
Augmented Reality, Mixed Reality, and Hybrid Approach in Healthcare Simulation: A Systematic Review


 ,
,  ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Simulation Approach
- Augmented reality (AR) simulator: an interactive simulator in which the real-world environment is enhanced by computer-generated content perceived by the user using different senses. In these simulators, the specifically designed physical component could be absent (using only pre-existing elements of the real-world environment, such as the ground, a wall etc.), passive (not actively participating in the simulation), or active (providing/enabling specific functionalities in the simulation).
- Hybrid simulator: an interactive simulator in which the system integrates both a virtual and a physical module. In these simulators the physical parts are always present, but they could play either a passive or active role in the simulation.
- Mixed reality (MR) simulator: an interactive simulator in which real content (physical objects) and virtual information (computer-generated content) are merged so that they can interact with each other in real time. In these simulators the physical parts can interact with the virtual content (and/or vice versa).
2.2. Literature Search
- (Augmented Reality OR AR) AND (Simulation OR Simulator) AND (Healthcare OR Medicine OR Surgery OR Surgical)
- (Mixed Reality OR MR) AND (Simulation OR Simulator) AND (Healthcare OR Medicine OR Surgery OR Surgical)
- (Hybrid) AND (Simulation OR Simulator) AND (Healthcare OR Medicine OR Surgery OR Surgical)
2.3. Study Selection
- Q1:
- Is the study relevant to healthcare simulation for improving the medical technical and/or non-technical skills?
- Q2:
- Are the simulation techniques based on AR, MR, and/or hybrid approach?
- Q3:
- Does the study concern the development of an ad-hoc simulator or the evaluation of a commercial simulator?
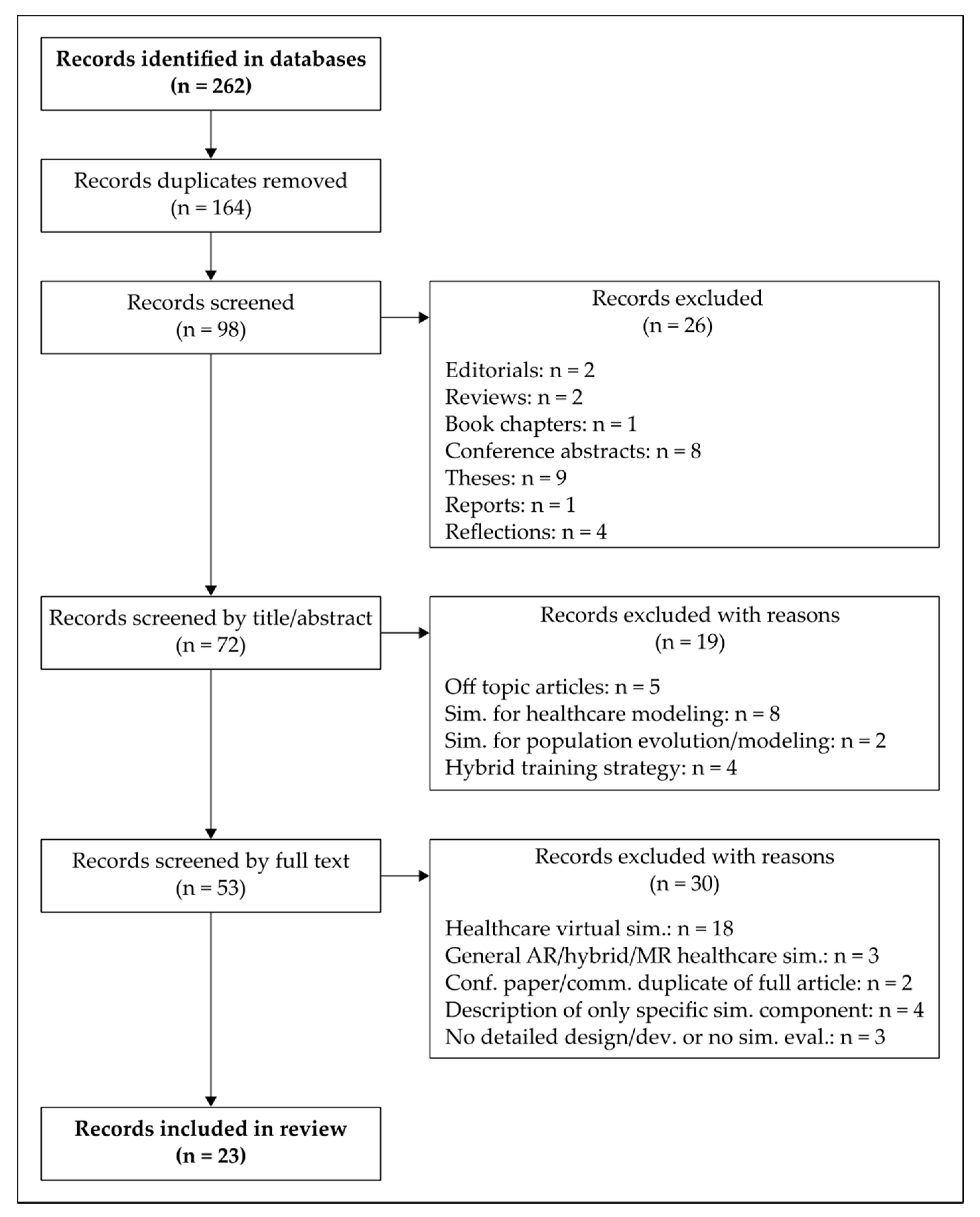
- Removal of duplicates from nine different databases. After removing them, 98 studies remained.
- Removal of editorials (1), reviews (2), book chapters (1), conference abstracts (8), thesis (9), reports (1), and reflections (4). After removing them, 72 studies remained for the next phase.
- Removal of studies after reading the title and abstract. The removed articles do not resolve question Q1. After removing them, 35 studies remained.
- Removal of studies after reading the full text, since some papers are still dubious after step 3. The removed articles do not resolve questions Q2 and Q3. A total of 23 studies remained relevant for our review.
2.4. Research Questions
3. Results
3.1. Target Clinical Area (GQ1, FQ1)
Surgical Approaches (FQ1)
3.2. Technical and Non-Technical Skills in Surgery (GQ2)
3.3. Haptic Feedback (GQ3, FQ2)
3.4. Implementation of the Virtual Component of the Simulators (FQ2–5)
3.4.1. Tracking Approach (FQ3)
- Vision-based approaches, that can be further categorized into two mutually non-exclusive methods: marker-based and marker-less (i.e., location-based position).
- A marker is a distinguishable artificial element that a computer system can detect using image segmentation, pattern recognition, and computer vision techniques. Marker-based methods are fast; however, inherent drawbacks of these approaches lie in the fact that marker detection is very sensitive to marker occlusion and poor ambient lighting (that can make the makers unrecognizable). As for the latter issue, infrared (IR) retro-reflective markers can be used to improve the reliability of tracking, reducing the effects of ambient illumination.
- 2.
- Other sensor-based approaches (apart from vision sensors) including electromagnetic tracking, acoustic tracking, and inertial tracking sensors.
- 3.
- Hybrid techniques that combine marker-based with marker-less approaches or vision-based and sensor-based techniques.
3.4.2. Visualization Modality (FQ4)
3.4.3. Artificial Intelligence Techniques Integrated in the Simulation (FQ5)
3.5. Implementation of the Physical Component of the Simulator (GQ4, FQ6–7)
3.5.1. Materials and Fabrication Techniques (FQ6–7)
3.5.2. Sensors Types (GQ4)
3.6. Patient-Specific Simulation (GQ5)
3.7. Reusability of Simulator Components (GQ6)
3.8. General Features of Simulation Systems (GQ7–9, FQ7–10)
3.8.1. Performance Evaluation Metrics (GQ7, FQ7–8)
3.8.2. Implementation of Different Levels of Complexity (GQ8)
3.8.3. Portability (GQ9)
3.9. Evaluation of Simulators (FQ9–10)
- Face validity refers to simulator realism, and it is assessed by experts by means of questionnaires or surveys;
- Content validity measures the appropriateness and usefulness of the simulator as a training tool, and it is typically assessed by experts with checklists;
- Construct validity determines the ability of simulator to differentiate between expert and novices;
- Concurrent validity indicates the correspondence between trainees’ performance tested on a simulator and on a gold standard method or against another, previously validated, simulator;
3.10. Trends of Simulation Techniques in Healthcare (SQ1–4)
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kerr, B.; O’Leary, J. The training of the surgeon: Dr. Halsted’s greatest legacy. Am. Surg. 1999, 65, 1101–1102. [Google Scholar] [PubMed]
- Scott, D.J.; Cendan, J.C.; Pugh, C.M.; Minter, R.M.; Dunnington, G.L.; Kozar, R.A. The changing face of surgical education: Simulation as the new paradigm. J. Surg. Res. 2008, 147, 189–193. [Google Scholar] [CrossRef]
- Tan, S.S.Y.; Sarker, S.K. Simulation in surgery: A review. Scott. Med. J. 2011, 56, 104–109. [Google Scholar] [CrossRef]
- Meier, A.H.; Rawn, C.L.; Krummel, T.M. Virtual reality: Surgical application--challenge for the new millennium. J. Am. Coll. Surg. 2001, 192, 372–384. [Google Scholar] [CrossRef]
- Hutter, M.M.; Kellogg, K.C.; Ferguson, C.M.; Abbott, W.M.; Warshaw, A.L. The impact of the 80-hour resident workweek on surgical residents and attending surgeons. Ann. Surg. 2006, 243, 864–875. [Google Scholar] [CrossRef] [PubMed]
- Sutherland, L.M.; Middleton, P.F.; Anthony, A.; Hamdorf, J.; Cregan, P.; Scott, D.; Maddern, G.J. Surgical simulation: A systematic review. Ann. Surg. 2006, 243, 291–300. [Google Scholar] [CrossRef]
- The Southern Surgeons Club; Moore, M.J.; Bennett, C.L. The learning curve for laparoscopic cholecystectomy. Am. J. Surg. 1995, 170, 55–59. [Google Scholar] [CrossRef]
- Scott, D.J. Patient Safety, Competency, and the Future of Surgical Simulation. Simul. Healthc. 2006, 1, 164–170. [Google Scholar] [CrossRef]
- Stefanidis, D.; Sevdalis, N.; Paige, J.; Zevin, B.; Aggarwal, R.; Grantcharov, T.; Jones, D.B. Simulation in surgery: What’s needed next? Ann. Surg. 2015, 261, 846–853. [Google Scholar] [CrossRef]
- Vozenilek, J.; Huff, J.S.; Reznek, M.; Gordon, J.A. See One, Do One, Teach One: Advanced Technology in Medical Education. Acad. Emerg. Med. 2004, 11, 1149–1154. [Google Scholar] [CrossRef]
- Bradley, P. The history of simulation in medical education and possible future directions. Med. Educ. 2006, 40, 254–262. [Google Scholar] [CrossRef] [PubMed]
- Gaba, D.M. The future vision of simulation in healthcare. Simul. Healthc. 2007, 2, 126–135. [Google Scholar] [CrossRef] [PubMed]
- Lateef, F. Simulation-based learning: Just like the real thing. J. Emerg. Trauma. Shock. 2010, 3, 348–352. [Google Scholar] [CrossRef]
- Ziv, A.; Wolpe, P.R.; Small, S.D.; Glick, S. Simulation-based medical education: An ethical imperative. Acad. Med. 2003, 78, 783–788. [Google Scholar] [CrossRef] [PubMed]
- Ziv, A.; Small, S.D.; Wolpe, P.R. Patient safety and simulation-based medical education. Med. Teach. 2000, 22, 489–495. [Google Scholar] [CrossRef] [PubMed]
- de Visser, H.; Watson, M.O.; Salvado, O.; Passenger, J.D. Progress in virtual reality simulators for surgical training and certification. Med. J. Aust. 2011, 194, S38–S40. [Google Scholar] [CrossRef] [PubMed]
- Gurusamy, K.; Aggarwal, R.; Palanivelu, L.; Davidson, B. Systematic review of randomized controlled trials on the effectiveness of virtual reality training for laparoscopic surgery. Br. J. Surg. 2008, 95, 1088–1097. [Google Scholar] [CrossRef]
- Loukas, C. Surgical Simulation Training Systems: Box Trainers, Virtual Reality and Augmented Reality Simulators. Int. J. Robot. Autom. 2016, 1, 1–9. [Google Scholar] [CrossRef]
- Badash, I.; Burtt, K.; Solorzano, C.A.; Carey, J.N. Innovations in surgery simulation: A review of past, current and future techniques. Ann. Transl. Med. 2016, 4, 453. [Google Scholar] [CrossRef]
- Dunkin, B.; Adrales, G.L.; Apelgren, K.; Mellinger, J.D. Surgical simulation: A current review. Surg. Endosc. 2007, 21, 357–366. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The, P.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Coelho, G.; Rabelo, N.N.; Vieira, E.; Mendes, K.; Zagatto, G.; Santos de Oliveira, R.; Raposo-Amaral, C.E.; Yoshida, M.; de Souza, M.R.; Fagundes, C.F.; et al. Augmented reality and physical hybrid model simulation for preoperative planning of metopic craniosynostosis surgery. Neurosurg. Focus 2020, 48, E19. [Google Scholar] [CrossRef]
- Condino, S.; Turini, G.; Parchi, P.D.; Viglialoro, R.M.; Piolanti, N.; Gesi, M.; Ferrari, M.; Ferrari, V. How to Build a Patient-Specific Hybrid Simulator for Orthopaedic Open Surgery: Benefits and Limits of Mixed-Reality Using the Microsoft HoloLens. J. Healthc. Eng. 2018, 2018, 5435097. [Google Scholar] [CrossRef] [PubMed]
- Condino, S.; Carbone, M.; Ferrari, V.; Faggioni, L.; Peri, A.; Ferrari, M.; Mosca, F. How to build patient-specific synthetic abdominal anatomies. An innovative approach from physical toward hybrid surgical simulators. Int. J. Med. Robot. Comput. Assist. Surg. 2011, 7, 202–213. [Google Scholar] [CrossRef]
- Feifer, A.; Al-Ammari, A.; Kovac, E.; Delisle, J.; Carrier, S.; Anidjar, M. Randomized controlled trial of virtual reality and hybrid simulation for robotic surgical training. BJU Int. 2011, 108, 1652–1656, discussion 1657. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, V.; Viglialoro, R.M.; Nicoli, P.; Cutolo, F.; Condino, S.; Carbone, M.; Siesto, M.; Ferrari, M. Augmented reality visualization of deformable tubular structures for surgical simulation. Int. J. Med. Robot. 2016, 12, 231–240. [Google Scholar] [CrossRef]
- Fuerst, D.; Hollensteiner, M.; Schrempf, A. A novel augmented reality simulator for minimally invasive spine surgery. In Proceedings of the 2014 Summer Simulation Multiconference, Monterey, CA, USA, 6–10 July 2014; p. 28. [Google Scholar]
- Fushima, K.; Kobayashi, M. Mixed-reality simulation for orthognathic surgery. Maxillofac. Plast Reconstr. Surg. 2016, 38, 13. [Google Scholar] [CrossRef] [PubMed]
- Halic, T.; Kockara, S.; Bayrak, C.; Rowe, R. Mixed reality simulation of rasping procedure in artificial cervical disc replacement (ACDR) surgery. BMC Bioinform. 2010, 11 (Suppl. 6), S11. [Google Scholar] [CrossRef]
- Huang, C.Y.; Thomas, J.B.; Alismail, A.; Cohen, A.; Almutairi, W.; Daher, N.S.; Terry, M.H.; Tan, L.D. The use of augmented reality glasses in central line simulation: “see one, simulate many, do one competently, and teach everyone”. Adv. Med. Educ. Pract. 2018, 9, 357–363. [Google Scholar] [CrossRef]
- Jain, S.; Lee, S.; Barber, S.R.; Chang, E.H.; Son, Y.-J. Virtual reality based hybrid simulation for functional endoscopic sinus surgery. IISE Trans. Healthc. Syst. Eng. 2020, 10, 127–141. [Google Scholar] [CrossRef]
- Keebler, J.R.; Lazzara, E.H.; Patzer, B. Building a Simulated Medical Augmented Reality Training System. Proc. Hum. Factors Ergon. Soc. Annu. Meet. 2014, 58, 1169–1173. [Google Scholar] [CrossRef]
- Lahanas, V.; Loukas, C.; Smailis, N.; Georgiou, E. A novel augmented reality simulator for skills assessment in minimal invasive surgery. Surg. Endosc. 2015, 29, 2224–2234. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Lee, J.; Lee, A.; Park, N.; Lee, S.; Song, S.; Seo, A.; Lee, H.; Kim, J.I.; Eom, K. Augmented reality intravenous injection simulator based 3D medical imaging for veterinary medicine. Vet. J. 2013, 196, 197–202. [Google Scholar] [CrossRef]
- Lin, Y.-K.; Tsai, K.-L.; Yau, H.-T. The Development of Optical See-through Display Based on Augmented Reality for Oral Implant Surgery Simulation. Comput. Aided Des. Appl. 2012, 9, 111–120. [Google Scholar] [CrossRef]
- Loukas, C.; Lahanas, V.; Georgiou, E. An integrated approach to endoscopic instrument tracking for augmented reality applications in surgical simulation training. Int. J. Med. Robot. 2013, 9, e34–e51. [Google Scholar] [CrossRef]
- Nomura, T.; Mamada, Y.; Nakamura, Y.; Matsutani, T.; Hagiwara, N.; Fujita, I.; Mizuguchi, Y.; Fujikura, T.; Miyashita, M.; Uchida, E. Laparoscopic skill improvement after virtual reality simulator training in medical students as assessed by augmented reality simulator. Asian J. Endosc. Surg. 2015, 8, 408–412. [Google Scholar] [CrossRef]
- Onishi, K.; Mizushino, K.; Ikemoto, H.; Noborio, H. AR Dental Surgical Simulator Using Haptic Feedback. In Proceedings of the International Conference on Human-Computer Interaction HCI 2013, Las Vegas, NV, USA, 21–26 July 2013; Springer: Berlin/Heidelberg, Germany, 2013; pp. 202–205. [Google Scholar]
- Parkes, R.; Forrest, N.; Baillie, S. A mixed reality simulator for feline abdominal palpation training in veterinary medicine. Stud. Health Technol. Inform. 2009, 142, 244–246. [Google Scholar] [PubMed]
- Yonghang, T.; Wei, L.; Zhou, H.; Peng, J.; Li, Q.; Li, F.; Zhang, J.; Shi, J. Augmented-reality-driven medical simulation platform for percutaneous nephrolithotomy with cybersecurity awareness. Int. J. Distrib. Sens. Netw. 2019, 15. [Google Scholar] [CrossRef]
- Thomas, G.W.; Johns, B.D.; Kho, J.Y.; Anderson, D.D. The Validity and Reliability of a Hybrid Reality Simulator for Wire Navigation in Orthopedic Surgery. IEEE Trans. Hum. Mach. Syst. 2015, 45, 119–125. [Google Scholar] [CrossRef]
- Tsujita, T.; Sase, K.; Chen, X.; Tomita, M.; Konno, A.; Nakayama, M.; Nakagawa, A.; Abe, K.; Uchiyama, M. Development of a Surgical Simulator for Training Retraction of Tissue with an Encountered-Type Haptic Interface Using MR Fluid. In Proceedings of the 2018 IEEE International Conference on Robotics and Biomimetics (ROBIO 2018), Kuala Lumpur, Malaysia, 12–15 December 2018; pp. 898–903. [Google Scholar]
- van Duren, B.H.; Sugand, K.; Wescott, R.; Carrington, R.; Hart, A. Augmented reality fluoroscopy simulation of the guide-wire insertion in DHS surgery: A proof of concept study. Med. Eng. Phys. 2018, 55, 52–59. [Google Scholar] [CrossRef]
- Viglialoro, R.M.; Esposito, N.; Condino, S.; Cutolo, F.; Guadagni, S.; Gesi, M.; Ferrari, M.; Ferrari, V. Augmented Reality to Improve Surgical Simulation: Lessons Learned Towards the Design of a Hybrid Laparoscopic Simulator for Cholecystectomy. IEEE Trans. Biomed. Eng. 2019, 66, 2091–2104. [Google Scholar] [CrossRef]
- Lynch, A. Simulation-based acquisition of non-technical skills to improve patient safety. Semin. Pediatric Surg. 2020, 29, 150906. [Google Scholar] [CrossRef]
- Agha, R.A.; Fowler, A.J.; Sevdalis, N. The role of non-technical skills in surgery. Ann. Med. Surg. 2015, 4, 422–427. [Google Scholar] [CrossRef]
- Escobar-Castillejos, D.; Noguez, J.; Neri, L.; Magana, A.; Benes, B. A Review of Simulators with Haptic Devices for Medical Training. J. Med. Syst. 2016, 40, 104. [Google Scholar] [CrossRef] [PubMed]
- Turini, G.; Condino, S.; Parchi, P.D.; Viglialoro, R.M.; Piolanti, N.; Gesi, M.; Ferrari, M.; Ferrari, V. A Microsoft HoloLens Mixed Reality Surgical Simulator for Patient-Specific Hip Arthroplasty Training. In Proceedings of the International Conference on Augmented Reality, Virtual Reality and Computer Graphics (AVR 2018), Otranto, Italy, 24–27 June 2018; Springer: Cham, Switzerland, 2018; pp. 201–210. [Google Scholar]
- Ryu, W.H.A.; Dharampal, N.; Mostafa, A.E.; Sharlin, E.; Kopp, G.; Jacobs, W.B.; Hurlbert, R.J.; Chan, S.; Sutherland, G.R. Systematic Review of Patient-Specific Surgical Simulation: Toward Advancing Medical Education. J. Surg. Educ. 2017, 74, 1028–1038. [Google Scholar] [CrossRef]
- Issenberg, B.; McGaghie, W.; Petrusa, E.; Gordon, D.; Scalese, R. Features and uses of high-fidelity medical simulations that lead to effective learning: A BEME systematic review. Med. Teach. 2005, 27, 10–28. [Google Scholar] [CrossRef] [PubMed]
- Cox, M.; Irby, D.; Epstein, R. Assessment in Medical Education. N. Engl. J. Med. 2007, 22, 13–16. [Google Scholar]
- Ryall, T.; Judd, B.K.; Gordon, C.J. Simulation-based assessments in health professional education: A systematic review. J. Multidiscip. Healthc. 2016, 9, 69–82. [Google Scholar] [PubMed]
- Bewley, W.; Oneil, H. Evaluation of Medical Simulations. Mil. Med. 2013, 178, 64–75. [Google Scholar] [CrossRef]
- Moglia, A.; Ferrari, V.; Morelli, L.; Ferrari, M.; Mosca, F.; Cuschieri, A. A Systematic Review of Virtual Reality Simulators for Robot-assisted Surgery. Eur. Urol. 2016, 69, 1065–1080. [Google Scholar] [CrossRef]
- Botden, S.M.; Jakimowicz, J.J. What is going on in augmented reality simulation in laparoscopic surgery? Surg. Endosc. 2009, 23, 1693–1700. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Type/Code | Research Questions | |
|---|---|---|
| General Questions | GQ1 | Which is the target clinical area? |
| GQ2 | Which skills are addressed by simulator? (technical skills, non-technical skills) | |
| GQ3 | Does the simulator integrate haptic feedback? | |
| GQ4 | What kind of sensors are used? | |
| GQ5 | Is the simulator patient-specific? (patient-specific, not-patient-specific) | |
| GQ6 | Are the simulator components reusable? | |
| GQ7 | Is a clinical performance evaluation performed? | |
| GQ8 | Does the simulator allow the selection of different scenarios based on trainee’s needs? | |
| GQ9 | How portable is the simulator? (very portable, portable, not portable) | |
| Focus Questions | FQ1 | How invasive is the simulated surgical approach? (non-inv., minimally-inv., inv.) |
| FQ2 | Which mode is used to convey haptic feedback? | |
| FQ3 | Which tracking approach is used to implement AR? (marker-based or marker-less) | |
| FQ4 | What visualization type is used? (monitor, hand-held display, HMD, projection) | |
| FQ5 | What kind of artificial intelligence technique is implemented? | |
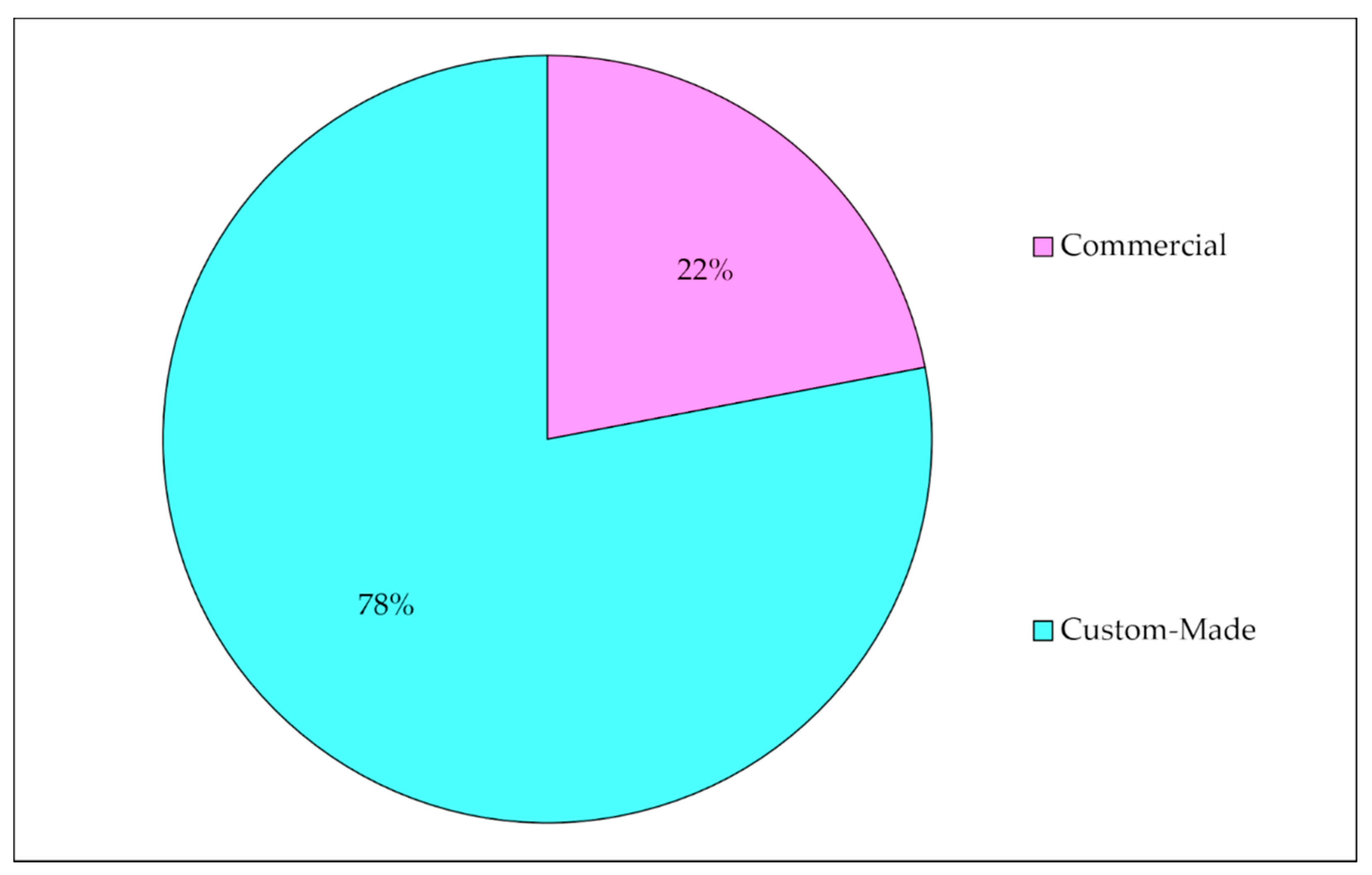
| FQ6 | Which types of phantom are used? (commercial, custom-made) | |
| FQ7 | Which simulator manufacturing technique is used? | |
| FQ8 | Which metric is used for performance evaluation? | |
| FQ9 | Which evaluation method is performed to validate the simulator? | |
| FQ10 | Is a statistical analysis performed? | |
| Statistical Questions | SQ1 | How many commercial simulators are used? |
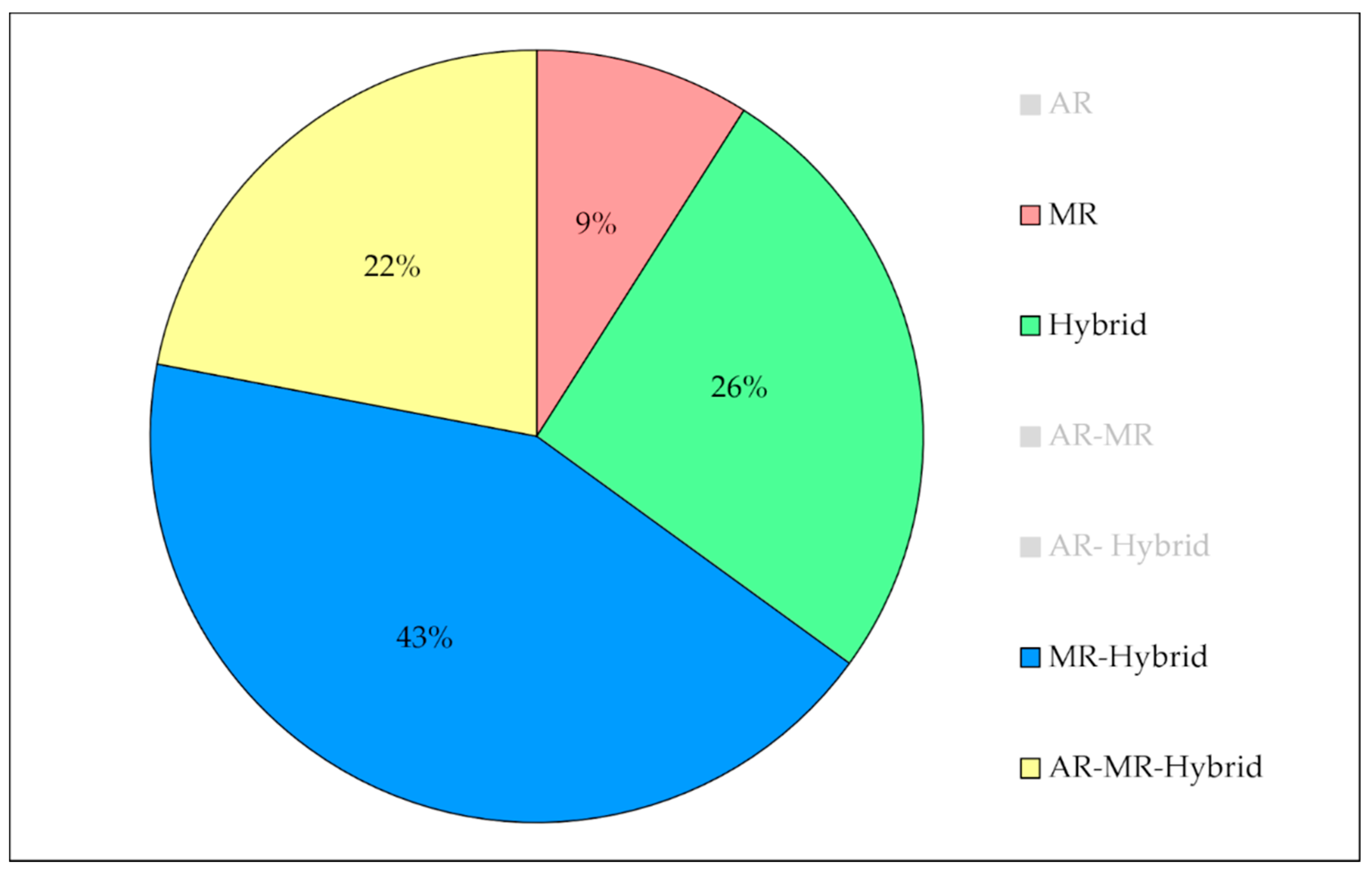
| SQ2 | How many AR simulators are there? | |
| SQ3 | How many MR simulators are there? | |
| SQ4 | How many hybrid simulators are there? | |
| Reference | Title of Selected Study |
|---|---|
| Coelho 2020 [22] | Augmented reality and physical hybrid model simulation for preoperative planning of metopic craniosynostosis surgery. |
| Condino 2018 [23] | How to build a patient-specific hybrid simulator for orthopedic open surgery: benefits and limits of mixed-reality using the Microsoft HoloLens. |
| Condino 2011 [24] | How to build patient-specific synthetic abdominal anatomies. An innovative approach from physical toward hybrid surgical simulators. |
| Feifer 2011 [25] | Randomized controlled trial of virtual reality and hybrid simulation for robotic surgical training. |
| Ferrari 2016 [26] | Augmented reality visualization of deformable tubular structures for surgical simulation. |
| Fuerst 2014 [27] | A novel augmented reality simulator for minimally invasive spine surgery. |
| Fushima 2016 [28] | Mixed-reality simulation for orthognathic surgery. |
| Halic 2010 [29] | Mixed reality simulation of rasping procedure in artificial cervical disc replacement (ACDR) surgery. |
| Huang 2018 [30] | The use of augmented reality glasses in central line simulation: “see one, simulate many, do one competently, and teach everyone” |
| Jain 2019 [31] | Virtual reality based hybrid simulation for functional endoscopic sinus surgery. |
| Keebler 2014 [32] | Building a simulated medical augmented reality training system. |
| Lahanas 2015 [33] | A novel augmented reality simulator for skills assessment in minimal invasive surgery. |
| Lee 2013 [34] | Augmented reality intravenous injection simulator based 3D medical imaging for veterinary medicine. |
| Lin 2012 [35] | The development of optical see-through display based on augmented reality for oral implant surgery simulation. |
| Loukas 2013 [36] | An integrated approach to endoscopic instrument tracking for augmented reality applications in surgical simulation training. |
| Nomura 2015 [37] | Laparoscopic skill improvement after virtual reality simulator training in medical students as assessed by augmented reality simulator. |
| Onishi 2013 [38] | AR dental surgical simulator using haptic feedback. |
| Parkes 2009 [39] | A mixed reality simulator for feline abdominal palpation training in veterinary medicine. |
| Tai 2009 [40] | Augmented-reality-driven medical simulation platform for percutaneous nephrolithotomy with cybersecurity awareness. |
| Thomas 2014 [41] | The validity and reliability of a hybrid reality simulator for wire navigation in orthopedic surgery. |
| Tsujita 2018 [42] | Development of a surgical simulator for training retraction of tissue with an encountered-type haptic interface using MR fluid. |
| Van Duren 2018 [43] | Augmented reality fluoroscopy simulation of the guide-wire. insertion in DHS surgery: a proof of concept study. |
| Viglialoro 2018 [44] | Augmented reality to improve surgical simulation. Lessons learned towards the design of a hybrid laparoscopic simulator for cholecystectomy. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Viglialoro, R.M.; Condino, S.; Turini, G.; Carbone, M.; Ferrari, V.; Gesi, M. Augmented Reality, Mixed Reality, and Hybrid Approach in Healthcare Simulation: A Systematic Review. Appl. Sci. 2021, 11, 2338. https://doi.org/10.3390/app11052338
Viglialoro RM, Condino S, Turini G, Carbone M, Ferrari V, Gesi M. Augmented Reality, Mixed Reality, and Hybrid Approach in Healthcare Simulation: A Systematic Review. Applied Sciences. 2021; 11(5):2338. https://doi.org/10.3390/app11052338
Chicago/Turabian StyleViglialoro, Rosanna Maria, Sara Condino, Giuseppe Turini, Marina Carbone, Vincenzo Ferrari, and Marco Gesi. 2021. "Augmented Reality, Mixed Reality, and Hybrid Approach in Healthcare Simulation: A Systematic Review" Applied Sciences 11, no. 5: 2338. https://doi.org/10.3390/app11052338
APA StyleViglialoro, R. M., Condino, S., Turini, G., Carbone, M., Ferrari, V., & Gesi, M. (2021). Augmented Reality, Mixed Reality, and Hybrid Approach in Healthcare Simulation: A Systematic Review. Applied Sciences, 11(5), 2338. https://doi.org/10.3390/app11052338