1. Introduction
An arteriovenous fistula is an abnormal connection between artery and vein; the blood contained in these veins becomes arterialized, venous pressure increases, and venous flow is altered in speed and direction [
1]. The clinical picture resulting in alteration of vascular dynamics is characterized by reduction of arterial perfusion, ocular hypoxia, and venous congestion.
Carotid-cavernous fistula (CCF) is an abnormal connection between the carotid arterial system (internal carotid artery and/or external carotid artery) and cavernous sinus.
According to the Barrow classification, CCFs are classified as direct (type A) and indirect (type B, C, and D) types [
1,
2].
Direct CCF, characterized by a direct connection between the internal carotid artery and cavernous sinus, are commonly post-traumatic [
1,
2].
Indirect carotid-cavernous fistula, also known as dural fistula of the cavernous sinus, is a special type of dural arteriovenous fistula where the immediate venous drainage is into the cavernous sinus [
1,
2]. Based on angiographic characteristics, dural fistula of cavernous sinus are classified into type B (the connection between dural branches of the internal carotid artery with cavernous sinus), type C (the connection between dural branches of the external carotid artery with cavernous sinus), and type D (the fistulous connection between dural branches of both internal and external carotid artery with cavernous sinus). Type B is the least common, whereas type D is the most commonly observed in clinical practice [
1,
2].
The etiology of the indirect carotid-cavernous fistula is not completely known; however, these could be associated with arterial hypertension, cerebral arteriosclerosis, diabetes, collagen diseases (Ehlers–Danlos syndrome, collagenosis), and post-menopausal age in women [
1,
2,
3].
Although dural carotid-cavernous fistula could be approached with conservatory therapy, untreated patients could present severe ocular and neurological complications, in particular the presence of ocular risk factors, such as increased intraocular pressure (IOP), retinal ischemia, and optic nerve edema [
3].
The advent of endovascular treatments significantly reduced the morbidity related to cavernous carotid fistula.
In this report, we describe a case of spontaneous dural carotid-cavernous fistula that occurred in a healthy woman, successfully treated with endovascular micro coil insertion.
2. Case Report
A 65-year-old woman presented to our attention complaining of two days of swelling in the right eye, reduced visual acuity, diplopia, and mild pain. The history was negative for recent trauma and confirmed good general health conditions. The physical examination revealed complete ophthalmoplegia (
Figure 1), non-pulsatile reducible axile exophthalmos, eyelid edema, significant chemosis, and conjunctival ectropion (
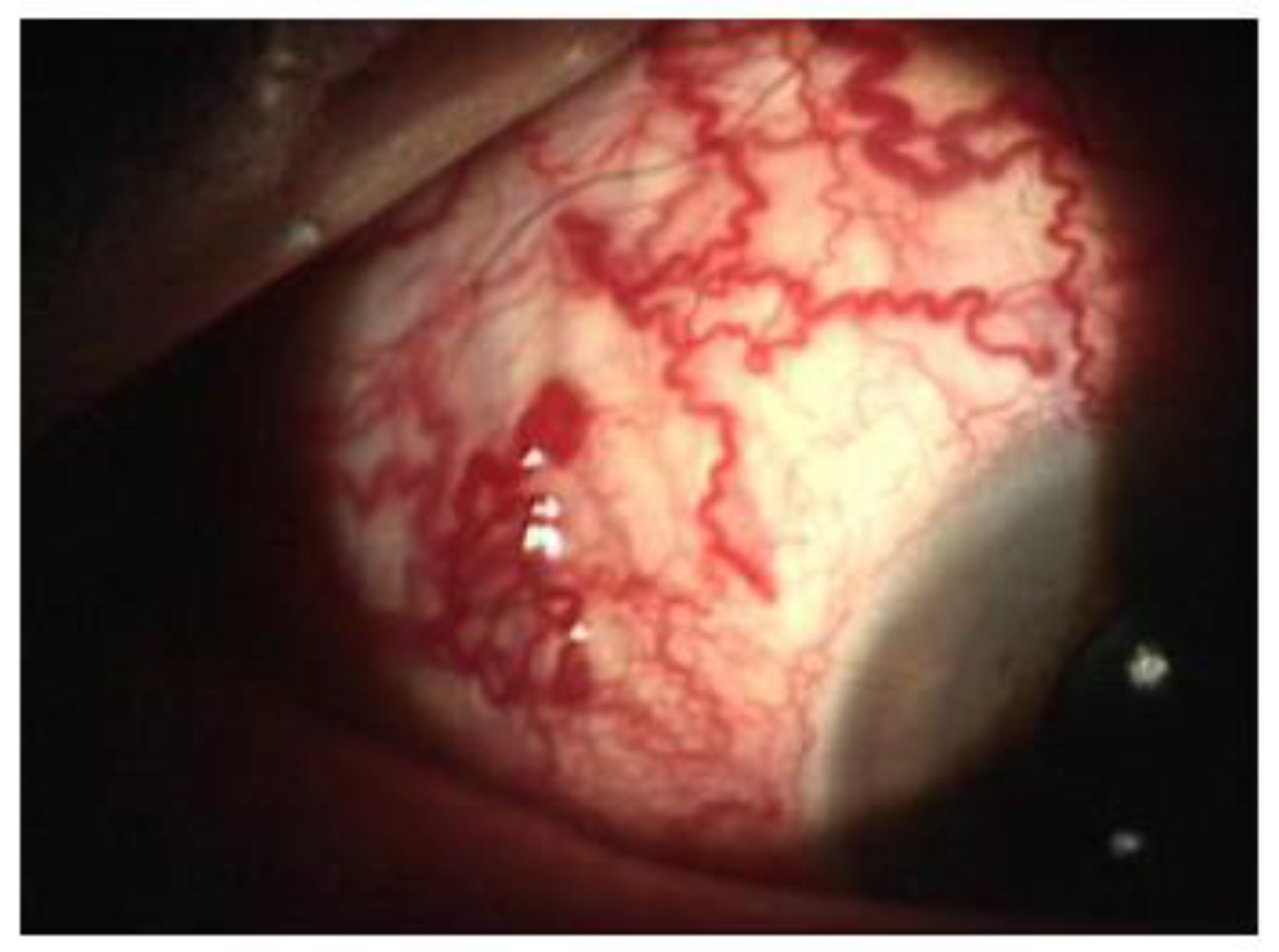
Figure 2). Visual acuity at the time of admission was 5/10 in the right eye and 10/10 in the left eye. The biomicroscopic examination of the anterior segment showed an important stasis of the episcleral vessels (
Figure 3) and a shallow anterior chamber, whereas the fellow eye was unremarkable.
Fundus examination showed an alteration of the normal arterio-venous ratio (A/V) from 1–4 to 1–2 and two extensive cotton exudates at the posterior pole (
Figure 4).
The intraocular pressure (IOP) was 30 mmHg in the right eye and 12 mmHg in the left eye.
To reduce the IOP, the patient was suddenly treated with intravenous 18% Mannitol, topical Timolol Maleate 5 mg/mL, and Dorzolamide 20 mg/mL drops twice a day.
Furthermore, US showed congestion at the level of the superior ophthalmic vein.
The selective cerebral angiography (
Figure 5), carried out through right femoral catheterization, revealed a dural fistula of the right cavernous sinus wall between the branches of the internal maxillary artery, most likely of the accessory meningeal artery, and the cavernous sinus with early opacification of the ophthalmic vein that presented an increased caliber.
The multidisciplinary team involved in this case comprised neurosurgeons and interventional neuroradiologists. The treatment decided was carried out two times; the first provided the insertion of a cannula needle in the right orbital vein by a trans-palpebral anterior approach, while the second provided for the embolization of the cavernous sinus seat of the venous part of the fistula, through the placement of 5 spirals (Vortex 2x5, Boston), up to the complete exclusion of the fistula. The angiographic control performed immediately after the affixing of the spirals showed the complete normalization of the circulation between the internal and external carotid (
Figure 6).
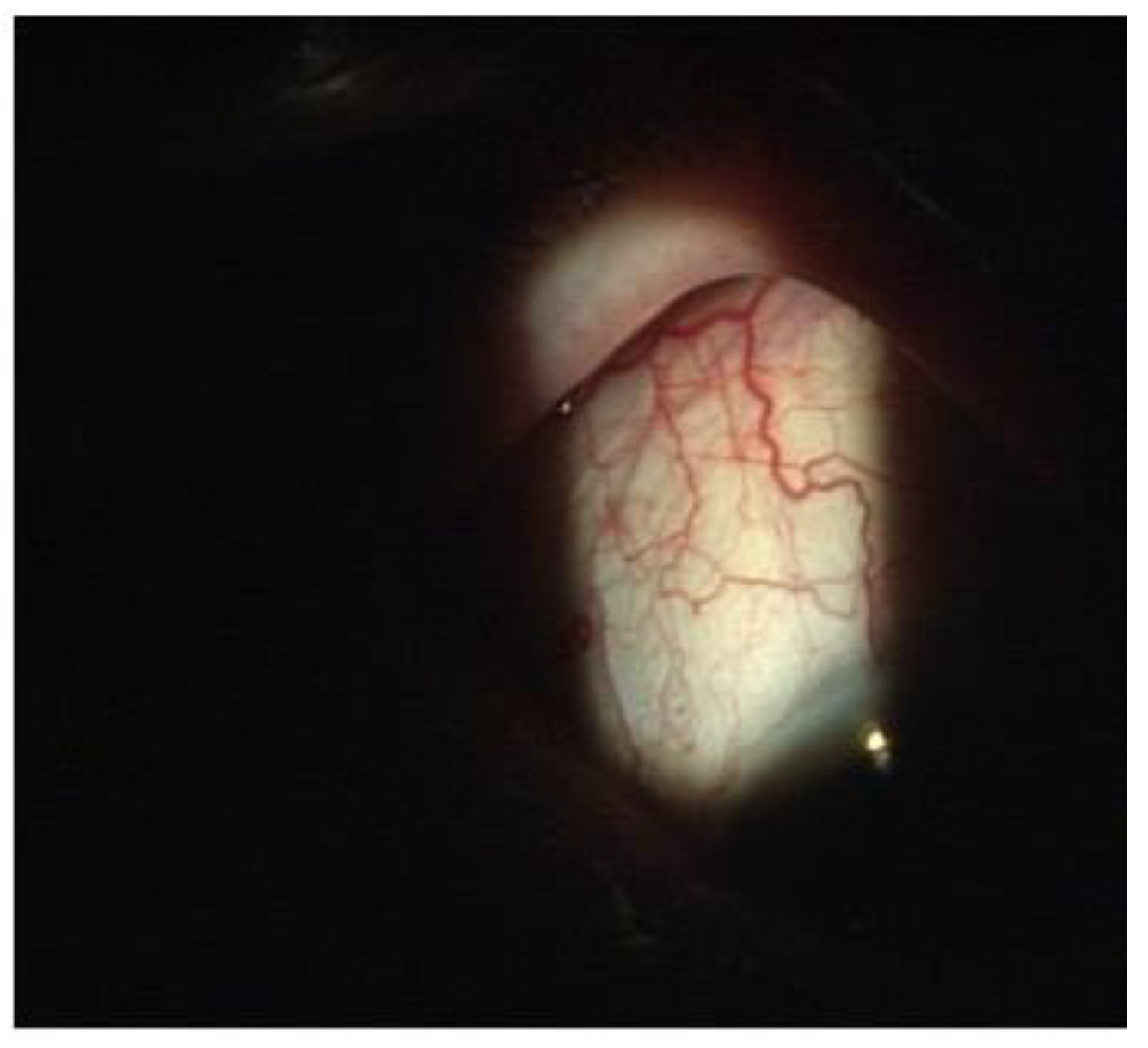
On the third post-operative day, the clinical condition was significantly improved in the following ways: a clear reduction of the exophthalmos and the congestion of the episcleral vessels (
Figure 7), a complete recovery of ocular motility (
Figure 8), visual acuity improved to 10/10, IOP was 14 mmHg, the disappearance of cotton exudates, and a normalization of the A/V ratio. Fifteen days after the surgery, the ocular conditions were stable.
3. Discussion
Dural fistulas represent a challenging disease to treat, either because of the difficulty of a prompt diagnosis or because of the difficulty of the intervention dictated by the size and tortuosity of the vessels and, not least, the difficulty of coordinating the multidisciplinary team [
1,
2].
All these problems must be promptly overcome in order to have integrative restitution of the whole visual apparatus.
Ophthalmologists are often the first doctors to come into contact with patients with carotid-cavernous fistula, and they should recognize and indicate the necessary examinations in a timely manner. The typical clinical manifestations are: unilateral proptosis, the tumescence of the eyelid, conjunctival chemosis, caput medusae, pulsation of the eyeball (always observed in direct fistula), increased IOP, and diplopia. Furthermore, these clinical features should be differentiated into endocrine orbitopathy, orbital-cellulitis, posterior scleritis, thrombosis of the sinus cavernous, and malignancies.
In some cases, when the diagnosis is delayed, the visual functionality could be irreparably damaged, with severe ocular and neurological complications [
1,
2].
A conservative approach could be indicated for patients with few clinical signs, in particular for indirect fistula, because of a good chance of spontaneous occlusion of the fistula; however, it is also necessary to ensure regular observation of psycho-physical functions, IOP, and the ocular fundus [
4,
5,
6,
7].
In our case, the increased IOP and the ischemic retinal features justified the urgency of treatment aimed at prompt fistula occlusion.
Currently, the most common treatment is endovascular embolization using means of spirals, detachable flasks, and, as a last resort given the side effects (such as diffuse thrombosis and post-operative inflammatory reaction), the use of a sclerotic substance [
8,
9,
10].
Transvenous via through the inferior petrosal sinus is the most common approach; however, when this access is absent for anatomical variations or thrombosis, direct access to the superior ophthalmic vein represents an alternative technique. Heran et al., in a recent study, reported successful results of imaging-guided percutaneous superior ophthalmic vein access in 20 patients with carotid-cavernous fistula treatment [
10].
In conclusion, our case demonstrated that a prompt diagnosis and multidisciplinary management are essential for clinical resolution and to preserve the visual function of the patient.
Author Contributions
Conceptualization, P.F.F. and L.D.S.; methodology, G.W.O.; investigation, P.F.F. and L.D.S.; resources, A.M.; data curation, L.I.; writing—original draft preparation, G.W.O.; writing—review and editing, G.W.O. and A.M.; supervision, A.M. and P.A. project administration, P.A.; funding acquisition, A.M. All authors have read and agreed to the published version of the manuscript.
Funding
The authors did not receive any financial support from any public or private sources. The authors have no financial or proprietary interest in a product, method, or material described.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Ke, L.; Yang, Y.-N.; Yuan, J. Bilateral carotid-cavernous fistula with spontaneous resolution: A case report and literature review. Medicine 2017, 96, e6869. [Google Scholar] [CrossRef] [PubMed]
- Henderson, A.D.; Miller, N.R. Carotid-cavernous fistula: Current concepts in aetiology, investigation, and management. Eye 2018, 32, 164–172. [Google Scholar] [CrossRef] [PubMed]
- Guo, H.; Yin, Q.; Liu, P.; Guan, N.; Huo, X.; Li, Y. Focus on the target: Angiographic features of the fistulous point and prognosis of transvenous embolization of cavernous sinus dural arteriovenous fistula. Interv. Neuroroadiol. 2018, 24, 197–205. [Google Scholar] [CrossRef] [PubMed]
- Feiner, L.; Bennett, J.; Volpe, N.J. Spontaneous carotido-cavernous fistulas: Phlebographic appearance. Curr. Neurol. Neurosci. Rep. 2003, 3, 415–420. [Google Scholar] [CrossRef] [PubMed]
- De Keizer, R. Carotid-cavernous and orbital arteriovenous fistulas: Ocular features, diagnostic and hemodynamic considerations in relation to visual impairment and morbidity. Orbit 2003, 22, 121–142. [Google Scholar] [CrossRef] [PubMed]
- Jozef, Č. Carotid-cavernous fistula from the perspective of an ophthalmologist A Review. Czech Slovak Ophthalmol. 2019, 76, 203–210. [Google Scholar] [CrossRef]
- Fattahi, T.T.; Brandt, M.T.; Jenkins, W.S.; Steinberg, B. Traumatic carotid—Cavernous fistula: Pathophysiology and treatment. J. Craniofacial Surg. 2003, 14, 240–246. [Google Scholar] [CrossRef] [PubMed]
- Gioulekas, J.; Mitchell, P.; McNab, A.A. Embolization of carotid cavernous fistulas via the superior ophthalmic vein. Aust. N. Z. J. Ophthalmol. 1997, 25, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Lim, N.C.S.; Lin, H.A.H.E.; Ong, C.K.; Sundar, G. Treatment of Dural Carotid-Cavernous Fistulas via the Medial Ophthalmic Vein. Orbit 2015, 34, 345–350. [Google Scholar] [CrossRef] [PubMed]
- Heran, M.K.S.; Volders, D.; Haw, C.; Shewchuk, J.R. Imaging-Guided Superior Ophthalmic Vein Access for Embolization of Dural Carotid Cavernous Fistulas: Report of 20 Cases and Review of the Literature. AJNR Am. J. Neuroradiol. 2019, 40, 699–702. [Google Scholar] [CrossRef] [PubMed]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}







