
Development of an Artificial 3D Liver Phantom for Analysis of Radiotherapeutic Effects In Vitro

 , ,
, , 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
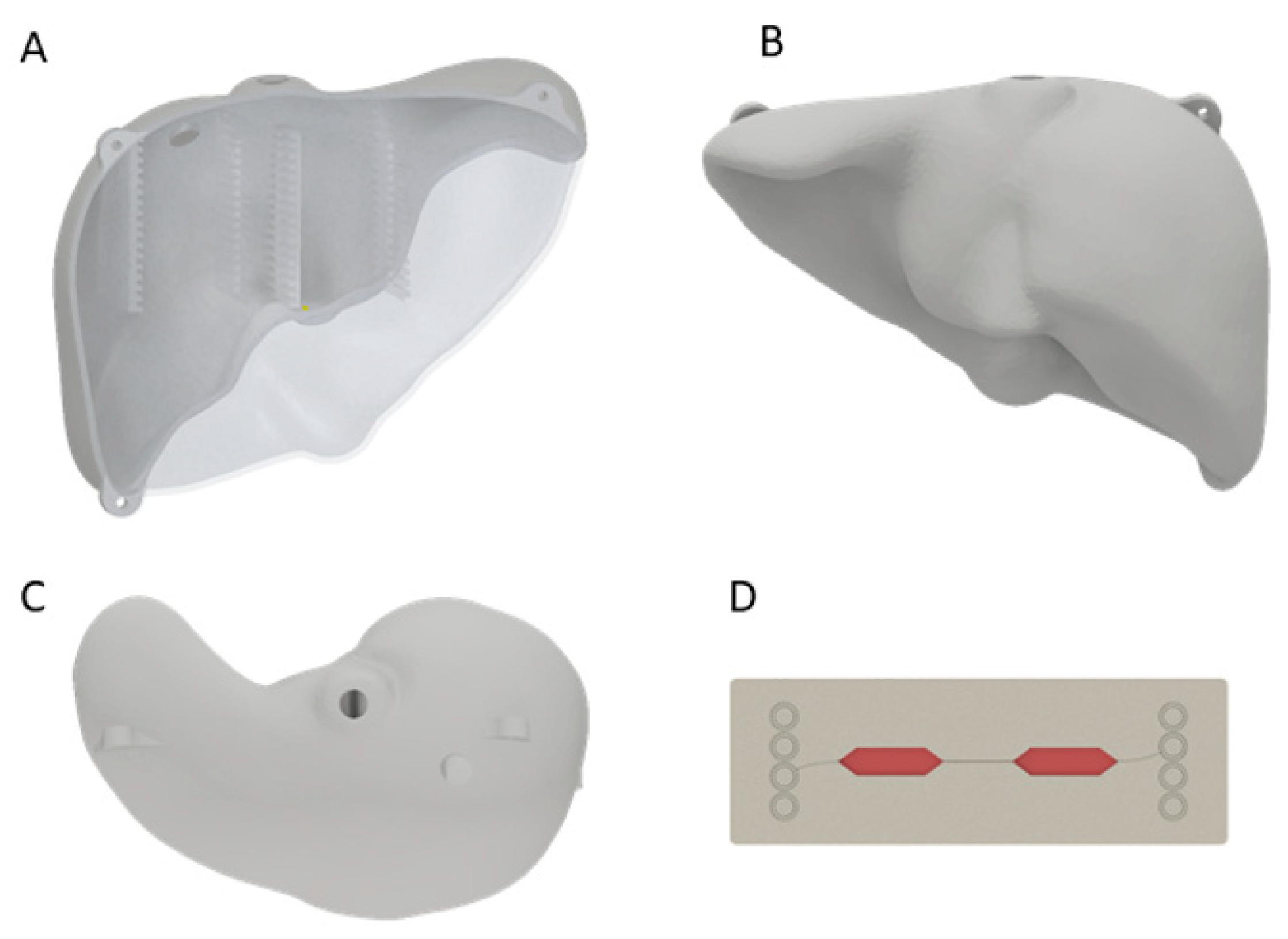
2.1. Three-Dimensional-Printed Liver Model
2.2. Treatment Planning for Liver Model
2.3. HepG2 Cell Cultivation
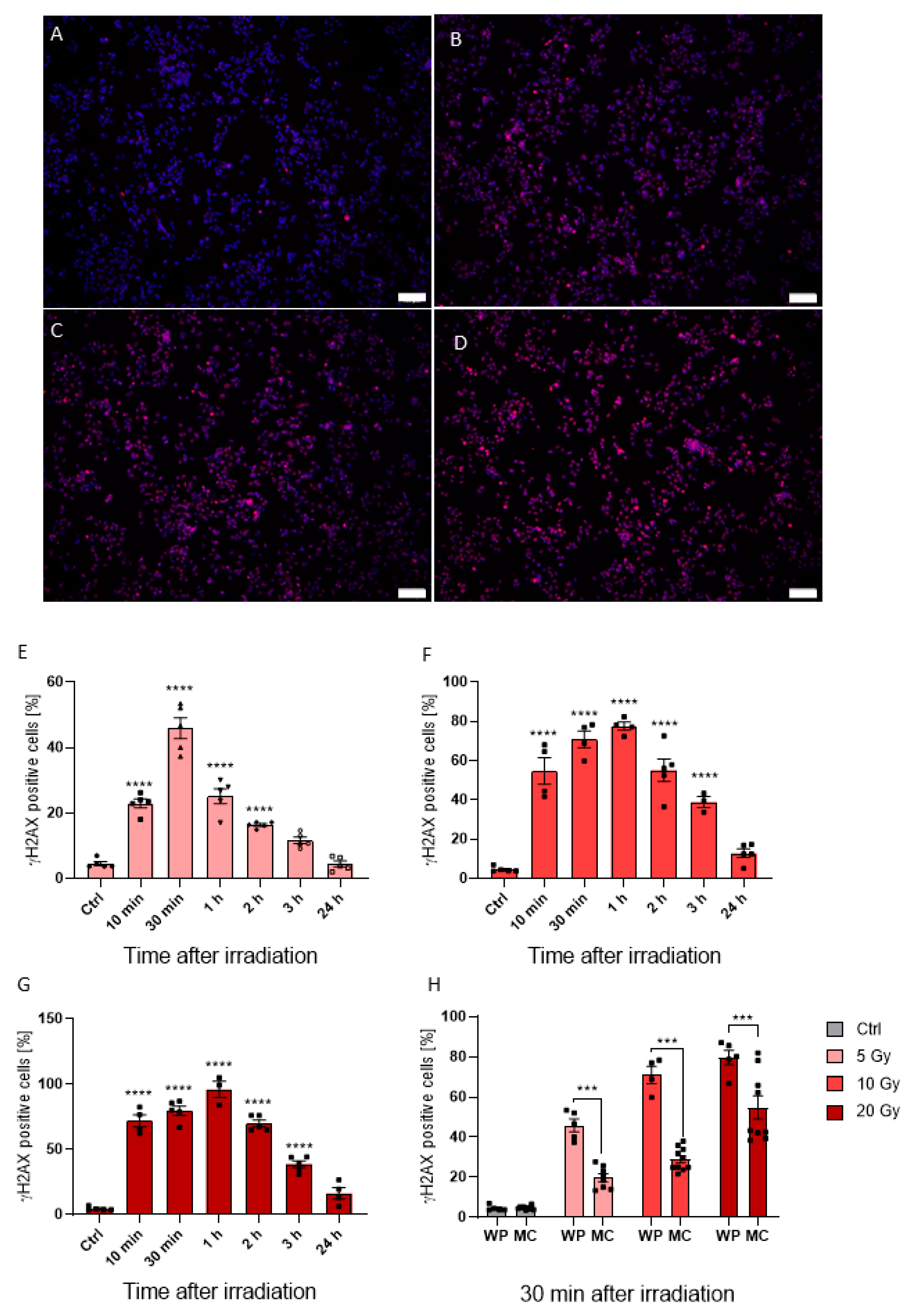
2.4. Dose-Dependent Irradiation of HepG2 Cells
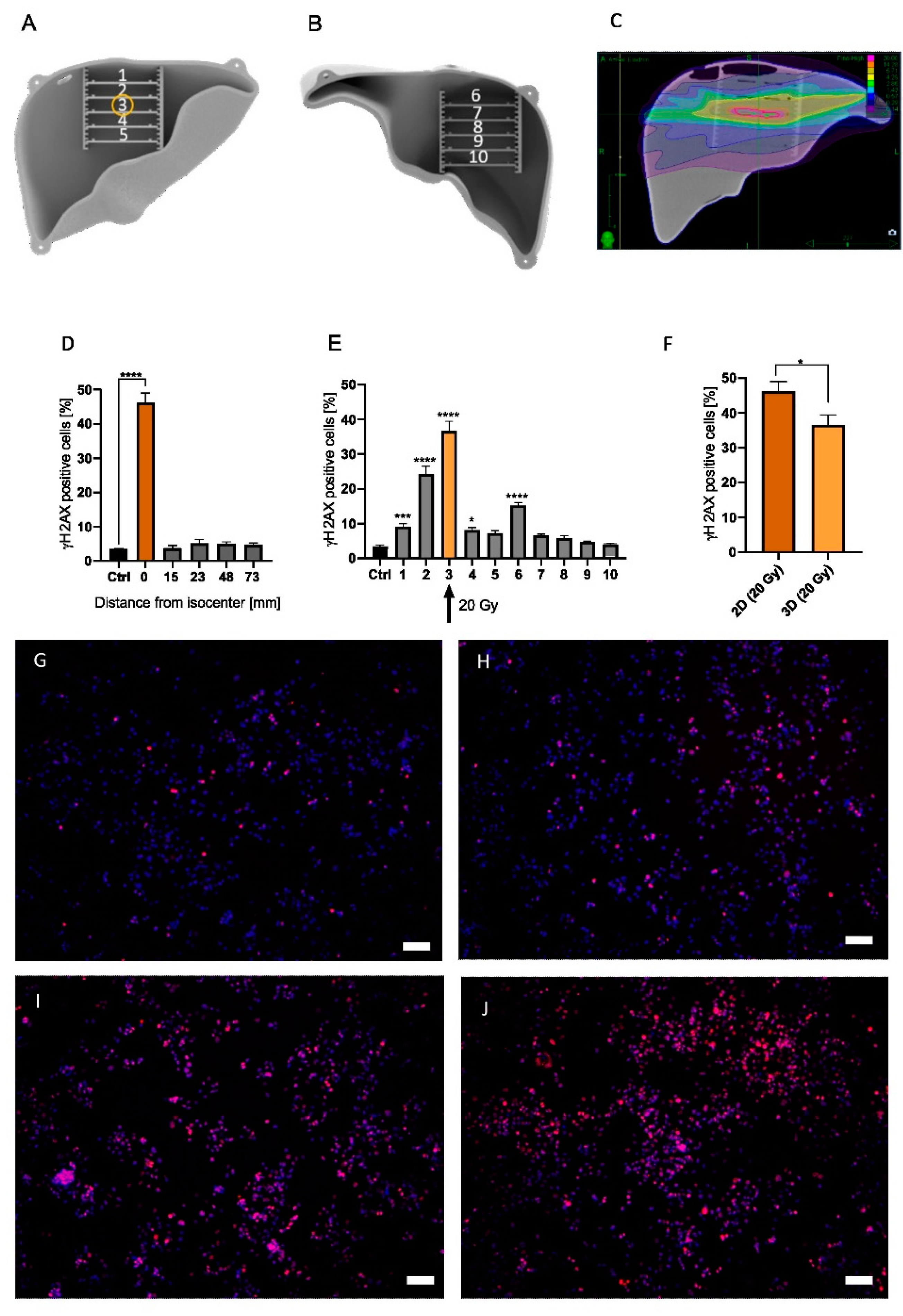
2.5. 2D and 3D In Vitro Irradiation
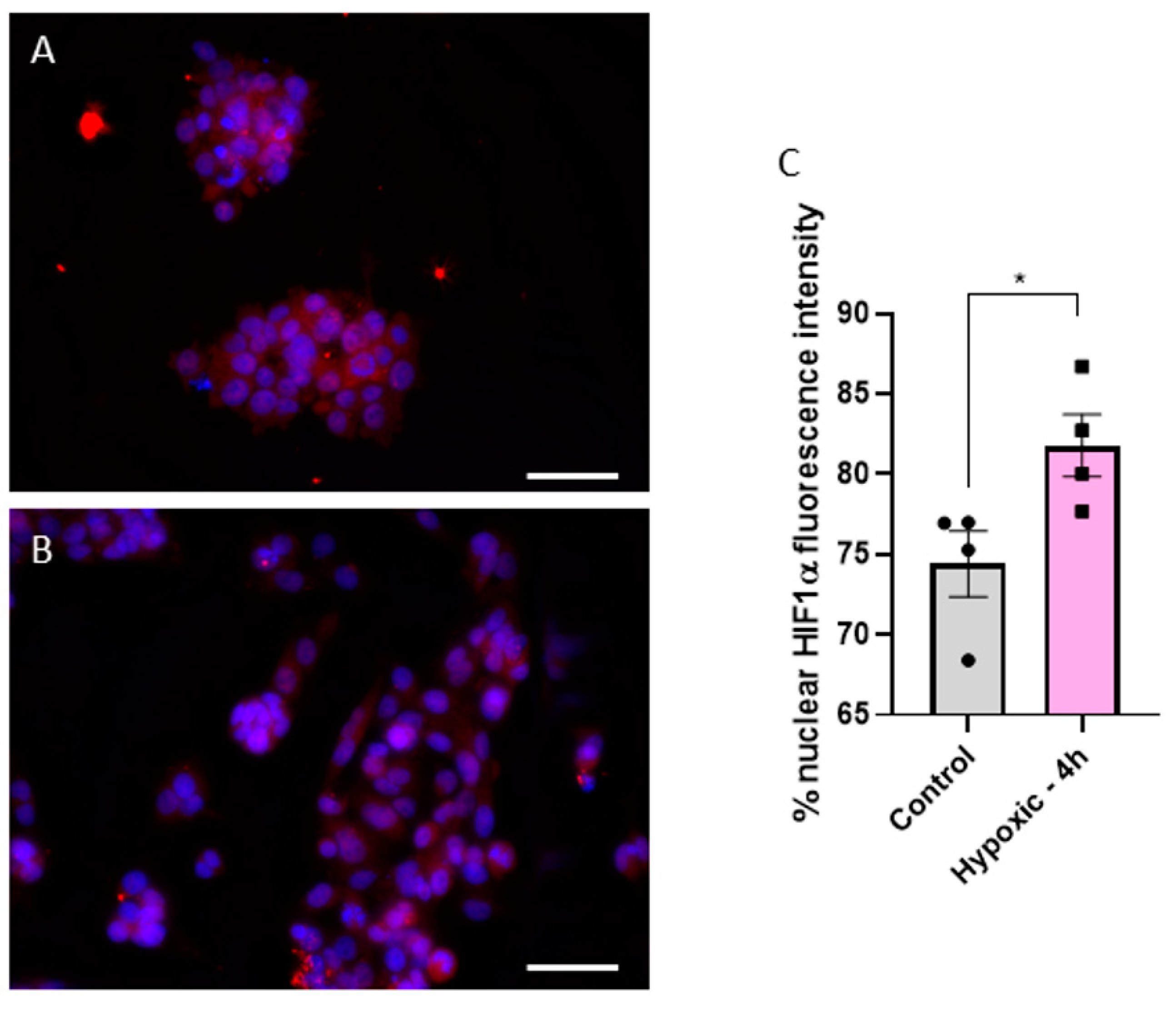
2.6. Validation of Hypoxic Condition
2.7. Immunofluorescence Staining
2.8. Image and Statistical Analysis
3. Results
3.1. Microfluidic Chips Successfully Simulate the Hypoxic Condition of a Solid Tumor
3.2. In Vitro Response to Photon Irradiation in Normoxic and Hypoxic Conditions
3.3. Analysis of 2D and 3D Radiotherapy on HepG2 Cells
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Guo, Y.; Xiao, Z.; Yang, L.; Gao, Y.; Zhu, Q.; Hu, L.; Huang, D.; Xu, Q. Hypoxia-inducible factors in hepatocellular carcinoma (Review). Oncol. Rep. 2020, 43, 3–15. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.-A.; Chang, L.-L.; Zhu, H.; He, Q.-J.; Yang, B. Hypoxic microenvironment and hepatocellular carcinoma treatment. Hepatoma Res. 2018, 4, 26. [Google Scholar] [CrossRef]
- Galle, P.R.; Forner, A.; Llovet, J.M.; Mazzaferro, V.; Piscaglia, F.; Raoul, J.-L.; Schirmacher, P.; Vilgrain, V. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [PubMed]
- Benson, A.B.; D’Angelica, M.I.; Abbott, D.E.; Abrams, T.A.; Alberts, S.R.; Saenz, D.A.; Are, C.; Brown, D.B.; Chang, D.T.; Covey, A.M.; et al. NCCN Guidelines Insights: Hepatobiliary Cancers, Version 1.2017. J. Natl. Compr. Canc. Netw. 2017, 15, 563–573. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Yoon, W.S.; Rim, C.H. Indications of external radiotherapy for hepatocellular carcinoma from updated clinical guidelines: Diverse global viewpoints. World J. Gastroenterol. 2020, 26, 393–403. [Google Scholar] [CrossRef] [PubMed]
- Shanker, M.D.; Liu, H.Y.; Lee, Y.Y.; Stuart, K.A.; Powell, E.E.; Wigg, A.; Pryor, D.I. Stereotactic radiotherapy for hepatocellular carcinoma: Expanding the multidisciplinary armamentarium. J. Gastroenterol. Hepatol. 2020, 36, 873–884. [Google Scholar] [CrossRef] [PubMed]
- Kuwahara, Y.; Li, L.; Baba, T.; Nakagawa, H.; Shimura, T.; Yamamoto, Y.; Ohkubo, Y.; Fukumoto, M. Clinically relevant radioresistant cells efficiently repair DNA double-strand breaks induced by X-rays. Cancer Sci. 2009, 100, 747–752. [Google Scholar] [CrossRef]
- Tesei, A.; Sarnelli, A.; Arienti, C.; Menghi, E.; Medri, L.; Gabucci, E.; Pignatta, S.; Falconi, M.; Silvestrini, R.; Zoli, W.; et al. In vitro irradiation system for radiobiological experiments. Radiat. Oncol. 2013, 8, 257. [Google Scholar] [CrossRef]
- Brüningk, S.C.; Rivens, I.; Box, C.; Oelfke, U.; Haar, G. ter. 3D tumour spheroids for the prediction of the effects of radiation and hyperthermia treatments. Sci. Rep. 2020, 10, 1653. [Google Scholar] [CrossRef] [PubMed]
- Ding, C.; Saw, C.B.; Timmerman, R.D. Cyberknife stereotactic radiosurgery and radiation therapy treatment planning system. Med. Dosim. 2018, 43, 129–140. [Google Scholar] [CrossRef] [PubMed]
- Theobald, J.; Ghanem, A.; Wallisch, P.; Banaeiyan, A.A.; Andrade-Navarro, M.A.; Taškova, K.; Haltmeier, M.; Kurtz, A.; Becker, H.; Reuter, S.; et al. Liver-Kidney-on-Chip To Study Toxicity of Drug Metabolites. ACS Biomater. Sci. Eng. 2018, 4, 78–89. [Google Scholar] [CrossRef] [PubMed]
- Chilov, D.; Camenisch, G.; Kvietikova, I.; Ziegler, U.; Gassmann, M.; Wenger, R.H. Induction and Nuclear Translocation of Hypoxia-Inducible Factor-1 (HIF-1): Heterodimerization with ARNT Is Not Necessary for Nuclear Accumulation of HIF-1alpha. Available online: https://www.zora.uzh.ch/id/eprint/66/ (accessed on 24 November 2021).
- Niebuhr, N.I.; Johnen, W.; Echner, G.; Runz, A.; Bach, M.; Stoll, M.; Giske, K.; Greilich, S.; Pfaffenberger, A. The ADAM-pelvis phantom-an anthropomorphic, deformable and multimodal phantom for MRgRT. Phys. Med. Biol. 2019, 64, 04NT05. [Google Scholar] [CrossRef] [PubMed]
- Aranda-Lara, L.; Torres-García, E.; Oros-Pantoja, R. Biological Tissue Modeling with Agar Gel Phantom for Radiation Dosimetry of 99mTc. Open J. Radiol. 2014, 04, 44–52. [Google Scholar] [CrossRef][Green Version]
- Singhrao, K.; Fu, J.; Wu, H.H.; Hu, P.; Kishan, A.U.; Chin, R.K.; Lewis, J.H. A novel anthropomorphic multimodality phantom for MRI-based radiotherapy quality assurance testing. Med. Phys. 2020, 47, 1443–1451. [Google Scholar] [CrossRef] [PubMed]
- Gillmann, C.; Homolka, N.; Johnen, W.; Runz, A.; Echner, G.; Pfaffenberger, A.; Mann, P.; Schneider, V.; Hoffmann, A.L.; Troost, E.G.C.; et al. Technical Note: ADAM PETer—An anthropomorphic, deformable and multimodality pelvis phantom with positron emission tomography extension for radiotherapy. Med. Phys. 2021, 48, 1624–1632. [Google Scholar] [CrossRef] [PubMed]
- Arzumanian, V.A.; Kiseleva, O.I.; Poverennaya, E.V. The Curious Case of the HepG2 Cell Line: 40 Years of Expertise. Int. J. Mol. Sci. 2021, 22, 13135. [Google Scholar] [CrossRef] [PubMed]
- Nwosu, Z.C.; Battello, N.; Rothley, M.; Piorońska, W.; Sitek, B.; Ebert, M.P.; Hofmann, U.; Sleeman, J.; Wölfl, S.; Meyer, C.; et al. Liver cancer cell lines distinctly mimic the metabolic gene expression pattern of the corresponding human tumours. J. Exp. Clin. Cancer Res. 2018, 37, 211. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Zhang, Y.; Mo, F.; Patel, G.; Butterworth, K.; Shao, C.; Prise, K.M. The Roles of HIF-1α in Radiosensitivity and Radiation-Induced Bystander Effects Under Hypoxia. Front. Cell Dev. Biol. 2021, 9, 637454. [Google Scholar] [CrossRef] [PubMed]
- Chaston, T.B.; Matak, P.; Pourvali, K.; Srai, S.K.; McKie, A.T.; Sharp, P.A. Hypoxia inhibits hepcidin expression in HuH7 hepatoma cells via decreased SMAD4 signaling. Am. J. Physiol. Cell Physiol. 2011, 300, C888–C895. [Google Scholar] [CrossRef] [PubMed]
- Zhao, W.; Cong, L.; Guerrero-Sánchez, Y. Radiation effects of nuclear physics rays on hepatoma cells. Open Phys. 2019, 17, 167–176. [Google Scholar] [CrossRef]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stengl, C.; Ghafoory, S.; Weidner, A.; Murphy, B.; Wölfl, S. Development of an Artificial 3D Liver Phantom for Analysis of Radiotherapeutic Effects In Vitro. Appl. Sci. 2022, 12, 10867. https://doi.org/10.3390/app122110867
Stengl C, Ghafoory S, Weidner A, Murphy B, Wölfl S. Development of an Artificial 3D Liver Phantom for Analysis of Radiotherapeutic Effects In Vitro. Applied Sciences. 2022; 12(21):10867. https://doi.org/10.3390/app122110867
Chicago/Turabian StyleStengl, Christina, Shahrouz Ghafoory, Artur Weidner, Brennah Murphy, and Stefan Wölfl. 2022. "Development of an Artificial 3D Liver Phantom for Analysis of Radiotherapeutic Effects In Vitro" Applied Sciences 12, no. 21: 10867. https://doi.org/10.3390/app122110867
APA StyleStengl, C., Ghafoory, S., Weidner, A., Murphy, B., & Wölfl, S. (2022). Development of an Artificial 3D Liver Phantom for Analysis of Radiotherapeutic Effects In Vitro. Applied Sciences, 12(21), 10867. https://doi.org/10.3390/app122110867