
Smoking and High-Sensitivity Troponin I Levels in Young and Healthy Adults from the General Population

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
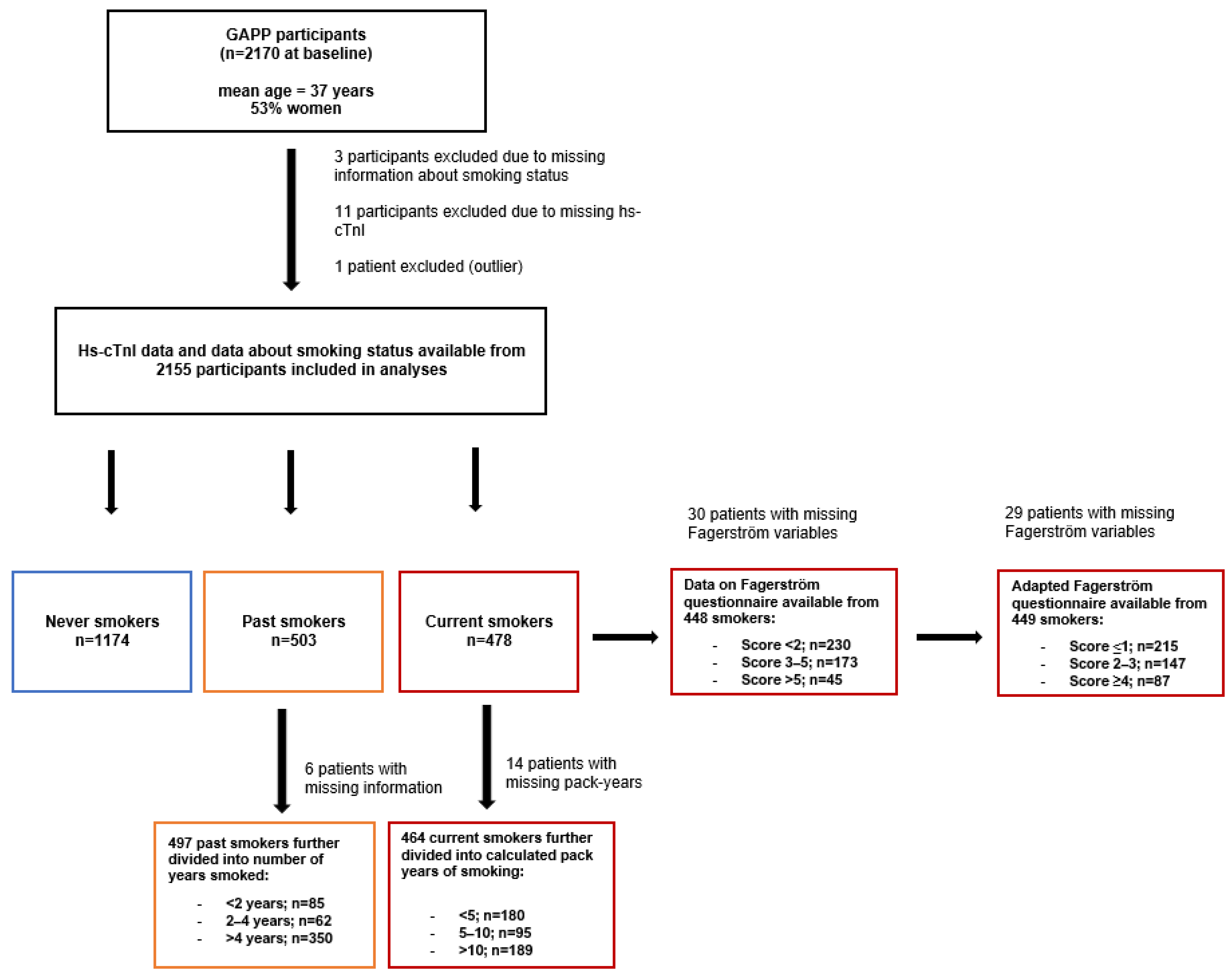
2.1. Study Participants
2.2. Assessment of Smoking
2.3. Assessment of Troponin and Other Laboratory Parameters
2.4. Assessment of Further Study Variables
2.5. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Blankenberg, S.; Salomaa, V.; Makarova, N.; Ojeda, F.; Wild, P.; Lackner, K.J.; Jørgensen, T.; Thorand, B.; Peters, A.; Nauck, M.; et al. Troponin I and cardiovascular risk prediction in the general population: The BiomarCaRE consortium. Eur. Hear. J. 2016, 37, 2428–2437. [Google Scholar] [CrossRef] [PubMed]
- van der Linden, N.; Klinkenberg, L.J.; Bekers, O.; van Loon, L.J.; van Dieijen-Visser, M.P.; Zeegers, M.; Meex, S.J. Prognostic value of basal high-sensitive cardiac troponin levels on mortality in the general population. Medicine 2016, 95, e5703. [Google Scholar] [CrossRef] [PubMed]
- Welsh, P.; Preiss, D.; Hayward, C.; Shah, A.; McAllister, D.; Briggs, A.; Boachie, C.; McConnachie, A.; Padmanabhan, S.; Welsh, C.; et al. Cardiac Troponin T and Troponin I in the General Population. Circulation 2019, 139, 2754–2764. [Google Scholar] [CrossRef] [PubMed]
- Skranes, J.B.; Claggett, B.L.; Myhre, P.L.; Lyngbakken, M.N.; Solomon, S.D.; Sabatine, M.S.; Pfeffer, M.A.; Omland, T. Current Smoking Is Associated With Lower Concentrations of High-Sensitivity Cardiac Troponin T in Patients With Stable Coronary Artery Disease: The PEACE Trial. Circulation 2019, 140, 2044–2046. [Google Scholar] [CrossRef] [PubMed]
- Nadruz, W.; Gonçalves, A.; Claggett, B.; Roca, G.Q.; Shah, A.M.; Cheng, S.; Heiss, G.; Ballantyne, C.M.; Solomon, S.D. Influence of cigarette smoking on cardiac biomarkers: The Atherosclerosis Risk in Communities (ARIC) Study. Eur. J. Hear. Fail. 2016, 18, 629–637. [Google Scholar] [CrossRef] [PubMed]
- Lyngbakken, M.N.; Skranes, J.B.; de Lemos, J.A.; Nygård, S.; Dalen, H.; Hveem, K.; Røsjø, H.; Omland, T. Impact of Smoking on Circulating Cardiac Troponin I Concentrations and Cardiovascular Events in the General Population. Circulation 2016, 134, 1962–1972. [Google Scholar] [CrossRef] [PubMed]
- Skranes, J.B.; Lyngbakken, M.N.; Hveem, K.; Røsjø, H.; Omland, T. Tobacco Consumption and High-Sensitivity Cardiac Troponin I in the General Population: The HUNT Study. J. Am. Hear. Assoc. 2022, 11, e021776. [Google Scholar] [CrossRef] [PubMed]
- Nance, R.; Delaney, J.; McEvoy, J.W.; Blaha, M.J.; Burke, G.L.; Navas-Acien, A.; Kaufman, J.D.; Oelsner, E.C.; McClelland, R.L. Smoking intensity (pack/day) is a better measure than pack-years or smoking status for modeling cardiovascular disease outcomes. J. Clin. Epidemiol. 2016, 81, 111–119. [Google Scholar] [CrossRef] [PubMed]
- Conen, D.; Schön, T.; Aeschbacher, S.; Paré, G.; Frehner, W.; Risch, M.; Risch, L. Genetic and phenotypic determinants of blood pressure and other cardiovascular risk factors (GAPP). Swiss Med. Wkly. 2013, 143, w13728. [Google Scholar] [CrossRef] [PubMed]
- Bossard, M.; Thériault, S.; Aeschbacher, S.; Schoen, T.; Kunz, S.; Von Rotz, M.; Estis, J.; Todd, J.; Risch, M.; Mueller, C.; et al. Factors independently associated with cardiac troponin I levels in young and healthy adults from the general population. Clin. Res. Cardiol. 2016, 106, 96–104. [Google Scholar] [CrossRef] [PubMed]
- Fagerstrom, K.O.; Heatherton, T.F.; Kozlowski, L.T. Nicotine addiction and its assessment. Ear Nose Throat J. 1990, 69, 763–765. [Google Scholar] [PubMed]
- Storr, C.L.; Reboussin, B.A.; Anthony, J.C. The Fagerström test for nicotine dependence: A comparison of standard scoring and latent class analysis approaches. Drug Alcohol. Depend. 2005, 80, 241–250. [Google Scholar] [CrossRef] [PubMed]
- Heatherton, T.F.; Kozlowski, L.T.; Frecker, R.C.; Fagerstrom, K.-O. The Fagerström Test for Nicotine Dependence: A revision of the Fagerstrom Tolerance Questionnaire. Br. J. Addict. 1991, 86, 1119–1127. [Google Scholar] [CrossRef] [PubMed]
- Aeschbacher, S.; Schoen, T.; Bossard, M.; van der Lely, S.; Glättli, K.; Todd, J.; Estis, J.; Risch, M.; Mueller, C.; Risch, L.; et al. Relationship Between High-Sensitivity Cardiac Troponin I and Blood Pressure Among Young and Healthy Adults. Am. J. Hypertens. 2014, 28, 789–796. [Google Scholar] [CrossRef] [PubMed]
- Todd, J.; Freese, B.; Lu, A.; Held, D.; Morey, J.; Livingston, R.; Goix, P. Ultrasensitive flow-based immunoassays using singlemolecule counting. Clin. Chem. 2007, 53, 1990–1995. [Google Scholar] [CrossRef] [PubMed]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.L.; Yngve, A.; Sallis, J.F.; et al. International Physical Activity Questionnaire: 12-Country Reliability and Validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed]
- IBM Corp. Released IBM SPSS Statistics for Windows, Version 26; IBM Corp.: Armonk, NY, USA, 2019.
- O’Donnell, M.J.; Xavier, D.; Liu, L.; Zhang, H.; Chin, S.L.; Rao-Melacini, P.; Rangarajan, S.; Islam, S.; Pais, P.; McQueen, M.J.; et al. Risk factors for ischaemic and intracerebral haemorrhagic stroke in 22 countries (the INTERSTROKE study): A case-control study. Lancet 2010, 376, 112–123. [Google Scholar] [CrossRef]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: Executive Summary. J. Am. Coll. Cardiol. 2019, 74, 1376–1414. [Google Scholar] [CrossRef] [PubMed]
- Neumann, J.; Havulinna, A.S.; Zeller, T.; Appelbaum, S.; Kunnas, T.; Nikkari, S.; Jousilahti, P.; Blankenberg, S.; Sydow, K.; Salomaa, V. Comparison of Three Troponins as Predictors of Future Cardiovascular Events—Prospective Results from the FINRISK and BiomaCaRE Studies. PLoS ONE 2014, 9, e90063. [Google Scholar] [CrossRef]
- Jansen, H.; Rothenbacher, D.; Koenig, W. Is twice better than once?—Challenges of troponin measurements for risk prediction in the general population. Ann. Transl. Med. 2019, 7, S238. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| N = 2155 | Never Smokers N = 1174 | Past Smokers N = 503 | Current Smokers N = 478 | p-Value |
|---|---|---|---|---|
| Sex, Female (%) | 667 (58.1) | 260 (51.7) | 222 (46.4) | <0.001 |
| Age, Years | 35.6 ± 5.3 | 35.8 ± 4.9 | 34.5 ± 5.3 | <0.001 |
| Height, cm | 172 ± 9.19 | 172 ± 9.09 | 172 ± 9.11 | 0.31 |
| Weight, kg | 71 ± 14 | 75 ± 16 | 75 ± 15 | <0.001 |
| BMI, kg/m² | 24 ± 4 | 25 ± 4 | 25 ± 4 | <0.001 |
| Physical Activity 1 (%) | 619 (52.7) | 270 (53.7) | 244 (51.0) | 0.70 |
| Alcohol Consumption, g/24 h | 0.00 (0.00; 1.44) | 0.80 (0.00; 2.14) | 0.80 (0.00; 2.35) | <0.001 |
| Highest Education Level (%) | 504 (43.4) | 175 (35.10) | 117 (24.8) | <0.001 |
| Fruit/Vegetable Consumption 2 (%) | 271 (23.1) | 110 (21.9) | 82 (17.2) | 0.03 |
| Systolic BP, mm Hg/24 h | 122.27 ± 11.53 | 124.91 ± 11.00 | 124.41 ± 11.89 | <0.001 |
| Diastolic BP, mm Hg/24 h | 78.15 ± 7.94 | 79.35 ± 8.06 | 79.53 ± 8.30 | <0.001 |
| Hypertension (%) | 163 (13.9) | 80 (15.9) | 59 (12.3) | 0.27 |
| LDL-C, mmol/L | 2.84 (2.35; 3.44) | 2.85 (2.31; 3.44) | 2.98 (2.38; 3.63) | 0.06 |
| HDL-C, mmol/L | 1.53 (1.30; 1.84) | 1.50 (1.22; 1.80) | 1.37 (1.11; 1.66) | <0.001 |
| Total Cholesterol, mmol/L | 4.81 (4.26; 5.48) | 4.78 (4.29; 5.35) | 4.78 (4.27; 5.52) | 0.81 |
| Hs-CTnl, ng/L | 0.70 (0.43; 1.23) | 0.69 (0.43; 1.28) | 0.67 (0.41; 1.04) | 0.04 |
| N = 2155 | Never Smokers N = 1174 | Past Smokers N = 503 | Current Smokers N = 478 | p-Value for Trend |
|---|---|---|---|---|
| Univariate | Ref | 0.01 (−0.07; 0.12), p = 0.54 | −0.05 (−0.21; −0.02), p = 0.02 | p = 0.03 |
| Sex and age adjusted | Ref | −0.01 (−0.10; 0.07), p = 0.69 | −0.09 (−0.28; −0.11), p < 0.001 | p < 0.001 |
| Multivariable adjusted 1 | Ref | −0.02 (−0.12; 0.04), p = 0.34 | −0.08 (−0.25; −0.08), p < 0.001 | p < 0.001 |
| Never Smokers N = 1174 | Past Smokers N = 503 | <5 Pack-Years N = 180 | 5–10 Pack-Years N = 95 | >10 Pack-Years N = 189 | p-Value for Trend | |
|---|---|---|---|---|---|---|
| Hs-cTnI 1 | 0.71 [0.30–1.10] | 0.69 [0.26–1.12] | 0.63 [0.31–0.94] | 0.66 [0.31–1.02] | 0.69 [0.42–0.95] | p = 0.26 |
| Univariate | Ref | 0.01 (−0.06; 0.12), p = 0.53 | −0.03 (−0.24; 0.04), p = 0.15 | −0.03 (−0.30; 0.08), p = 0.25 | −0.04 (−0.26; 0.02), p = 0.09 | p = 0.14 |
| Sex and age adjusted | Ref | −0.01 (−0.10; 0.07), p = 0.74 | −0.03 (−0.24; 0.01), p = 0.07 | −0.03 (−0.29; 0.04), p = 0.15 | −0.09 (−0.40; −0.16), p < 0.001 | p < 0.001 |
| Multivariable adjusted 2 | Ref | −0.02 (−0.12; 0.04), p = 0.37 | −0.03 (−0.23; 0.02), p = 0.09 | −0.02 (−0.27; 0.06), p = 0.21 | −0.08 (−0.36; −0.11), p < 0.001 | p < 0.001 |
| Current Smokers N = 448 | ||||||
|---|---|---|---|---|---|---|
| N = 2155 | Never Smokers N = 1174 | Past Smokers n = 503 | Fagerström-Score <2 N = 230 | Fagerström-Score 3–5 N = 173 | Fagerström-Score >5 N = 45 | p-Value for Trend |
| Hs-cTnI 1 | 0.71 (0.80) [0.30–1.10] | 0.69 (0.86) [0.26–1.12] | 0.68 (0.70) [0.34–1.02] | 0.66 (0.59) [0.35–0.94] | 0.66 (0.50) [0.41–0.91] | p = 0.14 |
| Univariate | Ref. | 0.01 (−0.07; 1.12), p = 0.59 | −0.02 (−0.18; 0.06), p = 0.35 | −0.06 (−0.33; −0.04), p = 0.013 | −0.04 (−0.51; 0.02), p = 0.07 | p = 0.03 |
| Sex and age adjusted | Ref. | 0.01 (−0.10; 0.07), p = 0.68 | −0.03 (−0.20; 0.02), p = 0.10 | −0.09 (−0.41; −0.16), p < 0.001 | −0.07 (−0.66; −0.19), p < 0.001 | p < 0.001 |
| Multivariable adjusted 2 | Ref. | −0.02 (−0.12; 0.04), p = 0.33 | −0.03 (−0.19; 0.03), p = 0.17 | −0.08 (−0.38; −0.12), p < 0.001 | −0.06 (−0.61; −0.13), p < 0.001 | p < 0.001 |
| Past Smokers N = 497 | ||||||
|---|---|---|---|---|---|---|
| N = 2149 | Never Smokers N = 1174 | Current Smokers N = 478 | <2 years N = 85 | 2–4 Years N = 62 | >4 Years N = 350 | p-Value for Trend |
| Hs-cTnI 1 Median (IQR) [25–75%] | 0.71 (0.80) [0.30–1.10] | 0.67 (0.62) [0.36–0.98] | 0.75 (1.11) [0.21–1.28] | 0.74 (0.63) [0.42–1.05] | 0.66 (0.87) [0.21–1.08] | p = 0.17 |
| Univariate | Ref. | −0.05 (−0.21; −0.02), p = 0.02 | 0.02 (−0.11; 0.28), p = 0.41 | 0.01 (−0.16; 0.30), p = 0.61 | 0.004 (−0.10; 0.12), p = 0.86 | p = 0.094 |
| Sex and age adjusted | Ref. | −0.09 (−0.28; −0.11) p = 0.001 | −0.01 (−0.21; 0.14) p = 0.72 | 0.01 (−0.14; 0.27), p = 0.52 | −0.01 (−0.12; 0.07), p = 0.55 | p = 0.001 |
| Multivariable adjusted 2 | Ref. | −0.08 (−0.25; −0.08) p = 0.001 | −0.01 (−0.21; 0.14) p = 0.67 | 0.01 (−0.15; 0.26) p = 0.58 | −0.02 (−0.15; 0.04) p = 0.23 | p = 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grossmann, K.; Aeschbacher, S.; Wohlwend, N.; Blum, S.; Weideli, O.C.; Telser, J.; Risch, M.; Risch, L.; Conen, D. Smoking and High-Sensitivity Troponin I Levels in Young and Healthy Adults from the General Population. Appl. Sci. 2022, 12, 9777. https://doi.org/10.3390/app12199777
Grossmann K, Aeschbacher S, Wohlwend N, Blum S, Weideli OC, Telser J, Risch M, Risch L, Conen D. Smoking and High-Sensitivity Troponin I Levels in Young and Healthy Adults from the General Population. Applied Sciences. 2022; 12(19):9777. https://doi.org/10.3390/app12199777
Chicago/Turabian StyleGrossmann, Kirsten, Stefanie Aeschbacher, Niklas Wohlwend, Steffen Blum, Ornella C. Weideli, Julia Telser, Martin Risch, Lorenz Risch, and David Conen. 2022. "Smoking and High-Sensitivity Troponin I Levels in Young and Healthy Adults from the General Population" Applied Sciences 12, no. 19: 9777. https://doi.org/10.3390/app12199777
APA StyleGrossmann, K., Aeschbacher, S., Wohlwend, N., Blum, S., Weideli, O. C., Telser, J., Risch, M., Risch, L., & Conen, D. (2022). Smoking and High-Sensitivity Troponin I Levels in Young and Healthy Adults from the General Population. Applied Sciences, 12(19), 9777. https://doi.org/10.3390/app12199777