


Requesting Help Module Interface Design on Key Partial Video with Action and Augmented Reality for Children with Autism Spectrum Disorder

Abstract
1. Introduction
- to explore the use of SGDs by non-verbal children with ASD;
- to compare the effectiveness of augmentative and alternative communication (AAC) with augmented reality (AR) in operating identification;
- to evaluate whether the intervention of AAC with AR can increase the users’ accuracy in question responses;
- to assess the difference in the independent completion rate of the interfaces with prompt;
- to discuss whether the interfaces with prompts could improve users’ communication ability.
2. Related Work
3. Methods
3.1. The Design Process of the Communication Menu
- In the first stage, we conducted preliminary interviews with more than ten children with autism, parents, and teachers. The Ethics Committee of the China Medical University, Taiwan Ministry of Public Health, provided ethical approval for this study. All participants signed a consent form when explaining the designed questionnaire. We used core vocabulary graphics recording 100 sentences and then select ten questions from all sentences (Appendix A and Supplementary File S1), and then made more than ten communication boards according to the grammar (Table 1) for the study and related words gleaned from these interviews to design the requesting-help communication menu [35]. Some parents, class tutors, and language therapists met regularly to discuss the core vocabulary graphics. They compiled a core vocabulary of more than a thousand commonly used communication terms to be used in our communication graphics system. The design team collected the details of how children with ASD learn communication skills by pointing at paper-based picture cards. They used the concept of core vocabulary to create an interface with which participants can learn by repeatedly practicing specific sentence patterns [36,37,38,39].
- In the second stage, researchers designed textbooks based on core vocabulary and the ISO copyright-free graphics library (available at https://isorepublic.com; accessed on 1 October 2021) to redesign and select the most frequently used words with graphics to make sentences. For example, Table 1 lists subject, verb, object, adverb, or subject, verb, adjective, adverb, and other combinations of sentence elements. The requesting help module provided the main communicative content—the core vocabulary. Because of different needs, the requesting help module and its dozens of vocabularies were organized into ten categories, and the vocabularies were used as marginal vocabularies, so it could provide the use and expression of choice judgments. [40,41]. Researchers used different colors to classify the different parts of speech (for example, yellow for subject words, orange for affirmative and negative words, green for verbs, and so on). They also used a structured layout design to guide participants in using lexical phrases in proper sequence [42,43,44].
- In the third stage, because the participants sometimes found the interface too complicated to easily use, we realized that we need to further study the differences in how children with ASD understand meaning. We hoped that this stage of intervention would help us to improve the participants’ abilities to engage in further operational communication and to request help. Therefore, we adjusted the interface to use in formulating eight modules of requesting help recognition concepts. The operational communication content of requesting help was then developed. Scenarios were created (Appendix A Table A1 and Supplementary File S1). We then gave our prototype to parents and caregivers to judge its value and verify its usability for children with ASD [45,46].
- In the fourth stage, the interface refinement and assessment stage, our system was installed onto a tablet device for the three children (the end users) to test. The designers, special education instructors, and speech therapists assessed the effectiveness of the refined interface. The interface showed a table of the parts of speech, subjects, verbs, objects, nouns, adjectives, adverbs, and conjunctions.
3.2. Using the Auto Organizational Menu with AR to Generate a Request for Help
3.2.1. Participants
3.2.2. Settings
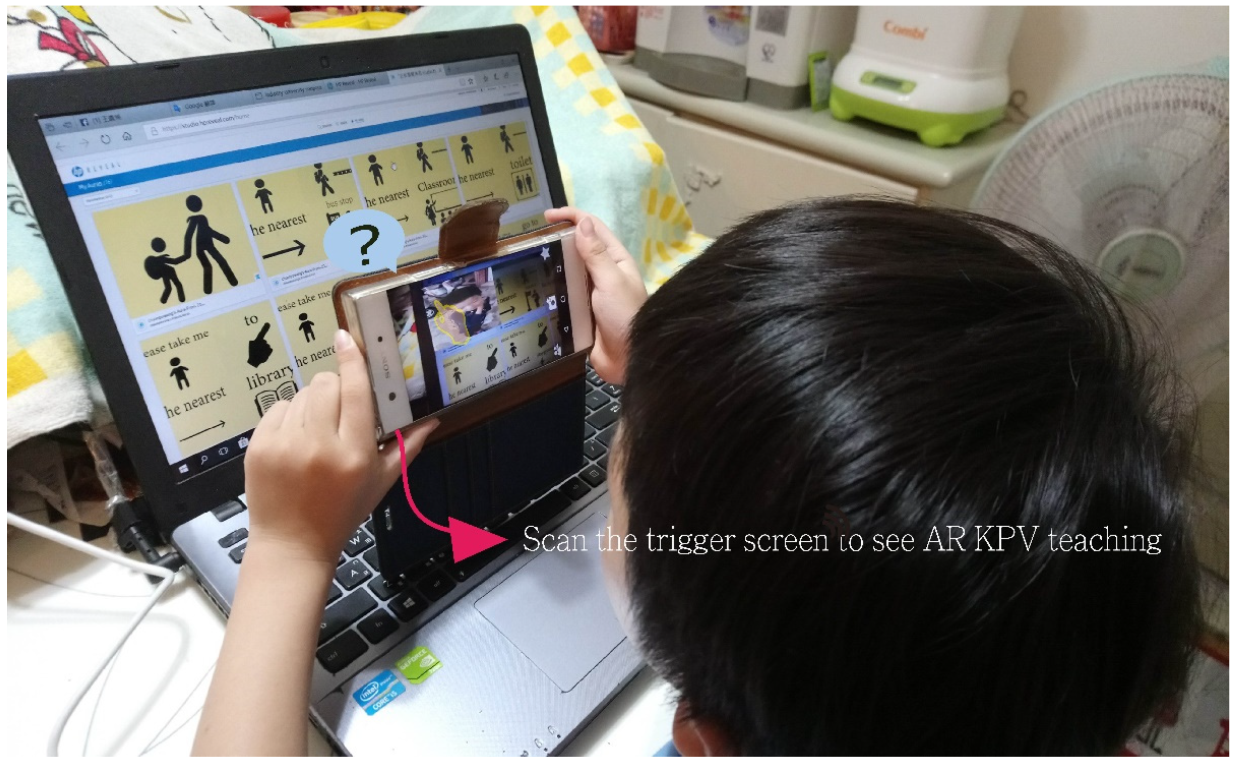
3.2.3. Key Partial Video with Action (KPV)
3.2.4. Operational Definitions
3.3. Intervention Strategy
3.3.1. How We Selected Standard Answers
3.3.2. Correct Judgment Rate of Children with ASD
3.3.3. Intervention and Evaluation of the Procedure
3.3.4. Intervention Definition
- A request for help and a transfer cognitive intervention: using AR and capturing KPV images to make participants’ intervention assessments of how to request help using photographs and identifying and recognizing action from schematic drawings, to teach participants with ASD how to understand the correct way to request help. Experimenters asked participants to choose the subjects, nouns, verbs, objects, adjectives, adverbs, and question words to allow the AOM to automatically organize sentences needed for the intervention task.
- The experimenters told the participants what kind of help to request, to execute the tasks in the Appendix A, to pay attention to social interaction distance and continuity, and to distinguish between two different kinds of real situations and between ways of requesting help. This study used a combination of multiple baseline and reversal designs: A-B-C-B to evaluate the two intervention phases and analyze the outcomes of the intervention.
- Task execution: the experimenter told the participants what kind of help in the test to request, and to evaluate whether they understood and performed the tasks in the Appendix A. They wanted to use some distance to evaluate the help-seeking activity, and they wanted to evaluate the continuous effectiveness of the training. They used two different real-world situations for the participants to perform the task of asking for help, and they used a combination of multiple baseline and reversal designs (A-B-C-B) to assess the two intervention phases and analyze the outcomes of the intervention.
4. Results
4.1. Results of KPV with AR, AOM Intervention, and Evaluation
4.1.1. Judgments of Perceptions of Others
4.1.2. Situational Comprehension
4.2. Interaction Effect
5. Conclusions
5.1. Discussion
5.2. Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Title Design/Session | The Correct Rate\Time | |||||
|---|---|---|---|---|---|---|
| Intervention | 1 | 2 | 1 | 2 | 1 | 2 |
| Participant | 1 | 2 | 3 | |||
| Requesting help | ||||||
| 1. Please help me go to the nearest convenience store. | ||||||
| 2. Please help me go to the nearest toilet. | ||||||
| 3. Please take me to the vegetarian restaurant. | ||||||
| 4. Please help me go to my teacher’s office. | ||||||
| 5. Please help me make a telephone call to my family. | ||||||
| 6. Please help me ask my family to be there. | ||||||
| 7. Please help me hand in homework to my teacher. | ||||||
| 8. Please take me to my school playground. | ||||||
| 9. Please take me to the nearest library. | ||||||
| 10. Please take me to the nearest health center. | ||||||
| Accuracy & Action% | ||||||
References
- Kurtcu, F. An analyze of high school web interface designs in terms of graphic design. Procedia Soc. Behav. Sci. 2012, 46, 5661–5665. [Google Scholar] [CrossRef][Green Version]
- Binger, C.; Light, J. The morphology and syntax of individuals who use AAC: Research review and implications for effective practice. Augment. Altern. Commun. 2008, 24, 123–138. [Google Scholar] [CrossRef] [PubMed]
- Beukelman, D.; Mirenda, P. Augmentative and Alternative Communication: Supporting Children and Adults with Complex Communication Needs, 4th ed.; Paul Brookes: Baltimore, MD, USA, 2013. [Google Scholar]
- Boesch, M.C.; Wendt, O.; Subramanian, A.; Hsu, N. Comparative efficacy of the Picture Exchange Communication System (PECS) versus a speech-generating device: Effects on social-communicative skills and speech development. Augment. Altern. Commun. 2013, 29, 197–209. [Google Scholar] [CrossRef] [PubMed]
- Van der Meer, L.A.J.; Rispoli, M. Communication interventions involving speech-generating devices for children with autism: A review of the literature. Dev. Neurorehabil. 2010, 13, 294–306. [Google Scholar] [CrossRef]
- Sigafoos, J.; Green, V.A.; Payne, D.; Son, S.H.; O’Reilly, M.; Lancioni, G.E. A Comparison of Picture Exchange and Speech-Generating Devices: Acquisition, Preference, and Effects on Social Interaction. Augment Altern. Commun. 2009, 25, 99–109. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Robert, C.; Pasquier, L.; Cohen, D.; Fradin, M.; Canitano, R.; Damaj, L.; Tordjman, S. Role of genetics in the etiology of Autistic Spectrum Disorder: Towards a hierarchical diagnostic strategy. Int. J. Mol. Sci. 2017, 18, 618. [Google Scholar] [CrossRef]
- Billinghurst, M.; Hirokazu, K.; Ivan, P. The Magic Book: A Transitional AR Interface. Comput. Graph. 2001, 25, 745–753. [Google Scholar] [CrossRef]
- Taipei Autism Children Social Welfare Foundation. Prevalence of Autism in Taiwan. Available online: http://www.ican.org.tw/content.asp?id=2 (accessed on 15 August 2021).
- Tick, B.; Bolton, P.; Happé, F.; Rutter, M.; Rijsdijk, F. Heritability of autism spectrum disorders: A meta-analysis of twin studies. J. Child Psychol. Psychiatry 2016, 57, 585–595. [Google Scholar] [CrossRef]
- Tordjman, S.; Somogyi, E.; Coulon, N.; Kermarrec, S.; Cohen, D.; Bronsard, G.; Xavier, J. Gene × environment interactions in autism spectrum disorders: Role of epigenetic mechanisms. Front. Psychiatry 2014, 5, 53. [Google Scholar] [CrossRef]
- Chen, C.H.; Lee, I.J.; Lin, L.Y. Augmented reality-based video-modeling storybook of nonverbal facial cues for children with autism spectrum disorder to improve their perceptions and judgments of facial expressions and emotions. Comput. Hum. Behav. 2016, 55, 477–485. [Google Scholar] [CrossRef]
- Chen, L.; Xu, L.; Dhar, S.; Li, M.; Talwar, D.; Jung, E. Autism spectrum disorders: A qualitative study of attitudes toward prenatal genetic testing and termination decisions of affected pregnancies. Clin. Genet. 2015, 88, 122–128. [Google Scholar] [CrossRef]
- Johnston, D.; Hauke, E.; Gavin, K. SoundFields: A virtual reality game designed to address auditory hypersensitivity in individuals with autism spectrum disorder. Appl. Sci. 2020, 10, 2996. [Google Scholar] [CrossRef]
- Masi, A.; DeMayo, M.M.; Glozier, N.; Guastella, A.J. An overview of Autism Spectrum Disorder, heterogeneity and treatment options. Neurosci. Bull. 2017, 33, 183–193. [Google Scholar] [CrossRef]
- Jiang, Y.; Wang, Y.; Xiu, X.; Choy, K.; Pursley, A.; Cheung, S. Genetic diagnosis of autism spectrum disorders: The opportunity and challenge in the genomics era. Crit. Rev. Clin. Lab. Sci. 2014, 51, 249–262. [Google Scholar] [CrossRef][Green Version]
- Rossi, M.; El-Khechen, D.; Black, M.H.; Hagman, K.D.F.; Tang, S.; Powis, Z. Outcomes of Diagnostic Exome Sequencing in Patients With Diagnosed or Suspected Autism Spectrum Disorders. Pediatr. Neurol. 2017, 70, 34–43. [Google Scholar] [CrossRef]
- Wijker, C.; van der Steen, S.; Spek, A.; Leontjevas, R.; Enders-Slegers, M.J. Social development of adults with autism spectrum disorder during dog-assisted therapy: A detailed observational analysis. Int. J. Environ. Res. Public Health 2020, 17, 5922. [Google Scholar] [CrossRef]
- ASHA, Definition of Communication and Appropriate Targets. Available online: https://www.asha.org/njc/definition-of-communication-and-appropriate-targets/ (accessed on 15 August 2021).
- McNaughton, D.; Light, J.; Beukelman, D.R.; Klein, C.; Nieder, D.; Nazareth, G. Building capacity in aac: A person-centred approach to supporting participation by people with complex communication needs. Augment. Altern. Commun. 2019, 35, 56–68. [Google Scholar] [CrossRef]
- Chung, Y.C.; Carter, E.W. Promoting peer interactions in inclusive classrooms for students who use speech-generating devices. Res. Pract. Pers. Sev. Disabil. 2013, 38, 94–109. [Google Scholar] [CrossRef]
- Escobedo, L.; Tentori, M.; Quintana, E.; Favela, J.; Garcia-Rosas, D. Using augmented reality to help children with autism stay focused. IEEE Pervasive Comput. 2014, 1, 38–46. [Google Scholar] [CrossRef]
- Shelton, B.E.; Hedley, N.R. Using Augmented Reality for Teaching Earth-Sun Relationships to Undergraduate Geography Students. In Proceedings of the First IEEE International Workshop Agumented Reality Toolkit, Darmstadt, Germany, 29 September 2002; Volume 8. [Google Scholar]
- Chen, C.H.; Chou, Y.Y.; Huang, C.Y. An augmented-reality-based concept map to support mobile learning for science. Asia-Pac. Educ. Res. 2016, 25, 567–578. [Google Scholar] [CrossRef]
- Berenguer, C.; Baixauli, I.; Gómez, S.; Andrés, M.D.E.P.; De Stasio, S. Exploring the impact of augmented reality in children and adolescents with autism spectrum disorder: A systematic review. Int. J. Environ. Res. Public Health 2020, 17, 6143. [Google Scholar] [CrossRef]
- Wang, C.P.; Tsai, C.H. Application of virtual reality to the study of festival culture in aboriginal literature. In Proceedings of the 2nd International Conference on Image and Graphics Processing, Singapore, 23–25 February 2019; pp. 136–139. [Google Scholar]
- Tsai, C.H.; Wang, C.P. An Analysis of the Development of Cultural Augmented Reality Education in Taiwanese Aboriginal Literature. Int. J. E-Educ. E-Bus. E-Manag. E-Learn. 2019, 9, 357–365. [Google Scholar] [CrossRef][Green Version]
- Lim, K.C.; Selamat, A.; Alias, R.A.; Krejcar, O.; Fujita, H. Usability Measures in Mobile-Based Augmented Reality Learning Applications: A Systematic Review. Appl. Sci. 2019, 9, 2718. [Google Scholar] [CrossRef]
- El-Seoud, M.; Halabi, O.; Geroimenko, V. Assisting Individuals with Autism and Cognitive Disorders: An Augmented Reality based Framework. Int. J. Online Biomed. Eng. 2019, 15, 28–39. [Google Scholar] [CrossRef]
- Quintero, J.; Baldiris Navarro, S.M.; Rubira, R.; Cerón, J.; Velez, G. Augmented Reality in Educational Inclusion. A Systematic Review on the Last Decade. Front. Psychol. 2019, 10, 1835. [Google Scholar] [CrossRef]
- Baragash, R.S.; Al-Samarraie, H.; Alzahrani, A.I.; Alfarraj, O. Augmented reality in special education: A meta-analysis of single-subject design studies. Eur. J. Spec. Needs Educ. 2019, 35, 382–397. [Google Scholar] [CrossRef]
- Marto, A.; Almeida, H.A.; Gonçalves, A. Using Augmented Reality in Patients with Autism: A Systematic Review. In Proceedings of the ECCOMAS Thematic Conference on Computational Vision and Medical Image Processing, Porto, Portugal, 16–18 October 2019; Springer: Cham, Switzerland, 2019; pp. 454–463. [Google Scholar]
- Khowaja, K.; Banire, B.; Al-Thani, D.; Sqalli, M.T.; Aqle, A.; Shah, A.; Salim, S.S. Augmented reality for learning of children and adolescents with autism spectrum disorder (ASD): A systematic review. IEEE Access 2020, 8, C78779–C78807. [Google Scholar] [CrossRef]
- Chen, C.H.; Wang, C.P.; Su, C.C. The effectiveness of using auto organizational menu to communicate with classmates: A case study of autism spectrum disorders. In Proceedings of the 6th International Conference on Software and Computer Applications, Bangkok, Thailand, 26–28 February 2017; pp. 304–309. [Google Scholar]
- Vanderheiden, G.; David, K. Comparative analysis of fixed-vocabulary communication acceleration techniques. Augment. Altern. Commun. 1987, 3, 196–206. [Google Scholar] [CrossRef]
- Hervás, R.; Bautista, S.; Méndez, G.; Galván, P.; Gervás, P. Predictive composition of pictogram messages for users with autism. J. Ambient. Intell. Humaniz. Comput. 2020, 11, 5649–5664. [Google Scholar] [CrossRef]
- Garcia, L.F.; de Oliveira, L.C.; de Matos, D.M. Evaluating pictogram prediction in a location-aware augmentative and alternative communication system. Assist. Technol. 2016, 28, 83–92. [Google Scholar] [CrossRef]
- Pereira, J.; Franco, N.; Fidalgo, R. A semantic grammar for augmentative and alternative communication systems. In Text, Speech, and Dialogue; Sojka, P., Kopeček, I., Pala, K., Horák, A., Eds.; Springer International Publishing: Cham, Switzerland, 2020; pp. 257–264. [Google Scholar]
- Martínez-Santiago, F.; Díaz-Galiano, M.C.; Urena-López, L.A.; Mitkov, R. A semantic grammar for beginning communicators. Knowl. -Based Syst. 2015, 86, 158–172. [Google Scholar] [CrossRef]
- Goldberg, Y.; Hirst, G. Neural Network Methods in Natural Language Processing; Morgan & Claypool: San Rafael, SR, USA, 2017; pp. 104–113. [Google Scholar]
- Franco, N.; Silva, E.; Lima, R.; Fidalgo, R. Towards a reference architecture for augmentative and alternative communication systems. In Brazilian Symposium on Computers in Education (Simpósio Brasileiro de Infor660 mática na Educação-SBIE); 2018; Volume 29, p. 1073. Available online: https://www.researchgate.net/publication/328735940_Towards_a_Reference_Architecture_for_Augmentative_and_Alternative_Communication_Systems (accessed on 1 July 2022).
- Ng, C.K.; Lam, S.H.; Tsang, S.T.; Yuen, C.; Chien, C.W. The relationship between affiliate stigma in parents of children with autism spectrum disorder and their children’s activity participation. Int. J. Environ. Res. Public Health 2020, 17, 1799. [Google Scholar] [CrossRef]
- Pereira, J.; Pena, C.; de Melo, M.; Cartaxo, B.; Fidalgo, R.; Soares, S. Facilitators and barriers to using alternative and augmentative communication systems by aphasic: Therapists perceptions. In Proceedings of the 2019 IEEE 32nd International Symposium on Computer-Based Medical Systems (CBMS), Cordoba, Spain, 5–7 June 2019; Volume 645, pp. 349–354. [Google Scholar]
- Donato, C.; Spencer, E.; Arthur-Kelly, M. A critical synthesis of barriers and facilitators to the use of aac by children with autism spectrum disorder and their communication partners. Augment. Altern. Commun. 2018, 34, 242–253. [Google Scholar] [CrossRef] [PubMed]
- Devlin, J.; Chang, M.W.; Lee, K.; Toutanova, K. BERT: Pre-training of Deep Bidirectional Transformers for Language Understanding. In Proceedings of the 2019 Conference of the North American Chapter of the 685 Association for Computational Linguistics: Human Language Technologies, Minneapolis, MN, USA, 2–7 June 2019; Volume 1, (Long and Short Papers). Association for Computational Linguistics: Minneapolis, MN, USA, 2019; pp. 4171–4186. Available online: https://www.aclweb.org/anthology/N19-1423 (accessed on 1 July 2022). [CrossRef]
- Scarlini, B.; Pasini, T.; Navigli, R. With More Contexts Comes Better Performance: Contextualized Sense Embeddings for All-Round Word Sense Disambiguation. In Proceedings of the 2020 Conference on Empirical 700 Methods in Natural Language Processing, Association for Computational Linguistics, Online, 16–20 November 2020. [Google Scholar] [CrossRef]
- Ko’s Obstetrics & Gynecology. The International Standards for Cytogenomic Arrays Cortium Analysis Application Procedure. Available online: http://www.genephile.com.tw/aCGH/htm/ISCA%20array.htm (accessed on 15 August 2021).
- Saturno, C.E.; Ramirez, A.R.G.; Conte, M.J.; Farhat, M.; Piucco, E.C. An augmentative and alternative communication tool for children and adolescents with cerebral palsy. Behav. Inf. Technol. 2015, 34, 632–645. [Google Scholar] [CrossRef]
- Lin, P.C.; Peng, L.Y.; Hsiao, R.C.; Chou, W.J.; Yen, C.F. Teacher harassment victimization in adolescents with high-functioning autism spectrum disorder: Related factors and its relationships with emotional problems. Int. J. Environ. Res. Public Health 2020, 17, 4057. [Google Scholar] [CrossRef] [PubMed]



| Style No. | Sentence and Rule | |||||
|---|---|---|---|---|---|---|
| 1 | S | V | N | |||
| 2 | S | V | Adj | |||
| 3 | S | V | Adv | Adj | ||
| 4 | S | V | Adj | N | ||
| 5 | S | Conj | O | V | Adv | Adj |
| 6 | S | Conj | O | V | Adj | N |
| Session\Participants | P1 | P2 | P3 | Average | TD1 | TD2 | Average |
|---|---|---|---|---|---|---|---|
| Baseline | 33 | 28 | 42 | 34 | 85 | 81 | 83 |
| Intervention1 | 70 | 69 | 69 | 69 | 98 | 96 | 97 |
| Intervention2 | 72 | 76 | 68 | 72 | 99 | 99 | 99 |
| Reversal | 53 | 57 | 57 | 56 | 93 | 90 | 92 |
| Maintenance | 58 | 58 | 58 | 58 | 93 | 95 | 94 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, C.-P.; Tsai, C.-H.; Lee, Y.-L. Requesting Help Module Interface Design on Key Partial Video with Action and Augmented Reality for Children with Autism Spectrum Disorder. Appl. Sci. 2022, 12, 8527. https://doi.org/10.3390/app12178527
Wang C-P, Tsai C-H, Lee Y-L. Requesting Help Module Interface Design on Key Partial Video with Action and Augmented Reality for Children with Autism Spectrum Disorder. Applied Sciences. 2022; 12(17):8527. https://doi.org/10.3390/app12178527
Chicago/Turabian StyleWang, Chuan-Po, Cheng-Hui Tsai, and Yann-Long Lee. 2022. "Requesting Help Module Interface Design on Key Partial Video with Action and Augmented Reality for Children with Autism Spectrum Disorder" Applied Sciences 12, no. 17: 8527. https://doi.org/10.3390/app12178527
APA StyleWang, C.-P., Tsai, C.-H., & Lee, Y.-L. (2022). Requesting Help Module Interface Design on Key Partial Video with Action and Augmented Reality for Children with Autism Spectrum Disorder. Applied Sciences, 12(17), 8527. https://doi.org/10.3390/app12178527