
Usability and Acceptance of Exergames Using Different Types of Training among Older Hypertensive Patients in a Simulated Mixed Reality


Abstract
1. Introduction
2. Related Work
2.1. Technology Acceptance Models
2.2. The Usability and Acceptance of HMD-Based VR Exergames in Older Adults
2.3. Exergames Using Holographic MR Headsets
2.4. Data Already Published from the Study
3. Materials and Methods
3.1. General
3.2. Procedure
3.3. Measures
3.3.1. Technology Usage Inventory
3.3.2. NASA Task Load Index
3.3.3. Immersive Tendencies Questionnaire and Presence Questionnaire
3.4. Materials
3.4.1. VITALab.Mobile
3.4.2. Equipment
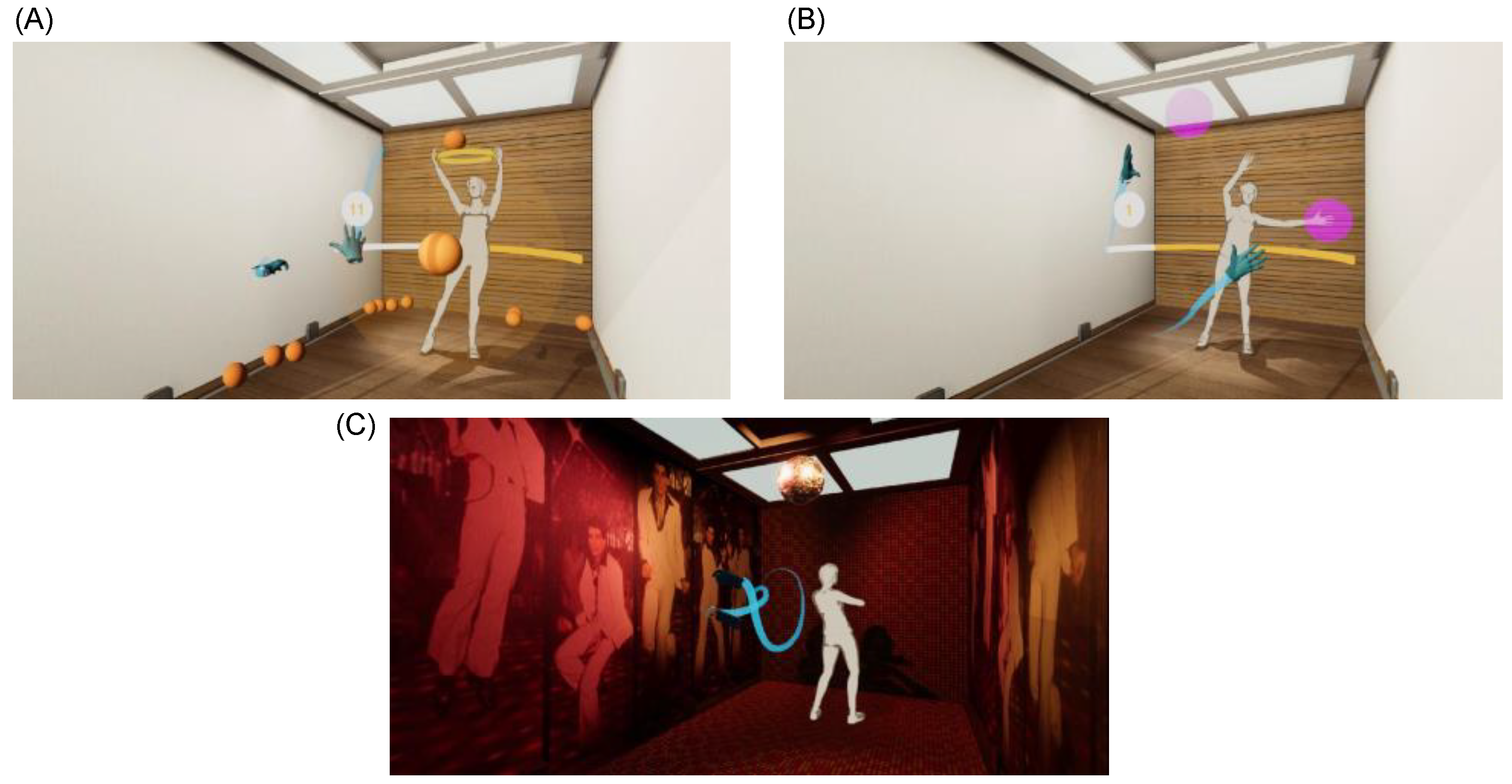
3.4.3. SET Exergame
3.4.4. ET Exergame
3.5. Participants
3.6. Statistical Analysis
4. Results
4.1. Technology Usage Inventory
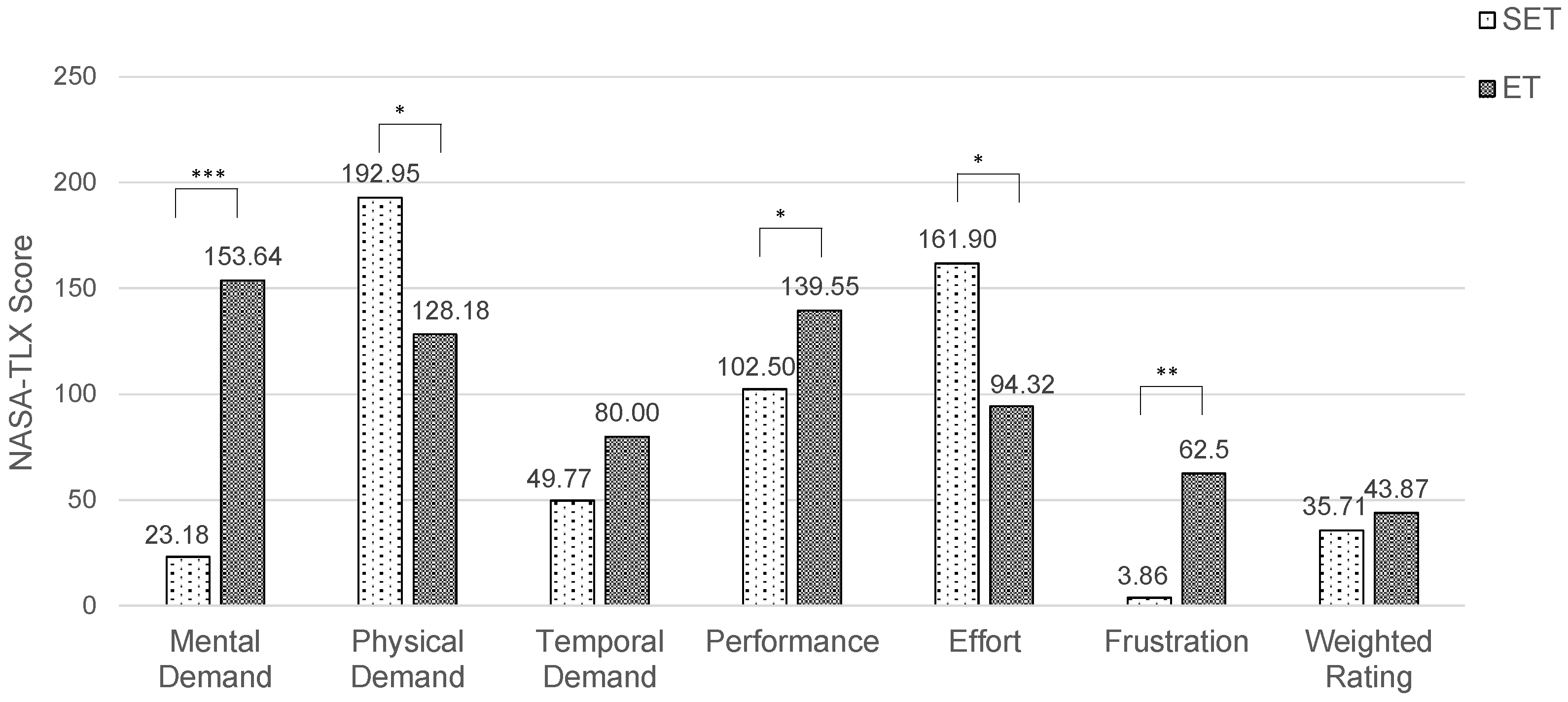
4.2. NASA-TLX
4.3. Immersive Tendencies Questionnaire
4.4. Presence Questionnaire
5. Discussion
5.1. Principal Findings
5.2. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Neuhauser, H.; Kuhnert, R.; Born, S. 12-Monats-Prävalenz von Bluthochdruck in Deutschland. J. Health Monit. 2017, 2, 57–63. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the Management of Arterial Hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef]
- Duque, E.; Fonseca, G.; Vieira, H.; Gontijo, G.; Ishitani, L. A Systematic Literature Review on User Centered Design and Participatory Design with Older People. In Proceedings of the 18th Brazilian Symposium on Human Factors in Computing Systems, Vitoria, ES, Brazil, 22–25 October 2019; Association for Computing Machinery: New York, NY, USA, 2019; pp. 1–11. [Google Scholar]
- Stamm, O.; Vorwerg, S.; Müller-Werdan, U. Exergames in Augmented Reality for Older Adults with Hypertension: A Qualitative Study Exploring User Requirements. In Proceedings of the Human Aspects of IT for the Aged Population. Social Media, Games and Assistive Environments, Orlando, FL, USA, 26–31 July 2019; Zhou, J., Salvendy, G., Eds.; Springer International Publishing: Cham, Switzerland, 2019; pp. 232–244. [Google Scholar]
- Vorwerg, S.; Stamm, O.; Müller-Werdan, U. Movement Training in Augmented Reality for Older Adults with Essential Hypertension: A Qualitative Study Determining Training Requirements. Games Health J. 2020, 9, 436–445. [Google Scholar] [CrossRef]
- Milgram, P.; Kishino, F. A Taxonomy of Mixed Reality Visual Displays. IEICE Trans. Inf. Syst. 1994, 77, 1321–1329. [Google Scholar]
- Skarbez, R.; Smith, M.; Whitton, M.C. Revisiting Milgram and Kishino’s Reality-Virtuality Continuum. Front. Virtual Real. 2021, 2, 647997. [Google Scholar] [CrossRef]
- Speicher, M.; Hall, B.D.; Nebeling, M. What Is Mixed Reality? In Proceedings of the 2019 CHI Conference on Human Factors in Computing Systems, Glasgow, UK, 4–9 May 2019; Association for Computing Machinery: New York, NY, USA, 2019; pp. 1–15. [Google Scholar]
- Yue, Y.-T.; Yang, Y.-L.; Ren, G.; Wang, W. SceneCtrl: Mixed Reality Enhancement via Efficient Scene Editing. In Proceedings of the 30th Annual ACM Symposium on User Interface Software and Technology, Québec City, QC, Canada, 22–25 October 2022; Association for Computing Machinery: New York, NY, USA, 2017; pp. 427–436. [Google Scholar]
- Davis, F.D. A Technology Acceptance Model for Empirically Testing New End-User Information Systems: Theory and Results. Ph.D. Thesis, Massachusetts Institute of Technology, Cambridge, MA, USA, 1985. [Google Scholar]
- Fishbein, M.; Ajzen, I. Belief, Attitude, Intention and Behavior: An Introduction to Theory and Research; Longman Higher Education: Reading, MA, USA, 1975; ISBN 978-0-201-02089-2. [Google Scholar]
- Davis, F.D.; Bagozzi, R.P.; Warshaw, P.R. User Acceptance of Computer Technology: A Comparison of Two Theoretical Models. Manag. Sci. 1989, 35, 982–1003. [Google Scholar] [CrossRef]
- Lai, P.C. The literature review of technology adoption models and theories for the novelty technology. J. Inf. Syst. Technol. Manag. 2017, 14, 21–38. [Google Scholar] [CrossRef]
- Venkatesh, V.; Morris, M.G.; Davis, G.B.; Davis, F.D. User Acceptance of Information Technology: Toward a Unified View. MIS Q. 2003, 27, 425–478. [Google Scholar] [CrossRef]
- Cechetti, N.P.; Bellei, E.A.; Biduski, D.; Rodriguez, J.P.M.; Roman, M.K.; De Marchi, A.C.B. Developing and Implementing a Gamification Method to Improve User Engagement: A Case Study with an m-Health Application for Hypertension Monitoring. Telemat. Inform. 2019, 41, 126–138. [Google Scholar] [CrossRef]
- Kothgassner, O.; Felnhofer, A.; Hauk, N. TUI Technology Usage Inventory Manual. Available online: https://www.ffg.at/sites/default/files/allgemeine_downloads/thematische%20programme/programmdokumente/tui_manual.pdf (accessed on 19 March 2021).
- Longo, L. Experienced Mental Workload, Perception of Usability, Their Interaction and Impact on Task Performance. PLoS ONE 2018, 13, e0199661. [Google Scholar] [CrossRef]
- Miller, K.J.; Adair, B.S.; Pearce, A.J.; Said, C.M.; Ozanne, E.; Morris, M.M. Effectiveness and Feasibility of Virtual Reality and Gaming System Use at Home by Older Adults for Enabling Physical Activity to Improve Health-Related Domains: A Systematic Review. Age Ageing 2014, 43, 188–195. [Google Scholar] [CrossRef]
- Tuena, C.; Pedroli, E.; Trimarchi, P.D.; Gallucci, A.; Chiappini, M.; Goulene, K.; Gaggioli, A.; Riva, G.; Lattanzio, F.; Giunco, F.; et al. Usability Issues of Clinical and Research Applications of Virtual Reality in Older People: A Systematic Review. Front. Hum. Neurosci. 2020, 14, 93. [Google Scholar] [CrossRef]
- Huygelier, H.; Schraepen, B.; van Ee, R.; Vanden Abeele, V.; Gillebert, C.R. Acceptance of Immersive Head-Mounted Virtual Reality in Older Adults. Sci. Rep. 2019, 9, 4519. [Google Scholar] [CrossRef]
- Cotten, S.R.; Yost, E.A.; Berkowsky, R.W.; Winstead, V.; Anderson, W.A. Designing Technology Training for Older Adults in Continuing Care Retirement Communities; CRC Press: Boca Raton, FL, USA, 2016; ISBN 978-1-315-38246-3. [Google Scholar]
- Mitzner, T.L.; Savla, J.; Boot, W.R.; Sharit, J.; Charness, N.; Czaja, S.J.; Rogers, W.A. Technology Adoption by Older Adults: Findings From the PRISM Trial. Gerontologist 2019, 59, 34–44. [Google Scholar] [CrossRef]
- Seifert, A.; Schlomann, A. The Use of Virtual and Augmented Reality by Older Adults: Potentials and Challenges. Front. Virtual Real. 2021, 2, 639718. [Google Scholar] [CrossRef]
- Kivelä, O.; Alavesa, P.; Visuri, A.; Ojala, T. Study on the Motivational and Physical Effects of Two VR Exergames. In Proceedings of the 2019 11th International Conference on Virtual Worlds and Games for Serious Applications (VS-Games), Vienna, Austria, 4–6 September 2019; pp. 1–2. [Google Scholar]
- Mishra, N.; Folmer, E. Measuring Physical Exertion in Virtual Reality Exercise Games. In Proceedings of the 24th ACM Symposium on Virtual Reality Software and Technology, New York, NY, USA, 28 November 2018; Association for Computing Machinery: New York, NY, USA, 2018; pp. 1–2. [Google Scholar]
- McDonough, D.J.; Pope, Z.C.; Zeng, N.; Liu, W.; Gao, Z. Comparison of College Students’ Blood Pressure, Perceived Exertion, and Psychosocial Outcomes During Virtual Reality, Exergaming, and Traditional Exercise: An Exploratory Study. Games Health J. 2020, 9, 290–296. [Google Scholar] [CrossRef]
- Colombo, V.; Mondellini, M.; Gandolfo, A.; Fumagalli, A.; Sacco, M. Usability and Acceptability of a Virtual Reality-Based System for Endurance Training in Elderly with Chronic Respiratory Diseases. In Proceedings of the Virtual Reality and Augmented Reality, Tallinn, Estonia, 23–25 October 2019; Bourdot, P., Interrante, V., Nedel, L., Magnenat-Thalmann, N., Zachmann, G., Eds.; Springer International Publishing: Cham, Switzerland, 2019; pp. 87–96. [Google Scholar]
- Karaosmanoglu, S.; Kruse, L.; Rings, S.; Steinicke, F. Canoe VR: An Immersive Exergame to Support Cognitive and Physical Exercises of Older Adults. In Proceedings of the Extended Abstracts of the 2022 CHI Conference on Human Factors in Computing Systems, New Orleans, LA, USA, 29 April–5 May 2022; Association for Computing Machinery: New York, NY, USA, 2022; pp. 1–7. [Google Scholar]
- Høeg, E.R.; Bruun-Pedersen, J.R.; Serafin, S. Virtual Reality-Based High-Intensity Interval Training For Pulmonary Rehabilitation: A Feasibility and Acceptability Study. In Proceedings of the 2021 IEEE Conference on Virtual Reality and 3D User Interfaces Abstracts and Workshops (VRW), Lisbon, Portuga, 27 March–1 April 2021; pp. 242–249. [Google Scholar]
- Shabbir, S.A.; Malwade, S.; Nursetyo, A.A.; Sood, M.; Bhatia, M.; Barsasella, D.; Liu, M.; Chang, C.-C.; Srinivasan, K.; Li, Y.C.; et al. Virtual Reality among the Elderly: A Usefulness and Acceptance Study from Taiwan. BMC Geriatr. 2019, 19, 223. [Google Scholar] [CrossRef]
- Chau, P.; Kwok, J.Y.Y.; Chan, M.; Kwan, K.; Wong, K.; Tang, Y.; Chau, K.; Lau, S.; Yiu, Y.; Kwong, M.; et al. Feasibility, Acceptability, and Efficacy of Virtual Reality Training for Older Adults and People with Disabilities: A Single-Armed Pretest–Posttest Design Study (Preprint). J. Med. Internet Res. 2021, 23, 27640. [Google Scholar] [CrossRef]
- Kruse, L.; Karaosmanoglu, S.; Rings, S.; Ellinger, B.; Steinicke, F. Enabling Immersive Exercise Activities for Older Adults: A Comparison of Virtual Reality Exergames and Traditional Video Exercises. Societies 2021, 11, 134. [Google Scholar] [CrossRef]
- Kunze, K.; Minamizawa, K.; Lukosch, S.; Inami, M.; Rekimoto, J. Superhuman Sports: Applying Human Augmentation to Physical Exercise. IEEE Pervasive Comput. 2017, 16, 14–17. [Google Scholar] [CrossRef]
- Kegeleers, M.; Miglani, S.; Reichert, G.M.W.; Salamon, N.Z.; Balint, J.T.; Lukosch, S.G.; Bidarra, R. STAR: Superhuman Training in Augmented Reality. In Proceedings of the First Superhuman Sports Design Challenge: First International Symposium on Amplifying Capabilities and Competing in Mixed Realities, New York, NY, USA, 2 July 2018; Association for Computing Machinery: New York, NY, USA, 2018; pp. 1–6. [Google Scholar]
- Miedema, N.A.; Vermeer, J.; Lukosch, S.; Bidarra, R. Superhuman Sports in Mixed Reality: The Multi-Player Game League of Lasers. In Proceedings of the 2019 IEEE Conference on Virtual Reality and 3D User Interfaces (VR), Osaka, Japan, 23–27 March 2019; pp. 1819–1825. [Google Scholar]
- Buckers, T.; Gong, B.; Eisemann, E.; Lukosch, S. VRabl: Stimulating Physical Activities through a Multiplayer Augmented Reality Sports Game. In Proceedings of the First Superhuman Sports Design Challenge: First International Symposium on Amplifying Capabilities and Competing in Mixed Realities, New York, NY, USA, 2 July 2018; Association for Computing Machinery: New York, NY, USA, 2018; pp. 1–5. [Google Scholar]
- Franzo, M.; Pascucci, S.; Serrao, M.; Marinozzi, F.; Bini, F. Exergaming in Mixed Reality for the Rehabilitation of Ataxic Patients. In Proceedings of the 2022 IEEE International Symposium on Medical Measurements and Applications (MeMeA), Messina, Italy, 22–24 June 2022; pp. 1–5. [Google Scholar]
- Vorwerg, S.; Stamm, O.; Haink, M. Virtual Reality Exergame in Older Patients with Hypertension: A Preliminary Study to Determine Load Intensity and Blood Pressure; PREPRINT (Version 1) Available at Research Square; 2022. Available online: https://www.researchsquare.com/article/rs-1284291/v1 (accessed on 10 October 2022).
- Stamm, O.; Vorwerg, S. Virtual Reality Sickness Evaluation in Exergames for Older Hypertensive Patients: A Comparative Study of Training Methods in a Virtual Environment. In Virtual, Augmented and Mixed Reality; Chen, J.Y.C., Fragomeni, G., Eds.; Lecture Notes in Computer Science; Springer International Publishing: Cham, Switzerland, 2021; Volume 12770, pp. 134–146. ISBN 978-3-030-77598-8. [Google Scholar]
- Kennedy, R.S.; Lane, N.E.; Berbaum, K.S.; Lilienthal, M.G. Simulator Sickness Questionnaire: An Enhanced Method for Quantifying Simulator Sickness. Int. J. Aviat. Psychol. 1993, 3, 203–220. [Google Scholar] [CrossRef]
- Buchem, I.; Vorwerg, S.; Stamm, O.; Hildebrand, K.; Bialek, Y. Gamification in Mixed-Reality Exergames for Older Adult Patients in a Mobile Immersive Diagnostic Center: A Pilot Study in the BewARe Project. In Proceedings of the 2021 7th International Conference of the Immersive Learning Research Network (iLRN), Eureka, CA, USA, 17 May–10 June 2021; pp. 1–8. [Google Scholar]
- Laugwitz, B.; Held, T.; Schrepp, M. Construction and Evaluation of a User Experience Questionnaire. In Proceedings of the HCI and Usability for Education and Work, Graz, Austria, 20–21 November 2008; Holzinger, A., Ed.; Springer: Berlin/Heidelberg, Germany, 2008; pp. 63–76. [Google Scholar]
- Buchem, I.; Vorwerg, S.; Stamm, O.; Kruschel, K. Designing for Rapport with Virtual Agents in a Simulated Mixed Reality Environment: Results from a Pilot Study with Senior Users in the BewARe Project. In Proceedings of the Advances in Usability, User Experience, Wearable and Assistive Technology, Virtual, 25–29 July 2021; Ahram, T.Z., Falcão, C.S., Eds.; Springer International Publishing: Cham, Switzerland, 2021; pp. 140–148. [Google Scholar]
- Ascora GmbH. BewARe-Sensor-Supported Movement Training for Seniors in an Intelligent Augmented Reality System. Available online: https://www.beware-projekt.de/en/index.html (accessed on 10 October 2022).
- Tinetti, M.E.; Williams, T.F.; Mayewski, R. Fall Risk Index for Elderly Patients Based on Number of Chronic Disabilities. Am. J. Med. 1986, 80, 429–434. [Google Scholar] [CrossRef]
- Brandt, J.; Spencer, M.; Folstein, M. The Telephone Interview for Cognitive Status. Cogn. Behav. Neurol. 1988, 1, 111–118. [Google Scholar]
- Witmer, B.G.; Singer, M.J. Measuring Presence in Virtual Environments: A Presence Questionnaire. Presence 1998, 7, 225–240. [Google Scholar] [CrossRef]
- Hart, S.G.; Staveland, L.E. Development of NASA-TLX (Task Load Index): Results of Empirical and Theoretical Research. In Advances in Psychology; Elsevier: Amsterdam, The Netherlands, 1988; Volume 52, pp. 139–183. ISBN 978-0-444-70388-0. [Google Scholar]
- Flägel, K.; Galler, B.; Steinhäuser, J.; Götz, K. The “National Aeronautics and Space Administration-Task Load Index” (NASA-TLX)—An Instrument for Measuring Consultation Workload within General Practice: Evaluation of Psychometric Properties. ZEFQ 2019, 147, 90–96. [Google Scholar] [CrossRef]
- Schmelter, T.; Rings, S.; Prasuhn, C.; Villwock, J.; Steinicke, F.; Hildebrand, K. VITALab.Mobile—A Mobile Living Lab. In Proceedings of the Mensch und Computer 2019, Hamburg, Germany, 8–11 September 2019; Association for Computing Machinery: New York, NY, USA, 2019; pp. 917–920. [Google Scholar]
- Fang, Y.-M.; Huang, Y.-J. Comparison of the Usability and Flow Experience of an Exercise Promotion Virtual Reality Programme for Different Age Groups. Behav. Inf. Technol. 2021, 40, 1250–1264. [Google Scholar] [CrossRef]
- Xu, W.; Liang, H.-N.; Yu, K.; Wen, S.; Baghaei, N.; Tu, H. Acceptance of Virtual Reality Exergames among Chinese Older Adults. Int. J. Hum.–Comput. Interact. 2022, 1–15. [Google Scholar] [CrossRef]
- Khundam, C.; Noël, F. A Study of Physical Fitness and Enjoyment on Virtual Running for Exergames. Int. J. Comput. Games Technol. 2021, 2021, 6668280. [Google Scholar] [CrossRef]
- Weech, S.; Kenny, S.; Barnett-Cowan, M. Presence and Cybersickness in Virtual Reality Are Negatively Related: A Review. Front. Psychol. 2019, 10, 158. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| TUI | Training | Mean (SD) | Median (95% CI) | Z-Score | p-Value |
|---|---|---|---|---|---|
| Interest | SET | 16.50 (5.48) | 17.00 (14.07–18.93) | −0.035 | 0.972 |
| ET | 16.59 (5.78) | 19.00 (14.03–19.15) | |||
| Usability | SET | 16.55 (3.49) | 17.00 (15.00–18.09) | −0.445 | 0.656 |
| ET | 16.29 (3.81) | 18.00 (14.55–18.02) | |||
| Immersion | SET | 16.68 (5.41) | 17.00 (14.28–19.08) | −0.141 | 0.888 |
| ET | 16.86 (5.06) | 16.00 (14.62–19.10) | |||
| Usefulness | SET | 13.55 (6.11) | 13.00 (10.83–16.26) | −0.358 | 0.720 |
| ET | 13.82 (4.49) | 14.00 (11.83–15.81) | |||
| Skepticism | SET | 10.18 (5.23) | 10.00 (7.87–12.50) | −1.196 | 0.232 |
| ET | 11.67 (4.95) | 13.00 (9.41–13.92) | |||
| Accessibility | SET | 10.18 (4.03) | 10.00 (8.39–11.97) | −1.734 | 0.083 |
| ET | 11.77(3.61) | 12.00 (10.17–13.37) | |||
| Intention to Use | SET | 134.00 (78.30) | 147.00 (99.29–168.71) | −0.261 | 0.794 |
| ET | 140.68 (86.99) | 132.00 (102.11–179.25) |
| ITQ | Sample | Mean (SD) | p-Value | Cohen’s d |
|---|---|---|---|---|
| Focus | Pre VR | 25.55 (3.97) | 0.395 | 0.185 |
| Reference 1 | 24.81 (7.54) | |||
| Involvement | Pre VR | 15.41 (4.96) | 0.941 | 0.016 |
| Reference 1 | 15.33 (8.67) | |||
| Emotions | Pre VR | 12.77 (3.73) | 0.077 | 0.396 |
| Reference 1 | 14.25 (6.70) | |||
| Game | Pre VR | 6.64 (2.87) | 0.902 | 0.027 |
| Reference 1 | 6.56 (4.95) | |||
| Total Score | Pre VR | 65.59 (10.75) | 0.525 | 0.138 |
| Reference 1 | 64.11 (13.11) |
| PQ | Training | Mean (SD) | Median (95% CI) | Z-Score | p-Value |
|---|---|---|---|---|---|
| Realism | SET | 40.09 (6.29) | 41.00 (37.30–42.88) | −2.667 | 0.008 |
| ET | 37.00 (7.25) | 39.00 (33.79–40.21) | |||
| Possibility to Act | SET | 22.18 (3.88) | 22.00 (20.46–23.90) | −3.213 | 0.001 |
| ET | 18.77 (4.81) | 20.00 (16.64–20.91) | |||
| Quality of Interface | SET | 14.59 (3.42) | 15.00 (13.08–16.11) | −1.049 | 0.294 |
| ET | 13.86 (3.36) | 13.00 (12.38–15.35) | |||
| Possibility to Examine | SET | 16.55 (3.08) | 17.00 (15.18–17.91) | −1.858 | 0.063 |
| ET | 15.41 (3.40) | 16.00 (13.90–16.92) | |||
| Self-Evaluation of Performance | SET | 11.77 (1.57) | 12.00 (11.08–12.47) | −1.998 | 0.046 |
| ET | 10.82 (2.46) | 11.00 (9.73–11.91) | |||
| Sounds | SET | 17.05 (3.51) | 18.00 (15.49–18.60) | −0.400 | 0.689 |
| ET | 16.91 (3.80) | 18.00 (15.22–18.60) | |||
| Haptic | SET | 11.73 (2.27) | 12.00 (10.72–12.73) | −3.336 | <0.001 |
| ET | 10.05 (2.59) | 11.00 (8.90–11.19) | |||
| Total 1 | SET | 112.59 (12.82) | 117 (106.91–118.27) | −3.114 | 0.002 |
| ET | 104.00 (15.83) | 107 (96.98–111.02) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stamm, O.; Vorwerg, S.; Haink, M.; Hildebrand, K.; Buchem, I. Usability and Acceptance of Exergames Using Different Types of Training among Older Hypertensive Patients in a Simulated Mixed Reality. Appl. Sci. 2022, 12, 11424. https://doi.org/10.3390/app122211424
Stamm O, Vorwerg S, Haink M, Hildebrand K, Buchem I. Usability and Acceptance of Exergames Using Different Types of Training among Older Hypertensive Patients in a Simulated Mixed Reality. Applied Sciences. 2022; 12(22):11424. https://doi.org/10.3390/app122211424
Chicago/Turabian StyleStamm, Oskar, Susan Vorwerg, Michele Haink, Kristian Hildebrand, and Ilona Buchem. 2022. "Usability and Acceptance of Exergames Using Different Types of Training among Older Hypertensive Patients in a Simulated Mixed Reality" Applied Sciences 12, no. 22: 11424. https://doi.org/10.3390/app122211424
APA StyleStamm, O., Vorwerg, S., Haink, M., Hildebrand, K., & Buchem, I. (2022). Usability and Acceptance of Exergames Using Different Types of Training among Older Hypertensive Patients in a Simulated Mixed Reality. Applied Sciences, 12(22), 11424. https://doi.org/10.3390/app122211424