Abstract
Since the low level of available evidence and the limited number of studies do not clarify whether clear aligners are a good option for extrusion, finite element (FE) analyses were performed to obtain more accurate biomechanical data about open-bite treatment in the upper arch. The aim of this study is to answer three questions: Are aligners efficient in performing upper incisor extrusion? Does the number, position, and shape of attachments influence the force system? Is posterior anchorage preserved during incisor extrusion? Six different simulations were performed with different attachment patterns. The results of this study were consistent with the biomechanical information obtained from clinical trials, and highlighted the need of better knowing undesired forces during teeth movement with clear aligners. Some attachment configuration seems to lead to a better force system. The presence of rectangular horizontal attachments on the buccal or palatal surface of upper incisors in combination with rectangular vertical attachments on posterior teeth was found to produce the most efficient force system with minimal aligner deformation.
1. Introduction
Since the beginning of the aligner orthodontics era, the possibility of vertical movement control with these appliances has been a strongly debated topic. From the 2014 review by Rossini et al., the accuracy for vertical movements performed with clear aligners was reported to range between 30% and 41% of the planned movement [1]. Unfortunately, cited data come from studies older than five years ago, thus not considering the technological improvements obtained in the last few years. In the past few months, four clinical studies analyzing outcomes of vertical movements with aligners [2,3,4,5] were published. Focusing on open-bite treatment, three cephalometric studies from Garnett et al. [4], Moshiri et al. [3], and Harris et al. [5] reported the results of correction with clear aligners.
The study of Moshiri et al. retrospectively analyzed 30 adult patients, measuring pre- and post-treatment cephalograms. The authors reported significant changes for several cephalometric values, stating that bite closure was mainly achieved by a combination of counterclockwise rotation of the mandibular plane, lower molar intrusion, and lower incisor extrusion [3].
Garnett et al. [4] compared the cephalometric outcomes of 36 adult patients treated with aligners, with 17 adult patients treated with fixed appliance. The authors did not register significant differences between the two groups, except for a slightly greater amount of lower incisor extrusion in the aligners group. In conclusion, it was stated that “significant retroclination of upper and lower incisors, good vertical control, and no significant extrusion of the posterior teeth appear to be the main mechanisms for open bite correction” [4].
The retrospective study of Harris et al. [5] demonstrated the effectiveness of clear aligners in treating open-bite cases by anterior extrusion and posterior intrusion. However, the Authors reported a “significant retraction of maxillary and mandibular incisors” during anterior extrusion [5].
From these three studies, a lack of significant bodily extrusion of the upper incisors could be inferred. Open-bite treatment seems to be performed as a combination of posterior vertical control, incisor retroclination, and mandibular rotation.
Considering the low level of available evidence due to the limited number of retrospective studies, Finite Element (FE) analyses were performed to obtain biomechanical information about clear aligner open-bite treatment effects in the maxillary arch.
FE analyses were performed to answer the following clinical/research questions:
- Are aligners efficient in performing upper incisors extrusion?
- Does the number, position, and shape of attachments influence the force system?
- Is posterior anchorage preserved during incisor extrusion?
2. Materials and Methods
For this study, a CAD template of a maxillary arch, designed based on ideal proportion of teeth, was used to create six models with different attachment setups. Periodontal ligaments (PDL) for each tooth were modeled on the root shape with a thickness of 0.25 mm, as reported in the scientific literature. The aligners were made as an external offset of 0.5 mm from the surface of teeth (and eventually attachments), which is the thickness of a standard aligner, as stated as a result of repeated measurements with a Micro-CT Scan (SkyScan 1172: Bruker-microCT; Kontich, Belgium) of Invisalign aligners (Align Technology, Inc., San Jose, CA, USA) [6]. Septa between teeth were manually removed, and the aligners were refined to smooth and remove edges and undercuts. All the models were created using CAD software (SpaceClaim Corporation; Canonsburg, PA, USA) and then imported into FE software (ANSYS 18.2, Inc.; Canonsburg, PA, USA).
In the FE software, teeth, attachments, and aligners were considered as isotropic and homogeneous materials (Table 1). Teeth and attachments were considered as one rigid body, while the difference in rigidity between enamel and dentin was not considered. With the aim of simulating the behavior of the PDL in the best possible way, it was set as a hyperelastic material. According to Barone et al., the interfaces between the PDL and teeth were set as bonded contacts, while the ones between aligners and teeth were set as frictionless contacts. All the external surfaces of the PDL were linked to fixed supports to simulate the effect of the alveolar bone [7].

Table 1.
Materials’ proprieties.
After a convergence study performed on a single tooth model, mesh sizes were set at 0.09 mm for all bodies.
Element type was set as linear for all geometries, with the quadrilateral dominant method being applied to the surface elements of teeth and aligners, while the hex dominant method was adopted for PDL elements.
The planned extrusion was of 0.1 mm for both central and lateral incisors, and simultaneously performed. The extrusion was planned for each incisor along its own long axis.
Six simulations were performed:
- Without attachments (NOATT);
- With horizontal rectangular attachments only on incisors (ATT1-2);
- With rectangular attachments from second molar to canine (ATT3-7);
- ATT3-7 + optimized extrusion attachments on incisors (OTT);
- ATT3-7 + rectangular buccal horizontal attachments on incisors (RETT);
- ATT3-7 + rectangular palatal horizontal attachments on incisors (PALAT).
Optimized attachments’ shapes were derived from the one designed by Align Technology for the Invisalign system. The rectangular attachment shape was 3 × 2 × 1 mm, like the ones used in the ClinCheck software (Align Technology, Inc., San Jose, CA, USA).
The adoption of palatal attachments was derived from a similar FE study by Savignano et al. [7]
The following outcomes were analyzed:
- Teeth displacement pattern;
- Aligner deformation;
- Equivalent stress of PDL;
- Contact pressure between aligner and tooth surface.
3. Results
The tooth displacement pattern resulted to be the same in all six configurations. Planning for a simultaneous extrusion of upper anterior teeth resulted in retroclination of the central incisors, with the lateral incisors being subjected to buccal flaring, with a tendency for buccal tipping for the premolars and molars (Figure 1).
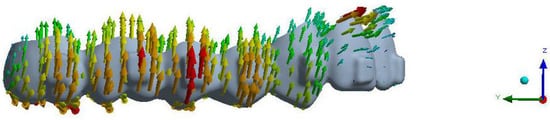
Figure 1.
Maximum deformation of the aligner in the analyses on the RETT model.
Consequently, aligner deformation was similar for all simulations. A strong tendency for buccal tipping and intrusion was observed at the molar, premolar, and canine levels, while for the incisors, a deformation of the aligners’ gingival margins away from the tooth surfaces was observed.
PDL stress accounted for, on average, 76.5 g/cm2, involving the mesio-buccal gingival parts of the central incisors’ roots and distal-buccal gingival parts of the lateral incisors’ roots (Figure 2).
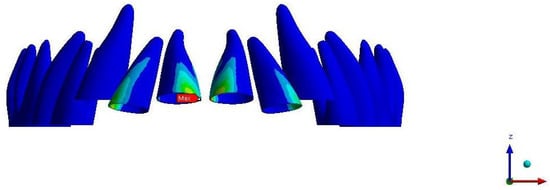
Figure 2.
Amount of stress on the PDL based on the analyses on the RETT model.
Regarding aligner pressure (Table 2), differences depending on the attachments’ settings were reported. In all simulations, pressure areas were located on buccal and palatal gingival margins of incisors. For NOATT, ATT3-7, ATT1-2, and OTT, maximum pressure areas were located on the lateral incisors’ buccal gingival surfaces, while in RETT and PALAT, they were located on the occlusal surface of rectangular attachments (Table 3 and Table 4).
Table 2.
Aligner maximum pressure locations.
Table 3.
Maximum tooth deformation and locations.
Table 4.
Minimum tooth deformation and locations.
4. Discussion
The obtained results evidenced the high unpredictability of aligner orthodontics in performing anterior teeth extrusion. The discrepancy between digital treatment planning and the clinical results may reside principally in the way the digital setup is performed [8]—the general thought that moving crowns in the setup will result in coherent mechanics in the achieving of the desired tooth position is increasingly going to be rejected, while deepening our biomechanical knowledge of this treatment modality.
The FE simulations of incisor extrusion are emblematic of this concept—planning a pure bodily extrusion of the four incisors, without any other movement that could generate undesired forces and displacements, will result in retroclination of anterior teeth, as well as buccal inclination and intrusion of the posterior ones, independently of the adopted attachments configuration.
Furthermore, for the first time in aligner orthodontics, published clinical trials [3,4,5] have reported outcomes which are consistent with the biomechanical information obtained from the present FE analyses. This matching in knowledge did not occur for distalization, for which only one protocol was tested [9]. The results demonstrated some biomechanical flaws that need to be improved.
Regarding open-bite treatment, with focus on upper incisor extrusion, it could be stated that the FE analyses were useful to obtain a biomechanical pattern, and that the obtained data are confirmed by the three retrospective studies by Garnett et al., Moshiri et al., and Harris et al. [3,4,5].
Furthermore, our simulations showed that the teeth presenting the worst inefficiencies were lateral incisors. Clinically, the lack of control on lateral incisors is an old issue for aligner orthodontics. No scientific paper has been published about this topic; however, it is common knowledge that the lateral incisors are the most difficult teeth to control with aligners, especially when extrusion movements are planned. For this reason, extra aligners are very often needed (Figure 3).
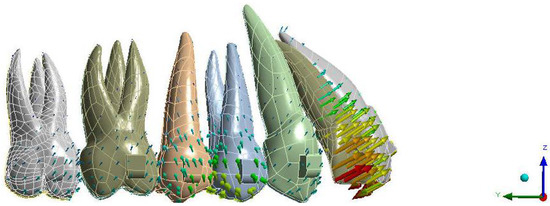
Figure 3.
Amount of deformation based on the analyses of the OTT model.
The lack of control on the lateral incisors, as well as the discrepancy between planned movement and the clinical result, in our opinion, could be interpreted correctly by analyzing aligner deformation. In open-bite FE simulations, the area of the lateral incisors experienced the greatest deformation, particularly at the gingival margin. Therefore, it may make sense to consider that the lack of adherence between aligner and tooth surface could lead to undesired forces and displacement.
Regarding aligner pressure, the analyzed configurations showed better results when posterior and anterior attachments were used in combination. Particularly when rectangular and vertical attachments are planned on canines, bicuspids, and molars, and rectangular horizontal attachments are planned on the buccal or the palatal surface of the upper incisors, the resulting force system is more efficient, with minimal aligner deformation. This attachments’ configuration allows for better anchorage control and more efficient control of the lateral incisors. The observed strong tendency for posterior teeth buccal tipping and intrusion should be considered as favorable from a clinical perspective—upper arch expansion and posterior intrusion represents treatment plan aspects that should be considered in adults’ open-bite treatments [10]. When using fixed appliances to treat non-growing open-bite patients, it generally results in extrusion of the molars, leading to an increase of the mandibular plane angle [10,11,12,13]. Therefore, a greater amount of incisor extrusion should be planned, reducing the efficiency of the treatment modality [11,14]. This study demonstrated that clear aligners may produce posterior intrusion and therefore, counterclockwise rotation of the mandible, facilitating anterior open-bite correction. A similar result was obtained in the retrospective study by Harris et al. [5]. From a clinical perspective, we should remember that a small amount of posterior intrusion can be obtained with aligners, even if not planned [15]. The well-known “bite block” effect of the aligners has been previously described and attributed to the thickness of aligners covering the occlusal surfaces and to the bite force exerted by patients [5,16]. This effect has been quantified in previous studies, ranging from 0.47 mm [5] to 0.6 mm [6,16].
In conclusion, biomechanical results match the observed clinical outcomes for open-bite treatment with orthodontic aligners. The efficiency and accuracy of treatment should be improved on the basis of biomechanical designed solutions, to improve control and understanding of the technique in the daily clinical setting.
Study Limitations
FEM studies represent one of the best ways to analyze force systems delivered by orthodontic appliances. However, in vitro and in vivo study results may differ. When analyzing aligner deformations, we should always keep in mind that polymer material, friction phenomena, thermoplastic material properties, thermoforming procedures, and insertion and removal of the appliance are all factors acting on aligner mechanical properties. Unfortunately, most of those factors are patented and not disclosed by companies, and therefore cannot be used to increase the complexity of FEM analyses. Another limitation of FEM studies in orthodontics is the approximation in modelling the material properties of biologic components, in particular PDL. Despite the increase in scientific evidence in this field, modelling of PDL properties remains an issue to consider when interpreting FEM studies’ results. Therefore, future FEM analyses should also consider those effects in analyzing orthodontic tooth movement biomechanics.
It is now possible to answer the clinical/research questions:
- Are aligners efficient in performing upper incisor extrusion?
As stated previously, the contemporary upper incisor extrusion biomechanics in aligner orthodontics is largely unpredictable. Extrusion of the four upper incisors results in central incisor retroclination, with lateral incisor flaring. Therefore, clear aligners seem to be not so efficient in controlling pure extrusion movements of the upper incisors.
- Does the number, position, and shape of attachments influence the force system?
RETT and PALAT configurations show better results in terms of force system, with minimal deformation in aligner’s gingival portion. This could lead to better control of lateral incisor movement. From a clinical perspective, clear aligners could be indicated in the treatment of open-bite patients with protruded upper incisors.
- Is posterior anchorage preserved during incisor extrusion?
There is a tendency of buccal tipping of the posterior teeth during extrusion. However, there is no evidence that this can cause a lack of posterior anchorage. Furthermore, the most efficient configurations showed the need for the use of attachments on posterior teeth in order to obtain better anchorage performances.
5. Conclusions
It is clear that more data have to be acquired to get better knowledge of the aligner’s biomechanics and to avoid undesired effects. Rectangular attachments seem to represent better configuration in order to control lateral incisors in both the PALAT and RETT configurations.
Upgrading the knowledge of undesired forces can lead to a better treatment plan, with less extra aligners needed.
Author Contributions
Conceptualization, G.R. and T.C.; methodology, G.R.; software, S.M.; validation, S.P. and A.D.; formal analysis, G.R.; data curation, S.M.; writing—original draft preparation, G.R.; writing—review and editing, T.C.; supervision, A.D.; project administration, T.C.; University funding acquisition, G.R. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were waived for this study, due to its in vitro design.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are partially available on request from the corresponding author. The data are not publicly available due to the fact that they could compromise the originality of in progress researches.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Rossini, G.; Parrini, S.; Castroflorio, T.; Deregibus, A.; Debernardi, C.L. Efficacy of clear aligners in controlling orthodontic tooth movement: A systematic review. Angle Orthod. 2015, 85, 881–889. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Hu, W. Force changes associated with different intrusion strategies for deep-bite correction by clear aligners. Angle Orthod. 2018, 88, 771–778. [Google Scholar] [CrossRef] [PubMed]
- Moshiri, S.; Araújo, E.A.; Mccray, J.F.; Thiesen, G.; Kim, K.B. Cephalometric evaluation of adult anterior open bite non-extraction treatment with Invisalign. Dental Press J. Orthod. 2017, 22, 30–38. [Google Scholar] [CrossRef] [PubMed]
- Garnett, B.S.; Mahood, K.; Nguyen, M.; Al-Khateeb, A.; Liu, S.; Boyd, R.; Oh, H. Cephalometric comparison of adult anterior open bite treatment using clear aligners and fixed appliances. Angle Orthod. 2019, 89, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Harris, K.; Ojima, K.; Dan, C.; Upadhyay, M.; Alshehri, A.; Kuo, C.L.; Mu, J.; Uribe, F.; Nanda, R. Evaluation of open bite closure using clear aligners: A retrospective study. Prog. Orthod. 2020, 21, 23. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, E.; Parrini, S.; Coda, E.; Cugliari, G.; Scotti, N.; Pasqualini, D.; Deregibus, A.; Castroflorio, T. Micro-CT evaluation of Invisalign aligners thickness homogeneity. Angle Orthod. in press.
- Barone, S.; Paoli, A.; Razionale, A.V.; Savignano, R. Computational design and engineering of polymeric orthodontic aligners. Int. J. Numer. Methods Biomed. Eng. 2017, 33, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Grünheid, T.; Loh, C.; Larson, B.E. How accurate is Invisalign in non extraction cases? Are predicted tooth positions achieved? Angle Orthod. 2017, 87, 809–815. [Google Scholar] [CrossRef] [PubMed]
- Rossini, G.; Schiaffino, M.; Parrini, S.; Sedran, A.; Deregibus, A.; Castroflorio, T. Upper Second Molar Distalization with Clear Aligners: A Finite Element Study. Appl. Sci. 2020, 10, 7739. [Google Scholar] [CrossRef]
- Deguchi, T.; Kurosaka, H.; Oikawa, H.; Kuroda, S.; Takahashi, I.; Yamashiro, T.; Takano-Yamamoto, T. Comparison of orthodontic treatment outcomes in adults with skeletal open bite between conventional edgewise treatment and implant-anchored orthodontics. Am. J. Orthod. Dentofac. Orthop. 2011, 139, S60–S68. [Google Scholar] [CrossRef] [PubMed]
- Arat, M.; Iseri, H. Orthodontic and orthopaedic approach in the treat-ment of skeletal open bite. Eur. J. Orthod. 1992, 14, 207–215.20. [Google Scholar] [CrossRef] [PubMed]
- Kucukkeles, N.; Acar, A.; Demirkaya, A.A.; Evrenol, B.; Enacar, A. Cephalometric evaluation of open bite treatment with NiTi arch wiresand anterior elastics. Am. J. Orthod. Dentofac. Orthop. 1999, 116, 555–562. [Google Scholar] [CrossRef]
- Chang, Y.I.; Moon, S.C. Cephalometric evaluation of the anterior open bite treatment. Am. J. Orthod. Dentofac. Orthop. 1999, 115, 29–38. [Google Scholar] [CrossRef]
- Ryan, M.J.; Schneider, B.J.; BeGole, E.A.; Muhl, Z.F. Opening rotations of the mandible during and after treatment. Am. J. Orthod. Dentofac. Orthop. 1998, 114, 142–149. [Google Scholar] [CrossRef] [PubMed]
- Robertson, L.; Kaur, H.; Fagundes, N.C.F.; Romanyk, D.; Major, P.; Flores Mir, C. Effectiveness of clear aligner therapy for orthodontic treatment: A systematic review. Orthod. Craniofac. Res. 2020, 23, 133–142. [Google Scholar] [CrossRef]
- Boyd, R.L. Esthetic orthodontic treatment using the invisalign appliance for moderate to complex malocclusions. J. Dent. Educ. 2008, 72, 948–967. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).