
Up-to-Date Optimization of the 90Y-PET/CT Reconstruction Protocol for Volumetric Quantification in Trans-Arterial RadioEmbolization (TARE) Procedures in the Era of Theranostics

 ,
, 
 , and
, and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
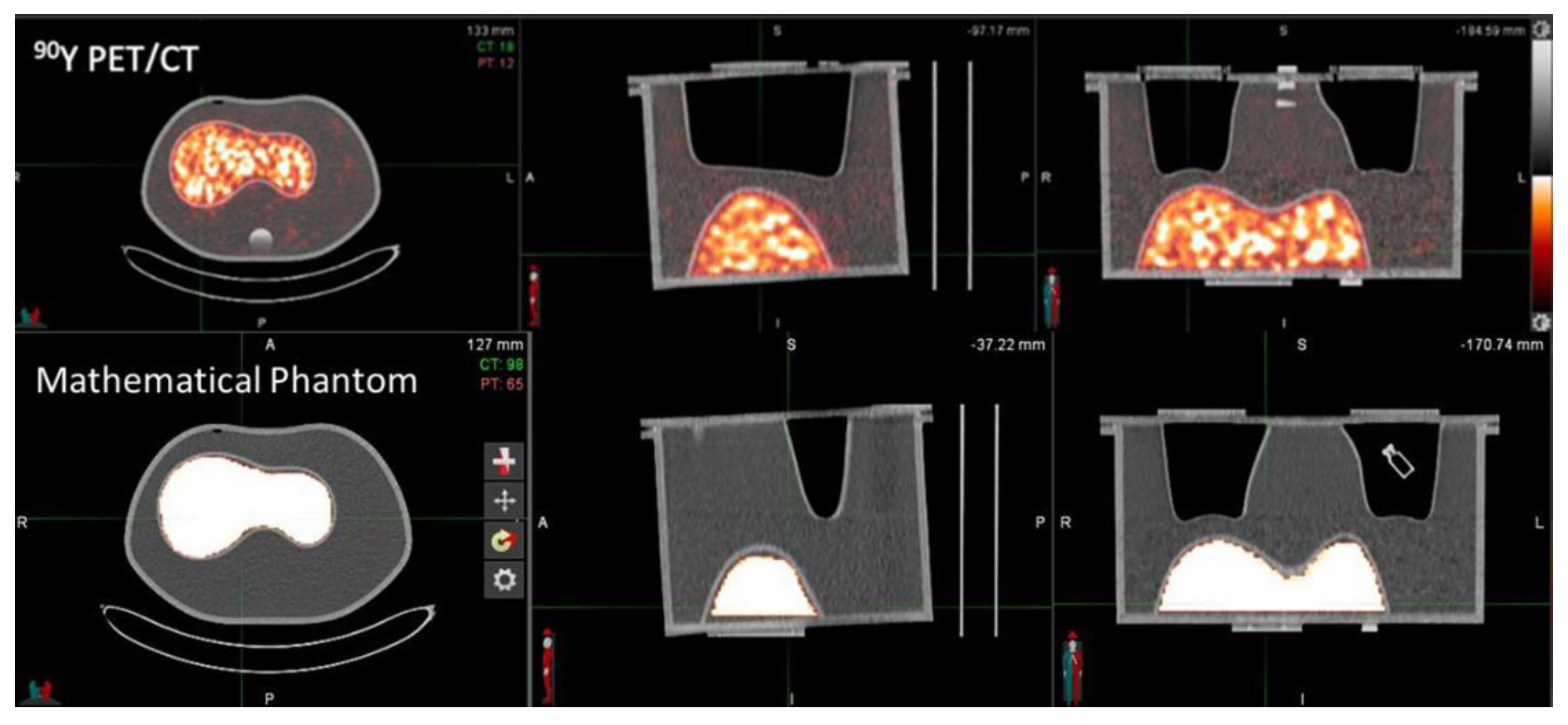
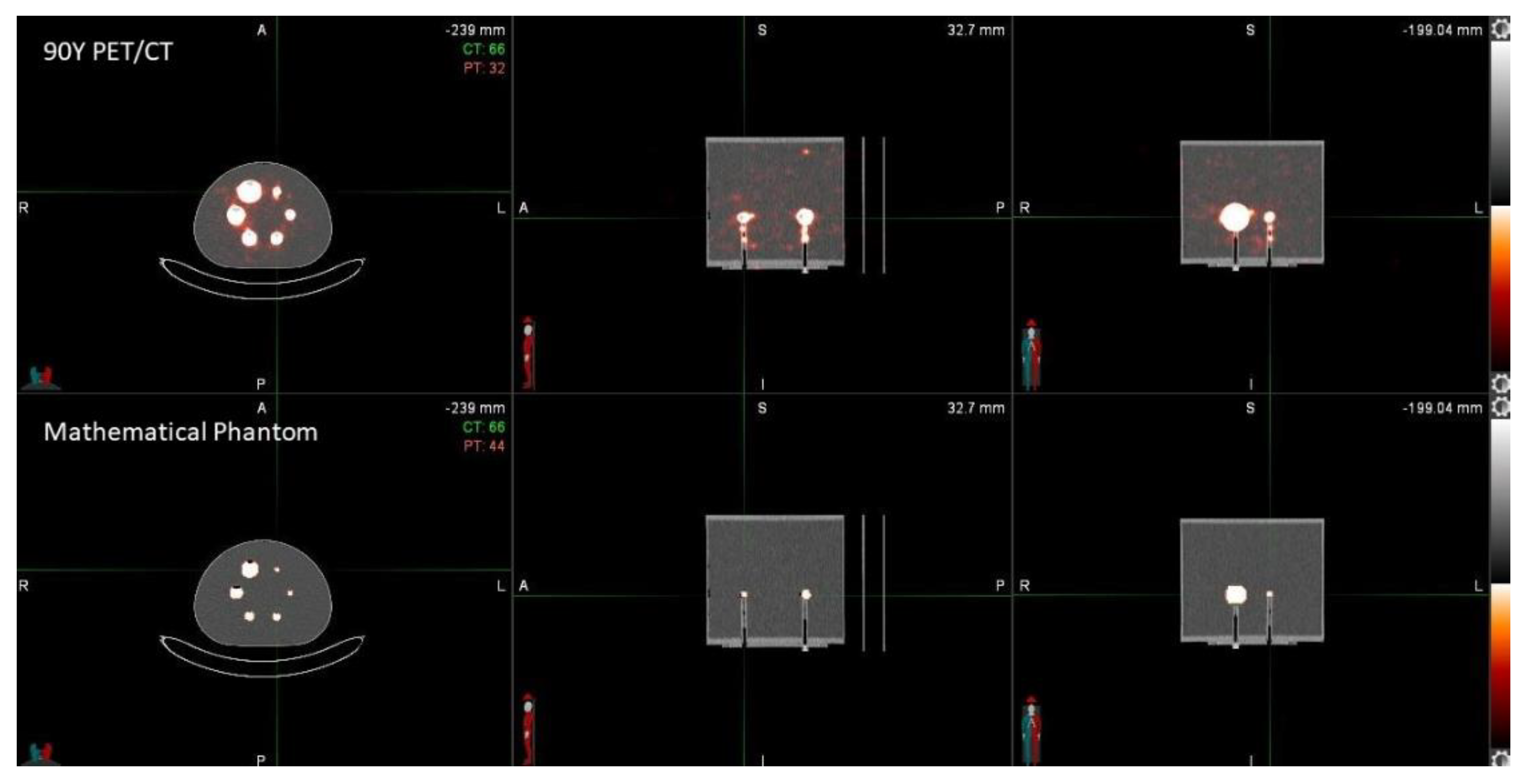
2.1. Data Acquisition, Phantom Description and VOI Segmentation
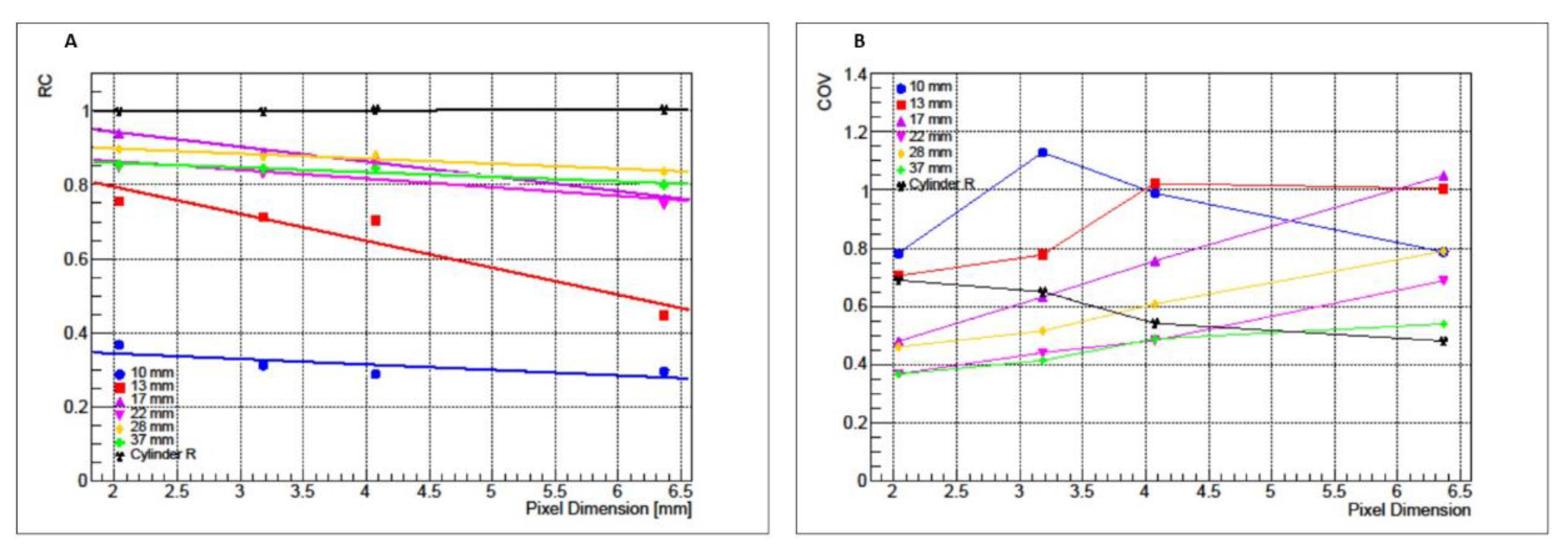
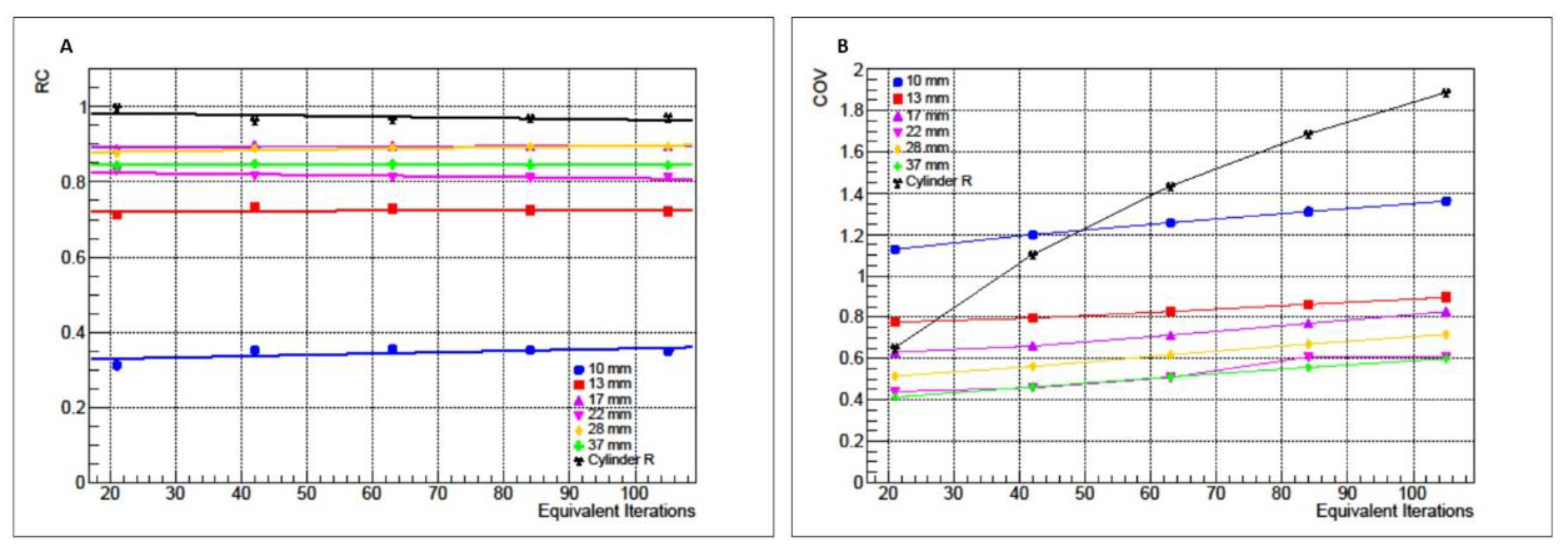
2.2. Matrix Size and Equivalent Iterations Analysis
2.3. Gaussian Filter Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cianni, R.; Urigo, C.; Notarianni, E.; Saltarelli, A.; Salvatori, R.; Pasqualini, V.; Dornbusch, T.; Cortesi, E. Selective internal radiation therapy with SIR-spheres for the treatment of unresectable colorectal hepatic metastases. Cardiovasc. Interv. Radiol. 2009, 32, 1179–1186. [Google Scholar] [CrossRef] [PubMed]
- Salem, R.; Thurston, K.G.; Carr, B.I.; Goin, J.E.; Geschwind, J.F.H. Yttrium-90 microspheres: Radiation therapy for unresectable liver cancer. J. Vasc. Interv. Radiol. 2002, 13, S223–S229. [Google Scholar] [CrossRef]
- Edeline, J.; Touchefeu, Y.; Guiu, B.; Farge, O.; Tougeron, D.; Baumgaertner, I.; Ayav, A.; Campillo-Gimenez, B.; Beuzit, L.; Pracht, M.; et al. Radioembolization plus chemotherapy for first-line treatment of locally advanced intrahepatic cholangiocarcinoma: A phase 2 clinical trial. JAMA Oncol. 2020, 6, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Mulcahy, M.; Salem, R.; Mahvash, A.; Pracht, M.; Montazeri, A.; Bandula, S.; Hermann, K.; Brown, E.; Zuckerman, D.; Wilson, G.; et al. LBA21 Radioembolization with chemotherapy for colorectal liver metastases: A randomized, open-label, international, multicenter, phase III trial (EPOCH study). Ann. Oncol. 2021, 32, S1295. [Google Scholar] [CrossRef]
- Dezarn, W.A.; Cessna, J.T.; DeWerd, L.A.; Feng, W.; Gates, V.L.; Halama, J.; Kennedy, A.S.; Nag, S.; Sarfaraz, M.; Sehgal, V.; et al. Recommendations of the American association of physicists in medicine on dosimetry, imaging, and quality assurance procedures for 90Y microsphere brachytherapy in the treatment of hepatic malignancies. Med. Phys. 2011, 38, 4824–4845. [Google Scholar] [CrossRef]
- Siman, W.; Mikell, J.K.; Kappadath, S. Practical reconstruction protocol for quantitative 90Y bremsstrahlung SPECT/CT. Med. Phys. 2016, 43, 5093–5103. [Google Scholar] [CrossRef]
- Walrand, S.; Hesse, M.; Demonceau, G.; Pauwels, S.; Jamar, F. Yttrium-90-labeled microsphere tracking during liver selective internal radiotherapy by bremsstrahlung pinhole SPECT: Feasibility study and evaluation in an abdominal phantom. EJNMMI Res. 2011, 1, 1–14. [Google Scholar] [CrossRef]
- Yue, J.; Mauxion, T.; Reyes, D.K.; Lodge, M.A.; Hobbs, R.F.; Rong, X.; Dong, Y.; Herman, J.M.; Wahl, R.L.; Geschwind, J.-F.H.; et al. Comparison of quantitative Y-90 SPECT and non-time-of-flight PET imaging in post-therapy radioembolization of liver cancer. Med. Phys. 2016, 43, 5779–5790. [Google Scholar] [CrossRef]
- Selwyn, R.G.; Nickles, R.J.; Thomadsen, B.R.; DeWerd, L.A.; Micka, J.A. A new internal pair production branching ratio of 90Y: The development of a non-destructive assay for 90Y and 90Sr. Appl. Radiat. Isot. 2007, 65, 318–327. [Google Scholar] [CrossRef]
- Wright, C.L.; Binzel, K.; Zhang, J.; Wuthrick, E.J.; Knopp, M.V. Clinical feasibility of 90 Y digital PET/CT for imaging microsphere biodistribution following radioembolization. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 1194–1197. [Google Scholar] [CrossRef]
- Elschot, M.; Vermolen, B.J.; Lam, M.G.; de Keizer, B.; van den Bosch, M.A.; de Jong, H.W. Quantitative comparison of PET and Bremsstrahlung SPECT for imaging the in vivo yttrium-90 microsphere distribution after liver radioembolization. PLoS ONE 2013, 8, e55742. [Google Scholar] [CrossRef] [PubMed]
- Martí-Climent, J.M.; Prieto, E.; Elosúa, C.; Rodríguez-Fraile, M.; Domínguez-Prado, I.; Vigil, C.; García-Velloso, M.J.; Arbizu, J.; Peñuelas, I.; Richter, J.A. PET optimization for improved assessment and accurate quantification of 90Y-microsphere biodistribution after radioembolization. Med. Phys. 2014, 41, 092503. [Google Scholar] [CrossRef]
- Ferrari, P.; Mariotti, F.; De Coste, V.; Capogni, M.; Pimpinella, M.; D’Arienzo, M. Phantom validation of quantitative Y-90 PET/CT-based dosimetry in liver radioembolization. EJNMMI Res. 2017, 7, 94. [Google Scholar]
- Walrand, S.; Hesse, M.; Jamar, F. Update on novel trends in PET/CT technology and its clinical applications. Br. J. Radiol. 2018, 91, 20160534. [Google Scholar] [CrossRef]
- Levillain, H.; Derijckere, I.D.; Marin, G.; Guiot, T.; Vouche, M.; Reynaert, N.; Hendlisz, A.; Vanderlinden, B.; Flamen, P. 90Y-PET/CT-based dosimetry after selective internal radiation therapy predicts outcome in patients with liver metastases from colorectal cancer. EJNMMI Res. 2018, 8, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Alsultan, A.A.; van Roekel, C.; Barentsz, M.W.; Smits, M.L.J.; Kunnen, B.; Koopman, M.; Braat, A.J.; Bruijnen, R.C.; de Keizer, B.; Lam, M.G. Dose-response and dose-toxicity relationships for glass 90Y radioembolization in patients with liver metastases from colorectal cancer. J. Nucl. Med. 2021, 62, 1616–1623. [Google Scholar] [CrossRef] [PubMed]
- Willowson, K.; Forwood, N.; Jakoby, B.W.; Smith, A.M.; Bailey, D.L. Quantitative 90Y image reconstruction in PET. Med. Phys. 2012, 39, 7153–7159. [Google Scholar] [CrossRef] [PubMed]
- Willowson, K.P.; Tapner, M.; Bailey, D.L. A multicentre comparison of quantitative 90 Y PET/CT for dosimetric purposes after radioembolization with resin microspheres. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 1202–1222. [Google Scholar] [CrossRef]
- Carlier, T.; Eugène, T.; Bodet-Milin, C.; Garin, E.; Ansquer, C.; Rousseau, C.; Ferrer, L.; Barbet, J.; Schoenahl, F.; Kraeber-Bodéré, F. Assessment of acquisition protocols for routine imaging of Y-90 using PET/CT. EJNMMI Res. 2013, 3, 1–12. [Google Scholar] [CrossRef]
- Attarwala, A.A.; Molina-Duran, F.; Büsing, K.A.; Schönberg, S.O.; Bailey, D.L.; Willowson, K.; Glatting, G. Quantitative and qualitative assessment of yttrium-90 PET/CT imaging. PLoS ONE 2014, 9, e110401. [Google Scholar] [CrossRef]
- Siman, W.; Mikell, J.K.; Mawlawi, O.R.; Mourtada, F.; Kappadath, S.C. Dose volume histogram-based optimization of image reconstruction parameters for quantitative 90Y-PET imaging. Med. Phys. 2019, 46, 229–237. [Google Scholar] [CrossRef] [PubMed]
- Capogni, M.; Antohe, A. Construction and implementation of a TDCR system at ENEA. Appl. Radiat. Isot. 2014, 87, 260–264. [Google Scholar] [CrossRef] [PubMed]
- Mini, G.; Pepe, F.; Tintori, C.; Capogni, M. A full digital approach to the TDCR method. Appl. Radiat. Isot. 2014, 87, 166–170. [Google Scholar] [CrossRef]
- Broda, R. A review of the triple-to-double coincidence ratio (TDCR) method for standardizing radionuclides. Appl. Radiat. Isot. 2003, 58, 585–594. [Google Scholar] [CrossRef]
- Bolch, W.E.; Bouchet, L.G.; Robertson, J.S.; Wessels, B.W.; Siegel, J.A.; Howell, R.W.; Erdi, A.K.; Aydogan, B.; Costes, S.; Watson, E.E.; et al. MIRD pamphlet no. 17: The dosimetry of nonuniform activity distributions—Radionuclide S values at the voxel level. J. Nucl. Med. 1999, 40, 11S–36S. [Google Scholar]
- Srinivas, S.M.; Natarajan, N.; Kuroiwa, J.; Gallagher, S.; Nasr, E.; Shah, S.N.; DiFilippo, F.P.; A Obuchowski, N.; Bazerbashi, B.; Yu, N.; et al. Determination of radiation absorbed dose to primary liver tumors and normal liver tissue using post-radioembolization 90Y PET. Front. Oncol. 2014, 4, 255. [Google Scholar] [CrossRef] [PubMed]
- Lhommel, R.; van Elmbt, L.; Goffette, P.; Eynde, M.V.D.; Jamar, F.; Pauwels, S.; Walrand, S. Feasibility of 90 Y TOF PET-based dosimetry in liver metastasis therapy using SIR-Spheres. Eur. J. Nucl. Med. Mol. Imaging 2010, 37, 1654–1662. [Google Scholar] [CrossRef]
- Kao, Y.-H.; Steinberg, J.D.; Tay, Y.-S.; Lim, G.K.; Yan, J.; Townsend, D.W.; A Budgeon, C.; A Boucek, J.; Francis, R.J.; Cheo, T.S.; et al. Post-radioembolization yttrium-90 PET/CT-part 2: Dose-response and tumor predictive dosimetry for resin microspheres. EJNMMI Res. 2013, 3, 1–12. [Google Scholar] [CrossRef]
- Kunnen, B.; Beijst, C.; Lam, M.G.E.H.; Viergever, M.A.; De Jong, H.W.A.M. Comparison of the biograph vision and biograph mCT for quantitative 90Y PET/CT imaging for radioembolisation. EJNMMI Phys. 2020, 7, 14. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Capotosti, A.; Moretti, R.; Milano, A.; Nardini, M.; Cusumano, D.; Annunziata, S.; Capogni, M.; D’Arienzo, M.; Placidi, L.; Indovina, L. Up-to-Date Optimization of the 90Y-PET/CT Reconstruction Protocol for Volumetric Quantification in Trans-Arterial RadioEmbolization (TARE) Procedures in the Era of Theranostics. Appl. Sci. 2022, 12, 8418. https://doi.org/10.3390/app12178418
Capotosti A, Moretti R, Milano A, Nardini M, Cusumano D, Annunziata S, Capogni M, D’Arienzo M, Placidi L, Indovina L. Up-to-Date Optimization of the 90Y-PET/CT Reconstruction Protocol for Volumetric Quantification in Trans-Arterial RadioEmbolization (TARE) Procedures in the Era of Theranostics. Applied Sciences. 2022; 12(17):8418. https://doi.org/10.3390/app12178418
Chicago/Turabian StyleCapotosti, Amedeo, Roberto Moretti, Alessia Milano, Matteo Nardini, Davide Cusumano, Salvatore Annunziata, Marco Capogni, Marco D’Arienzo, Lorenzo Placidi, and Luca Indovina. 2022. "Up-to-Date Optimization of the 90Y-PET/CT Reconstruction Protocol for Volumetric Quantification in Trans-Arterial RadioEmbolization (TARE) Procedures in the Era of Theranostics" Applied Sciences 12, no. 17: 8418. https://doi.org/10.3390/app12178418
APA StyleCapotosti, A., Moretti, R., Milano, A., Nardini, M., Cusumano, D., Annunziata, S., Capogni, M., D’Arienzo, M., Placidi, L., & Indovina, L. (2022). Up-to-Date Optimization of the 90Y-PET/CT Reconstruction Protocol for Volumetric Quantification in Trans-Arterial RadioEmbolization (TARE) Procedures in the Era of Theranostics. Applied Sciences, 12(17), 8418. https://doi.org/10.3390/app12178418