
Comparison between Personal Protective Equipment Wearing Protocols to Shorten Time to Treatment in Pre-Hospital Settings



Abstract
:1. Introduction
1.1. Pre-Hospital Setting
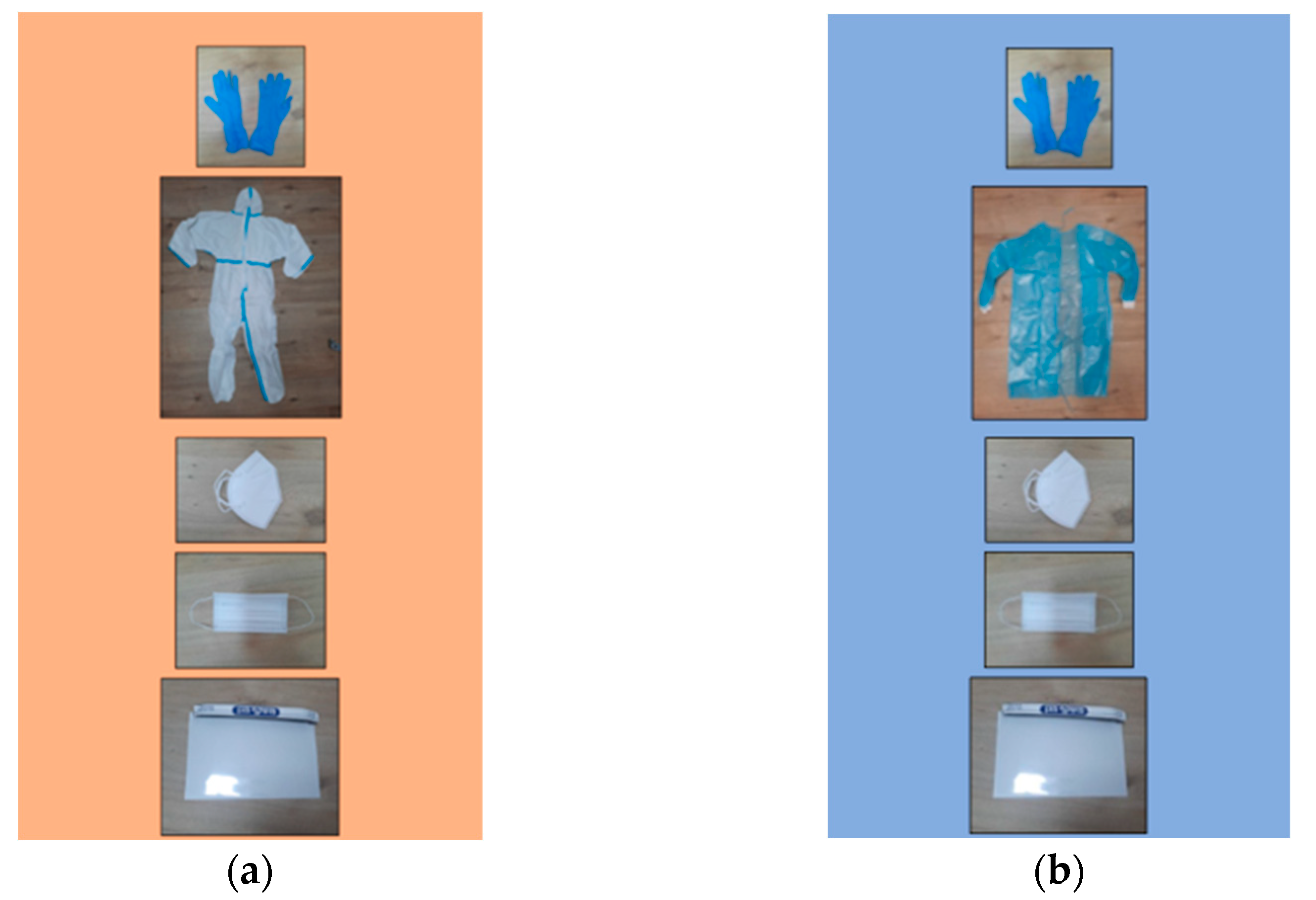
1.2. Personal Protective Equipment
1.3. A New Protective Protocol for EMS Personnel
1.4. Objectives
2. Materials and Methods
2.1. Settings and Intervention
2.2. Sample Size
2.3. Statistical Analysis
3. Results
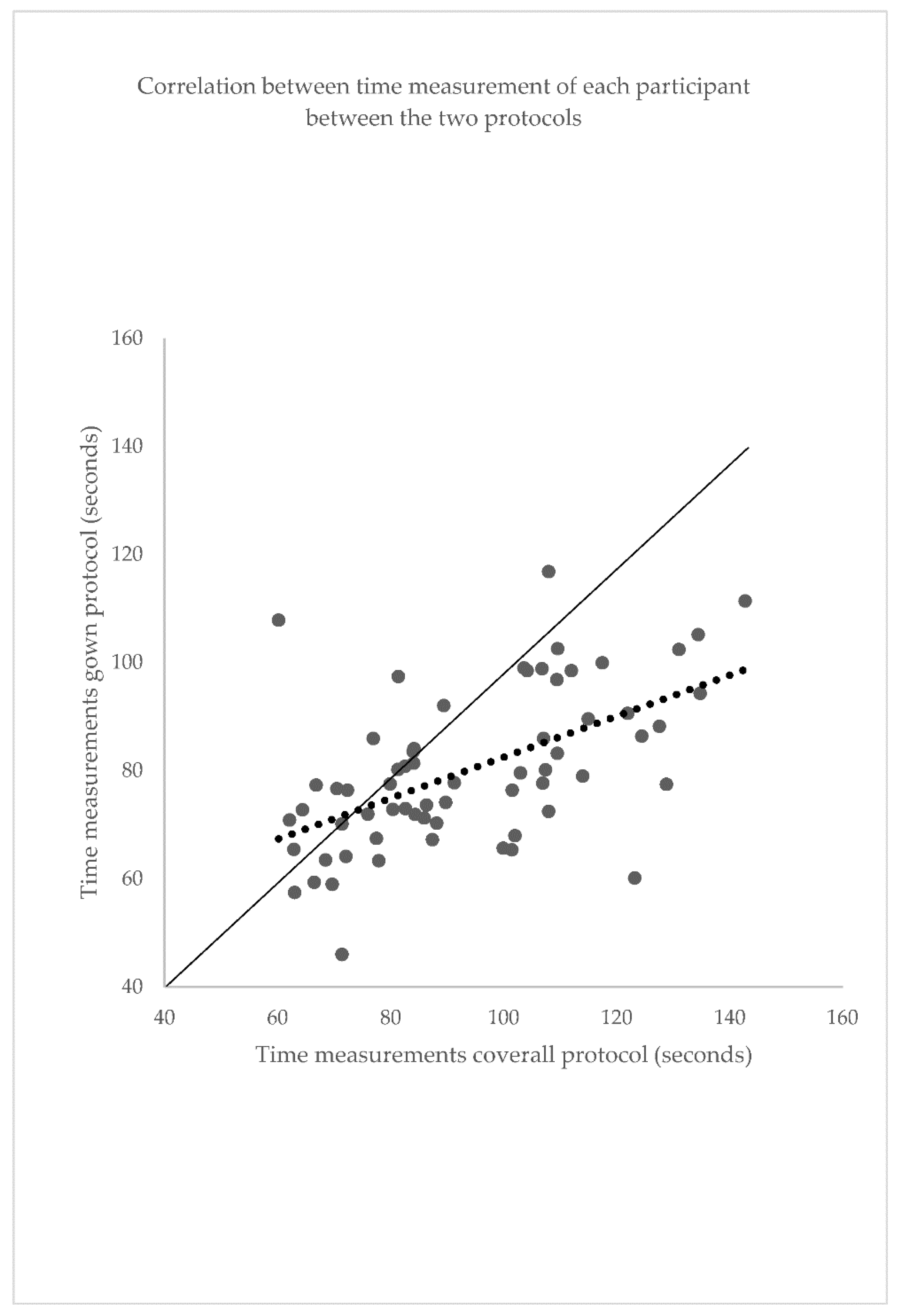
3.1. Comparison of Time Measurements between the Two Protocols: Coverall Protocol and Gown Protocol
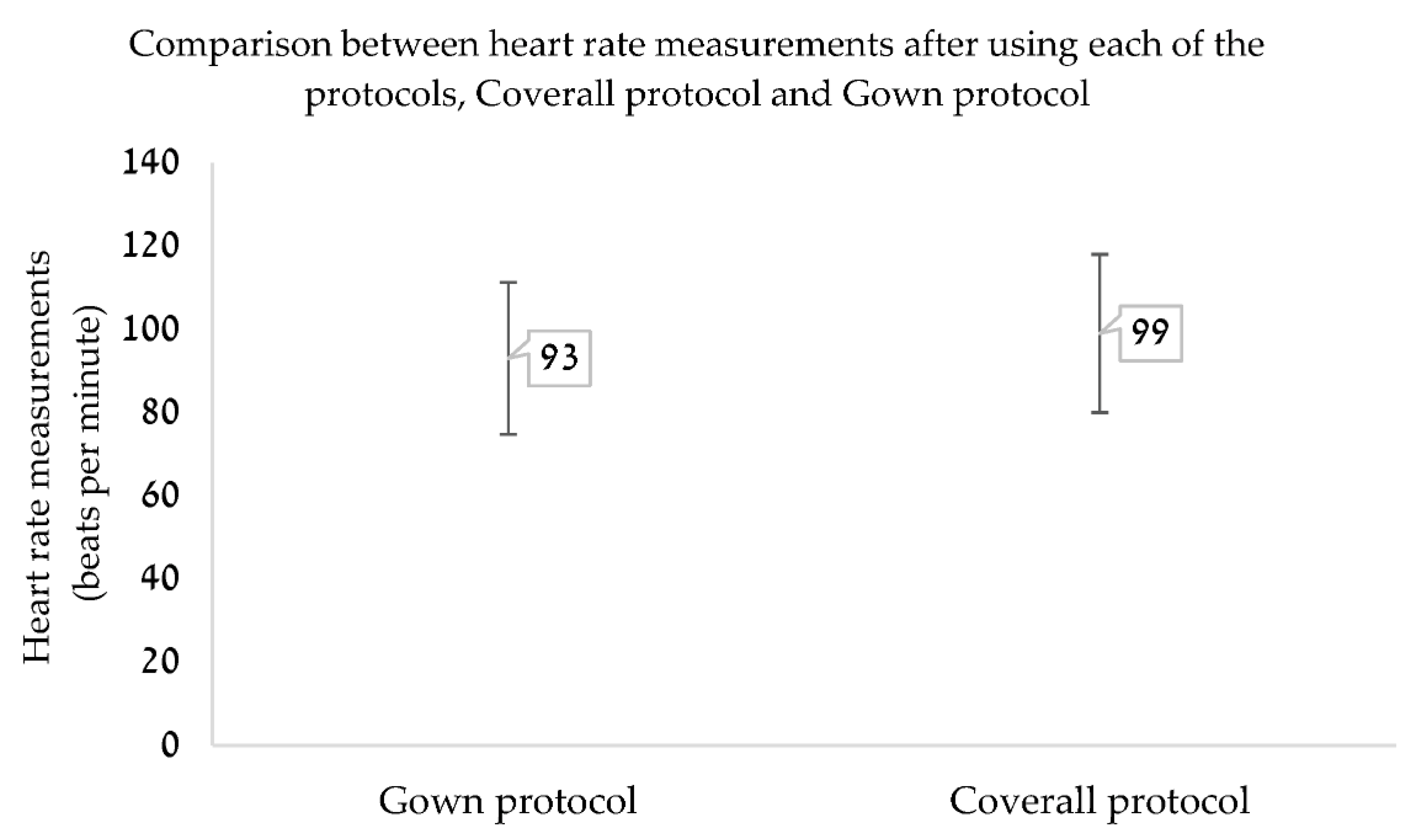
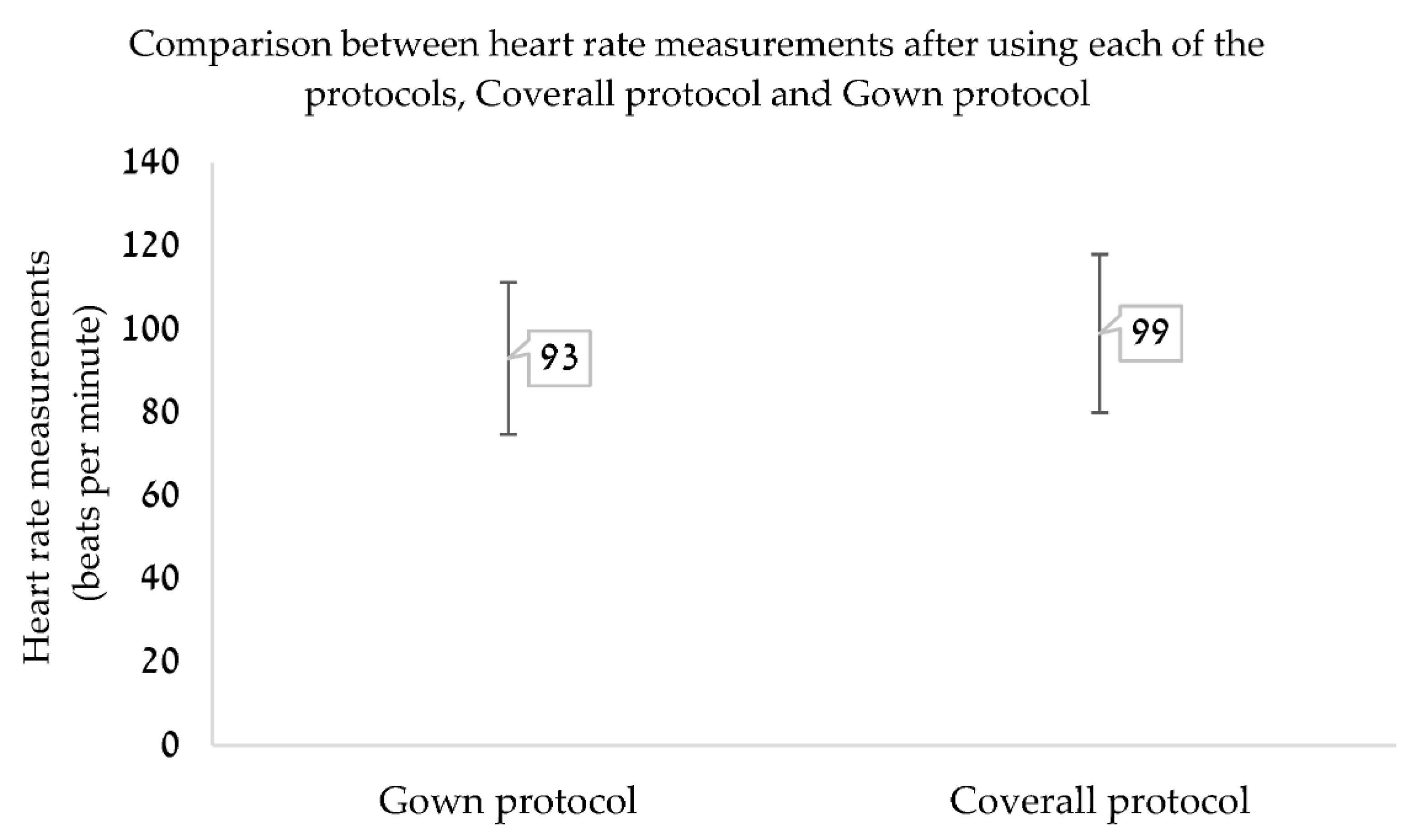
3.2. Heart Rate Measurements
3.3. Comfort Perception
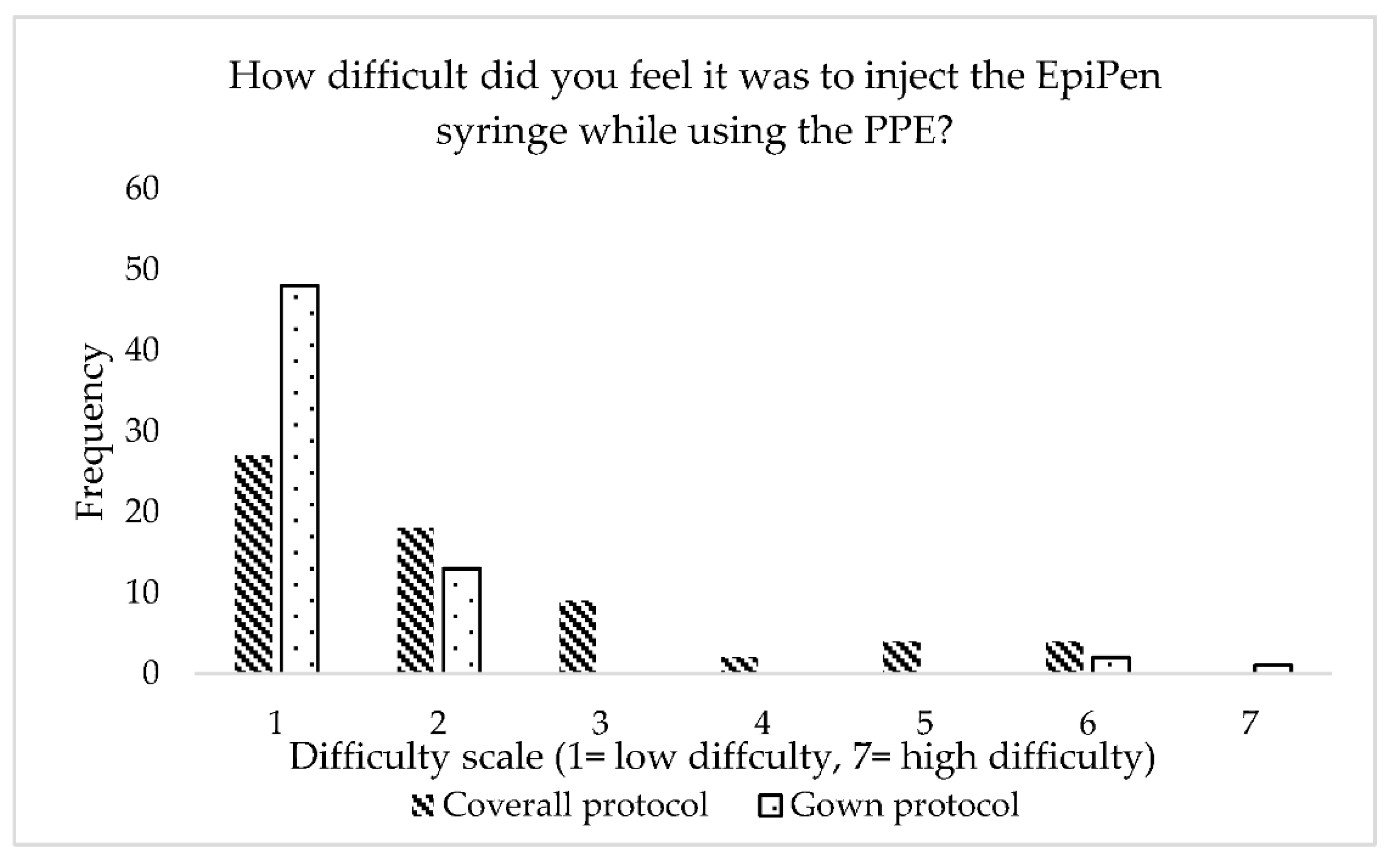
3.4. Difficulty in Providing Medical Care
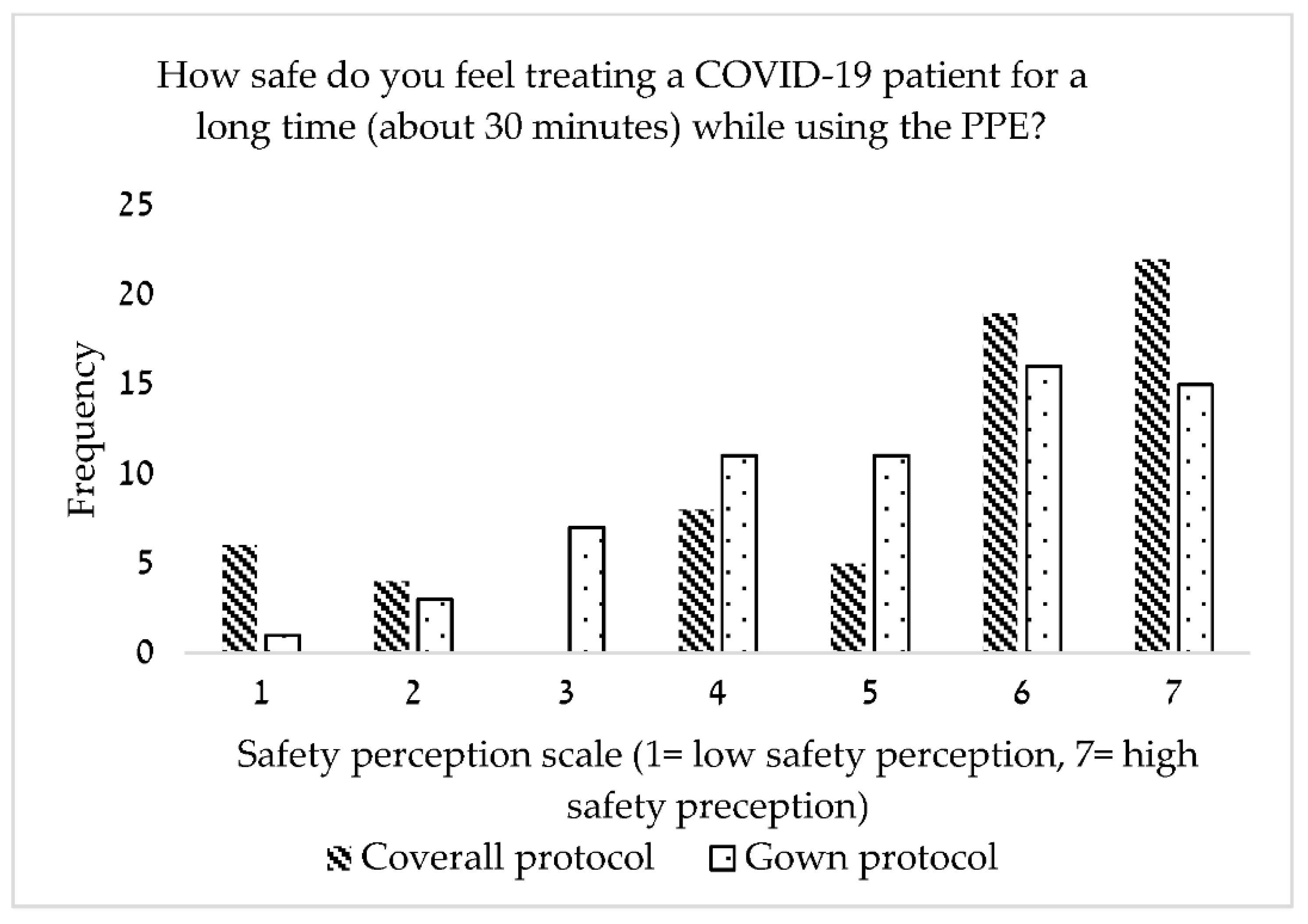
3.5. Safety Perception
4. Discussion
4.1. Duration of PPE Donning and Provision of Primary Medical Treatment: Coverall Protocol and Gown Protocol
4.2. Heart Rate Comparison between the Gown and Coverall Protocols
4.3. Subjective Indicators: Comfort Perceptions, Difficulty in Providing Medical Care, Safety Perceptions
4.3.1. Comfort Perceptions
4.3.2. Difficulty in Providing Medical Treatment
4.3.3. Safety Perceptions
4.3.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ahl, C.; Nyström, M. To handle the unexpected–The meaning of caring in pre-hospital emergency care. Int. Emerg. Nurs. 2011, 20, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Suserud, B.O.; Dahlberg, B.; Dahlberg, K. Initial assessment in ambulance nursing. Part One. Emerg. Nurse 2003, 10, 13–70. [Google Scholar] [PubMed]
- Campbell, J.P.; Gratton, M.C.; Salomone, J.A.; Watson, W.A. Ambulance arrival to patient contact: The hidden component of prehospital response time intervals. Ann. Emerg. Med. 1993, 22, 1254–1257. [Google Scholar] [CrossRef]
- O’Keeffe, C.; Nicholl, J.; Turner, J.; Goodacre, S. Role of ambulance response times in the survival of patients with out-of-hospital cardiac arrest. Emerg. Med. J. 2010, 28, 703–706. [Google Scholar] [CrossRef] [Green Version]
- Magen David Adom Madical Division. Medical Protocols for ALS Units; Magen David Adom: Tel Aviv, Israel, 2016; pp. 7–23. [Google Scholar]
- Magen David Adom Medical Division. Working procedures for ALS units. In Working Procedures, 4th ed.; Magen David Adom: Tel Aviv, Israel, 2016. [Google Scholar]
- Ong, J.J.Y.; Bharatendu, C.; Goh, Y.; Tang, J.Z.Y.; Sooi, K.W.X.; Tan, Y.L.; Tan, B.Y.; Teoh, H.; Ong, S.T.; Allen, D.M.; et al. Headaches Associated With Personal Protective Equipment–A Cross-Sectional Study among Frontline Healthcare Workers During COVID-19. Headache J. Head Face Pain 2020, 60, 864–877. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davey, S.L.; Lee, B.J.; Robbins, T.; Randeva, H.; Thake, C.D. Heat stress and PPE during COVID-19: Impact on healthcare workers’ performance, safety and well-being in NHS settings. J. Hosp. Infect. 2020, 108, 185–188. [Google Scholar] [CrossRef] [PubMed]
- Manivannan, V.; Hyde, R.J.; Hankins, D.G.; Bellolio, F.; Fedko, M.G.; Decker, W.W.; Campbell, R.L. Epinephrine use and outcomes in anaphylaxis patients transported by emergency medical services. Am. J. Emerg. Med. 2014, 32, 1097–1102. [Google Scholar] [CrossRef] [PubMed]
- Magen David Adom Medical Division. COVID-19 outbreak–recommendations for MDA teams. In Working Procedures; Magen David Adom: Tel Aviv, Israel, 2020. [Google Scholar]
- Centers of Disease Control and Prevention [Internet]. COVID-19, Types of Masks and Respirators. Available online: https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/types-of-masks.html (accessed on 8 January 2022).
- Chen, J.; Lu, K.-Z.; Yi, B.; Chen, Y. Chest Compression With Personal Protective Equipment During Cardiopulmonary Resuscitation. Medicine 2016, 95, e3262. [Google Scholar] [CrossRef] [PubMed]
- CDC. Core Infection Prevention and Control Practices for Safe Healthcare Delivery in All Settings–Recommendations of the Healthcare Infection Control Practices Advisory Committee. CDC [Internet]. 2017; pp. 1–15. Available online: https://www.cdc.gov/hicpac/pdf/core-practices.pdf (accessed on 2 August 2022).
- Shekhar, A.C.; Mercer, C.; Blumen, I.; Narula, J. Suboptimal rates of return of spontaneous circulation with prehospital CPR in the COVID-19 era. Resuscitation 2020, 154, 50–51. [Google Scholar] [CrossRef] [PubMed]
- Leblanc, V.R.; Macdonald, R.D.; McArthur, B.; King, K.; Lepine, T. Paramedic Performance in Calculating Drug Dosages Following Stressful Scenarios in a Human Patient Simulator. Prehospital Emerg. Care 2005, 9, 439–444. [Google Scholar] [CrossRef] [PubMed]
- LeBlanc, V.R.; Regehr, C.; Tavares, W.; Scott, A.K.; MacDonald, R.; King, K. The Impact of Stress on Paramedic Performance During Simulated Critical Events. Prehospital Disaster Med. 2012, 27, 369–374. [Google Scholar] [CrossRef] [PubMed]
- Yánez Benítez, C.; Güemes, A.; Aranda, J.; Ribeiro, M.; Ottolino, P.; Saverio, S.D.; Alexandrino, H.; Ponchietti, L.; Blas, J.; International Cooperation Group on PPE and Emergency Surgery; et al. Impact of personal protective equipment on surgical performance during the COVID-19 pandemic. World J. Surg. 2020, 44, 2842–2847. [Google Scholar] [CrossRef] [PubMed]
- Nirel, N.; Goldwag, R.; Feigenberg, Z.; Abadi, D.; Halpern, P. Stress, Work Overload, Burnout, and Satisfaction among Paramedics in Israel. Prehospital Disaster Med. 2008, 23, 537–546. [Google Scholar] [CrossRef] [Green Version]
- Hegde, S. Which type of personal protective equipment (PPE) and which method of donning or doffing PPE carries the least risk of infection for healthcare workers? Evid.-Based Dent. 2020, 21, 74–76. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.; Salahuddin, M.; Gibson-Young, L.; Oliver, G.D. Assessing personal protective equipment needs for healthcare workers. Health Sci. Rep. 2021, 4, e370. [Google Scholar] [CrossRef]
- Delgado, D.; Quintana, F.W.; Perez, G.; Sosa Liprandi, A.; Ponte-Negretti, C.; Mendoza, I.; Baranchuk, A. Personal Safety during the COVID-19 Pandemic: Realities and Perspectives of Healthcare Workers in Latin America. Int. J. Environ. Res. Public Health 2020, 17, 2798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Acharya, S.; Ghimire, A.; Dongol, D.; Maharjan, K. Non-COVID and COVID emergency department healthcare workers’ perception of COVID-19 at Patan Hospital, Nepal. J. Patan Acad. Health Sci. 2020, 7, 42–47. [Google Scholar] [CrossRef]
- Morawska, L.; Milton, D.K. Its time to address airbone transmission of COVID-19. Clin. Infect. Dis. 2020, 71, 2311–2313. [Google Scholar] [PubMed]
- The Lancet Respiratory Medicine. COVID-19 transmission—Up in the air. Lancet Respir. Med. 2020, 8, 1159. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Type | Main Indices |
|---|---|---|
| Age | Quantitative continuous | Mean = 25.08 +/− 2.797 Median = 25 years (range 18, 31) |
| Gender | Qualitative dichotomous | Female = 51.6% Male = 48.4% |
| Academic program | Qualitative nominal | School of Emergency Medicine = 73.4%, School of Nursing = 6.3%, School of Medicine = 14.1%, graduate program = 6.3% |
| Academic year | Quantitative discrete | Median = 2nd year (IQR 25% = 2, 50% = 2, 75% = 3; range 1, 6) first year = 14.1%, second year = 46.9%, third year = 28.1%, fourth year = 6.3%, fifth year = 1.6%, sixth year = 3.1% |
| Had the participant taken a first-aid course in the past? | Qualitative dichotomous | Yes = 100% |
| Had the participant used PPE in the past? | Qualitative dichotomous | Yes = 92.2% No = 7.8% |
| Had the participant used an EpiPen injector in the past? | Qualitative dichotomous | Yes = 64.1% No = 35.9% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lavi, O.; Wacht, O.; Menashe, I.; Jaffe, E.; Bitan, Y. Comparison between Personal Protective Equipment Wearing Protocols to Shorten Time to Treatment in Pre-Hospital Settings. Appl. Sci. 2022, 12, 7926. https://doi.org/10.3390/app12157926
Lavi O, Wacht O, Menashe I, Jaffe E, Bitan Y. Comparison between Personal Protective Equipment Wearing Protocols to Shorten Time to Treatment in Pre-Hospital Settings. Applied Sciences. 2022; 12(15):7926. https://doi.org/10.3390/app12157926
Chicago/Turabian StyleLavi, Or, Oren Wacht, Idan Menashe, Eli Jaffe, and Yuval Bitan. 2022. "Comparison between Personal Protective Equipment Wearing Protocols to Shorten Time to Treatment in Pre-Hospital Settings" Applied Sciences 12, no. 15: 7926. https://doi.org/10.3390/app12157926
APA StyleLavi, O., Wacht, O., Menashe, I., Jaffe, E., & Bitan, Y. (2022). Comparison between Personal Protective Equipment Wearing Protocols to Shorten Time to Treatment in Pre-Hospital Settings. Applied Sciences, 12(15), 7926. https://doi.org/10.3390/app12157926