). Available online: https://www.nifs.org/blog/posture-and-fitness-kyphosis-rounded-shoulders (accessed on 6 February 2022).
- Guduru, R.K.R.; Domeika, A.; Dubosiene, M. Analysis of muscle activation during sedentary positions in different upper extremities in office workers. Turk. J. Physiother. Rehabil. 2021, 32, 31655–31660. [Google Scholar]
- Seo, S.-S.; Choi, J.-S.; An, K.-C.; Kim, J.-H.; Kim, S.-B. The factors affecting stiffness occurring with rotator cuff tear. J. Shoulder Elb. Surg. 2012, 21, 304–309. [Google Scholar] [CrossRef]
- Hellig, T.; Rick, V.; Mertens, A.; Nitsch, V.; Brandl, C. Investigation of observational methods assessing workload of static working postures based on surface electromyography. Work 2019, 62, 185–195. [Google Scholar] [CrossRef]
- Mehrab, M.; de Vos, R.-J.; Kraan, G.A.; Mathijssen, N.M. Injury Incidence and Patterns Among Dutch CrossFit Athletes. Orthop. J. Sports Med. 2017, 5, 2325967117745263. [Google Scholar] [CrossRef]
- Roja, Z.; Kalkis, V.; Vain, A.; Kalkis, H.; Eglite, M. Assessment of skeletal muscle fatigue of road maintenance workers based on heart rate monitoring and myotonometry. J. Occup. Med. Toxicol. 2006, 1, 20. [Google Scholar] [CrossRef]
- Hess, S. Functional stability of the glenohumeral joint. Man. Ther. 2000, 5, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Bailey, L.B.; Shanley, E.; Hawkins, R.; Beattie, P.F.; Fritz, S.; Kwartowitz, D.; Thigpen, C.A. Mechanisms of Shoulder Range of Motion Deficits in Asymptomatic Baseball Players. Am. J. Sports Med. 2015, 43, 2783–2793. [Google Scholar] [CrossRef] [PubMed]
- Guduru, R.K.R.; Domeika, A.; Dubosiene, M.; Kazlauskiene, K. Prediction framework for upper body sedentary working behaviour by using deep learning and machine learning techniques. Soft Comput. 2021, 1–16. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Mechanical Characteristics | NSP (n = 20) | RSP (n = 20) | HSP (n = 20) | Calculated Statistics | (LCI, UCI) | p |
|---|---|---|---|---|---|---|
| Demographics | ||||||
| RSP | ||||||
| Sex (W/M) | 0/20 | 0/20 | - | - | - | - |
| Age (y) | 29.1 ± 2.8 | 29.6 ± 3.2 | - | t (38) = −0.56 | (−2.5 to 1.4) | 0.576 |
| Height (cm) | 176.4 ± 5.2 | 175.5 ± 5.2 | - | t (38) = 0.58 | (−2.3 to 4.3) | 0.561 |
| Body mass (kg) | 66.8 ± 6.3 | 67.1 ± 7.8 | - | t (38) = −0.11 | (−4.8 to 4.2) | 0.908 |
| BMI (kg/m2) | 21.4 ± 1.6 | 21.7 ± 2.1 | - | t (38) = −0.53 | (−1.5 to 0.8) | 0.594 |
| HSP | ||||||
| Sex (W/M) | 0/20 | - | 0/20 | - | - | - |
| Age (y) | 29.1 ± 2.8 | - | 28.6 ± 2.6 | t (38) = 0.57 | (−1.2 to 2.2) | 0.568 |
| Height (cm) | 176.4 ± 5.2 | - | 175.4 ± 5.1 | t (38) = 0.65 | (−2.2 to 4.3) | 0.516 |
| Body mass (kg) | 66.8 ± 6.3 | - | 67.6 ± 5.5 | t (38) = −0.40 | (−4.5 to 3.0) | 0.687 |
| BMI (kg/m2) | 21.4 ± 1.6 | - | 22.0 ± 1.8 | t (38) = −1.07 | (−1.7 to 0.5) | 0.289 |
| Clinical characteristics | ||||||
| RSA (°) | 44.6 ± 4.8 | 47.4 ± 2.5 | - | t (38) = −2.2 | (−5.2 to −0.2) | 0.030 |
| HSA (°) | 44.7 ± 4.3 | - | 50.9 ± 3.0 | t (38) = −5.16 | (−8.6 to −3.7) | <0.001 |
| Mechanical Parameters | NSP (n = 20) | RSP (n = 20) | Calculated Statistics | d (LCI, UCI) | p |
|---|---|---|---|---|---|
| Tone (Hz) | |||||
| UT | 18.6 ± 4.7 | 14.7 ± 1.8 | t (38) = 3.5 | 1.1 (0.4 to 1.8) | 0.002 |
| MT | 13.9 ± 2.3 | 18.2 ± 6.0 | t (38) = −3.0 | 1.0 (−1.6 to −0.3) | 0.006 |
| PM | 20.1 ± 4.0 | 12.4 ± 3.1 | t (38) = 6.9 | 2.2 (1.4 to 3.0) | <0.001 |
| PD | 16.0 ± 2.2 | 18.0 ± 3.8 | t (38) = −1.9 | 0.6 (−1.2 to 0.0) | 0.060 |
| Stiffness (N/m) | |||||
| UT | 350.4 ± 72.0 | 323.8 ± 71.4 | t (38) = 1.1 | 0.3 (−0.2 to 0.9) | 0.248 |
| MT | 282.0 ± 62.9 | 337.0 ± 111.9 | t (38) = −1.9 | 0.6 (−1.2 to 0.0) | 0.065 |
| PM | 235.9 ± 11.7 | 201.1 ± 45.8 | t (38) = 3.2 | 1.0 (0.3 to 1.6) | 0.003 |
| PD | 309.9 ± 70.7 | 348.15 ± 68.7 | t (38) = −1.7 | 0.5 (−1.1 to 0.0) | 0.046 |
| Elasticity (log DEC) | |||||
| UT | 1.2 ± 0.3 | 1.6 ± 0.2 | t (38) = −3.8 | −1.2 (−1.8 to −0.5) | 0.001 |
| MT | 1.7 ± 0.3 | 1.0 ± 0.08 | t (38) = 9.4 | 2.9 (2.0 to 3.9) | <0.001 |
| PM | 1.1 ± 0.5 | 0.9 ± 0.2 | t (38) = 1.5 | 0.4 (−0.15 to 1.1) | 0.143 |
| PD | 1.5 ± 0.1 | 1.4 ± 0.6 | t (38) = 1.0 | 0.3 (−0.2 to 0.9) | 0.302 |
| Mechanical Parameters | NSP (n = 20) | HSP (n = 20) | Calculated Statistics | d (LCI, UCI) | p |
|---|---|---|---|---|---|
| Tone (Hz) | |||||
| UT | 18.6 ± 4.7 | 17.9 ± 9.1 | t (38) = 0.3 | 0.10 (−0.5 to 0.7) | 0.731 |
| MT | 13.9 ± 2.3 | 11.2 ± 3.1 | t (38) = 3.0 | 0.96 (0.3 to 1.6) | 0.004 |
| PM | 20.1 ± 4.0 | 14.0 ± 4.8 | t (38) = 4.3 | 1.38 (0.6 to 2.0) | <0.001 |
| PD | 16.0 ± 2.2 | 22.2 ± 5.0 | t (38) = −4.9 | −1.57 (−2.2 to −0.8) | <0.001 |
| Stiffness (N/m) | |||||
| UT | 350.4 ± 72.0 | 278.6 ± 69.6 | t (38) = 3.2 | 1.0 (0.3 to 1.6) | 0.003 |
| MT | 282.0 ± 62.9 | 204.2 ± 9.5 | t (38) = 5.4 | 1.7 (0.9 to 2.4) | <0.001 |
| PM | 235.9 ± 11.7 | 192.5 ±19.7 | t (38) = 8.4 | 2.6 (1.8 to 3.5) | <0.001 |
| PD | 309.9 ± 70.7 | 441.7 ± 45.9 | t (38) = −6.9 | −2.2 (−2.9 to −1.4) | <0.001 |
| Elasticity (log DEC) | |||||
| UT | 1.2 ± 0.3 | 1.2 ± 0.3 | t (38) = 0.0 | 0.00 (−0.6 to 0.6) | 0.993 |
| MT | 1.7 ± 0.3 | 2.0 ± 0.2 | t (38) = −3.4 | 1.1 (−1.7 to −0.4) | 0.001 |
| PM | 1.1 ± 0.6 | 1.6 ± 0.1 | t (38) = −3.1 | 0.9 (−1.6 to −0.3) | 0.005 |
| PD | 1.5 ± 0.15 | 1.5 ± 0.1 | t (38) = −0.1 | 0.0 (−0.6 to 0.5) | 0.877 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guduru, R.K.R.; Domeika, A.; Domeikienė, A. Effect of Rounded and Hunched Shoulder Postures on Myotonometric Measurements of Upper Body Muscles in Sedentary Workers. Appl. Sci. 2022, 12, 3333. https://doi.org/10.3390/app12073333
Guduru RKR, Domeika A, Domeikienė A. Effect of Rounded and Hunched Shoulder Postures on Myotonometric Measurements of Upper Body Muscles in Sedentary Workers. Applied Sciences. 2022; 12(7):3333. https://doi.org/10.3390/app12073333
Chicago/Turabian StyleGuduru, Rama Krishna Reddy, Aurelijus Domeika, and Auksė Domeikienė. 2022. "Effect of Rounded and Hunched Shoulder Postures on Myotonometric Measurements of Upper Body Muscles in Sedentary Workers" Applied Sciences 12, no. 7: 3333. https://doi.org/10.3390/app12073333
APA StyleGuduru, R. K. R., Domeika, A., & Domeikienė, A. (2022). Effect of Rounded and Hunched Shoulder Postures on Myotonometric Measurements of Upper Body Muscles in Sedentary Workers. Applied Sciences, 12(7), 3333. https://doi.org/10.3390/app12073333