
Influence of Home Indoor Dampness Exposure on Volatile Organic Compounds in Exhaled Breath of Mothers and Their Infants: The NELA Birth Cohort

 ,
,  , ,
, ,  , ,
on behalf of the NELA Study Group
, ,
on behalf of the NELA Study Group
Abstract
:
1. Introduction
2. Results
2.1. Characteristics of the Study Population
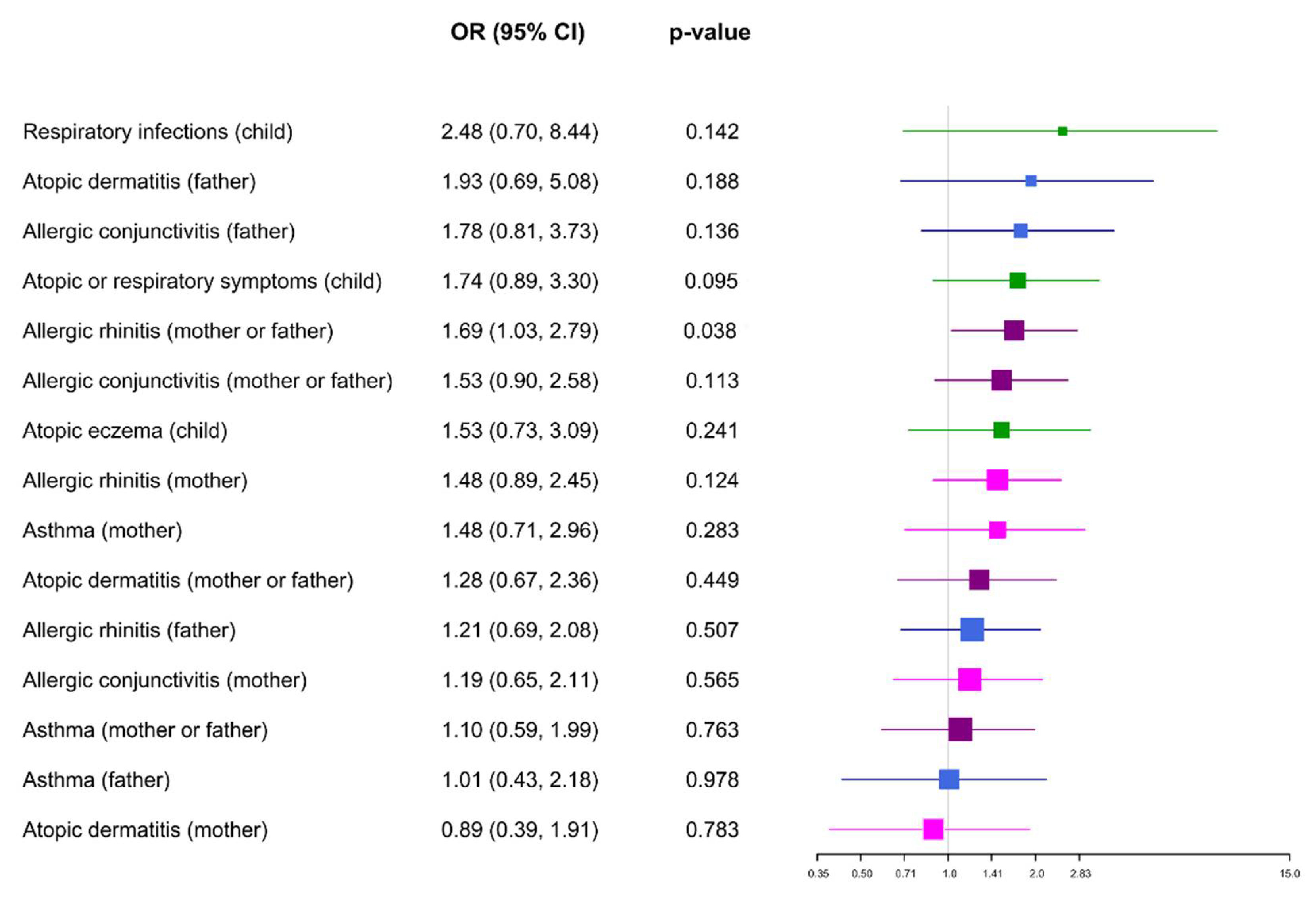
2.2. Home Dampness and Atopic Disorders
2.3. Home Dampness and Analysis of White-Blood-Cell (WBC) Counts
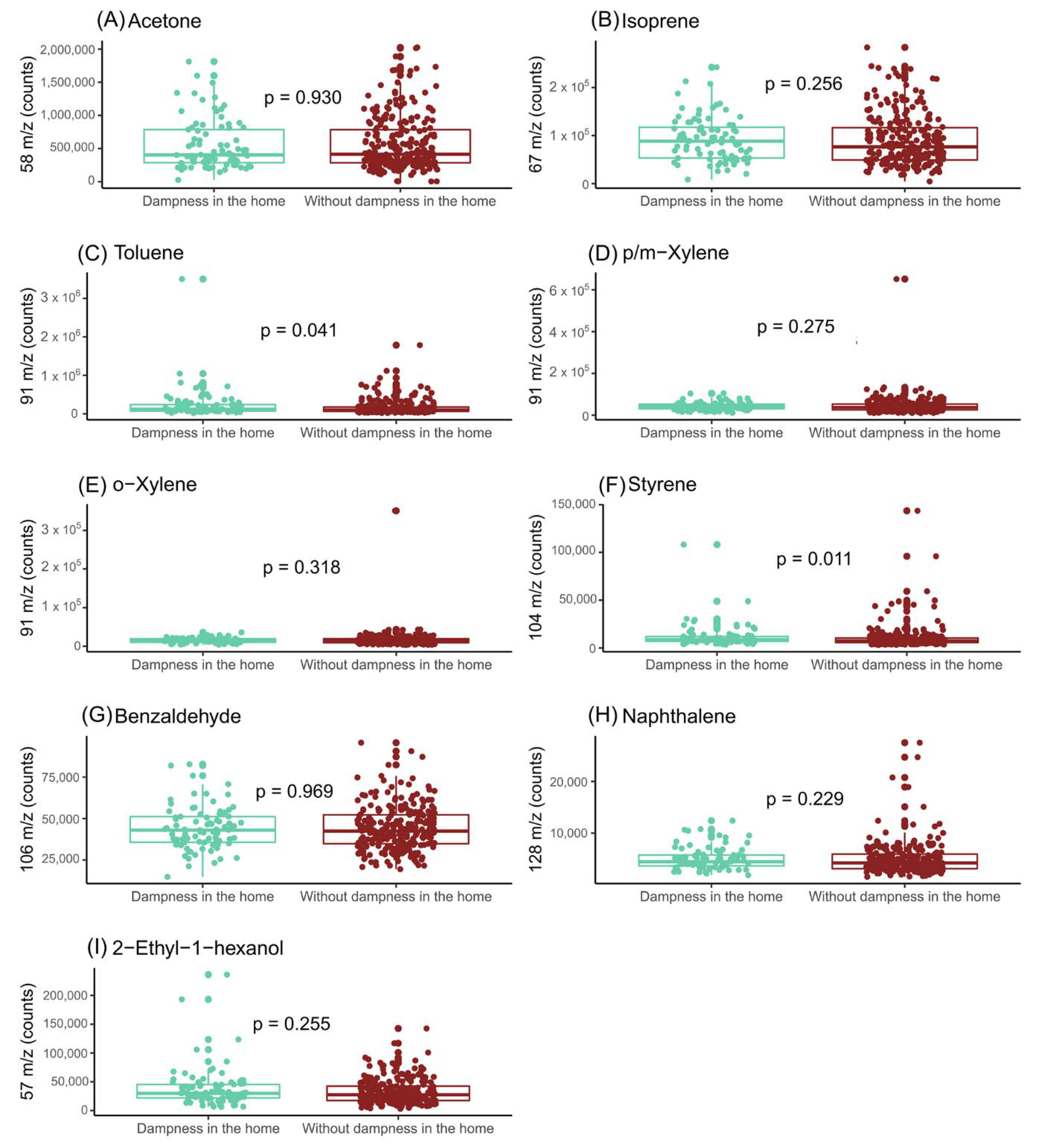
2.4. Home Dampness and Exhaled Breath of Mothers
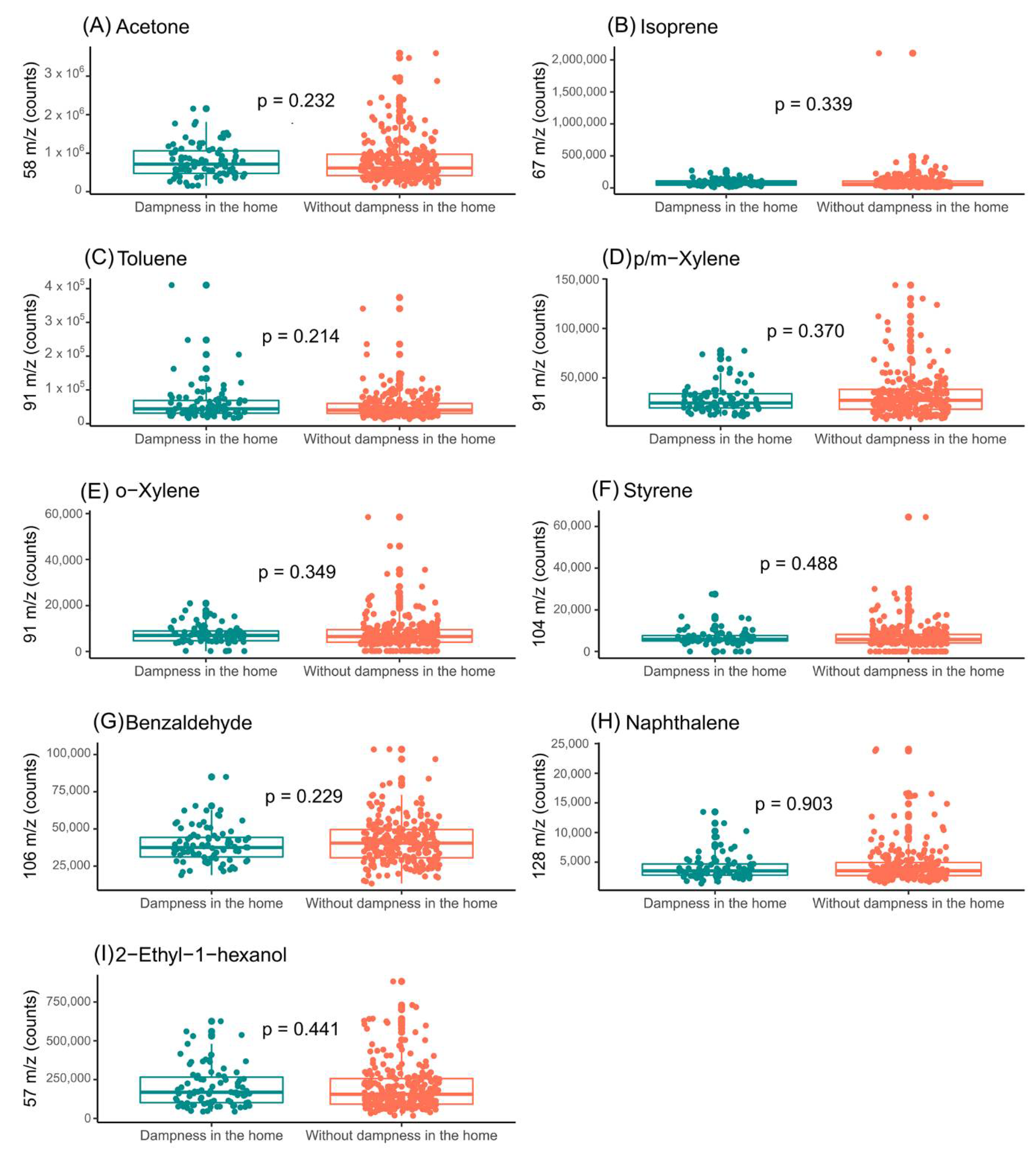
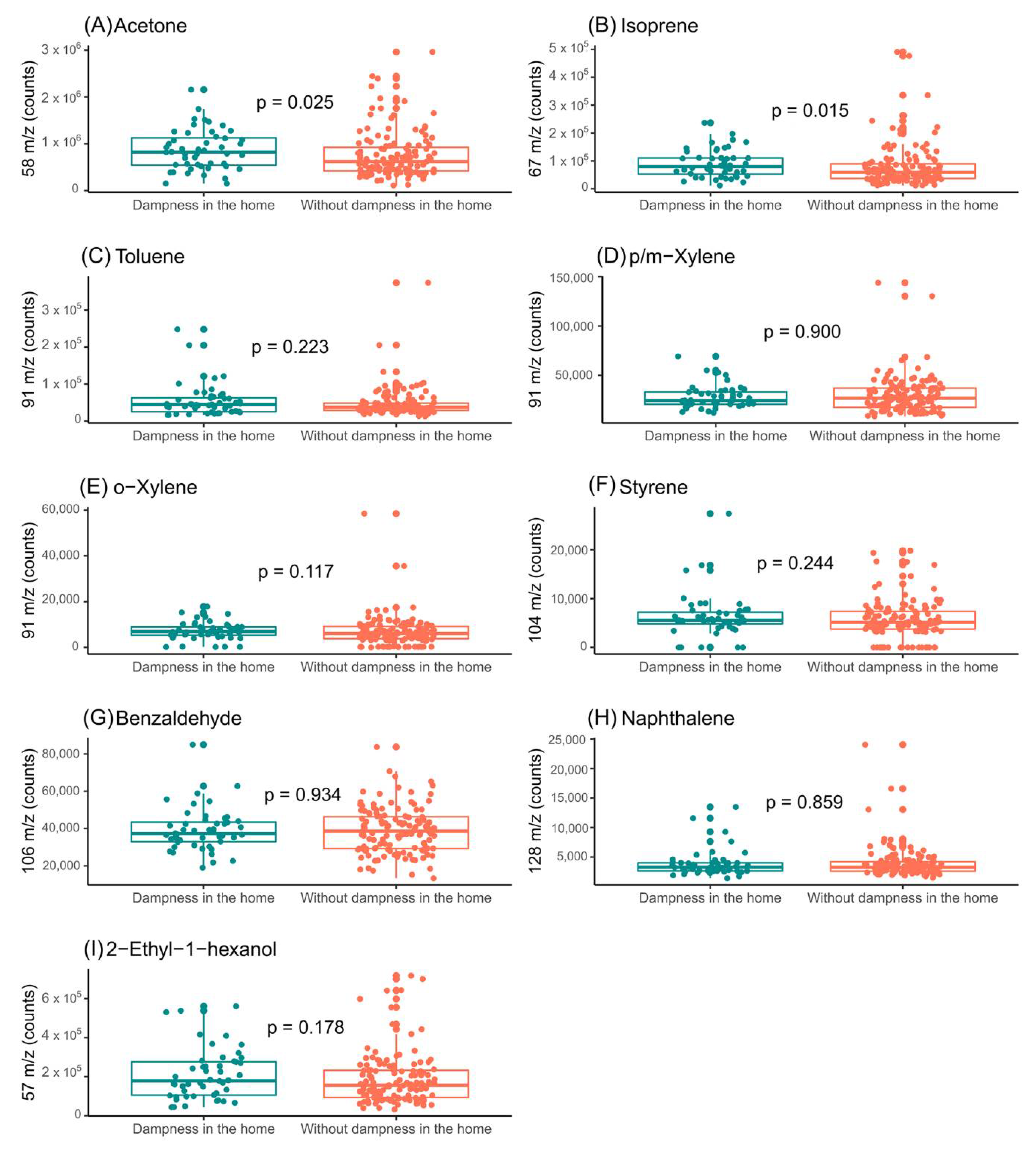
2.5. Home Dampness and Exhaled Breath of Infants
3. Discussion
Current Limitations
4. Materials and Methods
4.1. Study Design and Participants
4.2. Information on Indoor-Dampness Exposure, Health Outcomes and Other Variables
4.3. Collection and Analysis of Exhaled Breath
4.4. Data Preprocessing
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Beckhaus, A.A.; Garcia-Marcos, L.; Forno, E.; Pacheco-Gonzalez, R.M.; Celedõn, J.C.; Castro-Rodriguez, J.A. Maternal nutrition during pregnancy and risk of asthma, wheeze, and atopic diseases during childhood: A systematic review and meta-analysis. Allergy 2015, 70, 1588–1604. [Google Scholar] [CrossRef]
- Kansen, H.M.; Le, T.M.; Uiterwaal, C.S.P.M.; van Ewijk, B.E.; Balemans, W.A.F.; Gorissen, D.M.W.; de Vries, E.; van Velzen, M.F.; Slabbers, G.H.P.R.; Meijer, Y.; et al. Prevalence and predictors of uncontrolled asthma in children referred for asthma and other atopic diseases. J. Asthma Allergy 2020, 13, 67–75. [Google Scholar] [CrossRef] [Green Version]
- Amat, F.; Soria, A.; Tallon, P.; Bourgoin-Heck, M.; Lambert, N.; Deschildre, A.; Just, J. New insights into the phenotypes of atopic dermatitis linked with allergies and asthma in children: An overview. Clin. Exp. Allergy 2018, 48, 919–934. [Google Scholar] [CrossRef]
- van de Kant, K.D.G.; van Berkel, J.J.B.N.; Jobsis, Q.; Lima Passos, V.; Klaassen, E.M.M.; van der Sande, L.; van Schayck, O.C.P.; de Jongste, J.C.; van Schooten, F.J.; Derks, E.; et al. Exhaled breath profiling in diagnosing wheezy preschool children. Eur. Respir. J. 2013, 41, 183–188. [Google Scholar] [CrossRef]
- Potaczek, D.P.; Harb, H.; Michel, S.; Alhamwe, B.A.; Renz, H.; Tost, J. Epigenetics and allergy: From basic mechanisms to clinical applications. Epigenomics 2017, 9, 539–571. [Google Scholar] [CrossRef]
- Garn, H.; Potaczek, D.P.; Pfefferle, P.I. The Hygiene Hypothesis and New Perspectives-Current Challenges Meeting an Old Postulate. Front. Immunol. 2021, 12, 637087. [Google Scholar] [CrossRef]
- Adgate, J.L.; Church, T.R.; Ryan, A.D.; Ramachandran, G.; Fredrickson, A.L.; Stock, T.H.; Morandi, M.T.; Sexton, K. Outdoor, indoor, and personal exposure to VOCs in children. Environ. Health Perspect. 2004, 112, 1386–1392. [Google Scholar] [CrossRef] [Green Version]
- Sharpe, R.A.; Bearman, N.; Thornton, C.R.; Husk, K.; Osborne, N.J. Indoor fungal diversity and asthma: A meta-analysis and systematic review of risk factors. J. Allergy Clin. Immunol. 2015, 135, 110–122. [Google Scholar] [CrossRef]
- Testa, D.; Di Bari, M.; Nunziata, M.; De Cristofaro, G.; Massaro, G.; Marcuccio, G.; Motta, G. Allergic rhinitis and asthma assessment of risk factors in pediatric patients: A systematic review. Int. J. Pediatr. Otorhinolaryngol. 2020, 129, 109759. [Google Scholar] [CrossRef]
- Mendell, M.J.; Kumagai, K. Observation-based metrics for residential dampness and mold with dose–response relationships to health: A review. Indoor Air 2017, 27, 506–517. [Google Scholar] [CrossRef]
- Madureira, J.; Paciência, I.; Pereira, C.; Teixeira, J.P.; de O. Fernandes, E. Indoor air quality in Portuguese schools: Levels and sources of pollutants. Indoor Air 2016, 26, 526–537. [Google Scholar] [CrossRef] [Green Version]
- Billionnet, C.; Gay, E.; Kirchner, S.; Leynaert, B.; Annesi-Maesano, I. Quantitative assessments of indoor air pollution and respiratory health in a population-based sample of French dwellings. Environ. Res. 2011, 111, 425–434. [Google Scholar] [CrossRef]
- Kwon, J.-W.; Park, H.-W.; Kim, W.J.; Kim, M.-G.; Lee, S.-J. Exposure to volatile organic compounds and airway inflammation. Environ. Health 2018, 17, 65. [Google Scholar] [CrossRef]
- Nielsen, G.D.; Larsen, S.T.; Olsen, O.; Løvik, M.; Poulsen, L.K.; Glue, C.; Wolkoff, P. Do indoor chemicals promote development of airway allergy? Indoor Air 2007, 17, 236–255. [Google Scholar] [CrossRef]
- Son, B.; Breysse, P.; Yang, W. Volatile organic compounds concentrations in residential indoor and outdoor and its personal exposure in Korea. Environ. Int. 2003, 29, 79–85. [Google Scholar] [CrossRef]
- Arif, A.A.; Shah, S.M. Association between personal exposure to volatile organic compounds and asthma among US adult population. Int. Arch. Occup. Environ. Health 2007, 80, 711–719. [Google Scholar] [CrossRef]
- Rattray, N.J.W.; Hamrang, Z.; Trivedi, D.K.; Goodacre, R.; Fowler, S.J. Taking your breath away: Metabolomics breathes life in to personalized medicine. Trends Biotechnol. 2014, 32, 538–548. [Google Scholar] [CrossRef]
- de Lacy Costello, B.; Amann, A.; Al-Kateb, H.; Flynn, C.; Filipiak, W.; Khalid, T.; Osborne, D.; Ratcliffe, N.M. A review of the volatiles from the healthy human body. J. Breath Res. 2014, 8, 014001. [Google Scholar] [CrossRef]
- Caron-Beaudoin, É.; Valter, N.; Chevrier, J.; Ayotte, P.; Frohlich, K.; Verner, M.A. Gestational exposure to volatile organic compounds (VOCs) in Northeastern British Columbia, Canada: A pilot study. Environ. Int. 2018, 110, 131–138. [Google Scholar] [CrossRef]
- Storer, M.; Curry, K.; Squire, M.; Kingham, S.; Epton, M. Breath testing and personal exposure--SIFT-MS detection of breath acetonitrile for exposure monitoring. J. Breath Res. 2015, 9, 036006. [Google Scholar] [CrossRef]
- Amann, A.; de Lacy Costello, B.; Miekisch, W.; Schubert, J.; Buszewski, B.; Pleil, J.; Ratcliffe, N.; Risby, T. The human volatilome: Volatile organic compounds (VOCs) in exhaled breath, skin emanations, urine, feces and saliva. J. Breath Res. 2014, 8, 034001. [Google Scholar] [CrossRef]
- van de Kant, K.D.G.; van der Sande, L.J.T.M.; Jöbsis, Q.; van Schayck, O.C.P.; Dompeling, E. Clinical use of exhaled volatile organic compounds in pulmonary diseases: A systematic review. Respir. Res. 2012, 13, 117. [Google Scholar] [CrossRef] [Green Version]
- Jalali, M.; Zare Sakhvidi, M.J.; Bahrami, A.; Berijani, N.; Mahjub, H. Oxidative stress biomarkers in exhaled breath of workers exposed to crystalline silica dust by SPME-GC-MS. J. Res. Health Sci. 2016, 16, 153–161. [Google Scholar]
- Ferraro, V.A.; Carraro, S.; Pirillo, P.; Gucciardi, A.; Poloniato, G.; Stocchero, M.; Giordano, G.; Zanconato, S.; Baraldi, E. Breathomics in Asthmatic Children Treated with Inhaled Corticosteroids. Metabolites 2020, 10, 390. [Google Scholar] [CrossRef]
- Di Palmo, E.; Cantarelli, E.; Catelli, A.; Ricci, G.; Gallucci, M.; Miniaci, A.; Pession, A. The predictive role of biomarkers and genetics in childhood asthma exacerbations. Int. J. Mol. Sci. 2021, 22, 4651. [Google Scholar] [CrossRef]
- Ibrahim, W.; Carr, L.; Cordell, R.; Wilde, M.J.; Salman, D.; Monks, P.S.; Thomas, P.; Brightling, C.E.; Siddiqui, S.; Greening, N.J. Breathomics for the Clinician: The use of volatile organic compounds in respiratory diseases. Thorax 2021, 76, 514–521. [Google Scholar] [CrossRef]
- Sola-Martínez, R.A.; Lozano-Terol, G.; Gallego-Jara, J.; Morales, E.; Cantero-Cano, E.; Sanchez-Solis, M.; García-Marcos, L.; Jiménez-Guerrero, P.; Noguera-Velasco, J.; Cánovas Díaz, M.; et al. Exhaled volatilome analysis as a useful tool to discriminate asthma with other coexisting atopic diseases in women of childbearing age. Sci. Rep. 2021, 11, 13823. [Google Scholar] [CrossRef]
- Norbäck, D.; Lu, C.; Zhang, Y.; Li, B.; Zhao, Z.; Huang, C.; Zhang, X.; Qian, H.; Sun, Y.; Sundell, J.; et al. Onset and remission of childhood wheeze and rhinitis across China—Associations with early life indoor and outdoor air pollution. Environ. Int. 2019, 123, 61–69. [Google Scholar] [CrossRef]
- Deng, Q.; Lu, C.; Ou, C.; Chen, L.; Yuan, H. Preconceptional, prenatal and postnatal exposure to outdoor and indoor environmental factors on allergic diseases/symptoms in preschool children. Chemosphere 2016, 152, 459–467. [Google Scholar] [CrossRef]
- Lu, C.; Norbäck, D.; Zhang, Y.; Li, B.; Zhao, Z.; Huang, C.; Zhang, X.; Qian, H.; Sun, Y.; Wang, J.; et al. Furry pet-related wheeze and rhinitis in pre-school children across China: Associations with early life dampness and mould, furry pet keeping, outdoor temperature, PM10 and PM2.5. Environ. Int. 2020, 144, 106033. [Google Scholar] [CrossRef]
- Valtonen, V. Clinical diagnosis of the dampness and mold hypersensitivity syndrome: Review of the literature and suggested diagnostic criteria. Front. Immunol. 2017, 8, 951. [Google Scholar] [CrossRef] [Green Version]
- Saijo, Y.; Kishi, R.; Sata, F.; Katakura, Y.; Urashima, Y.; Hatakeyama, A.; Kobayashi, S.; Jin, K.; Kurahashi, N.; Kondo, T.; et al. Symptoms in relation to chemicals and dampness in newly built dwellings. Int. Arch. Occup. Environ. Health 2004, 77, 461–470. [Google Scholar] [CrossRef]
- Wakayama, T.; Ito, Y.; Sakai, K.; Miyake, M.; Shibata, E.; Ohno, H.; Kamijima, M. Comprehensive review of 2-ethyl-1-hexanol as an indoor air pollutant. J. Occup. Health 2019, 61, 19–35. [Google Scholar] [CrossRef] [Green Version]
- Fu, X.; Norbäck, D.; Yuan, Q.; Li, Y.; Zhu, X.; Hashim, J.H.; Hashim, Z.; Ali, F.; Hu, Q.; Deng, Y.; et al. Association between indoor microbiome exposure and sick building syndrome (SBS) in junior high schools of Johor Bahru, Malaysia. Sci. Total Environ. 2021, 753, 141904. [Google Scholar] [CrossRef]
- Fisk, W.J.; Lei-Gomez, Q.; Mendell, M.J. Meta-analyses of the associations of respiratory health effects with dampness and mold in homes. Indoor Air 2007, 17, 284–296. [Google Scholar] [CrossRef]
- Hope, A.P.; Simon, R.A. Excess dampness and mold growth in homes: An evidence-based review of the aeroirritant effect and its potential causes. Allergy Asthma Proc. 2007, 28, 262–270. [Google Scholar] [CrossRef]
- Quansah, R.; Jaakkola, M.S.; Hugg, T.T.; Heikkinen, S.A.M.; Jaakkola, J.J.K. Residential Dampness and Molds and the Risk of Developing Asthma: A Systematic Review and Meta-Analysis. PLoS ONE 2012, 7, 47526. [Google Scholar] [CrossRef]
- Norbäck, D.; Hashim, J.H.; Hashim, Z.; Cai, G.H.; Sooria, V.; Ismail, S.A.; Wieslander, G. Respiratory symptoms and fractional exhaled nitric oxide (FeNO) among students in Penang, Malaysia in relation to signs of dampness at school and fungal DNA in school dust. Sci. Total Environ. 2017, 577, 148–154. [Google Scholar] [CrossRef] [Green Version]
- Rufo, J.C.; Madureira, J.; Paciência, I.; Aguiar, L.; Teixeira, J.P.; Moreira, A.; de Oliveira Fernandes, E. Indoor air quality and atopic sensitization in primary schools: A follow-up study. Porto Biomed. J. 2016, 1, 142–146. [Google Scholar] [CrossRef] [Green Version]
- Wålinder, R.; Wieslander, G.; Norbäck, D.; Wessen, B.; Venge, P. Nasal lavage biomarkers: Effects of water damage and microbial growth in an office building. Arch. Environ. Health 2001, 56, 30–36. [Google Scholar] [CrossRef]
- Zhang, X.; Sahlberg, B.; Wieslander, G.; Janson, C.; Gislason, T.; Norback, D. Dampness and moulds in workplace buildings: Associations with incidence and remission of sick building syndrome (SBS) and biomarkers of inflammation in a 10year follow-up study. Sci. Total Environ. 2012, 430, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Vardoulakis, S.; Giagloglou, E.; Steinle, S.; Davis, A.; Sleeuwenhoek, A.; Galea, K.S.; Dixon, K.; Crawford, J.O. Indoor Exposure to Selected Air Pollutants in the Home Environment: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 8972. [Google Scholar] [CrossRef] [PubMed]
- Boots, A.W.; van Berkel, J.J.B.N.; Dallinga, J.W.; Smolinska, A.; Wouters, E.F.; van Schooten, F.J. The versatile use of exhaled volatile organic compounds in human health and disease. J. Breath Res. 2012, 6, 027108. [Google Scholar] [CrossRef] [PubMed]
- Sola-Martínez, R.A.; Pastor Hernández, J.M.; Yanes Torrado, Ó.; Cánovas Díaz, M.; de Diego Puente, T.; Vinaixa Crevillent, M. Exhaled volatile organic compounds analysis in clinical pediatrics: A systematic review. Pediatr. Res. 2021, 89, 1352–1363. [Google Scholar] [CrossRef] [PubMed]
- Morales, E.; Alcantara-Lopez, M.V.; Cabezas-Herrera, J.; de Diego, T.; Hernandez-Caselles, T.; Jimenez-Guerrero, P.; Larque, E.; Lopez-Soler, C.; Martinez-Gracia, C.; Martinez-Torres, A.; et al. The Nutrition in Early Life and Asthma (NELA) birth cohort study: Rationale, design, and methods. Paediatr. Perinat. Epidemiol. 2022, 36, 310–324. [Google Scholar] [CrossRef]
- Markowicz, P.; Larsson, L. Influence of relative humidity on VOC concentrations in indoor air. Environ. Sci. Pollut. Res. 2015, 22, 5772–5779. [Google Scholar] [CrossRef]
- Wei, X.-F.; Linde, E.; Hedenqvist, M.S. Plasticiser loss from plastic or rubber products through diffusion and evaporation. NPJ Mater. Degrad. 2019, 3, 18. [Google Scholar] [CrossRef] [Green Version]
- Nalli, S.; Horn, O.J.; Grochowalski, A.R.; Cooper, D.G.; Nicell, J.A. Origin of 2-ethylhexanol as a VOC. Environ. Pollut. 2006, 140, 181–185. [Google Scholar] [CrossRef]
- Wieslander, G.; Norbäck, D.; Nordström, K.; Wålinder, R.; Venge, P. Nasal and ocular symptoms, tear film stability and biomarkers in nasal lavage, in relation to building-dampness and building design in hospitals. Int. Arch. Occup. Environ. Health 1999, 72, 451–461. [Google Scholar] [CrossRef]
- Wieslander, G.; Kumlin, A.; Norbäck, D. Dampness and 2-ethyl-1-hexanol in floor construction of rehabilitation center: Health effects in staff. Arch. Environ. Occup. Health 2010, 65, 3–11. [Google Scholar] [CrossRef]
- Paciência, I.; Cavaleiro Rufo, J.; Silva, D.; Martins, C.; Mendes, F.; Farraia, M.; Delgado, L.; de Oliveira Fernandes, E.; Padrão, P.; Moreira, P.; et al. Exposure to indoor endocrine-disrupting chemicals and childhood asthma and obesity. Allergy 2019, 74, 1277–1291. [Google Scholar] [CrossRef] [PubMed]
- Sur, U.; Erkekoglu, P.; Bulus, A.D.; Andiran, N.; Kocer-Gumusel, B. Oxidative stress markers, trace elements, and endocrine disrupting chemicals in children with Hashimoto’s thyroiditis. Toxicol. Mech. Methods 2019, 29, 633–643. [Google Scholar] [CrossRef] [PubMed]
- Norback, D.; Wieslander, G.; Nordstrom, K.; Walinder, R. Asthma symptoms in relation to measured building dampness in upper concrete floor construction, and 2-ethyl-1-hexanol in indoor air. Int. J. Tuberc. Lung Dis. 2000, 4, 1016–1025. [Google Scholar] [PubMed]
- Gibson, P.G. Variability of blood eosinophils as a biomarker in asthma and COPD. Respirology 2018, 23, 12–13. [Google Scholar] [CrossRef] [Green Version]
- Pignatti, P.; Visca, D.; Cherubino, F.; Zampogna, E.; Lucini, E.; Saderi, L.; Sotgiu, G.; Spanevello, A. Do blood eosinophils strictly reflect airway inflammation in COPD? Comparison with asthmatic patients. Respir. Res. 2019, 20, 145. [Google Scholar] [CrossRef] [Green Version]
- Soma, T.; Iemura, H.; Naito, E.; Miyauchi, S.; Uchida, Y.; Nakagome, K.; Nagata, M. Implication of fraction of exhaled nitric oxide and blood eosinophil count in severe asthma. Allergol. Int. 2018, 67, S3–S11. [Google Scholar] [CrossRef]
- Zhang, X.; Norbäck, D.; Fan, Q.; Bai, X.; Li, T.; Zhang, Y.; Li, B.; Zhao, Z.; Huang, C.; Deng, Q.; et al. Dampness and mold in homes across China: Associations with rhinitis, ocular, throat and dermal symptoms, headache and fatigue among adults. Indoor Air 2019, 29, 30–42. [Google Scholar] [CrossRef]
- Jaakkola, J.J.K.; Hwang, B.F.; Jaakkola, M.S. Home dampness and molds as determinants of allergic rhinitis in childhood: A 6-year, population-based cohort study. Am. J. Epidemiol. 2010, 172, 451–459. [Google Scholar] [CrossRef] [Green Version]
- Caillaud, D.; Leynaert, B.; Keirsbulck, M.; Nadif, R.; Roussel, S.; Ashan-Leygonie, C.; Bex, V.; Bretagne, S.; Caillaud, D.; Colleville, A.C.; et al. Indoor mould exposure, asthma and rhinitis: Findings from systematic reviews and recent longitudinal studies. Eur. Respir. Rev. 2018, 27, 170137. [Google Scholar] [CrossRef] [Green Version]
- Miekisch, W.; Schubert, J.K.; Noeldge-Schomburg, G.F. Diagnostic potential of breath analysis—Focus on volatile organic compounds. Clin. Chim. Acta 2004, 347, 25–39. [Google Scholar] [CrossRef]
- Kercsmar, C.M.; Dearborn, D.G.; Schluchter, M.; Xue, L.; Kirchner, H.L.; Sobolewski, J.; Greenberg, S.J.; Vesper, S.J.; Allan, T. Reduction in asthma morbidity in children as a result of home remediation aimed at moisture sources. Environ. Health Perspect. 2006, 114, 1574–1580. [Google Scholar] [CrossRef] [PubMed]
- Barnes, C.S.; Horner, W.E.; Kennedy, K.; Grimes, C.; Miller, J.D.; Baxi, S.; Larenas-Linnemann, D.; Levetin, E.; Phipatanakul, W.; Williams, P.B.; et al. Home Assessment and Remediation. J. Allergy Clin. Immunol. Pract. 2016, 4, 423–431.e15. [Google Scholar] [CrossRef]
- Domingo-Salvany, A.; Regidor, E.; Alonso, J.; Alvarez-Dardet, C. Proposal for a social class measure. Working Group of the Spanish Society of Epidemiology and the Spanish Society of Family and Community Medicine. Aten. Primaria 2000, 25, 350–363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sola-Martínez, R.A.; Pastor Hernández, J.M.; Lozano Terol, G.; Gallego-Jara, J.; García-Marcos, L.; Cánovas Díaz, M.; De Diego Puente, T. Data preprocessing workflow for exhaled breath analysis by GC/MS using open sources. Sci. Rep. 2020, 10, 22008. [Google Scholar] [CrossRef] [PubMed]
- Martens, L.; Chambers, M.; Sturm, M.; Kessner, D.; Levander, F.; Shofstahl, J.; Tang, W.H.; Römpp, A.; Neumann, S.; Pizarro, A.D.; et al. mzML—A community standard for mass spectrometry data. Mol. Cell. Proteomics 2011, 10, R110.000133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adusumilli, R.; Mallick, P. Data conversion with proteoWizard msConvert. In Proteomics: Methods and Protocols; Comai, U., Katz, J.E., Mallick, P., Eds.; Humana: New York, NY, USA, 2017; Volume 1550, pp. 339–368. [Google Scholar]
- Smith, C.A.; Want, E.J.; O’Maille, G.; Abagyan, R.; Siuzdak, G. XCMS: Processing Mass Spectrometry Data for Metabolite Profiling Using Nonlinear Peak Alignment, Matching, and Identification. Anal. Chem. 2006, 78, 779–787. [Google Scholar] [CrossRef]
- Senan, O.; Aguilar-Mogas, A.; Navarro, M.; Capellades, J.; Noon, L.; Burks, D.; Yanes, O.; Guimerà, R.; Sales-Pardo, M. CliqueMS: A computational tool for annotating in-source metabolite ions from LC-MS untargeted metabolomics data based on a coelution similarity network. Bioinformatics 2019, 35, 4089–4097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Domingo-Almenara, X.; Brezmes, J.; Vinaixa, M.; Samino, S.; Ramirez, N.; Ramon-Krauel, M.; Lerin, C.; Díaz, M.; Ibáñez, L.; Correig, X.; et al. eRah: A Computational Tool Integrating Spectral Deconvolution and Alignment with Quantification and Identification of Metabolites in GC/MS-Based Metabolomics. Anal. Chem. 2016, 88, 9821–9829. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Without Dampness in the Home (n = 251) | Dampness in the Home (n = 86) | p-Value | |
|---|---|---|---|
| Age (years), mean (range) | 33 (18–43) | 33 (20–41) | 0.896 |
| BMI (Kg/m2), before pregnancy, mean (range) | 23.8 (15.9–40.4) | 24.3 (16.7–42.3) | 0.251 |
| Social class (Managers-technicians/skilled/semiskilled-unskilled/unemployed, no. %) | 38.2/19.9/19.1/22.7 | 31.4/22.1/24.4/22.1 | 0.602 |
| Educational level (Incomplete secondary or less/complete secondary/university, no. %) | 16.7/25.5/57.8 | 17.4/27.9/54.7 | 0.873 |
| Smoking during pregnancy, no. % | 35 (13.9%) | 13 (15.1%) | 0.858 |
| Without Dampness in the Home (n = 250) | Dampness in the Home (n = 87) | p-Value | |
|---|---|---|---|
| Males/females n/n | 119/131 | 39/48 | 0.709 |
| Birth weight (Kg), mean (range) | 3.239 (1.560–4.980) | 3.183 (1.940–4.505) | 0.366 |
| Birth height (cm), mean (range) | 51 (36–56) | 50 (46–54) | 0.153 |
| Without Dampness in the Home (n = 251) | Dampness in the Home (n = 86) | p-Value | |
|---|---|---|---|
| Leucocyte count, ×103/µL | 9.31 ± 2.13 | 9.05 ± 2.14 | 0.312 |
| Lymphocyte count, ×103/µL | 2.02 ± 0.61 | 1.95 ± 0.49 | 0.598 |
| Monocyte count, ×103/µL | 0.61 ± 0.18 | 0.60 ± 0.16 | 0.879 |
| Eosinophil count, ×103/µL | 0.14 ± 0.09 | 0.17 ± 0.10 | 0.049 |
| Neutrophil count, ×103/µL | 6.51 ± 1.67 | 6.30 ± 1.82 | 0.199 |
| Basophil count, ×103/µL | 0.03 ± 0.02 | 0.03 ± 0.01 | 0.117 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sola-Martínez, R.A.; Lozano Terol, G.; Gallego-Jara, J.; Morales, E.; García-Marcos, L.; Noguera-Velasco, J.A.; Cánovas Díaz, M.; de Diego Puente, T., on behalf of the NELA Study Group. Influence of Home Indoor Dampness Exposure on Volatile Organic Compounds in Exhaled Breath of Mothers and Their Infants: The NELA Birth Cohort. Appl. Sci. 2022, 12, 6864. https://doi.org/10.3390/app12146864
Sola-Martínez RA, Lozano Terol G, Gallego-Jara J, Morales E, García-Marcos L, Noguera-Velasco JA, Cánovas Díaz M, de Diego Puente T on behalf of the NELA Study Group. Influence of Home Indoor Dampness Exposure on Volatile Organic Compounds in Exhaled Breath of Mothers and Their Infants: The NELA Birth Cohort. Applied Sciences. 2022; 12(14):6864. https://doi.org/10.3390/app12146864
Chicago/Turabian StyleSola-Martínez, Rosa A., Gema Lozano Terol, Julia Gallego-Jara, Eva Morales, Luis García-Marcos, José Antonio Noguera-Velasco, Manuel Cánovas Díaz, and Teresa de Diego Puente on behalf of the NELA Study Group. 2022. "Influence of Home Indoor Dampness Exposure on Volatile Organic Compounds in Exhaled Breath of Mothers and Their Infants: The NELA Birth Cohort" Applied Sciences 12, no. 14: 6864. https://doi.org/10.3390/app12146864
APA StyleSola-Martínez, R. A., Lozano Terol, G., Gallego-Jara, J., Morales, E., García-Marcos, L., Noguera-Velasco, J. A., Cánovas Díaz, M., & de Diego Puente, T., on behalf of the NELA Study Group. (2022). Influence of Home Indoor Dampness Exposure on Volatile Organic Compounds in Exhaled Breath of Mothers and Their Infants: The NELA Birth Cohort. Applied Sciences, 12(14), 6864. https://doi.org/10.3390/app12146864