
A Comparative Analysis of Novel Biomarkers in Sepsis and Cardiovascular Disease

 ,
,  , ,
, , 
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Laboratory Analysis
2.2. Statistical Analysis
3. Results
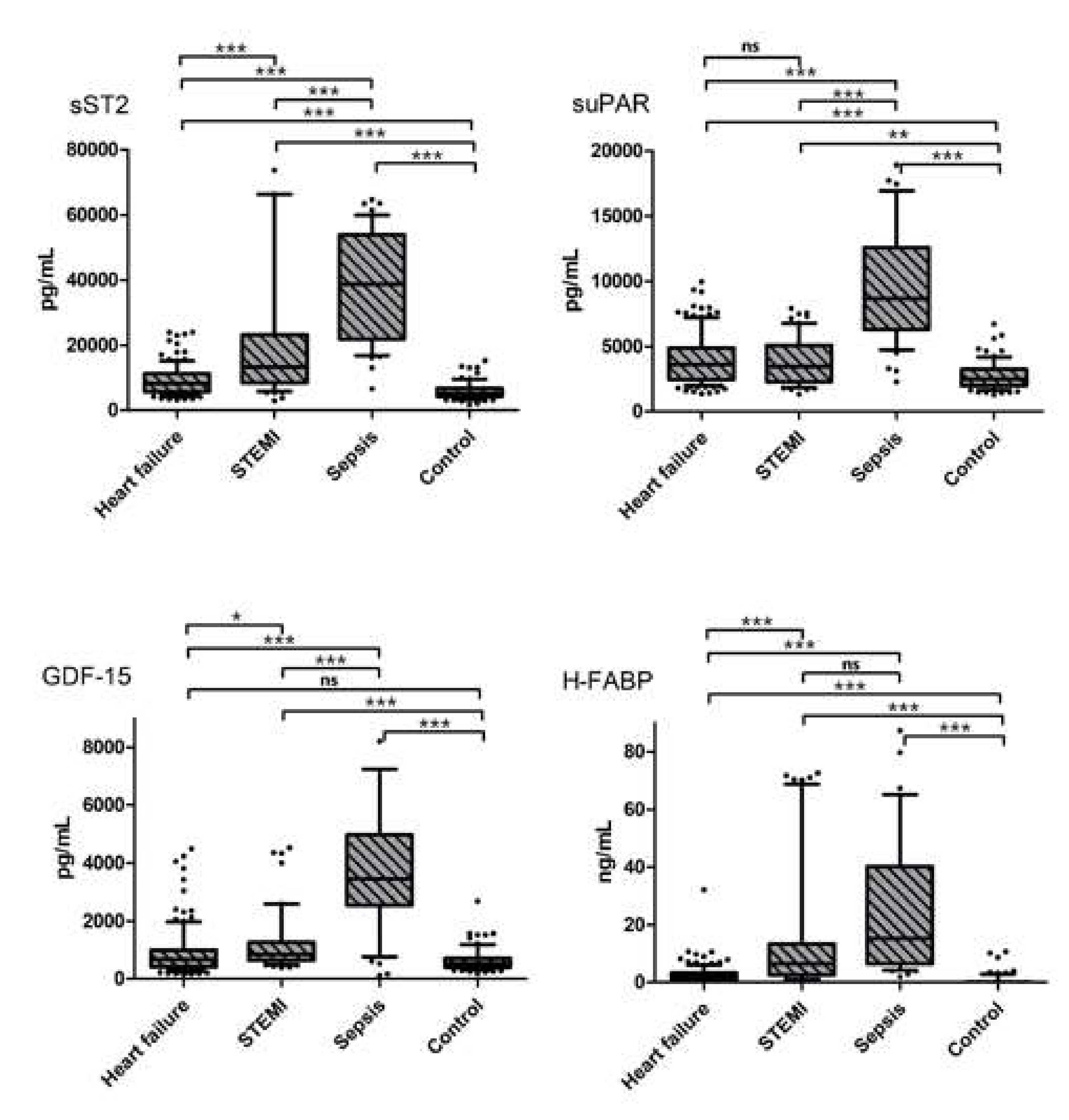
3.1. Biomarker Concentrations and Correlation Analysis
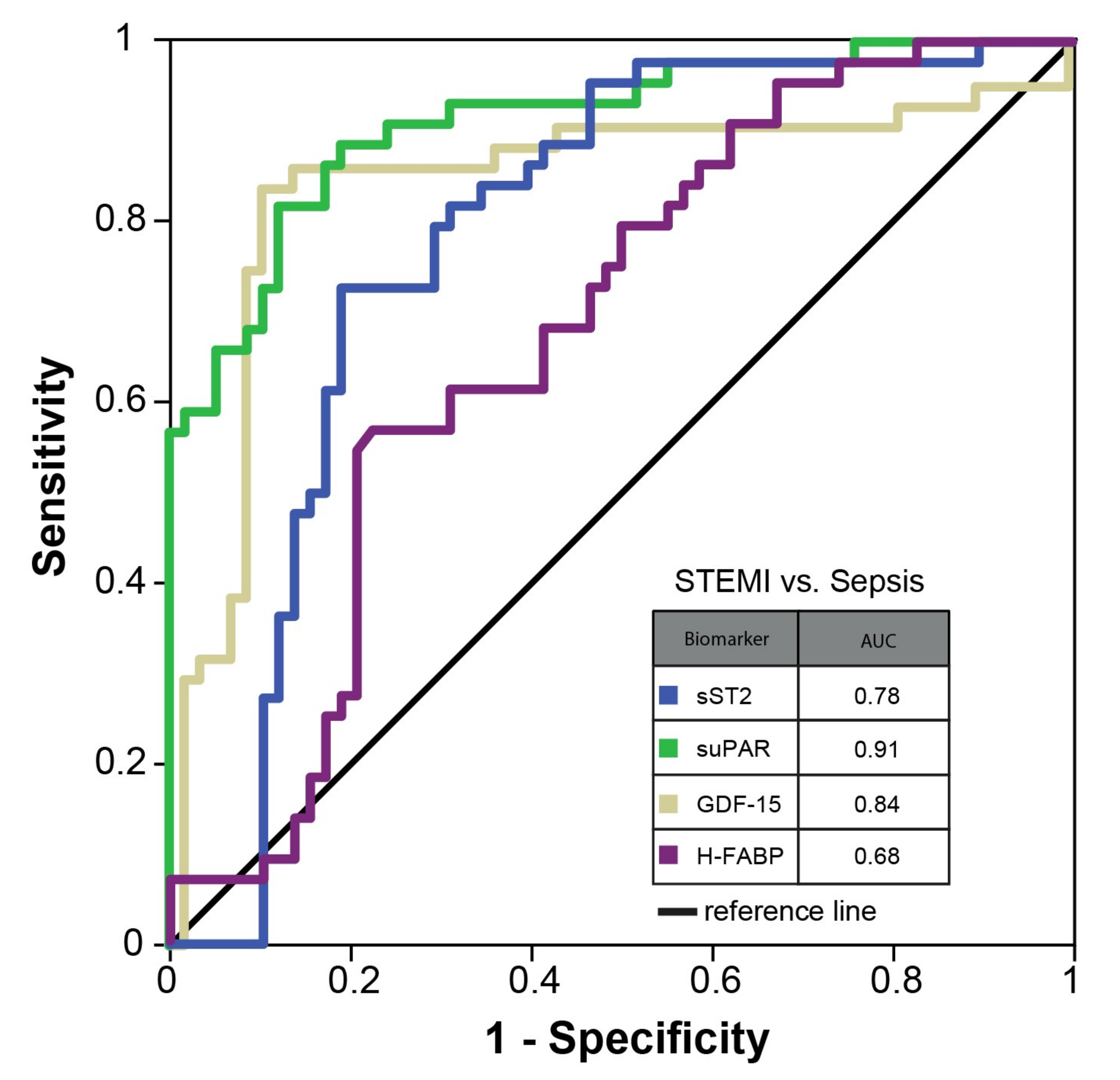
3.2. Binary Logistic Regression and ROC Analyses
4. Discussion
5. Conclusions
6. Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vincent, J.-L.; Sakr, Y.; Sprung, C.L.; Ranieri, V.M.; Reinhart, K.; Gerlach, H.; Moreno, R.; Carlet, J.; Le Gall, J.-R.; Payen, D. Sepsis in European intensive care units: Results of the SOAP study. Crit. Care Med. 2006, 34, 344–353. [Google Scholar] [CrossRef] [PubMed]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Lagu, T.; Rothberg, M.B.; Shieh, M.-S.; Pekow, P.S.; Steingrub, J.S.; Lindenauer, P.K. Hospitalizations, costs, and outcomes of severe sepsis in the United States 2003 to 2007. Crit. Care Med. 2012, 40, 754–761. [Google Scholar] [CrossRef]
- Arefian, H.; Heublein, S.; Scherag, A.; Brunkhorst, F.M.; Younis, M.Z.; Moerer, O.; Fischer, D.; Hartmann, M. Hospital-related cost of sepsis: A systematic review. J. Infect. 2016, 74, 107–117. [Google Scholar] [CrossRef]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2018, 39, 119–177. [Google Scholar]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.; Coats, A.J.; Falk, V.; González-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Heart Fail. 2016, 18, 891–975. [Google Scholar]
- Rhodes, A.; Evans, L.E.; Alhazzani, W.; Levy, M.M.; Antonelli, M.; Ferrer, R.; Kumar, A.; Sevransky, J.E.; Sprung, C.L.; Nunnally, M.E.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Crit. Care Med. 2017, 45, 486–552. [Google Scholar] [CrossRef]
- Han, X.; Zhang, S.; Chen, Z.; Adhikari, B.K.; Zhang, Y.; Zhang, J.; Sun, J.; Wang, Y. Cardiac biomarkers of heart failure in chronic kidney disease. Clin. Chim. Acta 2020, 510, 298–310. [Google Scholar] [CrossRef]
- Zeier, M.; Reiser, J. suPAR and chronic kidney disease—A podocyte story. Pflügers Arch. Eur. J. Physiol. 2017, 469, 1017–1020. [Google Scholar] [CrossRef]
- Rezar, R.; Jirak, P.; Gschwandtner, M.; Derler, R.; Felder, T.K.; Haslinger, M.; Kopp, K.; Seelmaier, C.; Granitz, C.; Hoppe, U.C.; et al. Heart-Type Fatty Acid-Binding Protein (H-FABP) and its Role as a Biomarker in Heart Failure: What Do We Know So Far? J. Clin. Med. 2020, 9, 164. [Google Scholar] [CrossRef] [Green Version]
- Ye, X.-D.; He, Y.; Wang, S.; Wong, G.T.; Irwin, M.; Xia, Z. Heart-type fatty acid binding protein (H-FABP) as a biomarker for acute myocardial injury and long-term post-ischemic prognosis. Acta Pharmacol. Sin. 2018, 39, 1155–1163. [Google Scholar] [CrossRef] [PubMed]
- Yin, L.; Mou, H.; Shao, J.; Zhu, Y.; Pang, X.; Yang, J.; Zhang, J.; Shi, W.; Yu, S.; Wang, H. Correlation between Heart fatty acid binding protein and severe COVID-19: A case-control study. PLoS ONE 2020, 15, e0231687. [Google Scholar] [CrossRef] [PubMed]
- Otaki, Y.; Watanabe, T.; Kubota, I. Heart-type fatty acid-binding protein in cardiovascular disease: A systemic review. Clin. Chim. Acta 2017, 474, 44–53. [Google Scholar] [CrossRef] [PubMed]
- Wischhusen, J.; Melero, I.; Fridman, W.H. Growth/Differentiation Factor-15 (GDF-15): From Biomarker to Novel Targetable Immune Checkpoint. Front. Immunol. 2020, 11, 951. [Google Scholar] [CrossRef]
- Buendgens, L.; Yagmur, E.; Bruensing, J.; Herbers, U.; Baeck, C.; Trautwein, C.; Koch, A.; Tacke, F. Growth Differentiation Factor-15 Is a Predictor of Mortality in Critically Ill Patients with Sepsis. Dis. Markers 2017, 18, 5271203. [Google Scholar] [CrossRef] [Green Version]
- Kretzschmar, D.; Betge, S.; Windisch, A.; Pistulli, R.; Rohm, I.; Fritzenwanger, M.; Jung, C.; Schubert, K.; Theis, B.; Petersen, I.; et al. Recruitment of circulating dendritic cell precursors into the infarcted myocardium and pro-inflammatory response in acute myocardial infarction. Clin. Sci. 2012, 123, 387–398. [Google Scholar] [CrossRef] [Green Version]
- Schmitz, J.; Owyang, A.; Oldham, E.; Song, Y.; Murphy, E.; McClanahan, T.K.; Zurawski, G.; Moshrefi, M.; Qin, J.; Li, X.; et al. IL-33, an Interleukin-1-like Cytokine that Signals via the IL-1 Receptor-Related Protein ST2 and Induces T Helper Type 2-Associated Cytokines. Immunity 2005, 23, 479–490. [Google Scholar] [CrossRef] [Green Version]
- Sanada, S.; Hakuno, D.; Higgins, L.J.; Schreiter, E.; McKenzie, A.N.; Lee, R.T. IL-33 and ST2 comprise a critical biomechanically induced and cardioprotective signaling system. J. Clin. Investig. 2007, 117, 1538–1549. [Google Scholar] [CrossRef] [Green Version]
- Griesenauer, B.; Paczesny, S. The ST2/IL-33 Axis in Immune Cells during Inflammatory Diseases. Front. Immunol. 2017, 8, 475. [Google Scholar] [CrossRef]
- Parenica, J.; Malaska, J.; Jarkovsky, J.; Lipkova, J.; Dastych, M.; Helanova, K.; Litzman, J.; Tomandl, J.; Littnerova, S.; Sevcikova, J.; et al. Soluble ST2 levels in patients with cardiogenic and septic shock are not predictors of mortality. Exp. Clin. Cardiol. 2012, 17, 205–209. [Google Scholar]
- Thuno, M.; Macho, B.; Eugen-Olsen, J. suPAR: The molecular crystal ball. Dis. Markers 2009, 27, 157–172. [Google Scholar] [CrossRef] [PubMed]
- Koch, A.; Voigt, S.; Kruschinski, C.; Sanson, E.; Dückers, H.; Horn, A.; Yagmur, E.; Zimmermann, H.; Trautwein, C.; Tacke, F. Circulating soluble urokinase plasminogen activator receptor is stably elevated during the first week of treatment in the intensive care unit and predicts mortality in critically ill patients. Crit. Care 2011, 15, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rasmussen, L.J.H.; Ladelund, S.; Haupt, T.H.; Ellekilde, G.; Poulsen, J.H.; Iversen, K.; Eugen-Olsen, J.; Andersen, O. Soluble urokinase plasminogen activator receptor (suPAR) in acute care: A strong marker of disease presence and severity, readmission and mortality. A retrospective cohort study. Emerg. Med. J. 2016, 33, 769–775. [Google Scholar] [CrossRef] [Green Version]
- Hodges, G.W.; Bang, C.N.; Wachtell, K.; Eugen-Olsen, J.; Jeppesen, J.L. suPAR: A New Biomarker for Cardiovascular Disease? Can. J. Cardiol. 2015, 31, 1293–1302. [Google Scholar] [CrossRef] [PubMed]
- Berrar, D.; Flach, P. Caveats and pitfalls of ROC analysis in clinical microarray research (and how to avoid them). Brief. Bioinform. 2011, 13, 83–97. [Google Scholar] [CrossRef] [PubMed]
- Janssens, A.; Martens, F.K. Reflection on modern methods: Revisiting the area under the ROC Curve. Int. J. Epidemiol. 2020, 49, 1397–1403. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Total Cohort (n= 311) | Heart Failure (n= 123) | STEMI (n= 60) | Sepsis (n= 53) | Control (n= 75) | p-Value | |
|---|---|---|---|---|---|---|
| Age (years; median (IQR)) | 61 (53–71) * | 60 (51–69) † | 60 (54–71) * | 62 (50–75) * | 65 (54–71) * | 0.372 |
| Height (m; median (IQR)) | 1.73 (1.64–1.80) * | 1.75 (1.68–1.80) † | 1.73 (1.64–1.78) * | 1.74 (1.67–1.80) * | 1.68 (1.61–1.77) * | 0.001 |
| Weight (kg; median (IQR)) | 80.5 (70.0–94.0) * | 83.0 (74.5–98.5) † | 80.0 (74.0–94.5) * | 80.0 (63.5–90.0) * | 76.5 (66.5–90.0) * | 0.009 |
| BMI (kg/m2; median (IQR)) | 27.6 (24.3–31.0) * | 28.2 (24.8–31.6) † | 28.0 (24.7–31.2) * | 26.2 (21.8–29.4) * | 27.4 (23.8–30.7) * | 0.030 |
| EF (%; median (IQR)) | 47 (33–63) ‡ | 36 (28–45) * | 55 (46–68) || | n.a. | 67 (63–74) ‡ | <0.0001 |
| CRP (mg/L; median (IQR)) | 61.1 (26.0–150.0) † | 3.1 (0.0–7.6) ‡ | 7.9 (2.5–11.6) * | 235.9 (93.0–336.6) * | 3.9 (3.2–5.4) § | <0.0001 |
| Creatinine (µmol/L; median (IQR)) | 82.0 (67.0–113.5) † | 90.0 (79.0–125.0) ‡ | 68.5 (61.8–81.8) * | 148.0 (107.3–208.3) * | 70.5 (64.0–83.5) * | <0.0001 |
| Urea (mmol/L; median (IQR)) | 6.4 (4.9–9.8) § | 6.8 (5.3–9.8) ‡ | 5.1 (4.1–6.4) † | 14.5 (9.0–22.0) † | 5.4 (4.5–6.7) ‡ | <0.0001 |
| Gender (% male, (n)) | 65.2 (193) * | 80.7 (88) † | 71.2 (42) * | 69.8 (37) * | 34.7 (26) * | <0.0001 |
| Diabetes (%, (n)) | 29.1 (83) * | 37.0 (40) † | 29.1 (16) * | 29.2 (14) * | 17.6 (13) * | 0.045 |
| Hypertension (%, (n)) | 68.6 (199) * | 59.3 (64) † | 92.7 (51) * | 39.6 (21) * | 85.1 (63) * | <0.0001 |
| Chronic kidney disease (%, (n)) | 11.3 (31) † | 20.0 (19) ‡ | 5.3 (3) * | 9.4 (5) * | 5.7 (4) * | 0.008 |
| Smoking (%, (n)) | 44.9 (102) ‡ | 45.4 (49) † | 63.5 (33) † | n.a. | 29.9 (20) † | 0.001 |
| Dyslipidemia (%, (n)) | 63.9 (129) ‡ | 71.3 (77) † | 62.5 (25) ‡ | n.a. | 50.0 (27) ‡ | 0.029 |
| Overweight (%, (n)) | 44.1 (104) ‡ | 38.0 (41) † | 54.5 (30) * | n.a. | 45.2 (33) * | 0.127 |
| Total Cohort | Heart Failure | STEMI | Sepsis | Control | p-Value | |
|---|---|---|---|---|---|---|
| sST2 (pg/mL; median (IQR)) | 8637.5 (5553.5–17141.0) | 8181.3 (5683.1–11217.4) | 13,210.9 (8496.9–23,113.5) | 38,701.9 (21,834.5–53,879.3) | 5209.9 (4242.9–6850.2) | <0.0001 |
| suPAR (pg/mL; median IQR)) | 3459.6 (2349.4–5363.7) | 3596.6 (2454.3–4897.3) | 3461.2 (2282.2–5091.0) | 8653.4 (6297.6–12,597.0) | 2513.0 (1975.2–3254.6) | <0.0001 |
| GDF-15 (pg/mL; median (IQR)) | 711.2 (489.2–1495.5) | 667.8 (420.5–1002.4) | 841.3 (644.1–1264.7) | 3455.9 (2545.3–4976.6) | 531.9 (397.8–706.2) | <0.0001 |
| H-FABP (ng/mL; median (IQR)) | 2.25 (0.00–6.84) | 1.90 (0.99–3.26) | 6.44 (2.69–13.39) | 15.28 (6.40–40.13) | 0.00 (0.00–0.00) | <0.0001 |
| Age (Years) | BMI (kg/m²) | EF (%) | CRP (mg/L) | Creatinine (µmol/L) | Urea (mmol/L) | ||
|---|---|---|---|---|---|---|---|
| sST2 (pg/mL) | rs | 0.038 | −0.019 | −0.306 | 0.438 | 0.336 | 0.329 |
| p-value | 0.525 | 0.748 | <0.0001 | <0.0001 | <0.0001 | <0.0001 | |
| suPAR (pg/mL) | rs | 0.104 | −0.090 | −0.241 | 0.461 | 0.395 | 0.399 |
| p-value | 0.081 | 0.134 | 0.001 | <0.0001 | <0.0001 | <0.0001 | |
| GDF-15 (pg/mL) | rs | 0.194 | −0.059 | −0.137 | 0.443 | 0.378 | 0.362 |
| p-value | 0.001 | 0.328 | 0,066 | <0.0001 | <0.0001 | <0.0001 | |
| HFABP (ng/mL) | rs | 0.064 | −0.027 | −0.365 | 0.256 | 0.308 | 0.310 |
| p-value | 0.281 | 0.647 | <0.0001 | 0.000 | <0.0001 | <0.0001 | |
| Biomarkers | Dependent Variable: Sepsis | ||
|---|---|---|---|
| Adjustment for: Age, CRP, Creatinine | |||
| B | 95%CI | p-Value | |
| sST2 (ng/mL) | 1.034 | 1.011–1.057 | 0.004 |
| suPAR (ng/mL) | 1.630 | 1.291–2.057 | <0.0001 |
| GDF-15 (ng/mL) | 1.777 | 1.308–2.415 | <0.0001 |
| H-FABP (ng/mL) | 1.031 | 1.009–1.053 | 0.006 |
| Optimal Cut-Off Values for Sepsis | |
|---|---|
| Biomarker | Cut-Off |
| sST2 | 15,909 pg/mL |
| GDF-15 | 2090 pg/mL |
| suPAR | 5414 pg/mL |
| H-FABP | 4 ng/mL |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jirak, P.; Haertel, F.; Mirna, M.; Rezar, R.; Lichtenauer, M.; Paar, V.; Motloch, L.J.; Topf, A.; Yilmaz, A.; Hoppe, U.C.; et al. A Comparative Analysis of Novel Biomarkers in Sepsis and Cardiovascular Disease. Appl. Sci. 2022, 12, 1419. https://doi.org/10.3390/app12031419
Jirak P, Haertel F, Mirna M, Rezar R, Lichtenauer M, Paar V, Motloch LJ, Topf A, Yilmaz A, Hoppe UC, et al. A Comparative Analysis of Novel Biomarkers in Sepsis and Cardiovascular Disease. Applied Sciences. 2022; 12(3):1419. https://doi.org/10.3390/app12031419
Chicago/Turabian StyleJirak, Peter, Franz Haertel, Moritz Mirna, Richard Rezar, Michael Lichtenauer, Vera Paar, Lukas J. Motloch, Albert Topf, Atilla Yilmaz, Uta C. Hoppe, and et al. 2022. "A Comparative Analysis of Novel Biomarkers in Sepsis and Cardiovascular Disease" Applied Sciences 12, no. 3: 1419. https://doi.org/10.3390/app12031419
APA StyleJirak, P., Haertel, F., Mirna, M., Rezar, R., Lichtenauer, M., Paar, V., Motloch, L. J., Topf, A., Yilmaz, A., Hoppe, U. C., Schulze, P. C., Nuding, S., Werdan, K., Kretzschmar, D., Pistulli, R., & Ebelt, H. (2022). A Comparative Analysis of Novel Biomarkers in Sepsis and Cardiovascular Disease. Applied Sciences, 12(3), 1419. https://doi.org/10.3390/app12031419