
Deep Learning Based Airway Segmentation Using Key Point Prediction

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Sample Collection and Information
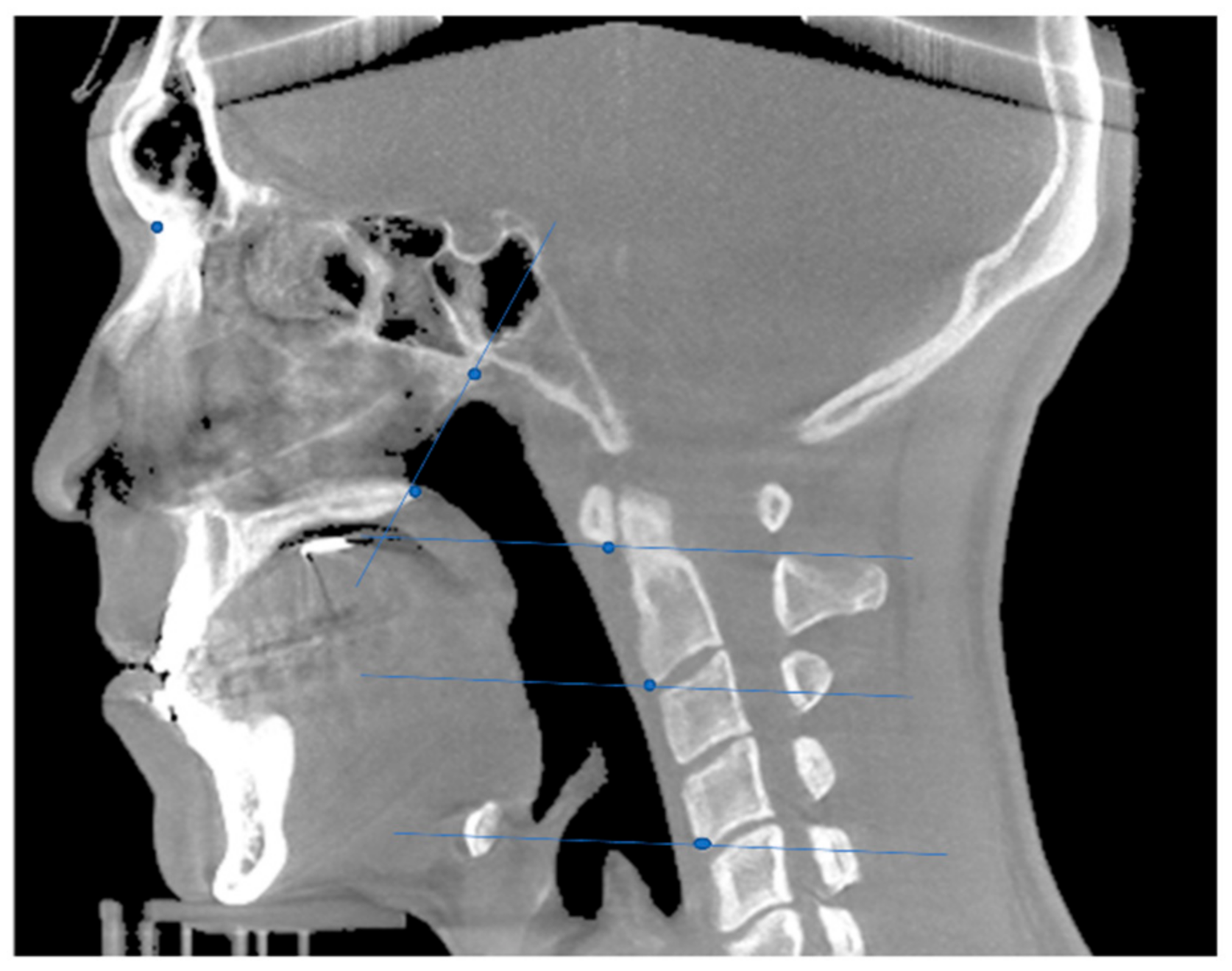
2.2. Coordinate Determination in the Mid-Sagittal Plane
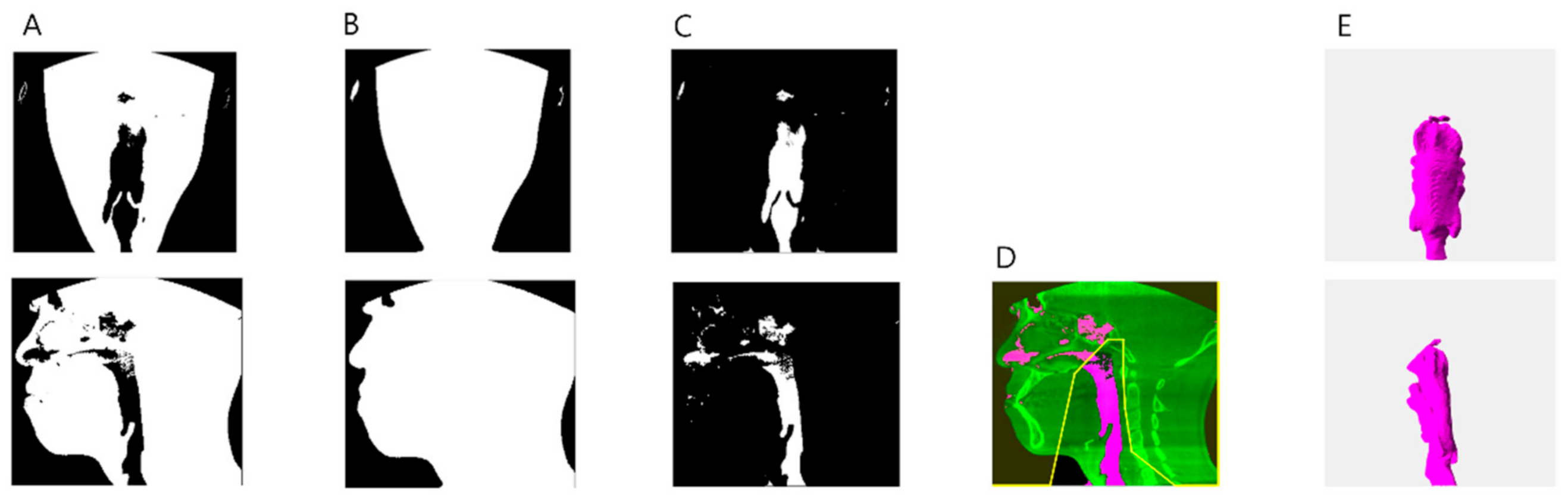
2.3. Airway Segmentation
2.4. Training via Regression Neural Network and Metrics for Accuracy Comparison
3. Results
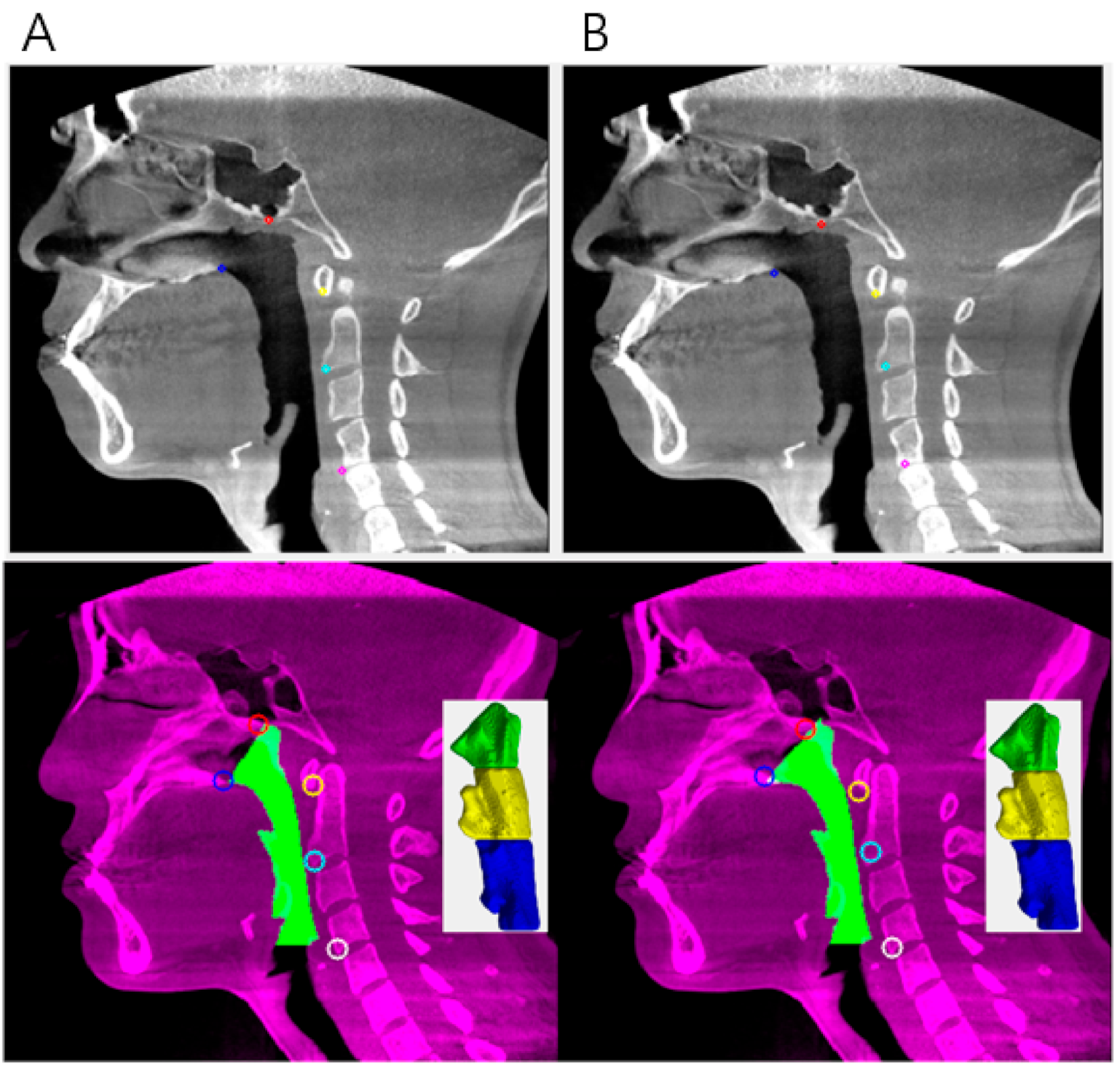
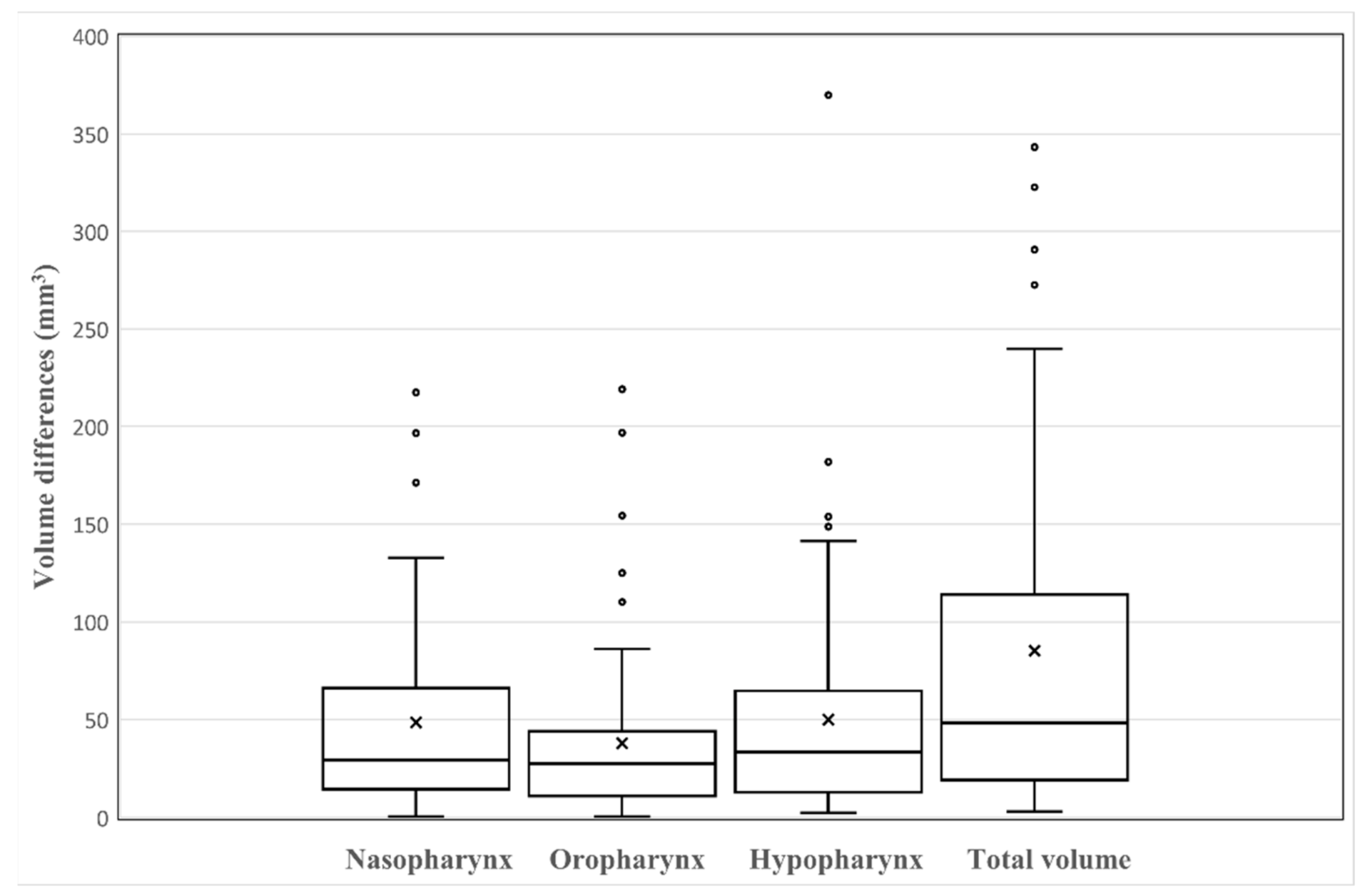
3.1. Measurements of the Differences between Manual Analysis and Deep Learning Analysis
3.2. Agreement Analysis
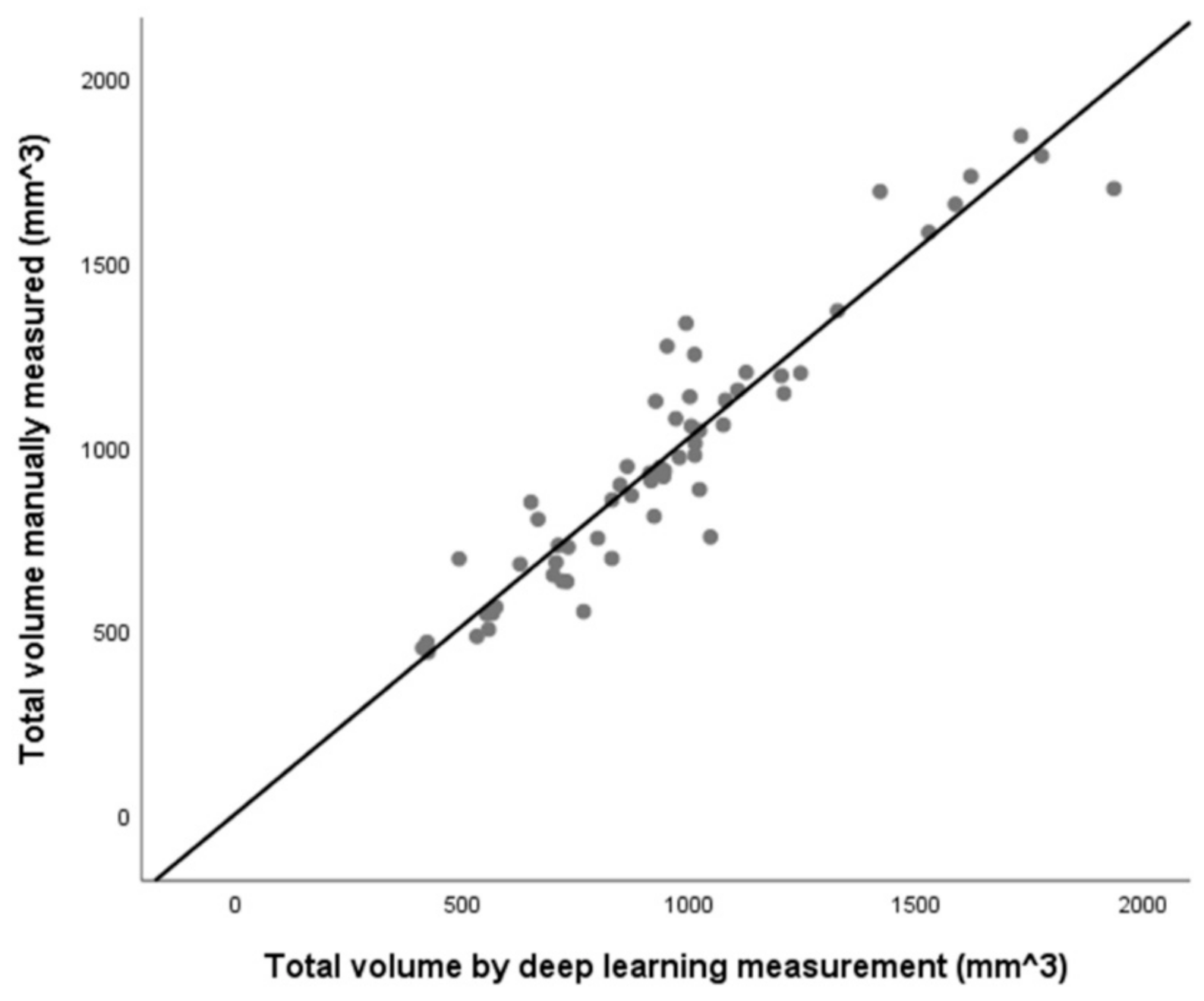
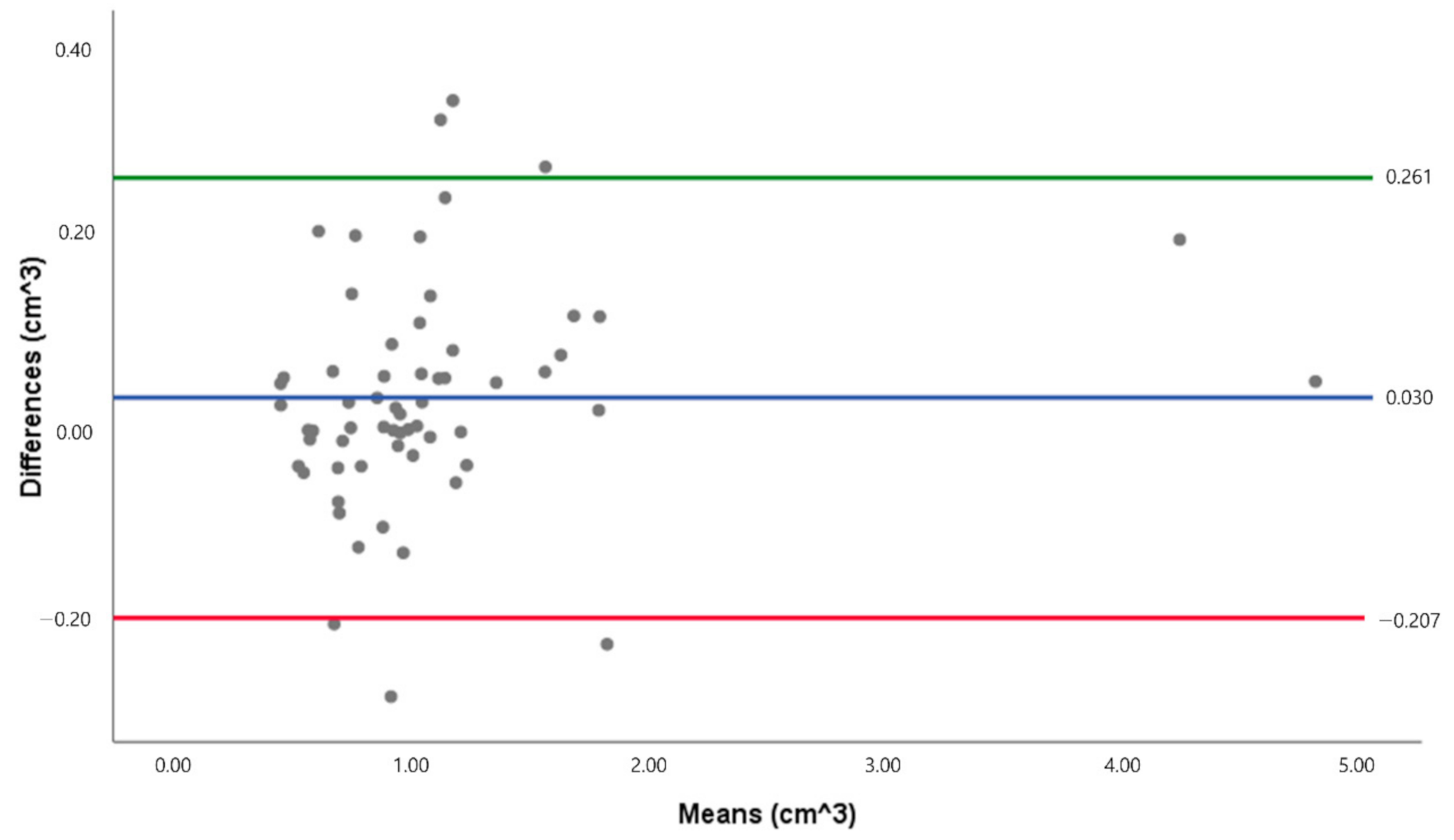
3.3. Linear Regression Scatter Plots and Bland-Altman Plot for the Total Volume Data Set
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yu, K.H.; Beam, A.L.; Kohane, I.S. Artificial intelligence in healthcare. Nat. Biomed. Eng. 2018, 2, 719–731. [Google Scholar] [CrossRef] [PubMed]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Anwar, S.M.; Majid, M.; Qayyum, A.; Awais, M.; Alnowami, M.; Khan, M.K. Medical Image Analysis using Convolutional Neural Networks: A Review. J. Med. Syst. 2018, 42, 226. [Google Scholar] [CrossRef] [PubMed]
- El Naqa, I.; Haider, M.A.; Giger, M.L.; Ten Haken, R.K. Artificial Intelligence: Reshaping the practice of radiological sciences in the 21st century. Br. J. Radiol. 2020, 93, 20190855. [Google Scholar] [CrossRef] [PubMed]
- Fourcade, A.; Khonsari, R.H. Deep learning in medical image analysis: A third eye for doctors. J. Stomatol. Oral Maxillofac. Surg. 2019, 120, 279–288. [Google Scholar] [CrossRef] [PubMed]
- Cho, Y.S.; Cho, K.; Park, C.J.; Chung, M.J.; Kim, J.H.; Kim, K.; Kim, Y.K.; Kim, H.J.; Ko, J.W.; Cho, B.H.; et al. Automated measurement of hydrops ratio from MRI in patients with Meniere’s disease using CNN-based segmentation. Sci. Rep. 2020, 10. [Google Scholar] [CrossRef] [PubMed]
- De Water, V.R.; Saridin, J.K.; Bouw, F.; Murawska, M.M.; Koudstaal, M.J. Measuring Upper Airway Volume: Accuracy and Reliability of Dolphin 3D Software Compared to Manual Segmentation in Craniosynostosis Patients. J. Stomatol. Oral Maxillofac. Surg. 2014, 72, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Alsufyani, N.A.; Hess, A.; Noga, M.; Ray, N.; Al-Saleh, M.A.Q.; Lagravere, M.O.; Major, P.W. New algorithm for semiautomatic segmentation of nasal cavity and pharyngeal airway in comparison with manual segmentation using cone-beam computed tomography. Am. J. Orthod. Dentofac. 2016, 150, 703–712. [Google Scholar] [CrossRef]
- Weissheimer, A.; de Menezes, L.M.; Sameshima, G.T.; Enciso, R.; Pham, J.; Grauer, D. Imaging software accuracy for 3-dimensional analysis of the upper airway. Am. J. Orthod. Dentofac. 2012, 142, 801–813. [Google Scholar] [CrossRef]
- Ruckschloss, T.; Ristow, O.; Berger, M.; Engel, M.; Freudlsperger, C.; Hoffmann, J.; Seeberger, R. Relations between mandible-only advancement surgery, the extent of the posterior airway space, and the position of the hyoid bone in Class II patients: A three-dimensional analysis. Br. J. Oral Maxillofac. Surg. 2019, 57, 1032–1038. [Google Scholar] [CrossRef]
- Ruckschloss, T.; Ristow, O.; Jung, A.; Roser, C.; Pilz, M.; Engel, M.; Hoffmann, J.; Seeberger, R. The relationship between bimaxillary orthognathic surgery and the extent of posterior airway space in class II and III patients—A retrospective three-dimensional cohort analysis. J. Oral Maxillofac. Pathol. 2021, 33, 30–38. [Google Scholar] [CrossRef]
- Kamano, E.; Terajima, M.; Kitahara, T.; Takahashi, I. Three-dimensional analysis of changes in pharyngeal airway space after mandibular setback surgery. Orthod. Waves 2017, 76, 1–8. [Google Scholar] [CrossRef]
- Jang, S.I.; Ahn, J.; Paeng, J.Y.; Hong, J. Three-dimensional analysis of changes in airway space after bimaxillary orthognathic surgery with maxillomandibular setback and their association with obstructive sleep apnea. Maxillofac. Plast. Reconstr. Surg. 2018, 40, 33. [Google Scholar] [CrossRef]
- Kim, S.C.; Min, K.; Jeong, W.S.; Kwon, S.M.; Koh, K.S.; Choi, J.W. Three-Dimensional Analysis of Airway Change After LeFort III Midface Advancement with Distraction. Ann. Plast. Surg. 2018, 80, 359–363. [Google Scholar] [CrossRef]
- Niu, X.W.; Di Carlo, G.; Cornelis, M.A.; Cattaneo, P.M. Three-dimensional analyses of short- and long-term effects of rapid maxillary expansion on nasal cavity and upper airway: A systematic review and meta-analysis. Orthod. Craniofac. Res. 2020, 23, 250–276. [Google Scholar] [CrossRef]
- Yamashita, A.L.; Iwaki, L.; Leite, P.C.C.; Navarro, R.D.; Ramos, A.L.; Previdelli, I.T.S.; Ribeiro, M.H.D.; Iwaki, L.C.V. Three-dimensional analysis of the pharyngeal airway space and hyoid bone position after orthognathic surgery. J. Craniomaxillofac. Surg. 2017, 45, 1408–1414. [Google Scholar] [CrossRef]
- Wen, X.; Wang, X.Y.; Qin, S.Q.; Franchi, L.; Gu, Y. Three-dimensional analysis of upper airway morphology in skeletal Class Ill patients with and without mandibular asymmetry. Angle Orthod. 2017, 87, 526–533. [Google Scholar] [CrossRef]
- Louro, R.S.; Calasans-Maia, J.A.; Mattos, C.T.; Masterson, D.; Calasans-Maia, M.D.; Maia, L.C. Three-dimensional changes to the upper airway after maxillomandibular advancement with counterclockwise rotation: A systematic review and meta-analysis. Int. J. Oral Maxillofac. Surg. 2018, 47, 622–629. [Google Scholar] [CrossRef]
- Tan, S.K.; Tang, A.T.H.; Leung, W.K.; Zwahlen, R.A. Three-Dimensional Pharyngeal Airway Changes After 2-Jaw Orthognathic Surgery with Segmentation in Dento-Skeletal Class III Patients. J. Craniofac. Surg. 2019, 30, 1533–1538. [Google Scholar] [CrossRef]
- Christovam, I.O.; Lisboa, C.O.; Ferreira, D.M.T.P.; Cury-Saramago, A.A.; Mattos, C.T. Upper airway dimensions in patients undergoing orthognathic surgery: A systematic review and meta-analysis. Int. J. Oral Maxillofac. Surg. 2016, 45, 460–471. [Google Scholar] [CrossRef]
- Bianchi, A.; Betti, E.; Tarsitano, A.; Morselli-Labate, A.M.; Lancellotti, L.; Marchetti, C. Volumetric three-dimensional computed tomographic evaluation of the upper airway in patients with obstructive sleep apnoea syndrome treated by maxillomandibular advancement. Br. J. Oral Maxillofac. Surg. 2014, 52, 831–837. [Google Scholar] [CrossRef] [PubMed]
- Stratemann, S.; Huang, J.C.; Maki, K.; Hatcher, D.; Miller, A.J. Three-dimensional analysis of the airway with cone-beam computed tomography. Am. J. Orthod. Dentofac. 2011, 140, 607–615. [Google Scholar] [CrossRef] [PubMed]
- Alsufyani, N.A.; Flores-Mir, C.; Major, P.W. Three-dimensional segmentation of the upper airway using cone beam CT: A systematic review. Dentomaxillofac. Radiol. 2012, 41, 276–284. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; van Eijnatten, M.; Wolff, J.; de Lange, J.; van der Stelt, P.F.; Lobbezoo, F.; Aarab, G. Reliability and accuracy of three imaging software packages used for 3D analysis of the upper airway on cone beam computed tomography images. Dentomaxillofac. Radiol. 2017, 46. [Google Scholar] [CrossRef]
- Torres, H.M.; Evangelista, K.; Torres, E.M.; Estrela, C.; Leite, A.F.; Valladares-Neto, J.; Silva, M.A.G. Reliability and validity of two software systems used to measure the pharyngeal airway space in three-dimensional analysis. Int. J. Oral Maxillofac. Surg. 2020, 49, 602–613. [Google Scholar] [CrossRef]
- Burkhard, J.P.M.; Dietrich, A.D.; Jacobsen, C.; Roos, M.; Lubbers, H.T.; Obwegeser, J.A. Cephalometric and three-dimensional assessment of the posterior airway space and imaging software reliability analysis before and after orthognathic surgery. J. Craniomaxillofac. Surg. 2014, 42, 1428–1436. [Google Scholar] [CrossRef]
- Zimmerman, J.N.; Lee, J.; Pliska, B.T. Reliability of upper pharyngeal airway assessment using dental CBCT: A systematic review. Eur. J. Orthodont. 2017, 39, 489–496. [Google Scholar] [CrossRef]
- Lee, J.Y.; Kim, Y.I.; Hwang, D.S.; Park, S.B. Effect of Maxillary Setback Movement on Upper Airway in Patients with Class III Skeletal Deformities: Cone Beam Computed Tomographic Evaluation. J. Craniofac. Surg. 2013, 24, 387–391. [Google Scholar] [CrossRef]
- Chan, H.P.; Samala, R.K.; Hadjiiski, L.M.; Zhou, C. Deep Learning in Medical Image Analysis. Adv. Exp. Med. Biol. 2020, 1213, 3–21. [Google Scholar] [CrossRef]
- Shen, D.; Wu, G.; Suk, H.I. Deep Learning in Medical Image Analysis. Annu. Rev. Biomed. Eng. 2017, 19, 221–248. [Google Scholar] [CrossRef]
- Yun, J.; Park, J.; Yu, D.; Yi, J.; Lee, M.; Park, H.J.; Lee, J.G.; Seo, J.B.; Kim, N. Improvement of fully automated airway segmentation on volumetric computed tomographic images using a 2.5 dimensional convolutional neural net. Med. Image Anal. 2019, 51, 13–20. [Google Scholar] [CrossRef]
- Kuo, C.F.J.; Leu, Y.S.; Hu, D.J.; Huang, C.C.; Siao, J.J.; Leon, K.B.P. Application of intelligent automatic segmentation and 3D reconstruction of inferior turbinate and maxillary sinus from computed tomography and analyze the relationship between volume and nasal lesion. Biomed. Signal Process Control 2020, 57, 19. [Google Scholar] [CrossRef]
- Otsu, N. Threshold Selection Method from Gray-Level Histograms. IEEE Trans. Syst. Man Cybern. 1979, 9, 62–66. [Google Scholar] [CrossRef]
- El, H.; Palomo, J.M.; Halazonetis, D.J. Measuring the airway in 3 dimensions: A reliability and accuracy study. Am. J. Orthod. Dentofac. 2010, 137, S50.e1–S50.e9. [Google Scholar] [CrossRef]
- Sutthiprapaporn, P.; Tanimoto, K.; Ohtsuka, M.; Nagasaki, T.; Iida, Y.; Katsumata, A. Positional changes of oropharyngeal structures due to gravity in the upright and supine positions. Dentomaxillofac. Radiol. 2008, 37, 130–135. [Google Scholar] [CrossRef]
- Lee, J.H.; Yu, H.J.; Kim, M.J.; Kim, J.W.; Choi, J. Automated cephalometric landmark detection with confidence regions using Bayesian convolutional neural networks. BMC Oral Health 2020, 20, 270. [Google Scholar] [CrossRef]
- Guijarro-Martinez, R.; Swennen, G.R.J. Cone-beam computerized tomography imaging and analysis of the upper airway: A systematic review of the literature. Int. J. Oral Maxillofac. Surg. 2011, 40, 1227–1237. [Google Scholar] [CrossRef]
- Muto, T.; Takeda, S.; Kanazawa, M.; Yamazaki, A.; Fujiwara, Y.; Mizoguchi, I. The effect of head posture on the pharyngeal airway space (PAS). Int. J. Oral Maxillofac. Surg. 2002, 31, 579–583. [Google Scholar] [CrossRef]
- Weber, D.W.; Fallis, D.W.; Packer, M.D. Three-dimensional reproducibility of natural head position. Am. J. Orthod. Dentofac. Orthop. 2013, 143, 738–744. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Definition | Explanation |
|---|---|
| Reference Points | |
| PNS | Most posterior point of palate |
| VP | Most posterior point of vomer |
| CV1 | Most anterior inferior point of anterior arch of atlas |
| CV2 | Most anterior inferior point of anterior arch of second vertebra |
| CV4 | Most anterior inferior point of anterior arch of fourth vertebra |
| Reference planes | |
| PNS-Vp plane | The plane was perpendicular to the midsagittal plane passing through the PNS and the Vp. |
| CV1 plane | The plane was parallel to the natural head position plane passing through CV1. |
| CV2 plane | The plane was parallel to the natural head position plane passing through CV2. |
| CV3 plane | The plane was parallel to the natural head position plane passing through CV3. |
| CV4 plane | The plane was parallel to the natural head position plane passing through CV4. |
| Volume | |
| Nasopharynx | From PNS-VP plane to CV1 plane |
| Oropharynx | From CV1 plane to CV2 plane |
| Hypopharynx | From CV2 plane to CV4 plane |
| Average | SD | |
|---|---|---|
| Volume (mm3) | ||
| Nasopharynx | 48.620 | 49.468 |
| Oropharynx | 37.987 | 43.289 |
| Hypopharynx | 50.010 | 57.891 |
| Total volume | 85.256 | 86.504 |
| Distances between M and DL (mm) | ||
| PNS | 2.817 | 1.806 |
| VP | 2.837 | 1.924 |
| CV1 | 2.571 | 2.028 |
| CV2 | 2.896 | 2.205 |
| CV4 | 4.156 | 2.379 |
| Variables | ICC | 95% CI | |
|---|---|---|---|
| Lower Limit | Upper Limit | ||
| Volume | |||
| Nasopharynx | 0.912 | 0.858 | 0.946 |
| Oropharynx | 0.984 | 0.973 | 0.99 |
| Hypopharynx | 0.964 | 0.941 | 0.978 |
| Total volume | 0.986 | 0.977 | 0.992 |
| Coordinate | |||
| PNS(x) | 0.908 | 0.852 | 0.944 |
| PNS(y) | 0.952 | 0.921 | 0.971 |
| Vp(x) | 0.908 | 0.842 | 0.946 |
| Vp(y) | 0.939 | 0.89 | 0.965 |
| CV1(x) | 0.929 | 0.885 | 0.957 |
| CV1(y) | 0.956 | 0.928 | 0.974 |
| CV2(x) | 0.963 | 0.939 | 0.978 |
| CV2(y) | 0.924 | 0.877 | 0.954 |
| CV4(x) | 0.953 | 0.924 | 0.972 |
| CV4(y) | 0.868 | 0.79 | 0.919 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, J.; Hwang, J.; Ryu, J.; Nam, I.; Kim, S.-A.; Cho, B.-H.; Shin, S.-H.; Lee, J.-Y. Deep Learning Based Airway Segmentation Using Key Point Prediction. Appl. Sci. 2021, 11, 3501. https://doi.org/10.3390/app11083501
Park J, Hwang J, Ryu J, Nam I, Kim S-A, Cho B-H, Shin S-H, Lee J-Y. Deep Learning Based Airway Segmentation Using Key Point Prediction. Applied Sciences. 2021; 11(8):3501. https://doi.org/10.3390/app11083501
Chicago/Turabian StylePark, Jinyoung, JaeJoon Hwang, Jihye Ryu, Inhye Nam, Sol-A Kim, Bong-Hae Cho, Sang-Hun Shin, and Jae-Yeol Lee. 2021. "Deep Learning Based Airway Segmentation Using Key Point Prediction" Applied Sciences 11, no. 8: 3501. https://doi.org/10.3390/app11083501
APA StylePark, J., Hwang, J., Ryu, J., Nam, I., Kim, S.-A., Cho, B.-H., Shin, S.-H., & Lee, J.-Y. (2021). Deep Learning Based Airway Segmentation Using Key Point Prediction. Applied Sciences, 11(8), 3501. https://doi.org/10.3390/app11083501