
Efficacy of Instruments for Professional Oral Hygiene on Dental Implants: A Systematic Review



Abstract
1. Introduction
2. Materials and Methods
- -
- Population: patients with dental implants not affected by perimplantitis
- -
- Intervention: any instrument for professional oral hygiene on dental implants
- -
- Comparison: any instrument for professional oral hygiene on dental implants different from intervention
- -
- Outcomes: cleaning efficacy
2.1. Search Strategy
- oral hygiene techniques on dental implants or dental implant materials,
- studies of the last ten years (since 1 January 2010),
- no patients affected by perimplantitis
- no patients with orthodontic appliances
- no patients affected by systemic pathologies
2.2. Screening and Selection
2.3. Data Extraction
2.4. Quality Assessment
3. Results
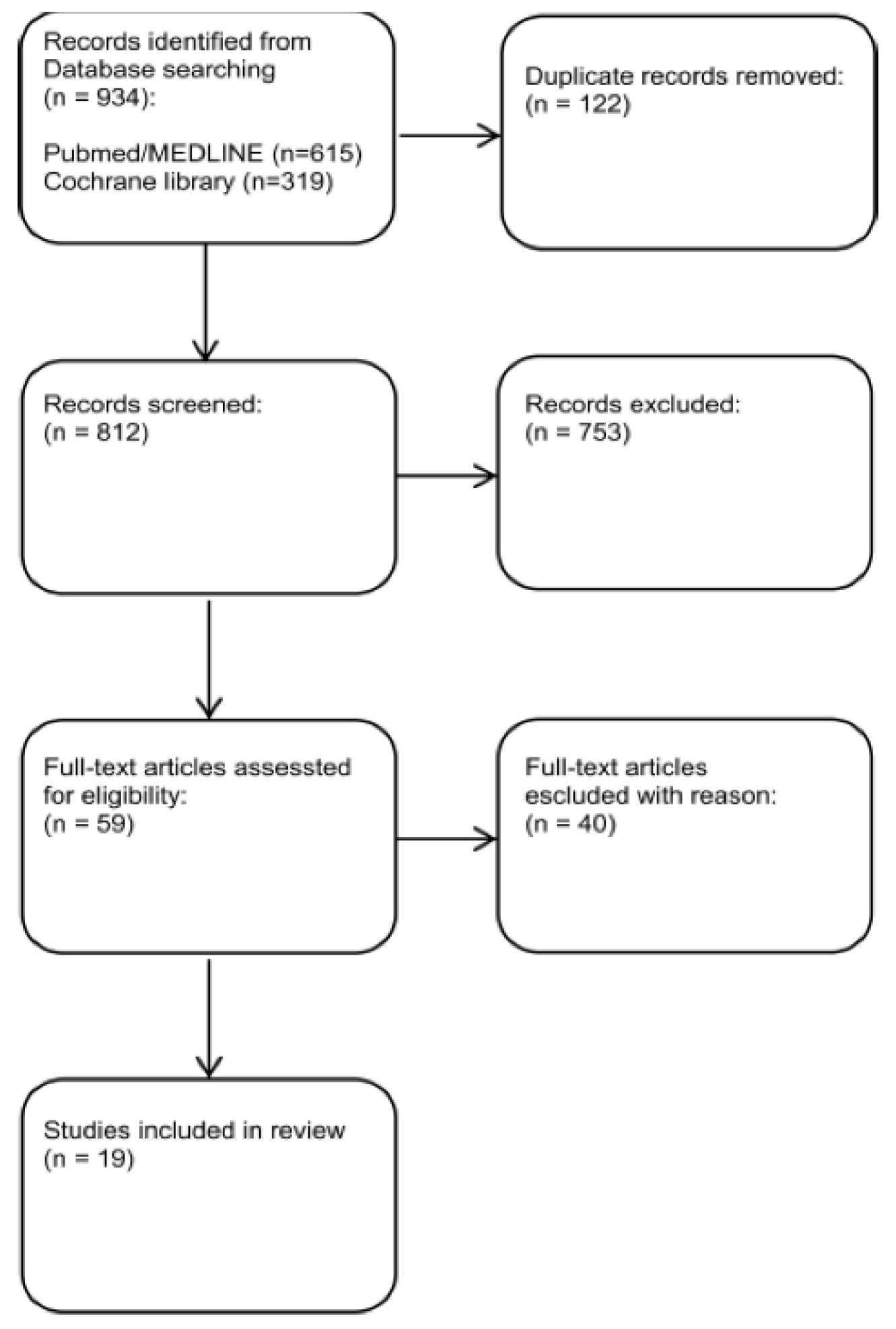
3.1. Bibliographic Search and Study Selection
3.2. Description of Included Studies
3.3. Excluded Studies
3.4. Quality Assessment of Included Studies
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Study | Reason for Exclusion |
|---|---|
| Amate-Fernández et al., 2021 | Not focused on efficacy |
| Salles et al., 2021 | Home oral hygiene |
| Iatrou et al., 2021 | Simulation of peri-implant defects |
| Salles et al., 2021 | Home oral hygiene |
| Hu et al., 2020 | Not focused on efficacy |
| Mensi et al.2020 | Simulation of peri-implant defects |
| Hu et al., 2020 | Not focused on efficacy |
| Gümüş et al., 2020 | Not focused on efficacy |
| Vyas et al., 2020 | No instrument comparison |
| Vyas et al., 2020 | No instrument comparison |
| Huang et al., 2019 | Not focused on efficacy |
| Cha et al., 2019 | Not focused on efficacy |
| Keim et al., 2019 | Simulation of peri-implant defects |
| Biazussi et al., 2019 | Not focused on efficacy |
| Harrel et al., 2019 | Not focused on efficacy |
| Takagi et al., 2018 | Not focused on efficacy |
| Cao et al., 2018 | Not focused on efficacy |
| Larsen et al., 2017 | Not focused on efficacy |
| Quintero et al., 2017 | Not focused on efficacy |
| Schmidt et al., 2017 | Not focused on efficacy |
| Hakki et al., 2017 | Not focused on efficacy |
| Kister et al., 2017 | Not focused on efficacy |
| Ronay et al., 2017 | Simulation of peri-implant defects |
| Bertoldi et al., 2017 | Not focused on efficacy |
| Tastepe et al., 2017 | No instrument comparison |
| Chen et al., 2016 | Not focused on efficacy |
| Rios et al., 2016 | Not focused on efficacy |
| Lang et al., 2016 | Not focused on efficacy |
| Park et al., 2015 | Not focused on efficacy |
| Yang et al., 2015 | Not focused on efficacy |
| Anastassiadis et al., 2015 | Not focused on efficacy |
| Sahrmann et al., 2015 | Simulation of peri-implant defects |
| Menini et al., 2015 | Not focused on efficacy |
| Schmage et al., 2012 | Not focused on efficacy |
| Park et al., 2013 | Not focused on efficacy |
| Sahrmann et al., 2013 | Simulation of peri-implant defects |
| Mussano et al., 2013 | Not focused on efficacy |
| Nemer Vieira et al., 2012 | Not focused on efficacy |
| Park et al., 2012 | Not focused on efficacy |
| Mann et al., 2012 | Not focused on efficacy |
References
- Baldi, D.; Menini, M.; Colombo, J.; Lertora, E.; Pera, P. Evaluation of a New Ultrasonic Insert for Prosthodontic Preparation. Int. J. Prosthodont. 2017, 30, 496–498. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Baldi, D.; Colombo, J.; Robiony, M.; Menini, M.; Bisagni, E.; Pera, P. Temperature variations in pulp chamber: An in-vitro comparison between ultrasonic and rotating instruments in tooth preparation. Part 1. Minerva Stomatol. 2020, 69, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Baldi, D.; Colombo, J.; Stacchi, C.; Menini, M.; Oronos, A.; Pera, P. Pulp vitality during ultrasonic tooth preparation. Part 2. Minerva Stomatol. 2020, 69, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Mann, M.; Parmar, D.; Walmsley, A.D.; Lea, S.C. Effect of plastic covered ultrasonic scalers on titanium implant surfaces. Clin. Oral Implant. Res. 2012, 23, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Menini, M.; Piccardo, P.; Baldi, D.; Dellepiane, E.; Pera, P. Morphological and chemical characteristics of different titanium surfaces treated by bicarbonate and glycine powder air abrasive systems. Implant. Dent. 2015, 24, 47–56. [Google Scholar] [CrossRef]
- Menini, M.; Setti, P.; Dellepiane, E.; Zunino, P.; Pera, P.; Pesce, P. Comparison of biofilm removal using glycine air polishing versus sodium bicarbonate air polishing or hand instrumentation on full-arch fixed implant rehabilitations: A split-mouth study. Quintessence Int. 2019, 8, 2–10. [Google Scholar]
- Menini, M.; Delucchi, F.; Bagnasco, F.; Pera, F.; Di Tullio, N.; Pesce, P. Efficacy of air-polishing devices without removal of implant-supported full-arch prostheses. Int. J. Oral Implantol. 2021, 14, 401–416. [Google Scholar]
- Sison, S.G. Implant Maintenance and the Dental Hygienist. Available online: http://www.kiezenoftrekken.nl/downloads/supimplant.pdf (accessed on 30 April 2021).
- Fody, A.; Marsh, L. Importance of Implant Maintenance. Dimens. Dent. Hyg. 2020, 18, 16–18, 21. Available online: https://dimensionsofdentalhygiene.com/article/importance-of-implant-maintenance/ (accessed on 30 April 2021).
- Lang, M.S.; Cerutis, D.R.; Miyamoto, T.; Nunn, M.E. Cell Attachment Following Instrumentation with Titanium and Plastic Instruments, Diode Laser, and Titanium Brush on Titanium, Titanium-Zirconium, and Zirconia Surfaces. Int. J. Oral Maxillofac. Implant. 2016, 31, 799–806. [Google Scholar] [CrossRef]
- Lupi, S.M.; Granati, M.; Butera, A.; Collesano, V.; Baena, R.R.Y. Air-abrasive debridement with glycine powder versus manual debridement and chlorhexidine administration for the maintenance of peri-implant health status: A six-month randomized clinical trial. Int. J. Dent. Hyg. 2016, 15, 287–294. [Google Scholar] [CrossRef]
- Yang, S.-M.; Park, J.-B.; Ko, Y. Use of confocal microscopy for quantification of plastic remnants on rough titanium after instrumentation and evaluation of efficacy of removal. Int. J. Oral Maxillofac. Implant. 2015, 30, 519–525. [Google Scholar] [CrossRef]
- Matsubara, V.H.; Leong, B.W.; Leong, M.J.L.; Lawrence, Z.; Becker, T.; Quaranta, A. Cleaning potential of different air abrasive powders and their impact on implant surface roughness. Clin. Implant. Dent. Relat. Res. 2020, 22, 96–104. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef]
- Howick, J.; Chalmers, I.; Glasziou, P.; Greenhalgh, T.; Heneghan, C.; Liberati, A. The 2011 Oxford CEBM Evidence Levels of Evidence (Introductory Document); Oxford Center for Evidence-Based Medicine: Oxford, UK, 2011; pp. 1–3. [Google Scholar]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle–Ottawa Scale (NOS) for Assessing the Quality of Non-Randomized Studies in Meta-Analysis; Ottawa Hospital Research Institute: Ottawa, ON, Canada, 2000; Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 30 September 2021).
- Higgins, J.P.T.; Green, S. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated 11]. In The Cochrane Collaboration; 20 March 2011; Available online: www.handbook.cochrane.org (accessed on 30 September 2021).
- Fletcher, P.; Linden, E.; Cobb, C.; Zhao, D.; Rubin, J.; Planzos, P. Efficacy of Removal of Residual Dental Cement by Laser, Ultrasonic Scalers, and Titanium Curette: An In Vitro Study. Compend Contin Educ Dent. 2021, 42, e5–e9. [Google Scholar]
- Tong, Z.; Fu, R.; Zhu, W.; Shi, J.; Yu, M.; Si, M. Changes in the surface topography and element proportion of clinically failed SLA implants after in vitro debridement by different methods. Clin. Oral Implant. Res. 2021, 32, 263–273. [Google Scholar] [CrossRef]
- Di Tinco, R.; Bertani, G.; Pisciotta, A.; Bertoni, L.; Bertacchini, J.; Colombari, B.; Conserva, E.; Blasi, E.; Consolo, U.; Carnevale, G. Evaluation of Antimicrobial Effect of Air-Polishing Treatments and Their Influence on Human Dental Pulp Stem Cells Seeded on Titanium Disks. Int. J. Mol. Sci. 2021, 22, 865. [Google Scholar] [CrossRef] [PubMed]
- Sirinirund, B.; Garaicoa-Pazmino, C.; Wang, H.L. Effects of Mechanical Instrumentation with Commercially Available Instruments Used in Supportive Peri-implant Therapy: An In Vitro Study. Int. J. Oral Maxillofac. Implant. 2019, 34, 1370–1378. [Google Scholar] [CrossRef]
- Schmidt, K.E.; Auschill, T.M.; Sculean, A.; Arweiler, N.B. Clinical evaluation of non-surgical cleaning modalities on titanium dental implants during maintenance care: A 1-year follow-up on prosthodontic superstructures. Clin. Oral Investig. 2019, 23, 1921–1930. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, K.E.; Auschill, T.M.; Heumann, C.; Frankenberger, R.; Eick, S.; Sculean, A.; Arweiler, N.B. Clinical and laboratory evaluation of the effects of different treatment modalities on titanium healing caps: A randomized, controlled clinical trial. Clin. Oral Investig. 2018, 22, 2149–2160. [Google Scholar] [CrossRef]
- Al Ghazal, L.; O’Sullivan, J.; Claffey, N.; Polyzois, I. Comparison of two different techniques used for the maintenance of peri-implant soft tissue health: A pilot randomized clinical trial. Acta Odontol. Scand. 2017, 75, 542–549. [Google Scholar] [CrossRef]
- Al-Hashedi, A.A.; Laurenti, M.; Benhamou, V.; Tamimi, F. Decontamination of titanium implants using physical methods. Clin. Oral Implant. Res. 2017, 28, 1013–1021. [Google Scholar] [CrossRef] [PubMed]
- Ziebolz, D.; Klipp, S.; Schmalz, G.; Schmickler, J.; Rinke, S.; Kottmann, T.; Fresmann, S.; Einwag, J. Comparison of different maintenance strategies within supportive implant therapy for prevention of peri-implant inflammation during the first year after implant restoration. A randomized, dental hygiene practice-based multicenter study. Am. J. Dent. 2017, 30, 190–196. [Google Scholar]
- Chun, K.A.; Kum, K.Y.; Lee, W.C.; Baek, S.H.; Choi, H.W.; Shon, W.J. Evaluation of the safety and efficiency of novel metallic implant scaler tips manufactured by the powder injection molding technique. BMC Oral Health 2017, 17, 110. [Google Scholar] [CrossRef]
- Matthes, R.; Duske, K.; Kebede, T.G.; Pink, C.; Schlüter, R.; von Woedtke, T.; Weltmann, K.D.; Kocher, T.; Jablonowski, L. Osteoblast growth, after cleaning of biofilm-covered titanium discs with air-polishing and cold plasma. J. Clin. Periodontol. 2017, 44, 672–680. [Google Scholar] [CrossRef] [PubMed]
- John, G.; Becker, J.; Schwarz, F. Effectivity of air-abrasive powder based on glycine and tricalcium phosphate in removal of initial biofilm on titanium and zirconium oxide surfaces in an ex vivo model. Clin. Oral Investig. 2016, 20, 711–719. [Google Scholar] [CrossRef]
- John, G.; Schwarz, F.; Becker, J. Taurolidine as an effective and biocompatible additive for plaque-removing techniques on implant surfaces. Clin. Oral Investig. 2015, 19, 1069–1077. [Google Scholar] [CrossRef] [PubMed]
- Schmage, P.; Kahili, F.; Nergiz, I.; Scorziello, T.M.; Platzer, U.; Pfeiffer, P. Cleaning effectiveness of implant prophylaxis instruments. Int. J. Oral Maxillofac. Implant. 2014, 29, 331–337. [Google Scholar] [CrossRef]
- Swierkot, K.; Brusius, M.; Leismann, D.; Nonnenmacher, C.; Nüsing, R.; Lubbe, D.; Schade-Brittinger, C.; Mengel, R. Manual versus sonic-powered toothbrushing for plaque reduction in patients with dental implants: An explanatory randomised controlled trial. Eur. J. Oral Implantol. 2013, 6, 133–144. [Google Scholar]
- Amate-Fernández, P.; Figueiredo, R.; Blanc, V.; Àlvarez, G.; León, R.; Valmaseda-Castellón, E. Erythritol-enriched powder and oral biofilm regrowth on dental implants: An in vitro study. Med. Oral Patol. Oral Cir. Bucal. 2021, 26, e602–e610. [Google Scholar] [CrossRef]
- Salles, M.M.; de Cássia Oliveira, V.; Macedo, A.P.; Silva-Lovato, C.H.; de Freitas de Oliveira Paranhos, H. Effectiveness of Brushing Associated with Oral Irrigation in Maintenance of Peri-Implant Tissues and Overdentures: Clinical Parameters and Patient Satisfaction. J. Oral Implantol. 2021, 47, 117–123. [Google Scholar] [CrossRef]
- Iatrou, P.; Chamilos, C.; Nickles, K.; Ratka, C.; Eickholz, P.; Petsos, H. In Vitro Efficacy of Three Different Nonsurgical Implant Surface Decontamination Methods in Three Different Defect Configurations. Int. J. Oral Maxillofac. Implant. 2021, 36, 271–280. [Google Scholar] [CrossRef] [PubMed]
- Salles, M.M.; Oliveira, V.C.; Macedo, A.P.; do Nascimento, C.; Silva-Lovato, C.H.; Paranhos, H.F.O. Brushing associated with oral irrigation in maintaining implants and overdentures hygiene—A randomized clinical trial. Odontology 2021, 109, 284–294. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Atsuta, I.; Ayukawa, Y.; Zhou, T.; Narimatsu, I.; Koyano, K. Effect of titanium or zirconia implant abutments on epithelial attachments after ultrasonic cleaning. J. Oral Sci. 2020, 62, 331–334. [Google Scholar] [CrossRef] [PubMed]
- Mensi, M.; Viviani, L.; Agosti, R.; Scotti, E.; Garzetti, G.; Calza, S. Comparison between four different implant surface debridement methods: An in-vitro experimental study. Minerva Stomatol. 2020, 69, 286–294. [Google Scholar] [CrossRef]
- Hu, J.; Atsuta, I.; Ayukawa, Y.; Zhou, X.; Dwi Rakhmatia, Y.; Koyano, K. The impact of surface alteration on epithelial tissue attachment after the mechanical cleaning of titanium or zirconia surface. J. Oral Rehabil. 2020, 47, 1065–1076. [Google Scholar] [CrossRef]
- Gümüş, K.Ç.; Ustaoğlu, G.; Kara, L.; Ercan, E.; Albayrak, Ö.; Tunali, M. Nano-Hydroxyapatite Airborne-Particle Abrasion System as an Alternative Surface Treatment Method on Intraorally Contaminated Titanium Discs. Int. J. Periodontics Restorative Dent. 2020, 40, e179–e187. [Google Scholar] [CrossRef]
- Vyas, N.; Sammons, R.L.; Kuehne, S.A.; Johansson, C.; Stenport, V.; Wang, Q.X.; Walmsley, A.D. The effect of standoff distance and surface roughness on biofilm disruption using cavitation. PLoS ONE 2020, 15, e0236428. [Google Scholar] [CrossRef]
- Vyas, N.; Grewal, M.; Kuehne, S.A.; Sammons, R.L.; Walmsley, A.D. High speed imaging of biofilm removal from a dental implant model using ultrasonic cavitation. Dent. Mater. 2020, 36, 733–743. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.S.; Hung, C.Y.; Huang, H.H. Surface changes and bacterial adhesion on implant abutment materials after various clinical cleaning procedures. J. Chin. Med. Assoc. 2019, 82, 643–650. [Google Scholar] [CrossRef]
- Cha, J.K.; Paeng, K.; Jung, U.W.; Choi, S.H.; Sanz, M.; Sanz-Martín, I. The effect of five mechanical instrumentation protocols on implant surface topography and roughness: A scanning electron microscope and confocal laser scanning microscope analysis. Clin. Oral Implant. Res. 2019, 30, 578–587. [Google Scholar] [CrossRef]
- Keim, D.; Nickles, K.; Dannewitz, B.; Ratka, C.; Eickholz, P.; Petsos, H. In vitro efficacy of three different implant surface decontamination methods in three different defect configurations. Clin. Oral Implant. Res. 2019, 30, 550–558. [Google Scholar] [CrossRef] [PubMed]
- Biazussi, B.R.; Perrotti, V.; D’Arcangelo, C.; Elias, C.N.; Bianchini, M.A.; Tumedei, M.; de Vasconcellos, D.K. Evaluation of the Effect of Air Polishing With Different Abrasive Powders on the Roughness of Implant Abutment Surface: An In Vitro Study. J. Oral Implantol. 2019, 45, 202–206. [Google Scholar] [CrossRef] [PubMed]
- Harrel, S.K.; Wilson, T.G., Jr.; Pandya, M.; Diekwisch, T.G.H. Titanium particles generated during ultrasonic scaling of implants. J. Periodontol. 2019, 90, 241–246. [Google Scholar] [CrossRef]
- Takagi, T.; Aoki, A.; Ichinose, S.; Taniguchi, Y.; Tachikawa, N.; Shinoki, T.; Meinzer, W.; Sculean, A.; Izumi, Y. Effective removal of calcified deposits on microstructured titanium fixture surfaces of dental implants with erbium lasers. J. Periodontol. 2018, 89, 680–690. [Google Scholar] [CrossRef]
- Cao, J.; Wang, T.; Pu, Y.; Tang, Z.; Meng, H. Influence on proliferation and adhesion of human gingival fibroblasts from different titanium surface decontamination treatments: An in vitro study. Arch. Oral Biol. 2018, 87, 204–210. [Google Scholar] [CrossRef]
- Quintero, D.G.; Taylor, R.B.; Miller, M.B.; Merchant, K.R.; Pasieta, S.A. Air-Abrasive Disinfection of Implant Surfaces in a Simulated Model of Periimplantitis. Implant. Dent. 2017, 26, 423–428. [Google Scholar] [CrossRef]
- Schmidt, K.E.; Auschill, T.M.; Heumann, C.; Frankenberger, R.; Eick, S.; Sculean, A.; Arweiler, N.B. Influence of different instrumentation modalities on the surface characteristics and biofilm formation on dental implant neck, in vitro. Clin. Oral Implant. Res. 2017, 28, 483–490. [Google Scholar] [CrossRef]
- Hakki, S.S.; Tatar, G.; Dundar, N.; Demiralp, B. The effect of different cleaning methods on the surface and temperature of failed titanium implants: An in vitro study. Lasers Med. Sci. 2017, 32, 563–571. [Google Scholar] [CrossRef]
- Kister, F.; Specht, O.; Warkentin, M.; Geis-Gerstorfer, J.; Rupp, F. Peri-implantitis cleaning instrumentation influences the integrity of photoactive nanocoatings. Dent. Mater. 2017, 33, e69–e78. [Google Scholar] [CrossRef] [PubMed]
- Ronay, V.; Merlini, A.; Attin, T.; Schmidlin, P.R.; Sahrmann, P. In vitro cleaning potential of three implant debridement methods. Simulation of the non-surgical approach. Clin. Oral Implant. Res. 2017, 28, 151–155. [Google Scholar] [CrossRef] [PubMed]
- Bertoldi, C.; Lusuardi, D.; Battarra, F.; Sassatelli, P.; Spinato, S.; Zaffe, D. The maintenance of inserted titanium implants: In-vitro evaluation of exposed surfaces cleaned with three different instruments. Clin. Oral Implant. Res. 2017, 28, 57–63. [Google Scholar] [CrossRef]
- Larsen, O.I.; Enersen, M.; Kristoffersen, A.K.; Wennerberg, A.; Bunæs, D.F.; Lie, S.A.; Leknes, K.N. Antimicrobial Effects of Three Different Treatment Modalities on Dental Implant Surfaces. J. Oral Implantol. 2017, 43, 429–436. [Google Scholar] [CrossRef]
- Tastepe, C.S.; Lin, X.; Donnet, M.; Wismeijer, D.; Liu, Y. Parameters That Improve Cleaning Efficiency of Subgingival Air Polishing on Titanium Implant Surfaces: An In Vitro Study. J. Periodontol. 2017, 88, 407–414. [Google Scholar] [CrossRef]
- Chen, C.J.; Ding, S.J.; Chen, C.C. Effects of Surface Conditions of Titanium Dental Implants on Bacterial Adhesion. Photomed. Laser Surg. 2016, 34, 379–388. [Google Scholar] [CrossRef]
- Rios, F.G.; Viana, E.R.; Ribeiro, G.M.; González, J.C.; Abelenda, A.; Peruzzo, D.C. Temperature evaluation of dental implant surface irradiated with high-power diode laser. Lasers Med. Sci. 2016, 31, 1309–1316. [Google Scholar] [CrossRef]
- Park, J.B.; Lee, S.H.; Kim, N.; Park, S.; Jin, S.H.; Choi, B.K.; Kim, K.K.; Ko, Y. Instrumentation with Ultrasonic Scalers Facilitates Cleaning of the Sandblasted and Acid-Etched Titanium Implants. J. Oral Implantol. 2015, 41, 419–428. [Google Scholar] [CrossRef]
- Anastassiadis, P.M.; Hall, C.; Marino, V.; Bartold, P.M. Surface scratch assessment of titanium implant abutments and cementum following instrumentation with metal curettes. Clin. Oral Investig. 2015, 19, 545–551. [Google Scholar] [CrossRef]
- Sahrmann, P.; Ronay, V.; Hofer, D.; Attin, T.; Jung, R.E.; Schmidlin, P.R. In vitro cleaning potential of three different implant debridement methods. Clin. Oral Implant. Res. 2015, 26, 314–319. [Google Scholar] [CrossRef] [PubMed]
- Park, J.B.; Jang, Y.J.; Choi, B.K.; Kim, K.K.; Ko, Y. Treatment with various ultrasonic scaler tips affects efficiency of brushing of SLA titanium discs. J. Craniofac. Surg. 2013, 24, e119–e123. [Google Scholar] [CrossRef] [PubMed]
- Sahrmann, P.; Ronay, V.; Sener, B.; Jung, R.E.; Attin, T.; Schmidlin, P.R. Cleaning potential of glycine air-flow application in an in vitro peri-implantitis model. Clin. Oral Implant. Res. 2013, 24, 666–670. [Google Scholar] [CrossRef] [PubMed]
- Mussano, F.; Rovasio, S.; Schierano, G.; Baldi, I.; Carossa, S. The effect of glycine-powder airflow and hand instrumentation on peri-implant soft tissues: A split-mouth pilot study. Int. J. Prosthodont. 2013, 26, 42–44. [Google Scholar] [CrossRef]
- Vieira, L.F.N.; Cardoso, E.S.; Machado, S.J.; da Silva, C.P.; Vidigal, G.M., Jr. Effectiveness of implant surface decontamination using a high-pressure sodium bicarbonate protocol: An in vitro study. Implant. Dent. 2012, 21, 390–393. [Google Scholar] [CrossRef] [PubMed]
- Park, J.B.; Kim, N.; Ko, Y. Effects of ultrasonic scaler tips and toothbrush on titanium disc surfaces evaluated with confocal microscopy. J. Craniofac. Surg. 2012, 23, 1552–1558. [Google Scholar] [CrossRef] [PubMed]
- Schmage, P.; Thielemann, J.; Nergiz, I.; Scorziello, T.M.; Pfeiffer, P. Effects of 10 cleaning instruments on four different implant surfaces. Int. J. Oral Maxillofac. Implant. 2012, 27, 308–317. [Google Scholar]

| Author(s) | Publication Year | Title | Study Design | Surface Treated | Number of Samples | Instruments Compared | Outcomes/Methodology | Results |
|---|---|---|---|---|---|---|---|---|
| Menini M, Delucchi F, Bagnasco F, Pera F, Di Tullio N, Pesce P. | 2021 | Efficacy of air-polishing devices without removal of implant-supported full-arch prostheses. | Randomized controlled trial | Titanium implants and conical abutments | 357 | Air polishing with glycine powder, ultrasonic device with a polyetheretherketone fibre tip, carbon fibre curettes, sponge floss | Plaque Index, peri-implant spontaneous bleeding, probing depth and bleeding on probing | Glycine powder air polishing resulted in a significantly higher reduction in plaque around implants. |
| Fletcher P, Linden E, Cobb C, Zhao D, Rubin J, Planzos P. | 2021 | Efficacy of Removal of Residual Dental Cement by Laser, Ultrasonic Scalers, and Titanium Curette: An In Vitro Study. | In vitro study | Implants with 3 different surface textures | 39 | Dental lasers, ultrasonic scalers, titanium curette | Scanning electron microscopy (SEM) | No treatment removed all residual cement from any of the 3 implant surfaces. |
| Tong Z, Fu R, Zhu W, Shi J, Yu M, Si M. | 2021 | Changes in the surface topography and element proportion of clinically failed SLA implants after in vitro debridement by different methods. | In vitro study | Implants | 30 | Physiologic saline irrigation, glycine powder, ethylenediaminetetraacetic acid (EDTA), ultrasonic scaler with polyetheretherketone (PEEK) tip | Relative contaminated area reduction (RCAR), visual analogue scale (VAS) and surface roughness assessed using scanning electron microscopy (SEM), stereoscopic microscopy (SM), white light interferometry (WLI) | PEEK tip ultrasonic scaling was more effective in eliminating visible contamination. |
| Di Tinco R, Bertani G, Pisciotta A, Bertoni L, Bertacchini J, Colombari B, Conserva E, Blasi E, Consolo U, Carnevale G. | 2021 | Evaluation of Antimicrobial Effect of Air-Polishing Treatments and Their Influence on Human Dental Pulp Stem Cells Seeded on Titanium Disks. | In vitro study | Titanium disks | - | Glycine and tagatose powders | Immunofluorescence analyses | Both the powders have a great in vitro cleaning potential. |
| Matsubara VH, Leong BW, Leong MJL, Lawrence Z, Becker T, Quaranta A. | 2020 | Cleaning potential of different air abrasive powders and their impact on implant surface roughness. | In vitro study | Implants | 20 | Sodium bicarbonate, glycine, Erythritol, water alone | Digital photography, graphic software, SEM and optical profilometry | Large-sized powder showed the greatest cleaning capacity, but caused more alterations to the implant surface. |
| Sirinirund B, Garaicoa-Pazmino C, Wang HL. | 2019 | Effects of Mechanical Instrumentation with Commercially Available Instruments Used in Supportive Peri-implant Therapy: An In Vitro Study. | In vitro study | Implants | 14 | Three curettes (stainless steel, plastic, titanium), two ultrasonic tips (metal tip, plastic tip), a titanium brush, and an air-polishing device | Stereomicroscopy, atomic force microscopy, and SEM | Artificial calculus removal by mechanical instrumentation, with the exception of PT, was proven to be clinically effective. |
| Menini M, Setti P, Dellepiane E, Zunino P, Pera P, Pesce P | 2019 | Comparison of biofilm removal using glycine air polishing versus sodium bicarbonate air polishing or hand instrumentation on full-arch fixed implant rehabilitations: a split-mouth study | Randomized controlled trial | Titanium implants and conical abutments | 134 | Glycine air polishing, sodium bicarbonate air polishing, manual scaling with carbon-fiber curette | Spontaneous Bleeding (SB), Plaque Index (PI) were recorded before and after hygiene. Patient’s satisfaction towards the three techniques was analyzed by questionnaires | Sodium bicarbonate air polishing was the most effective method for plaque reduction but was more aggressive on soft tissue and was the least preferred treatment by patients. Glycine powder air polishing was both clinically effective for plaque removal and highly accepted by patients |
| Schmidt KE, Auschill TM, Sculean A, Arweiler NB | 2019 | Clinical evaluation of non-surgical cleaning modalities on titanium dental implants during maintenance care: a 1-year follow-up on prosthodontic superstructures | Randomized controlled trial | Implants | 32 | Titanium curettes, stainless steel ultrasonic tip, erythritol air-polishing or rubber cup polishing | Probing depths (PDs), bleeding on probing (BOP), modified gingival (mucosal) bleeding index (GBI) around implants | All tested treatment modalities yielded comparable clinical improvements |
| Schmidt KE, Auschill TM, Heumann C, Frankenberger R, Eick S, Sculean A, Arweiler NB. | 2018 | Clinical and laboratory evaluation of the effects of different treatment modalities on titanium healing caps: a randomized, controlled clinical trial. | Randomized controlled trial | Titanium healing caps | 72 | Titanium curettes, stainless steel ultrasonic tip, erythritol air-polishing powder, rubber cup polishing | Probing depths (PD), bleeding on probing (BOP), matrix metalloproteinase 8 (MMP-8), and periopathogens | All treatments performed yielded comparable outcomes. |
| Lupi SM, Granati M, Butera A, Collesano V, Rodriguez Y Baena R. | 2017 | Air-abrasive debridement with glycine powder versus manual debridement and chlorhexidine administration for the maintenance of peri-implant health status: a six-month randomized clinical trial. | Randomized clinical trial | Implants | 88 | Glycine powder, manual debridement and clorexidine | Plaque index (PI), bleeding index (BOP), probing depth (PD), clinical attachment level (CAL) and bleeding score (BS) | Treatment with glycine seems more effective than the traditional treatment with plastic curette and chlorhexidine. |
| Al Ghazal L, O’Sullivan J, Claffey N, Polyzois I. | 2017 | Comparison of two different techniques used for the maintenance of peri-implant soft tissue health: a pilot randomized clinical trial. | Pilot randomized clinical trial | Implants | 25 | Low abrasive air polishing powder (Air-Flow® Perio, EMS), titanium curettes | Bleeding on probing (BOP), peri-implant crevicular fluid analysis | Both treatment methods were proven to be effective in reducing peri-implant inflammation and preventing further disease progression. |
| Al-Hashedi AA, Laurenti M, Benhamou V, Tamimi F | 2017 | Decontamination of titanium implants using physical methods. | In vitro study | Implants | - | Metal and plastic curettes, Ti brushes and Er: YAG laser | SEM, X-ray photoelectron spectroscopy, live-dead assays | Ti brushes were more effective than curettes (metal or plastic) and Er: YAG laser in decontaminating Ti implant surfaces. |
| Ziebolz D, Klipp S, Schmalz G, Schmickler J, Rinke S, Kottmann T, Fresmann S, Einwag J | 2017 | Comparison of different maintenance strategies within supportive implant therapy for prevention of peri-implant inflammation during the first year after implant restoration. A randomized, dental hygiene practice-based multicenter study | Clinical trial | Implants | 101 | Manual curettes, a sonic-driven scaler, and a prophylaxis brush, chlorhexidine (CHX) varnish, air polishing with glycine powder | Peri-implant probing depths (PPD), mucosal recession (MR), and bleeding on probing (BOP) | All strategies were effective in preventing peri-implant inflammation. The supplemental application of chlorhexidine varnish had no significant additional benefit |
| Chun KA, Kum KY, Lee WC, Baek SH, Choi HW, Shon WJ. | 2017 | Evaluation of the safety and efficiency of novel metallic implant scaler tips manufactured by the powder injection molding technique. | In vitro study | Titanium surfaces | Copper (CU), bronze, 316 L stainless steel (SS), conventional stainless steel ultrasonic tips | SEM, confocal laser scanning microscopy (CLSM) | The efficiency of the SS tip was about 3 times higher than that of CU tip. | |
| Matthes R, Duske K, Kebede TG, Pink C, Schlüter R, von Woedtke T, Weltmann KD, Kocher T, Jablonowski L. | 2017 | Osteoblast growth, after cleaning of biofilm-covered titanium discs with air-polishing and cold plasma. | In vitro study | Titanium disks | Erythritol powder (AP), cold atmospheric pressure argon plasma | SEM | An AP treatment has the potential to remove biofilm from rough implant surfaces completely. | |
| John G, Becker J, Schwarz F. | 2016 | Effectivity of air-abrasive powder based on glycine and tricalcium phosphate in removal of initial biofilm on titanium and zirconium oxide surfaces in an ex vivo model. | Ex vivo study | Implants | 138 | Sodium bicarbonate, glycine, glycine + tricalcium phosphate | Residual plaque areas (RPA) and treatment time | Glycine + tricalcium phosphate seemed to be more effective than the control groups for biofilm removal on titanium and zirconium implant surfaces. |
| John G, Schwarz F, Becker J | 2015 | Taurolidine as an effective and biocompatible additive for plaque-removing techniques on implant surfaces. | In vitro study | Implants | - | Plastic curettes (PC) and glycine powder airflow (GLY) in combination with taurolidine (T), chlorhexidine (CHX), or pure water (PW) | Plaque Index, clean implant surface (CIS) | Taurolidine seems to enhance effectiveness of plaque-removing procedures with plastic curettes and glycine powder airflow. |
| Schmage P, Kahili F, Nergiz I, Scorziello TM, Platzer U, Pfeiffer P. | 2014 | Cleaning effectiveness of implant prophylaxis instruments. | In vitro study | Titanium disks | 80 | Manual plastic curette, manual carbon fiber-reinforced plastic (CFRP) curette, sonic-driven prophylaxis brush, rotating rubber cup with prophylaxis paste, sonic-driven polyether ether ketone (PEEK) plastic tip, ultrasonic-driven PEEK plastic tip, and air polishing with amino acid (glycine) powder | Light microscopy | The cleaning effectiveness of the plastic curette was significantly lower.Superior results, with less than 4% of the biofilm remaining, were obtained for both oscillating PEEK plastic tips and air polishing. |
| Swierkot K, Brusius M, Leismann D, Nonnenmacher C, Nüsing R, Lubbe D, Schade-Brittinger C, Mengel R | 2013 | Manual versus sonic-powered toothbrushing for plaque reduction in patients with dental implants: an explanatory randomised controlled trial. | Randomized controlled trial | Implants | - | Sonic toothbrush, manual toothbrush | Real-time polymerase chain reaction, chromatography-electrospray spectrometry | The plaque index difference between baseline and 12 months at implants showed no significant difference between sonic or manual toothbrushing. |
| Study | Selection | Comparability | Outcome/Exposure | NOS Score |
|---|---|---|---|---|
| Ziebolz et al. 2017 | ••◦◦ | •◦ | ◦◦•• | 5 |
| John et al. 2016 | ••◦◦ | •◦ | ◦◦•• | 5 |
| Study | Selection Bias Sequence Generation | Selection Bias Allocation Concealment | Performance Bias | Detection Bias | Attrition Bias | Selective Reporting Bias | Other Potential Risk of Bias |
|---|---|---|---|---|---|---|---|
| Menini et al., 2021 | Low | Low | High | Unclear | Low | Low | Low |
| Menini et al., 2019 | Low | Low | High | Low | Low | Low | Low |
| Schmidt et al., 2019 | Low | High | High | Low | High | Low | Low |
| Schmidt et al., 2018 | Low | High | High | Low | High | Low | Low |
| Lupi et al., 2017 | Low | Low | High | Unclear | Low | Low | Low |
| Al Ghazal et al., 2017 | Low | High | High | Unclear | Low | Low | Low |
| Swierkot et al., 2013 | Low | Unclear | High | Unclear | Low | Low | Low |
| Level of Evidence Oxford | |||
|---|---|---|---|
| Study | Reference Number | Degree of Recommendation | Level of Evidence |
| Fletcher et al., 2021 | 19 | B | 2C |
| Tong et al., 2021 | 20 | B | 2C |
| Di Tinco et al., 2021 | 21 | B | 2C |
| Matsubara et al., 2020 | 13 | B | 2C |
| Sirinirund et al., 2019 | 22 | B | 2C |
| Al-Hashedi et al., 2017 | 26 | B | 2C |
| Chun et al., 2017 | 28 | B | 2C |
| Matthes et al., 2017 | 29 | B | 2C |
| John et al., 2015 | 31 | B | 2C |
| Schmage et al., 2014 | 32 | B | 2C |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baldi, D.; De Giorgis, L.; Menini, M.; Motta, F.; Colombo, J. Efficacy of Instruments for Professional Oral Hygiene on Dental Implants: A Systematic Review. Appl. Sci. 2022, 12, 26. https://doi.org/10.3390/app12010026
Baldi D, De Giorgis L, Menini M, Motta F, Colombo J. Efficacy of Instruments for Professional Oral Hygiene on Dental Implants: A Systematic Review. Applied Sciences. 2022; 12(1):26. https://doi.org/10.3390/app12010026
Chicago/Turabian StyleBaldi, Domenico, Luisa De Giorgis, Maria Menini, Franco Motta, and Jacopo Colombo. 2022. "Efficacy of Instruments for Professional Oral Hygiene on Dental Implants: A Systematic Review" Applied Sciences 12, no. 1: 26. https://doi.org/10.3390/app12010026
APA StyleBaldi, D., De Giorgis, L., Menini, M., Motta, F., & Colombo, J. (2022). Efficacy of Instruments for Professional Oral Hygiene on Dental Implants: A Systematic Review. Applied Sciences, 12(1), 26. https://doi.org/10.3390/app12010026