
Perception of Professionals from Different Healthcare Units Regarding the Use of Spray Technology for the Instantaneous Decontamination of Personal Protective Equipment during the Coronavirus Disease Pandemic: A Short Analysis

 , ,
, ,
Abstract
:Featured Application
Abstract

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Introduction
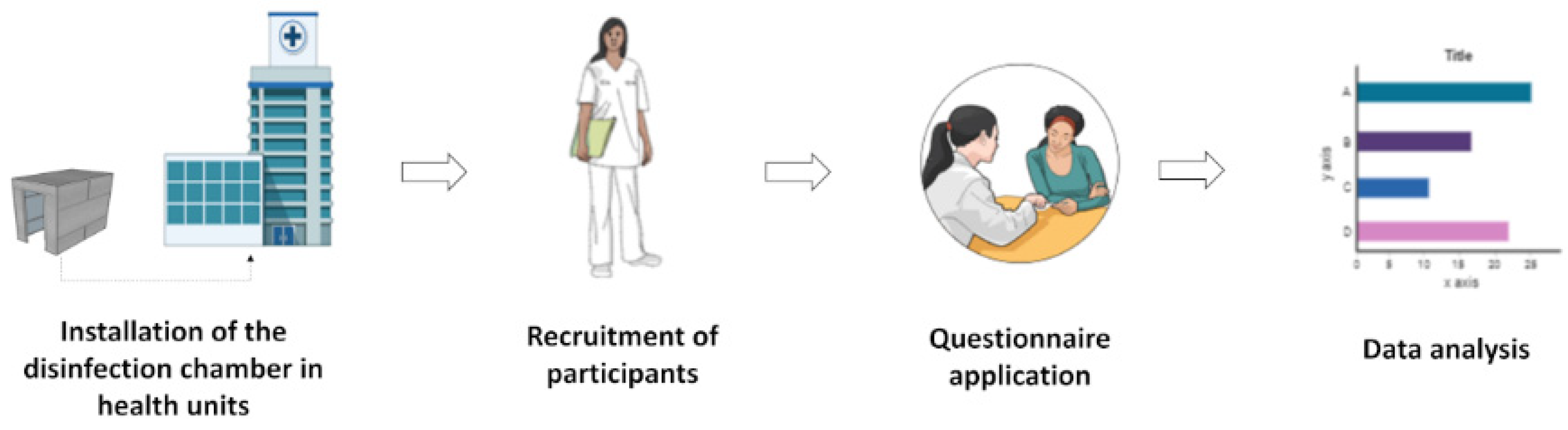
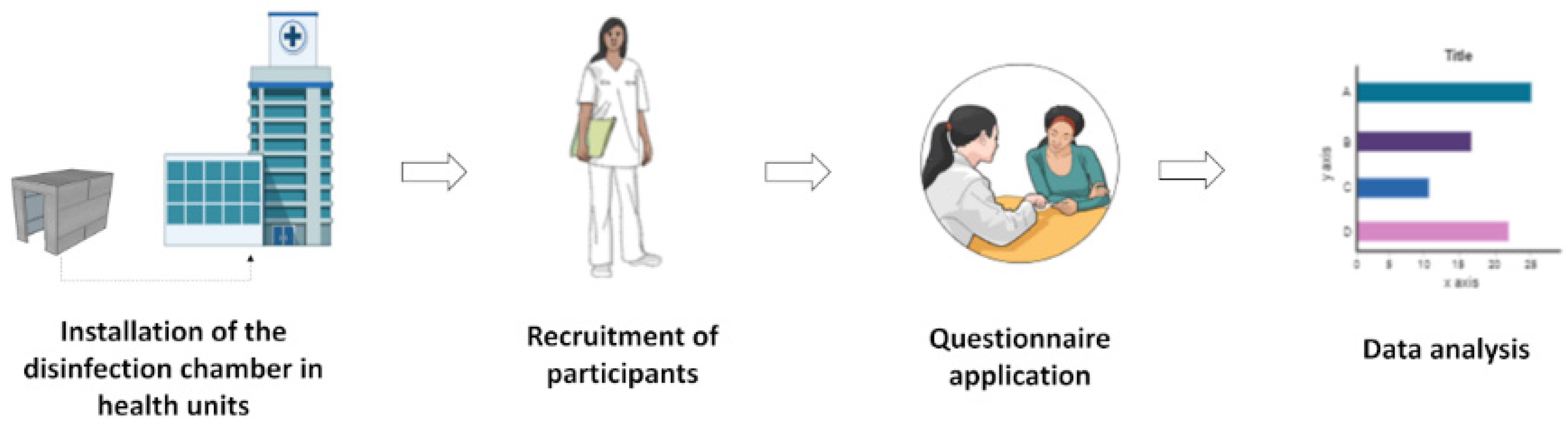
2. Materials and Methods
2.1. Installation of the Disinfection Chamber in Hospitals and Reference Healthcare Units Designated for the Treatment of COVID-19
2.2. Study Design
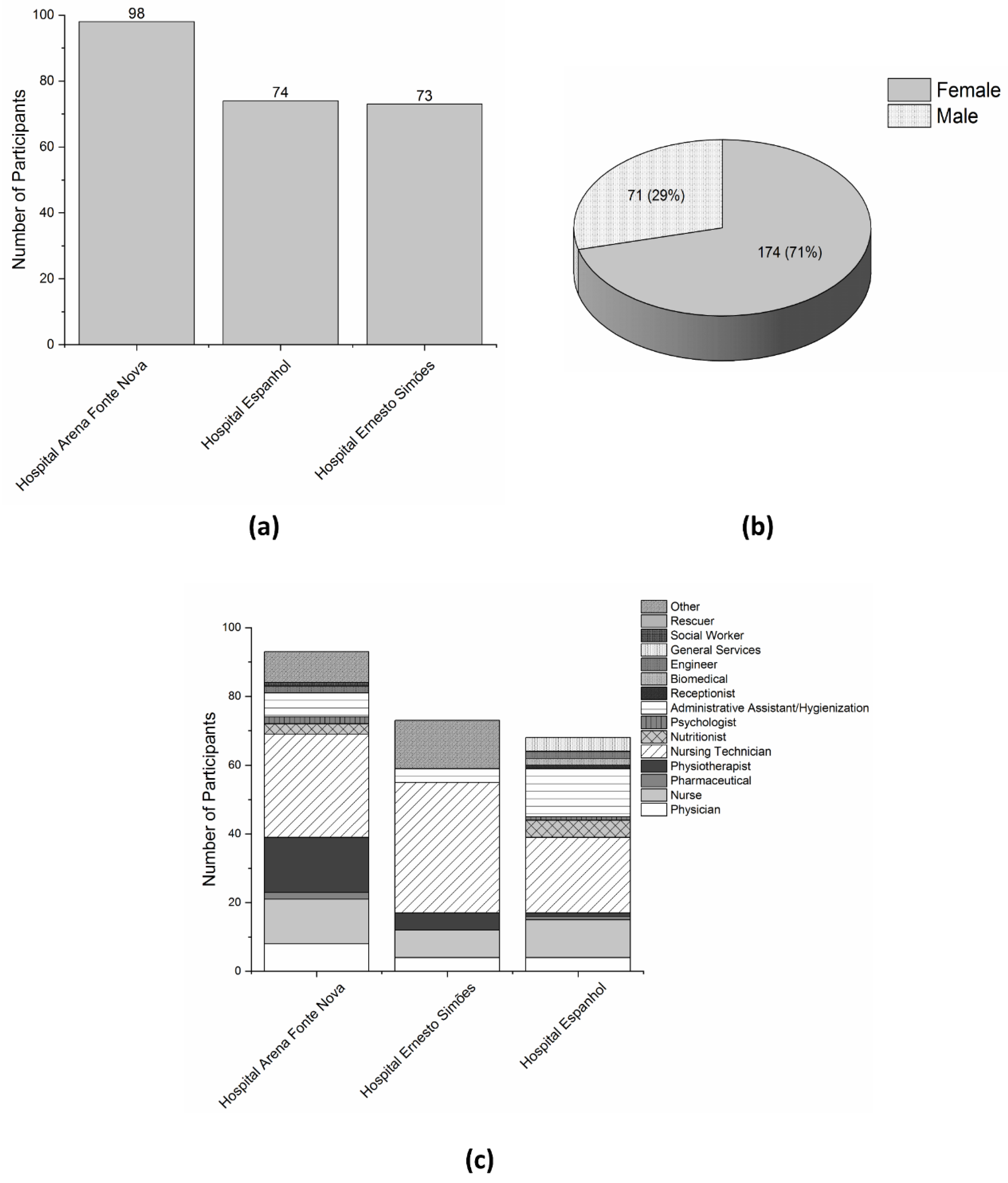
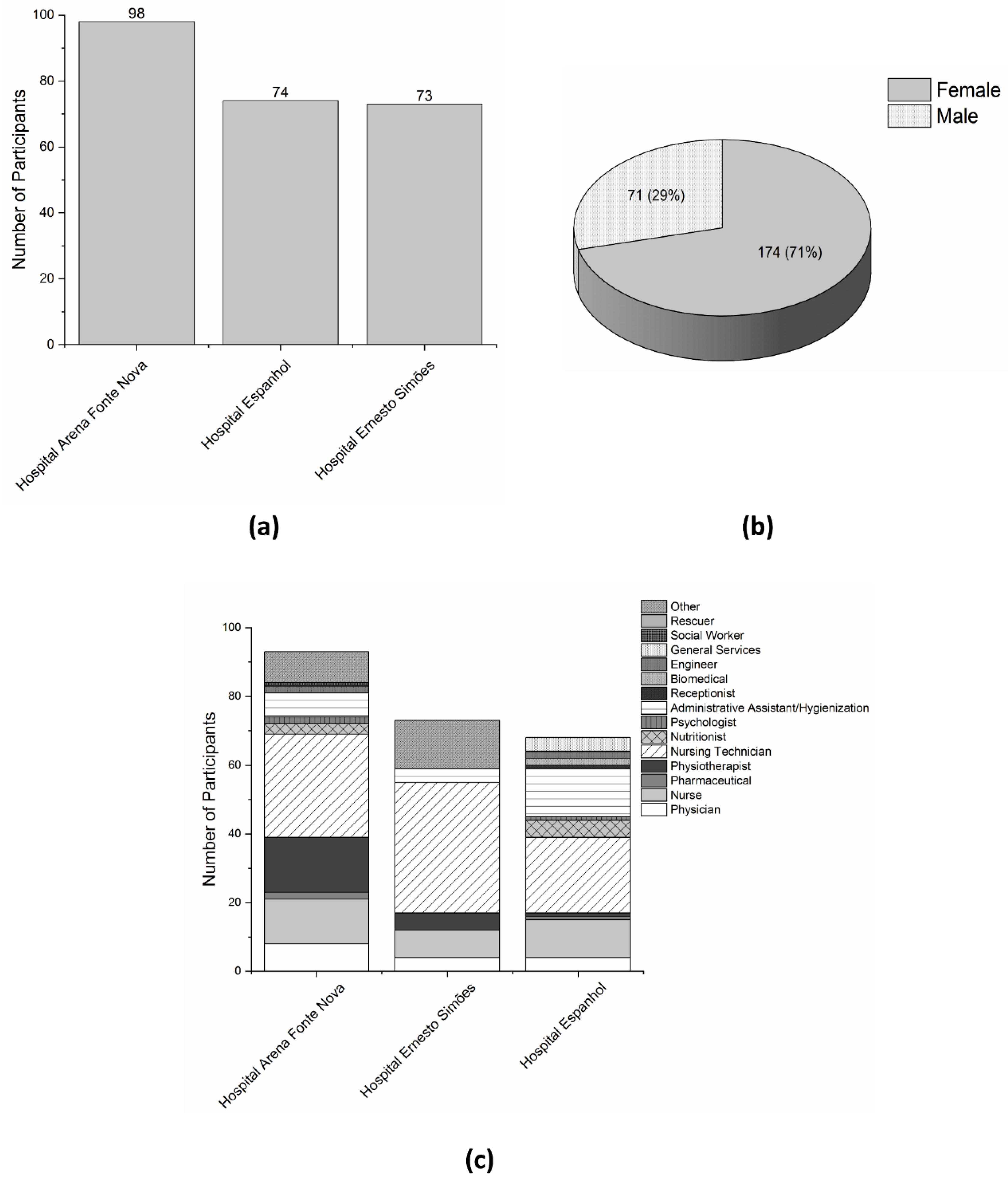
2.3. Survey Population
2.4. Data Collection (Questionnaire Development and Application)
- What is your occupation?
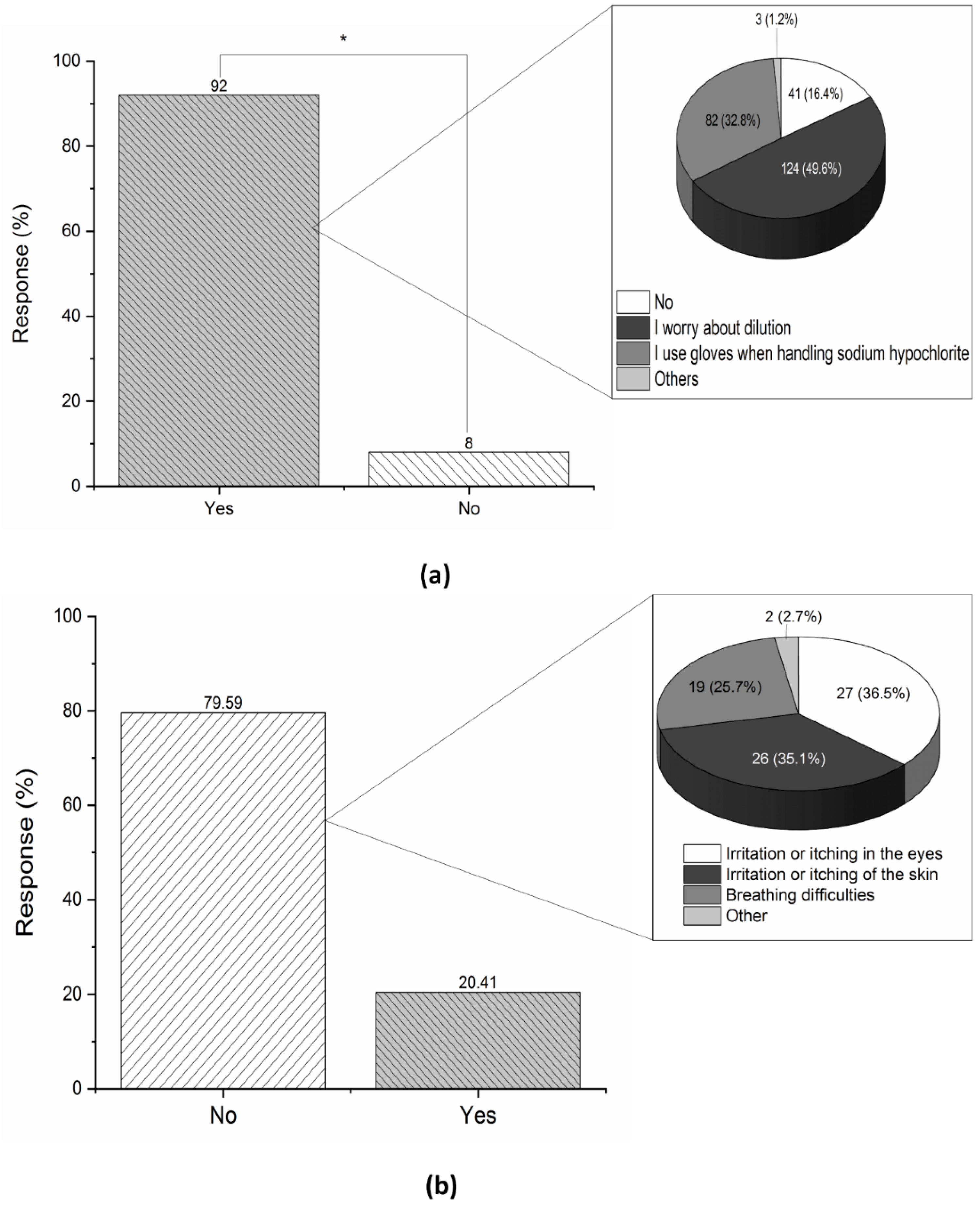
- Do you use sodium hypochlorite to clean/disinfect surfaces in your home?
- If the answer to the previous question was yes, do you take any precautions when handling sodium hypochlorite?
- Have you experienced any type of prior adverse reaction to sodium hypochlorite in previous contact? If yes, please indicate the type(s) of reaction(s).
- Do you consider that sodium hypochlorite is a good disinfectant?
- Did you know that sodium hypochlorite (0.1% to 0.5%) is effective for the inactivation of the new coronavirus (SARS-CoV-2), and is recommended by the World Health Organization (WHO) for the disinfection of home and hospital environments?
- Did you know that a sodium hypochlorite solution is used in the chamber for the instantaneous disinfection of Personal Protective Equipment (PPE)?
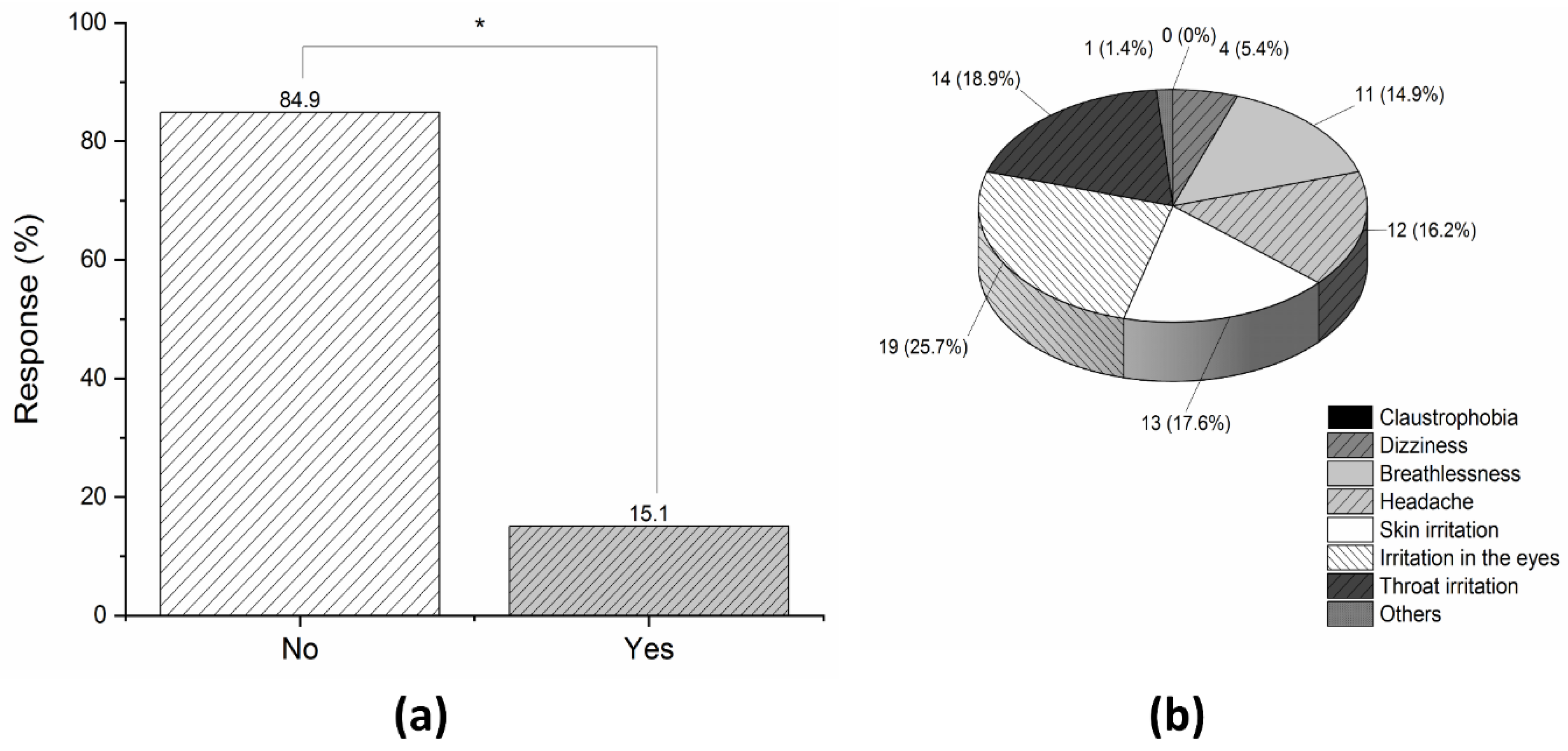
- Did you experience any discomfort when using the disinfection chamber? If yes, please indicate the discomfort(s) you felt and specify the degree of irritation.
- Did you know that the chamber was developed to reduce the microbial load, including that of SARS-CoV-2, on the surface of PPE?
- Do you consider the use of the disinfection chamber before the PPE doffing process to be a safe alternative? If you answered NO to the previous question, why do you not find it to be a safe alternative?
- Did you check that all of the PPE was uniformly humidified after using the chamber?
- Do you consider the disinfection chamber to be effective as an additional protective barrier for healthcare workers?
- Do you consider that the use of the disinfection chamber can lead to a false sense of safety? If you answered YES to the previous question, why do you think using the disinfection chamber leads to a false sense of security?
- Did you know that even with the use of the chamber, all PPE doffing procedures and protocols must be followed strictly?
- After using the chamber, have you followed all the appropriate procedures for the doffing of the PPE?
- Do you have any remarks or comments you want to add about the chamber?
2.5. Data Analysis
2.6. Ethics Approval and Consent to Participate
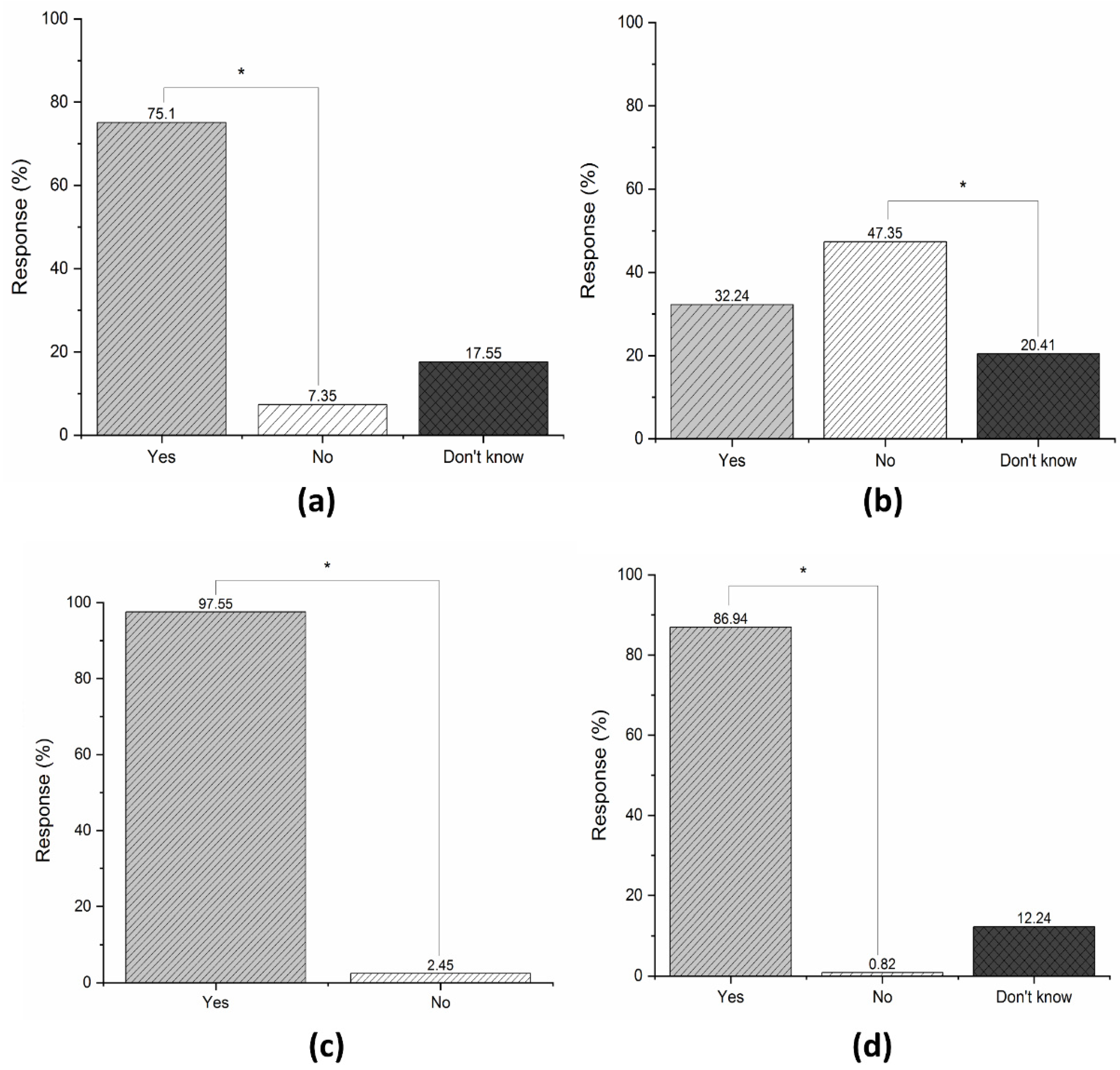
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lineback, C.B.; Nkemngong, C.A.; Wu, S.T.; Li, X.; Teska, P.J.; Oliver, H.F. Hydrogen peroxide and sodium hypochlorite disinfectants are more effective against Staphylococcus aureus and Pseudomonas aeruginosa biofilms than quaternary ammonium compounds. Antimicrob. Resist. Infect. Control 2018, 7, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Quinn, M.M.; Henneberger, P.K.; Braun, B.; Delclos, G.L.; Fagan, K.; Huang, V.; Knaack, J.L.S.; Kusek, L.; Lee, S.J.; Le Moual, N.; et al. Cleaning and disinfecting environmental surfaces in health care: Toward an integrated framework for infection and occupational illness prevention. Am. J. Infect. Control 2015, 43, 424–434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cadnum, J.L.; Jencson, A.L.; Livingston, S.H.; Li, D.; Redmond, S.N.; Pearlmutter, B.; Wilson, B.M.; Donskey, C.J. Evaluation of an Electrostatic Spray Disinfectant Technology for Rapid Decontamination of Portable Equipment and Large Open Areas in the Era of SARS-CoV-2. Am. J. Infect. Control 2020, 48, 951–954. [Google Scholar] [CrossRef]
- Hardy, K.J.; Szczepura, A.; Davies, R.; Bradbury, A.; Stallard, N.; Gossain, S.; Walley, P.; Hawkey, P.M. A study of the efficacy and cost-effectiveness of MRSA screening and monitoring on surgical wards using a new, rapid molecular test (EMMS). BMC Health Serv. Res. 2007, 7, 160. [Google Scholar] [CrossRef] [Green Version]
- Medeiros, M.A.P.; de Melo, A.P.V.; de Oliveira Bento, A.; de Souza, L.B.F.C.; de Assis Bezerra Neto, F.; Garcia, J.B.L.; Zuza-Alves, D.L.; Francisco, E.C.; de Azevedo Melo, A.S.; Chaves, G.M. Epidemiology and prognostic factors of nosocomial candidemia in Northeast Brazil: A six-year retrospective study. PLoS ONE 2019, 14, e0221033. [Google Scholar] [CrossRef] [PubMed]
- Fong, M.W.; Leung, N.H.L.; Xiao, J.; Chu, D.K.W.; Cheng, S.M.S.; So, H.C.; Li, Y.; Ip, D.K.M.; Peiris, J.S.M.; Cowling, B.J. Presence of Influenza Virus on Touch Surfaces in Kindergartens and Primary Schools. J. Infect. Dis. 2020, 222, 1329–1333. [Google Scholar] [CrossRef] [PubMed]
- Ranjan, K. Environmental Persistence of SARS-CoV-2 and Disinfection of Work Surfaces in View of Pandemic Outbreak of COVID-19. In Disinfection of Viruses; IntechOpen: London, UK, 2022; ISBN 978-1-83962-416-2. [Google Scholar]
- Lu, H.; Stratton, C.W.; Tang, Y. Outbreak of pneumonia of unknown etiology in Wuhan, China: The mystery and the miracle. J. Med. Virol. 2020, 92, 401–402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, A.L.; Millet, J.K.; Daniel, S.; Freed, J.H.; Whittaker, G.R. Rapid viral diagnosis and ambulatory management of suspected COVID-19 cases presenting at the infectious diseases referral hospital in Marseille, France,—January 31st to March 1st, 2020: A respiratory virus snapshot. Travel Med. Infect. Dis. 2020, 36, 101632. [Google Scholar]
- WHO. WHO Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 12 July 2022).
- Machado, B.A.S.; Hodel, K.V.S.; dos Santos Fonseca, L.M.; Pires, V.C.; Mascarenhas, L.A.B.; da Silva Andrade, L.P.C.; Moret, M.A.; Badaró, R. The Importance of Vaccination in the Context of the COVID-19 Pandemic: A Brief Update Regarding the Use of Vaccines. Vaccines 2022, 10, 591. [Google Scholar] [CrossRef]
- Machado, B.A.S.; Hodel, K.V.S.; dos Santos Fonseca, L.M.; Mascarenhas, L.A.B.; da Silva Andrade, L.P.C.; Rocha, V.P.C.; Soares, M.B.P.; Berglund, P.; Duthie, M.S.; Reed, S.G.; et al. The Importance of RNA-Based Vaccines in the Fight against COVID-19: An Overview. Vaccines 2021, 9, 1345. [Google Scholar] [CrossRef]
- Llanes, A.; Restrepo, C.M.; Caballero, Z.; Rajeev, S.; Kennedy, M.A.; Lleonart, R. Betacoronavirus Genomes: How Genomic Information has been Used to Deal with Past Outbreaks and the COVID-19 Pandemic. Int. J. Mol. Sci. 2020, 21, 4546. [Google Scholar] [CrossRef] [PubMed]
- Silva, D.F.; Toledo Neto, J.L.; Machado, M.F.; Bochnia, J.R.; Garcez, A.S.; Foggiato, A.A. Effect of photodynamic therapy potentiated by ultrasonic chamber on decontamination of acrylic and titanium surfaces. Photodiagnosis Photodyn. Ther. 2019, 27, 345–353. [Google Scholar] [CrossRef] [PubMed]
- Ning, P.; Shan, D.; Hong, E.; Liu, L.; Zhu, Y.; Cui, R.; Zhou, Y.; Wang, B. Disinfection performance of chlorine dioxide gas at ultra-low concentrations and the decay rules under different environmental factors. J. Air Waste Manag. Assoc. 2020, 70, 721–728. [Google Scholar] [CrossRef] [PubMed]
- Gardam, M.; McGeer, A.; Mertz, D. Portable ultraviolet light surface-disinfecting devices for prevention of hospital-acquired infections: A health technology assessment. Ont. Health Technol. Assess. Ser. 2018, 18, 1. [Google Scholar]
- Rezaieid, A.; Leite, G.G.S.; Melmed, G.Y.; Mathur, R.; Jesus Villanueva-Millan, M.; Parodi, G.; Sin, J.; Germano, J.F.; Morales, W.; Weitsman, S.; et al. Ultraviolet A light effectively reduces bacteria and viruses including coronavirus. PLoS ONE 2020, 15, e0236199. [Google Scholar] [CrossRef]
- Ishikawa, S.; Ueno, S.; Mitsui, M.; Matsumura, Y.; Hatsuoka, T. Construction of its evaluation system in originally designed test-chamber system and sporicidal activity of aerosolized hypochlorite solution to bacillus subtilis spores. Biocontrol Sci. 2019, 24, 57–65. [Google Scholar] [CrossRef] [Green Version]
- Rothe, C.; Schunk, M.; Sothmann, P.; Bretzel, G.; Froeschl, G.; Wallrauch, C.; Zimmer, T.; Thiel, V.; Janke, C.; Guggemos, W.; et al. Transmission of 2019-nCoV Infection from an Asymptomatic Contact in Germany. N. Engl. J. Med. 2020, 382, 970–971. [Google Scholar] [CrossRef] [Green Version]
- Álvarez-Pomar, L.; Rojas-Galeano, S. Impact of Personal Protection Habits on the Spread of Pandemics: Insights from an Agent-Based Model. Sci. World J. 2021, 2021, 6616654. [Google Scholar] [CrossRef]
- Kim, D.K.; Kang, D.H. UVC LED irradiation effectively inactivates aerosolized viruses, bacteria, and fungi in a chamber-type air disinfection system. Appl. Environ. Microbiol. 2018, 84, e00944-18. [Google Scholar] [CrossRef] [Green Version]
- Wickramatillake, A.; Kurukularatne, C. SARS-CoV-2 human disinfection chambers: A critical analysis. Occup. Med. 2020, 70, 330–334. [Google Scholar] [CrossRef] [PubMed]
- OPDD Critical Equipment and Technologies Developed by DRDO for Combating COVID19 Pandemic. Available online: https://www.drdo.gov.in/sites/default/files/whats_new_document/attach2.pdf (accessed on 9 June 2020).
- Dadlani, D. COVID-19: Dubai Silicon Oasis Authority Develops Disinfection Tunnel. Available online: https://www.constructionweekonline.com/products-and-services/264707-covid-19-dubai-silicon-oasis-authority-develops-disinfection-tunnel (accessed on 14 August 2020).
- Lee, Z. Disinfection Tunnels Built to Clean People within 20 s Amid Coronavirus Outbreak. Available online: https://www.scmp.com/video/china/3051038/disinfection-tunnels-built-clean-people-within-20-seconds-amid-coronavirus (accessed on 14 August 2020).
- Último Segundo iG. Cidade Cria “Túnel de Desinfecção” Para Combater Covid-19. Available online: https://ultimosegundo.ig.com.br/2020-04-09/cidade-cria-tunel-de-desinfeccao-para-combater-covid-19.html (accessed on 14 August 2020).
- Mascarenhas, L.A.B.; Oliveira, F.O.; da Silva, E.S.; dos Santos, L.M.C.; de Alencar Pereira Rodrigues, L.; Neves, P.R.F.; Santos, A.Á.B.; Moreira, G.A.F.; Lobato, G.M.; Nascimento, C.; et al. Technological Advances in Ozone and Ozonized Water Spray Disinfection Devices. Appl. Sci. 2021, 11, 3081. [Google Scholar] [CrossRef]
- Mehtar, S.; Bulabula, A.N.H.; Nyandemoh, H.; Jambawai, S. Deliberate exposure of humans to chlorine-the aftermath of Ebola in West Africa. Antimicrob. Resist. Infect. Control 2016, 5, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anvisa NOTA TÉCNICA No 38/2020/SEI/COSAN/GHCOS/DIRE3/ANVISA. Available online: https://sei.anvisa.gov.br/sei/controlador.php?acao=documento_imprimir_web&acao_origem=arvore_visualizar&id_documento=1118935&infra_sis…1/5 (accessed on 5 August 2020).
- DIVISA PORTARIA DIVISA No 002, DE 25 DE MAIO DE 2020. Available online: http://www.saude.ba.gov.br/wp-content/uploads/2020/05/PORTARIA-DIVISA-N°-002-2020-DE-25-DE-MAIO-DE-2020.pdf (accessed on 30 August 2020).
- Kim, S.W.; Sung, J.J.; Lee, H.; Oh, J.H.; Lim, J.; Lee, S.H.; Choi, J.H.; Leeid, J. Containment of a healthcare-associated COVID-19 outbreak in a university hospital in Seoul, Korea: A single-center experience. PLoS ONE 2020, 15, e0237692. [Google Scholar] [CrossRef] [PubMed]
- Batista, R.C.S.; Arruda, C.V.B.; Cassimiro, M.; Gominho, L.; Moura, A.C.; Albuquerque, D.S.; Romeiro, K. The Role of the Dental Surgeon in Controlling the Dissemination of COVID-19: A Literature Review. Sci. World J. 2020, 2020, 7945309. [Google Scholar] [CrossRef]
- West, A.M.; Teska, P.J.; Lineback, C.B.; Oliver, H.F. Strain, disinfectant, concentration, and contact time quantitatively impact disinfectant efficacy. Antimicrob. Resist. Infect. Control 2018, 7, 49. [Google Scholar] [CrossRef]
- Ryu, B.-H.; Cho, Y.; Cho, O.-H.; In, S.; Md, H.; Kim, S.; Lee, S. Environmental contamination of SARS-CoV-2 during the COVID-19 outbreak in South Korea. Am. J. Infect. Control 2020, 48, 875–879. [Google Scholar] [CrossRef]
- Petersen, E.; Hui, D.; Hamer, D.H.; Blumberg, L.; Madoff, L.C.; Pollack, M.; Shan Lee, S.; McLellan, S.; Memish, Z.; Praharaj, I.; et al. Li Wenliang, a face to the frontline healthcare worker. The first doctor to notify the emergence of the SARS-CoV-2, (COVID-19), outbreak. Int. J. Infect. Dis. 2020, 93, 205–207. [Google Scholar] [CrossRef]
- Qi, B.; Peng, H.; Shou, K.; Pan, Z.; Zhou, M.; Li, R.; Deng, L.; Shen, J.; Rao, X.; Yu, A. Protecting Healthcare Professionals during the COVID-19 Pandemic. BioMed Res. Int. 2020, 2020, 8469560. [Google Scholar] [CrossRef]
- Felice, C.; Luca, G.; Tanna, D.; Zanus, G.; Grossi, U. Impact of COVID-19 Outbreak on Healthcare Workers in Italy: Results from a National E-Survey. J. Community Health 2020, 45, 675–683. [Google Scholar] [CrossRef]
- Kursumovic, E.; Lennane, S.; Cook, T.M. Deaths in healthcare workers due to COVID-19: The need for robust data and analysis. Anaesthesia 2020, 75, 989–992. [Google Scholar] [CrossRef]
- PAHO. Despite Overall Drop in New Infections This Week, Pandemic Continues to Challenge Health Care Workers in the Americas. Available online: https://www.paho.org/en/news/9-2-2022-despite-overall-drop-new-infections-week-pandemic-continues-challenge-health-care (accessed on 14 June 2022).
- Duprat, I.P.; Melo, G.C. de Análise de casos e óbitos pela COVID-19 em profissionais de enfermagem no Brasil. Rev. Bras. Saúde Ocup. 2020, 45, 1–7. [Google Scholar] [CrossRef]
- Smallwood, N.; Harrex, W.; Rees, M.; Willis, K.; Bennett, C.M. COVID-19 infection and the broader impacts of the pandemic on healthcare workers. Respirology 2022, 27, 411–426. [Google Scholar] [CrossRef] [PubMed]
- Lilleri, D.; Marena, C.; Baldanti, F. SARS-CoV-2 Infection in Vaccinated Health Care Workers. N. Engl. J. Med. 2022, 386, 199–200. [Google Scholar] [CrossRef] [PubMed]
- Gammon, J.; Hunt, J.; Williams, S.; Daniel, S.; Rees, S.; Matthewson, S. Infection prevention control and organisational patient safety culture within the context of isolation: Study protocol. BMC Health Serv. Res. 2019, 19, 296. [Google Scholar] [CrossRef] [PubMed]
- Thadathilankal-Jess, J.; Karin, H.; Hellmuth, W. Donning and doffing of personal protective equipment (PPE) for angiography during the COVID-19 crisis. Eur. Heart J. 2020, 41, 1786–1787. [Google Scholar] [CrossRef] [Green Version]
- Jinadatha, C.; Simmons, S.; Dale, C.; Ganachari-Mallappa, N.; Villamaria, F.C.; Goulding, N.; Tanner, B.; Stachowiak, J.; Stibich, M. Disinfecting personal protective equipment with pulsed xenon ultraviolet as a risk mitigation strategy for health care workers. Am. J. Infect. Control 2015, 43, 412–414. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Ning, Z.; Chen, Y.; Guo, M.; Liu, Y.; Gali, N.K.; Sun, L.; Duan, Y.; Cai, J.; Westerdahl, D.; et al. Aerodynamic analysis of SARS-CoV-2 in two Wuhan hospitals. Nature 2020, 582, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Bernardes, G.C.S.; Godoi, A.P.N.; de Almeida, N.A.; Nogueira, L.S.; Pinheiro, M.B. Doffing personal protective equipment in times of COVID-19. Rev. Bras. Med. do Trab. 2021, 19, 88–93. [Google Scholar] [CrossRef] [PubMed]
- Saran, S.; Gurjar, M.; Garg, A. Identifying and Implementing Strategies to Reduce the Risk of Self-Contamination of Health Care Workers Caused by Doffing of Personal Protective Equipment During the COVID-19 Pandemic. Disaster Med. Public Health Prep. 2022, 16, 445–448. [Google Scholar] [CrossRef]
- Brêda Mascarenhas, L.A.; Machado, B.A.S.; Rodrigues, L.d.A.P.; Saraiva Hodel, K.V.; Bandeira Santos, A.Á.; Freitas Neves, P.R.; da Silva Andrade, L.P.C.; Soares, M.B.; de Andrade, J.B.; Badaró, R. Potential application of novel technology developed for instant decontamination of personal protective equipment before the doffing step. PLoS ONE 2021, 16, e0250854. [Google Scholar] [CrossRef]
- Kampf, G.; Todt, D.; Pfaender, S.; Steinmann, E. Persistence of coronaviruses on inanimate surfaces and their inactivation with biocidal agents. J. Hosp. Infect. 2020, 104, 246–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Water, Sanitation, Hygiene and Waste Management for the COVID-19 Virus; World Health Organization: Geneva, Switzerland, 2020; pp. 1–9. [Google Scholar]
- WHO. Cleaning and Disinfection of Environmental Surfaces in the Context of COVID-19. Available online: https://apps.who.int/iris/rest/bitstreams/1277966/retrieve (accessed on 30 August 2020).
- Mascarenhas, L.A.B.; Machado, B.A.S.; Rodrigues, L.A.P.; Hodel, K.V.S.; Santos, A.A.B.; Neves, P.R.F.; Andrade, L.P.C.S.; Soares, M.B.; De Andrade, J.B.; Badaró, R. Development and evaluation of spray disinfection technology for instant decontamination of personal protective equipment before the doffing step: Potential application during the SARS-CoV-2 pandemic. PLoS ONE 2021, 16, e0250854. [Google Scholar]
- OPAS. O Uso de Túneis e Outras Tecnologias Para Desinfecção de Humanos Usando Aspersão de Produtos Químicos ou Radiação UV-C. Available online: https://iris.paho.org/handle/10665.2/52243 (accessed on 30 August 2020).
- Boyce, J.M. Modern technologies for improving cleaning and disinfection of environmental surfaces in hospitals. Antimicrob. Resist. Infect. Control 2016, 5, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, D.J.; Knelson, L.P.; Moehring, R.W.; Lewis, S.S.; Weber, D.J.; Chen, L.F.; Triplett, P.F.; Blocker, M.; Cooney, R.M.; Schwab, J.C.; et al. Implementation Lessons Learned from the Benefits of Enhanced Terminal Room (BETR) Disinfection Study: Process and Perceptions of Enhanced Disinfection with Ultraviolet Disinfection Devices. Infect. Control Hosp. Epidemiol. 2018, 39, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Roupa, Z.; Polychronis, G.; Latzourakis, E.; Nikitara, M.; Ghobrial, S.; Chrysafi, A.; Noula, M. Assessment of Knowledge and Perceptions of Health Workers Regarding COVID-19: A Cross-Sectional Study from Cyprus. J. Community Health 2021, 46, 251–258. [Google Scholar] [CrossRef]
- Sesab Governo do Estado Abre 20 Novos Leitos de UTI COVID-19 No Hospital Espanhol Nesta Segunda. Available online: http://www.saude.ba.gov.br/2020/12/14/governo-do-estado-abre-20-novos-leitos-de-uti-covid-19-no-hospital-espanhol-nesta-segunda/ (accessed on 20 July 2022).
- AratuOn Hospital Geral Ernesto Simões Será Exclusivo Para Pacientes com COVID-19. Available online: https://aratuon.com.br/noticia/coronavirus/hospital-geral-ernesto-simoes-sera-exclusivo-para-pacientes-com-covid-19-saiba-mais (accessed on 20 July 2022).
- Agência Brasil Hospital de Campanha de Salvador Recebe Primeiros Pacientes. Available online: https://agenciabrasil.ebc.com.br/saude/noticia/2021-03/hospital-de-campanha-de-salvador-recebe-primeiros-pacientes (accessed on 20 July 2022).
- Zucchi, P. Funcionários por leito: Estudo em alguns hospitais públicos e privados. Rev. Adm. Pública 1998, 32, 65–76. [Google Scholar]
- Martínez-Mesa, J.; González-Chica, D.A.; Duquia, R.P.; Bonamigo, R.R.; Bastos, J.L. Sampling: How to select participants in my research study? An. Bras. Dermatol. 2016, 91, 326–330. [Google Scholar] [CrossRef] [PubMed]
- Association, W.M. World Medical Association Declaration of Helsinki Ethical Principles for Medical Research Involving Human Subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef]
- CNS RESOLUÇÃO No 466, DE 12 DE DEZEMBRO DE 2012. Available online: https://conselho.saude.gov.br/resolucoes/2012/Reso466.pdf (accessed on 30 August 2020).
- Matuschek, C.; Moll, F.; Fangerau, H.; Fischer, J.C.; Zänker, K.; van Griensven, M.; Schneider, M.; Kindgen-Milles, D.; Trudo Knoefel, W.; Lichtenberg, A.; et al. The history and value of face masks. Eur. J. Med. Res. 2020, 25, 23. [Google Scholar] [CrossRef]
- Rosenberger, L.H.; Riccio, L.M.; Campbell, K.T.; Politano, A.D.; Sawyer, R.G. Quarantine, Isolation, and Cohorting: From Cholera to Klebsiella. Surg. Infect. 2012, 13, 69–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zell, R.; Groth, M.; Krumbholz, A.; Lange, J.; Philipps, A.; Dürrwald, R. Cocirculation of Swine H1N1 Influenza A Virus Lineages in Germany. Viruses 2020, 12, 762. [Google Scholar] [CrossRef] [PubMed]
- Taubenberger, J.K.; Morens, D.M. The 1918 Influenza Pandemic and Its Legacy. Cold Spring Harb. Perspect. Med. 2019, 10, a038695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murray, M.J. Ebola Virus Disease: A Review of Its Past and Present. Anesth. Analg. 2015, 121, 798–809. [Google Scholar] [CrossRef]
- Holmes, K.V. SARS coronavirus: A new challenge for prevention and therapy. J. Clin. Investig. 2003, 111, 1605–1609. [Google Scholar] [CrossRef] [PubMed]
- De Wit, E.; Van Doremalen, N.; Falzarano, D.; Munster, V.J. SARS and MERS: Recent insights into emerging coronaviruses. Nat. Rev. Microbiol. 2016, 14, 523–534. [Google Scholar] [CrossRef]
- Sun, W.; Singh, A.K. Plague vaccine: Recent progress and prospects. npj Vaccines 2018, 4, 11. [Google Scholar] [CrossRef] [Green Version]
- Morens, D.M.; Daszak, P.; Markel, H.; Taubenberger, J.K. Pandemic COVID-19 Joins History’s Pandemic Legion. Clin. Sci. Epidemiol. 2020, 11, e00812-20. [Google Scholar] [CrossRef]
- Zhang, N.; Wang, L.; Deng, X.; Liang, R.; Su, M.; He, C.; Hu, L.; Su, Y.; Ren, J.; Yu, F.; et al. Recent advances in the detection of respiratory virus infection in humans. J. Med. Virol. 2020, 92, 408–417. [Google Scholar] [CrossRef]
- Oldfield, E.; Malwal, S.R. COVID-19 and Other Pandemics: How Might They Be Prevented? ACS Infect. Dis. 2020, 6, 1563–1566. [Google Scholar] [CrossRef]
- Sande-Meijide, M.; Lorenzo-Gonzalez, M.; Mori-Gamarra, F.; Cortes-Gago, I.; Gonzalez-Vazquez, A.; Moure-Rodríguez, L.; Herranz-Urbasos, M. Perceptions and attitudes of patients and health care workers toward patient empowerment in promoting hand hygiene. Am. J. Infect. Control 2018, 47, 45–50. [Google Scholar] [CrossRef] [Green Version]
- Kabała, M.; Aptekorz, M.; Martirosian, G. The role of hospital environment and the hands of medical staff in the transmission of the clostridioides (Clostridium) difficile infection. Med. Pract. 2019, 70, 739–745. [Google Scholar] [CrossRef] [PubMed]
- Morens, D.M.; Taubenberger, J.K. The mother of all pandemics is 100 years old (and going strong)! Am. J. Public Health 2018, 108, 1449–1454. [Google Scholar] [CrossRef] [PubMed]
- de Souza, W.M.; Buss, L.F.; da Silva Candido, D.; Carrera, J.-P.; Li, S.; Zarebski, A.E.; Pereira, R.H.M.; Prete, C.A.; de Souza-Santos, A.A.; Parag, K.V.; et al. Epidemiological and clinical characteristics of the COVID-19 epidemic in Brazil. Nat. Hum. Behav. 2020, 4, 856–865. [Google Scholar] [CrossRef] [PubMed]
- Ministério da Saúde do Brasil Coronavírus Brasil. Available online: https://covid.saude.gov.br/ (accessed on 16 September 2020).
- Ponce, D. The impact of coronavirus in Brazil: Politics and the pandemic. Nat. Rev. Nephrol. 2020, 16, 483. [Google Scholar] [CrossRef] [PubMed]
- Marson, F.A.L.; Ortega, M.M. COVID-19 in Brazil. Pulmonology 2020, 26, 241–244. [Google Scholar] [CrossRef]
- Lancet, T. COVID-19 in Brazil: “So what?”. Lancet 2020, 395, 10235. [Google Scholar] [CrossRef]
- Murari, T.B.; Nascimento-Filho, A.S.; Rocha-Filho, T.; Scorza, C.A.; Scorza, F.A.; Almeida, A.C.G.; Moret, M.A. Evidences of reduction in SARS-CoV-2 transmission due to local measures and policies in early stages of the pandemic. BMJ 2021, 375, e068302. [Google Scholar]
- SESAB SEI—COVID-19. Available online: https://infovis.sei.ba.gov.br/covid19/ (accessed on 16 August 2020).
- SESA Governo do Ceará já Abriu 2.648 Novos Leitos Exclusivos Para Pacientes com COVID-19. Available online: https://www.saude.ce.gov.br/2020/06/01/governo-do-ceara-ja-abriu-2-648-novos-leitos-exclusivos-para-pacientes-com-covid-19/ (accessed on 16 August 2020).
- SES PE Zera Fila de UTI Para Pacientes com a COVID-19. Available online: http://portal.saude.pe.gov.br/noticias/secretaria/pe-zera-fila-de-uti-para-pacientes-com-covid-19 (accessed on 16 August 2020).
- SUSAM Ocupação de Leitos-Resumo. Available online: http://www.saude.am.gov.br/docs/covid19/OC_LEITOS_20200816.pdf (accessed on 16 August 2020).
- Coronavírus: Cidade do Interior de SP Instala “Túnel Desinfetante” Contra COVID-19. Available online: https://noticias.uol.com.br/saude/ultimas-noticias/redacao/2020/04/01/cidade-do-interior-de-sp-instala-tunel-desinfetante-contra-coronavirus.htm (accessed on 14 August 2020).
- Túneis de Desinfecção São Adotados em Cidades do Brasil: Equipamento Tem Alguma Utilidade Contra COVID-19? Available online: https://epoca.globo.com/sociedade/tuneis-de-desinfeccao-sao-adotados-em-cidades-do-brasil-equipamento-tem-alguma-utilidade-contra-covid-19-24424580 (accessed on 14 August 2020).
- Já Instalados no Centro de Teixeira, Túneis de Desinfecção Ajudam No Combate a COVID-19. Available online: https://www.sulbahianews.com.br/video-ja-instalados-no-centro-de-teixeira-tuneis-de-desinfeccao-ajudam-no-combate-a-covid-19/ (accessed on 14 August 2020).
- Rock, C.; Curless, M.S.; Carson, K.A.; Nowakowski, E.; Scheeler, V.; Maragakis, L.L. Patient and health careworker perceptions of daily use of ultraviolet-C technology as an adjunct to daily cleaning in an academic hospital: Secondary study of Ultra Violet-C Light Evaluation as an Adjunct to Removing Multi-Drug Resistant Organisms. Am. J. Infect. Control 2018, 46, 348–349. [Google Scholar] [CrossRef]
- Dunn, A.N.; Vaisberg, P.; Fraser, T.G.; Donskey, C.J.; Deshpande, A. Perceptions of Patients, Health Care Workers, and Environmental Services Staff Regarding Ultraviolet Light Room Decontamination Devices. Am. J. Infect. Control 2019, 47, 1290–1293. [Google Scholar] [CrossRef]
- Benenson, S.; Cohen, M.J.; Schwartz, C.; Revva, M.; Moses, A.E.; Levin, P.D. Is it financially beneficial for hospitals to prevent nosocomial infections? BMC Health Serv. Res. 2020, 20, 653. [Google Scholar] [CrossRef]
- Morales, E.; Cots, F.; Sala, M.; Comas, M.; Belvis, F.; Riu, M.; Salvadá, M.; Grau, S.; Horcajada, J.P.; Montero, M.M.; et al. Hospital costs of nosocomial multi-drug resistant Pseudomonas aeruginosa acquisition. BMC Health Serv. Res. 2012, 12, 122. [Google Scholar] [CrossRef] [Green Version]
- Tübbicke, A.; Hübner, C.; Hübner, N.O.; Wegner, C.; Kramer, A.; Fleßa, S. Cost comparison of MRSA screening and management—A decision tree analysis. BMC Health Serv. Res. 2012, 12, 438. [Google Scholar] [CrossRef] [PubMed]
- Slaughter, R.J.; Watts, M.; Vale, J.A.; Grieve, J.R.; Schep, L.J. The clinical toxicology of sodium hypochlorite. Clin. Toxicol. 2019, 57, 303–311. [Google Scholar] [CrossRef] [PubMed]
- Nikpour, S.; Masoumi-Moghaddam, E.; Pazoki, S.; Hassanian-Moghaddam, H.; Zamani, N. Upper Gastrointestinal Endoscopic Evaluation Following Household Sodium Hypochlorite Ingestion. J. Burn Care Res. 2017, 39, 1. [Google Scholar] [CrossRef] [PubMed]
- Matulonga, B.; Rava, M.; Siroux, V.; Bernard, A.; Dumas, O.; Pin, I.; Zock, J.-P.; Nadif, R.; Leynaert, B.; Le Moual, N. Women using bleach for home cleaning are at increased risk of non-allergic asthma. Respir. Med. 2016, 117, 264–271. [Google Scholar] [CrossRef] [PubMed]
- Murashevych, B.; Girenko, D.; Maslak, H.; Stepanskyi, D.; Abraimova, O.; Netronina, O.; Zhminko, P. Acute inhalation toxicity of aerosolized electrochemically generated solution of sodium hypochlorite. Inhal. Toxicol. 2022, 34, 1–13. [Google Scholar] [CrossRef]
- Carpenter, A.; Cox, A.T.; Marion, D.; Phillips, A.; Ewington, I. A case of a chlorine inhalation injury in an Ebola treatment unit. J. R. Army Med. Corps 2016, 162, 229–231. [Google Scholar] [CrossRef]
- Ma, Q.-X.; Shan, H.; Zhang, H.-L.; Li, G.-M.; Yang, R.-M.; Chen, J.-M. Potential utilities of mask-wearing and instant hand hygiene for fighting SARS-CoV-2. J. Med. Virol. 2020, 92, 1567–1571. [Google Scholar] [CrossRef]
- Saini, V.; Sikri, K.; Dhingra Batra, S.; Kalra, P.; Gautam, K. Development of a highly effective low-cost vaporized hydrogen peroxide-based method for disinfection of personal protective equipment for their selective reuse during pandemics. Gut Pathog. 2020, 12, 29. [Google Scholar] [CrossRef]
- Rogers, R.; O’brien, T.; Aridi, J.; Beckwith, C.G. The COVID-19 Diagnostic Dilemma: A Clinician’s Perspective. J. Clin. Microbiol. 2020, 58, e01287-20. [Google Scholar] [CrossRef]
- OMS. Rational Use of Personal Protective Equipment for Coronavirus Disease (COVID-19) and Considerations during Severe Shortages: Interim Guidance; OMS: Geneva, Switzerland, 2020. [Google Scholar]
- Roszak, A.; Jensen, F.; Wild, R.; Yeskey, K.; Handrigan, M. Implications of the Emergency Medical Treatment and Labor Act (EMTALA) During Public Health Emergencies and on Alternate Sites of Care. Disaster Med. Public Health Prep. 2009, 3, S172–S175. [Google Scholar] [CrossRef]
- Essén, A.; Lindblad, S. Innovation as emergence in healthcare: Unpacking change from within. Soc. Sci. Med. 2013, 93, 203–211. [Google Scholar] [CrossRef]
- Sukkird, V.; Shirahada, K. Technology challenges to healthcare service innovation in aging Asia: Case of value co-creation in emergency medical support system. Technol. Soc. 2015, 43, 122–128. [Google Scholar] [CrossRef]
- Pasquier, P.; Luft, A.; Gillard, J.; Boutonnet, M.; Vallet, C.; Pontier, J.-M.; Duron-Martinaud, S.; Dia, A.; Puyeo, L.; Debrus, F.; et al. How do we fight COVID-19? Military medical actions in the war against the COVID-19 pandemic in France. BMJ Mil. Health Mon. 2020, 167, 269–274. [Google Scholar] [CrossRef] [PubMed]
- Harris, M.; Bhatti, Y.; Buckley, J.; Sharma, D. Fast and frugal innovations in response to the COVID-19 pandemic. Nat. Med. 2020, 26, 814–821. [Google Scholar] [CrossRef] [PubMed]
- Cawthorne, K.-R.; Cooke, R. Innovative technologies for hand hygiene monitoring are urgently needed in the fight against COVID-19. J. Hosp. Infect. 2020, 105, 362–363. [Google Scholar] [CrossRef] [PubMed]
- Menardi, E.; Ballari, G.P.; Racca, E.; Gagliardi, M.; Gonella, A.; Sbarro, F.; Musso, R.; Cagliero, S.; Baralis, G. Telemedicine during COVID-19 pandemic. J. Arrhythmia 2020, 36, 804–805. [Google Scholar] [CrossRef] [PubMed]
- Jiménez-Rodríguez, D.; Santillán García, A.; Montoro Robles, J.; Rodríguez Salvador, M.d.M.; Muñoz Ronda, F.J.; Arrogante, O. Increase in Video Consultations During the COVID-19 Pandemic: Healthcare Professionals’ Perceptions about Their Implementation and Adequate Management. Int. J. Environ. Res. Public Health 2020, 17, 5112. [Google Scholar] [CrossRef] [PubMed]
- Brown, H.; Preston, D.; Bhoja, R. Thinking Outside the Box. Anesthesiology 2020, 133, 683–684. [Google Scholar] [CrossRef]
- Motara, F.; Laher, A.E.; Du Plessis, J.; Moolla, M. The “Intubox”: Enhancing Frontline Healthcare Worker Safety During Coronavirus Disease 2019 (COVID-19). Cureus 2020, 12, e8530. [Google Scholar] [CrossRef]
- Oliveira, F.; Dos Santos, L.M.C.; da Silva, E.S.; de Alencar Pereira Rodrigues, L.; Freitas Neves, P.R.; Fernandes Moreira, G.A.; Lobato, G.M.; Nascimento, C.; Gerhardt, M.; Bandeira Santos, A.A.; et al. Disinfecting Efficacy of an Ozonated Water Spray Chamber: Scientific Evidence of the Total and Partial Biocidal Effect on Personal Protective Equipment and in Vitro Analysis of a Viral Experimental Model. Ozone Sci. Eng. 2022, 2022, 1–19. [Google Scholar] [CrossRef]
- Xia, J.; Gao, J.; Tang, W. Nosocomial infection and its molecular mechanisms of antibiotic resistance. Biosci. Trends 2016, 10, 14–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weber, D.J.; Kanamori, H.; Rutala, W.A. “No touch” technologies for environmental decontamination: Focus on ultraviolet devices and hydrogen peroxide systems. Curr. Opin. Infect. Dis. 2016, 29, 424–431. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mascarenhas, L.A.B.; Machado, B.A.S.; Rodrigues, L.d.A.P.; Hodel, K.V.S.; Santos, A.Á.B.; Andrade, L.P.C.d.S.; Badaró, R. Perception of Professionals from Different Healthcare Units Regarding the Use of Spray Technology for the Instantaneous Decontamination of Personal Protective Equipment during the Coronavirus Disease Pandemic: A Short Analysis. Appl. Sci. 2022, 12, 7771. https://doi.org/10.3390/app12157771
Mascarenhas LAB, Machado BAS, Rodrigues LdAP, Hodel KVS, Santos AÁB, Andrade LPCdS, Badaró R. Perception of Professionals from Different Healthcare Units Regarding the Use of Spray Technology for the Instantaneous Decontamination of Personal Protective Equipment during the Coronavirus Disease Pandemic: A Short Analysis. Applied Sciences. 2022; 12(15):7771. https://doi.org/10.3390/app12157771
Chicago/Turabian StyleMascarenhas, Luís Alberto Brêda, Bruna Aparecida Souza Machado, Leticia de Alencar Pereira Rodrigues, Katharine Valéria Saraiva Hodel, Alex Álisson Bandeira Santos, Leone Peter Correia da Silva Andrade, and Roberto Badaró. 2022. "Perception of Professionals from Different Healthcare Units Regarding the Use of Spray Technology for the Instantaneous Decontamination of Personal Protective Equipment during the Coronavirus Disease Pandemic: A Short Analysis" Applied Sciences 12, no. 15: 7771. https://doi.org/10.3390/app12157771
APA StyleMascarenhas, L. A. B., Machado, B. A. S., Rodrigues, L. d. A. P., Hodel, K. V. S., Santos, A. Á. B., Andrade, L. P. C. d. S., & Badaró, R. (2022). Perception of Professionals from Different Healthcare Units Regarding the Use of Spray Technology for the Instantaneous Decontamination of Personal Protective Equipment during the Coronavirus Disease Pandemic: A Short Analysis. Applied Sciences, 12(15), 7771. https://doi.org/10.3390/app12157771