
Automated Breast Lesion Detection and Characterization with the Wavelia Microwave Breast Imaging System: Methodological Proof-of-Concept on First-in-Human Patient Data

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
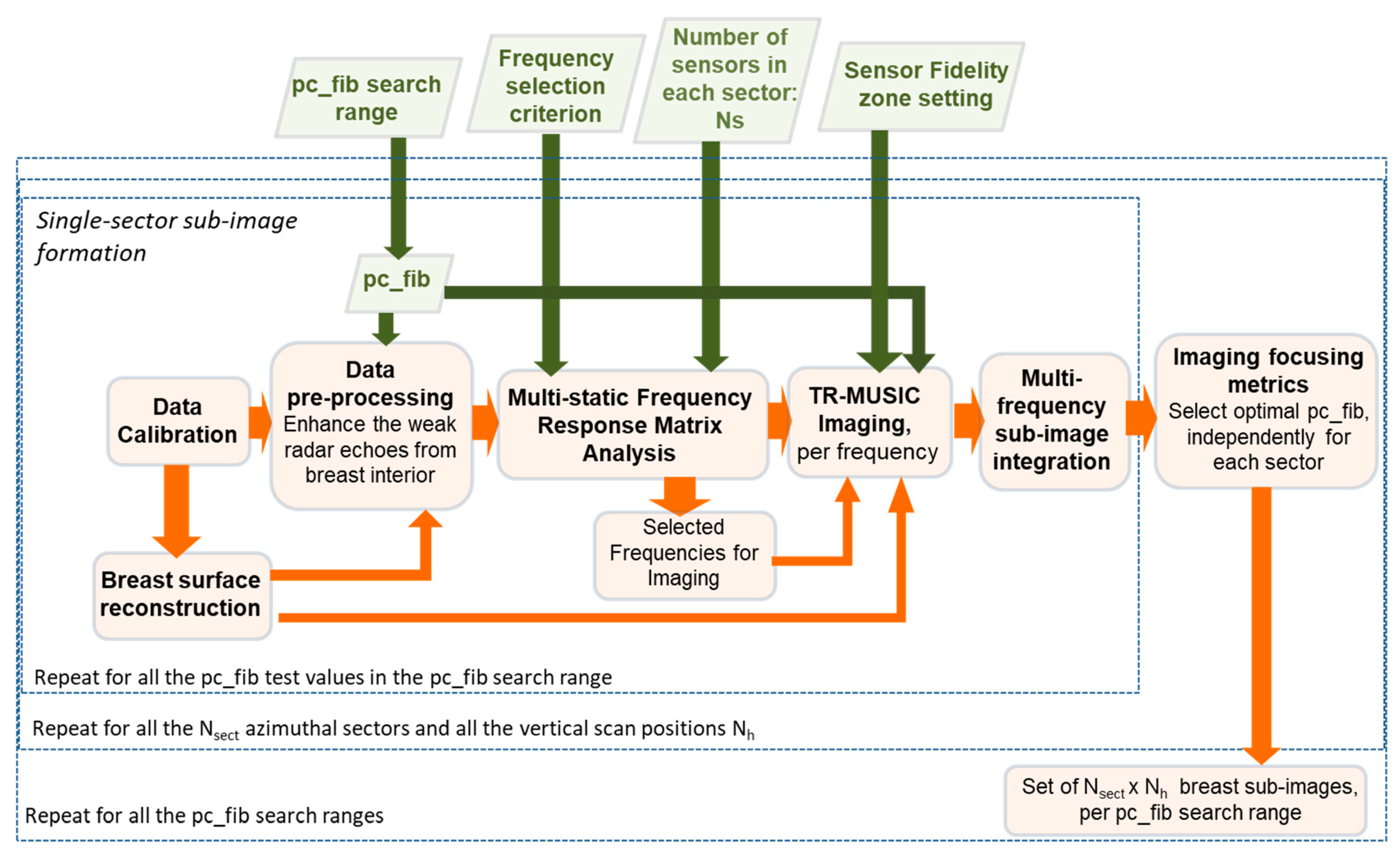
2.1. Wavelia MBI: Parametric Radar Image Formation
- Sectorization of the imaging scene: Considering the high level of heterogeneity of the breast tissues, but also the potentially irregularly shaped breast tumours, MBI image formation is performed using sectorized subsets of the circular sensor network of the Wavelia MBI system, at each vertical scan position. Both the physical size of the sensor sub-array (sector) and the number Ns of sensors used for the elementary sub-image formation is critical to the achievable performance of the MBI system, in terms of unambiguous detection and valid characterization of breast lesions. Ns = 6 was fixed in the Wavelia QIF for the FiH clinical investigation.
- Sensor fidelity zone setting: Bounding the portion of the imaging scene, being efficiently illuminated by each sensor sub-array. In the current implementation of the Wavelia QIF, a spatial filter activates the contribution of a given antenna to a given pixel p in the imaging scene, only if the Euclidean distance between the pixel and the phase centre of the antenna is inferior to a pre-set value dmax.
- Automated, data-driven, frequency selection for imaging: The TR-MUSIC imaging is performed per frequency. In the Wavelia QIF, a limited number of frequency points is automatically selected for imaging in each azimuthal sector of illumination, based on the information content of the MFRM at each frequency. The employed frequency selection criterion was previously defined in [15].
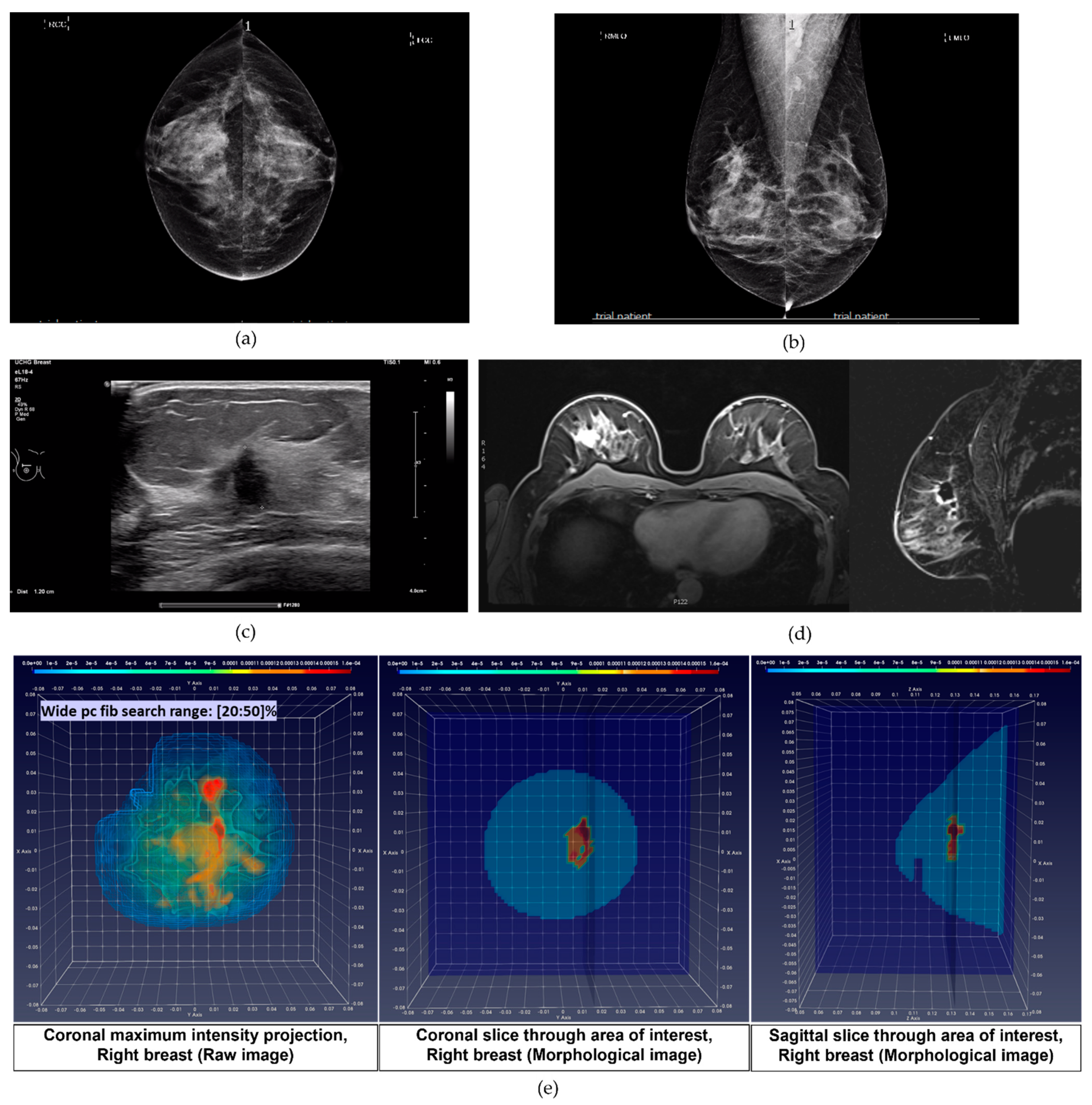
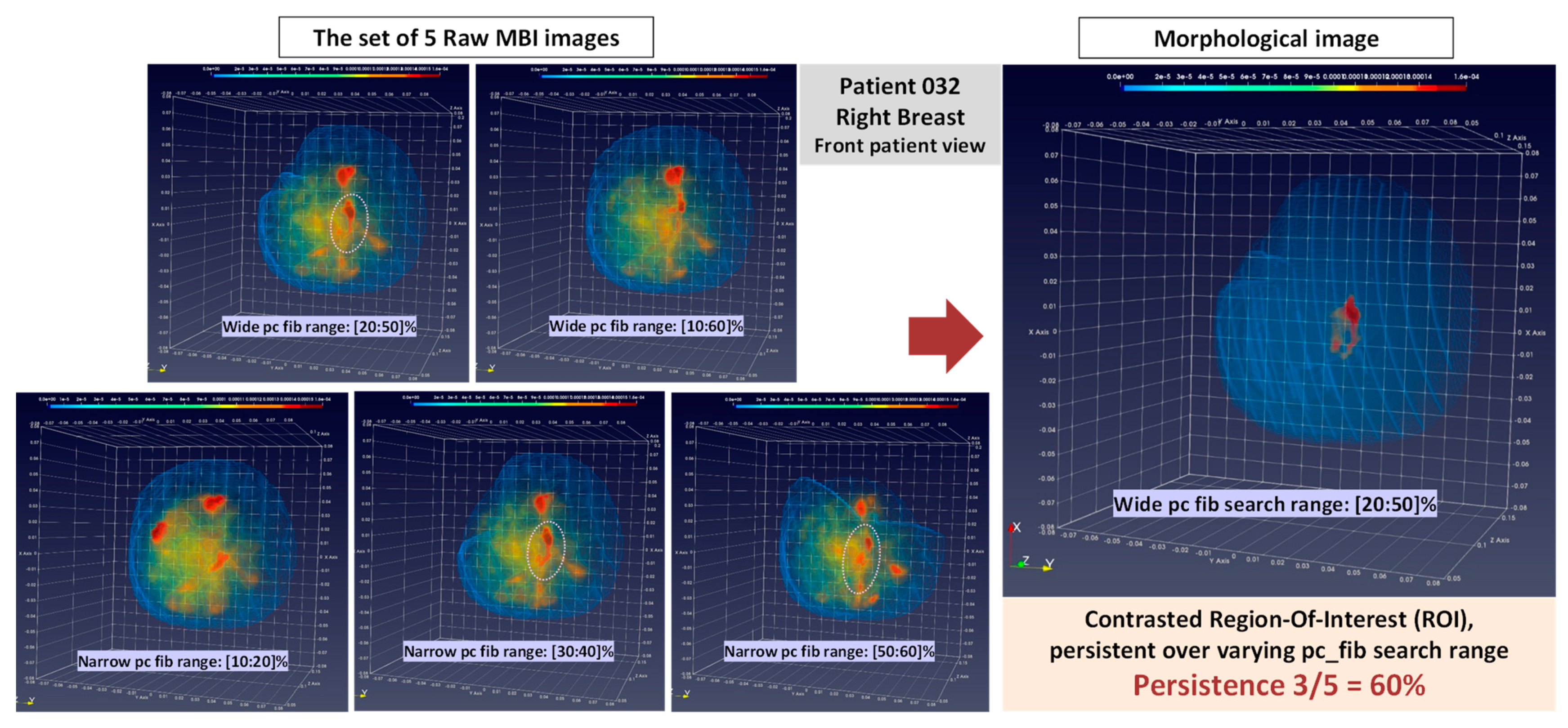
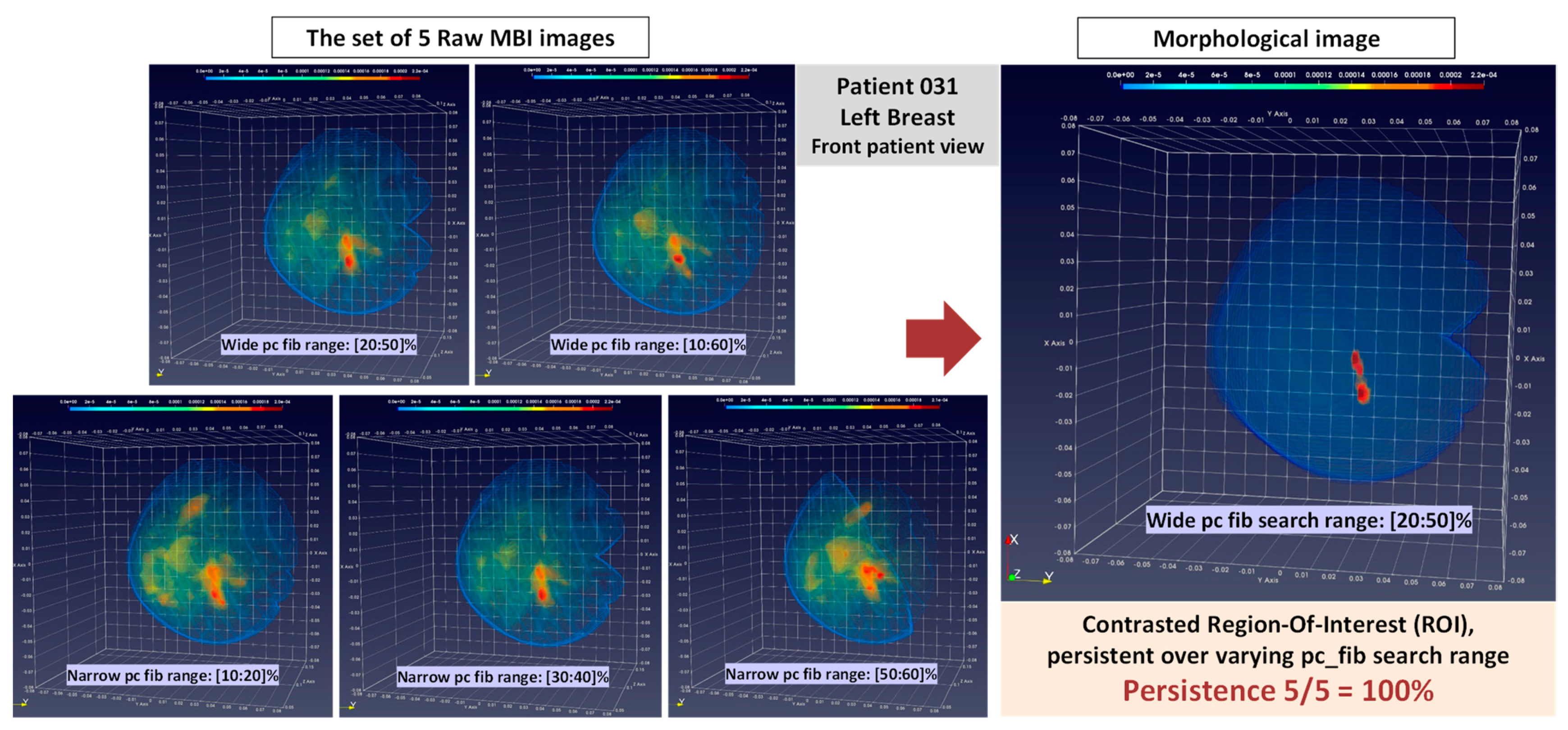
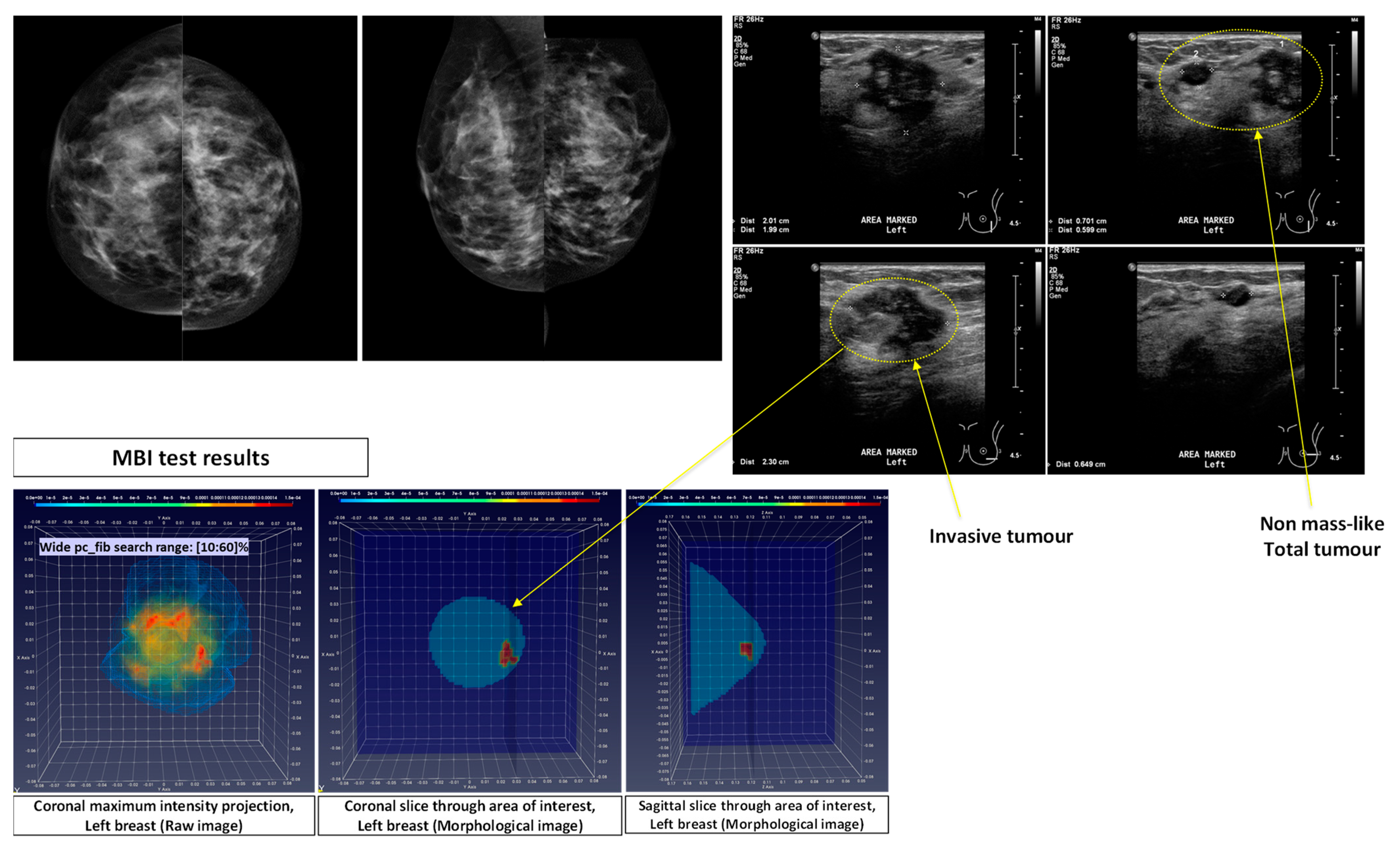
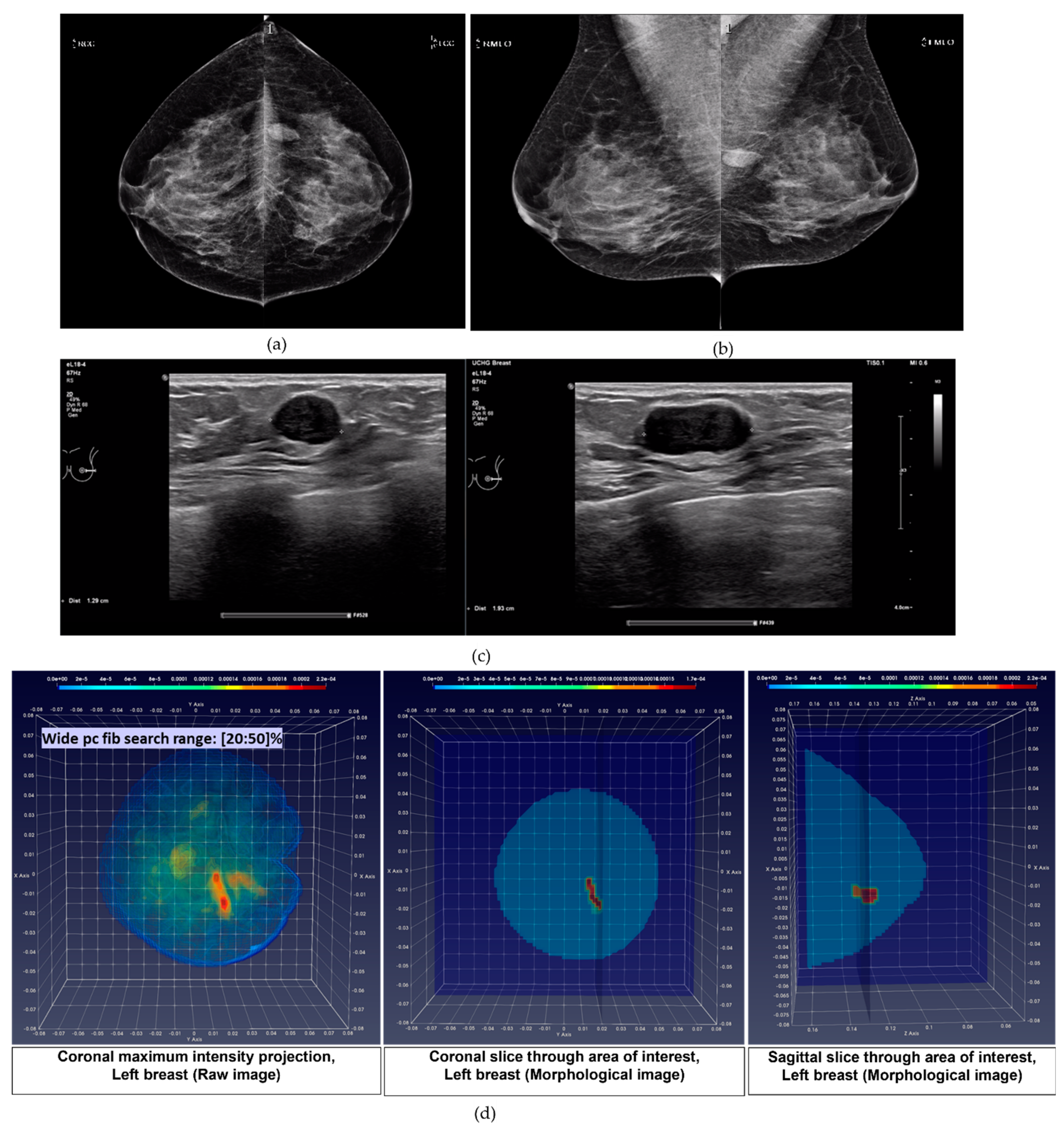
- pc_fib parameter setting in multiple search ranges: A large variability exists in the dielectric properties of each breast tissue type over the population, as demonstrated by multiple studies involving ex-vivo dielectric measurements of a large sample of excised breast tissues [18,19,20,21]. Considering that the full dielectric map of each breast cannot become practically available, data-driven techniques are employed in the Wavelia QIF to deduce the unknown dielectric properties of the healthy breast tissue in each breast, by assessing the pc_fib parameter. The pc_fib parameter, which is involved in the formulation of the illumination vector of the MBI sensor array, is physically associated with the percentage of fibro-glandular tissue along the propagation path within the breast, from a given transmitting antenna to the interrogated imaging pixel and back to a given receiving antenna, as defined in Equations (1)–(3). The Wavelia QIF generates a set of parametric MBI radar images under various assumptions on pc_fib. The generated set of parametric images is further evaluated in terms of focusing, using the image curvature [22,23] as a focusing quality measure. To better handle the heterogeneity of the breast and potentially better reveal the non-uniform angular response of the breast lesions to MBI, the pc_fib parameter setting is performed independently in each azimuthal imaging sector, while employing multiple search ranges. In the Wavelia QIF, X1 wide and X2 narrow pc_fib parameter search ranges are systematically employed for image formation, thus a total number of X = (X1 + X2) MBI images are formed per patient’s breast.
- Wide pc_fib search range #1 (W1): pc_fib ϵ [10 20 30 40 50 60]%
- Wide pc_fib search range #2 (W2): pc_fib ϵ [20 30 40 50]%
- Narrow pc_fib search range #1 (n1): pc_fib ϵ [10 20]%
- Narrow pc_fib search range #2 (n2): pc_fib ϵ [30 40]%
- Narrow pc_fib search range #3 (n3): pc_fib ϵ [50 60]%
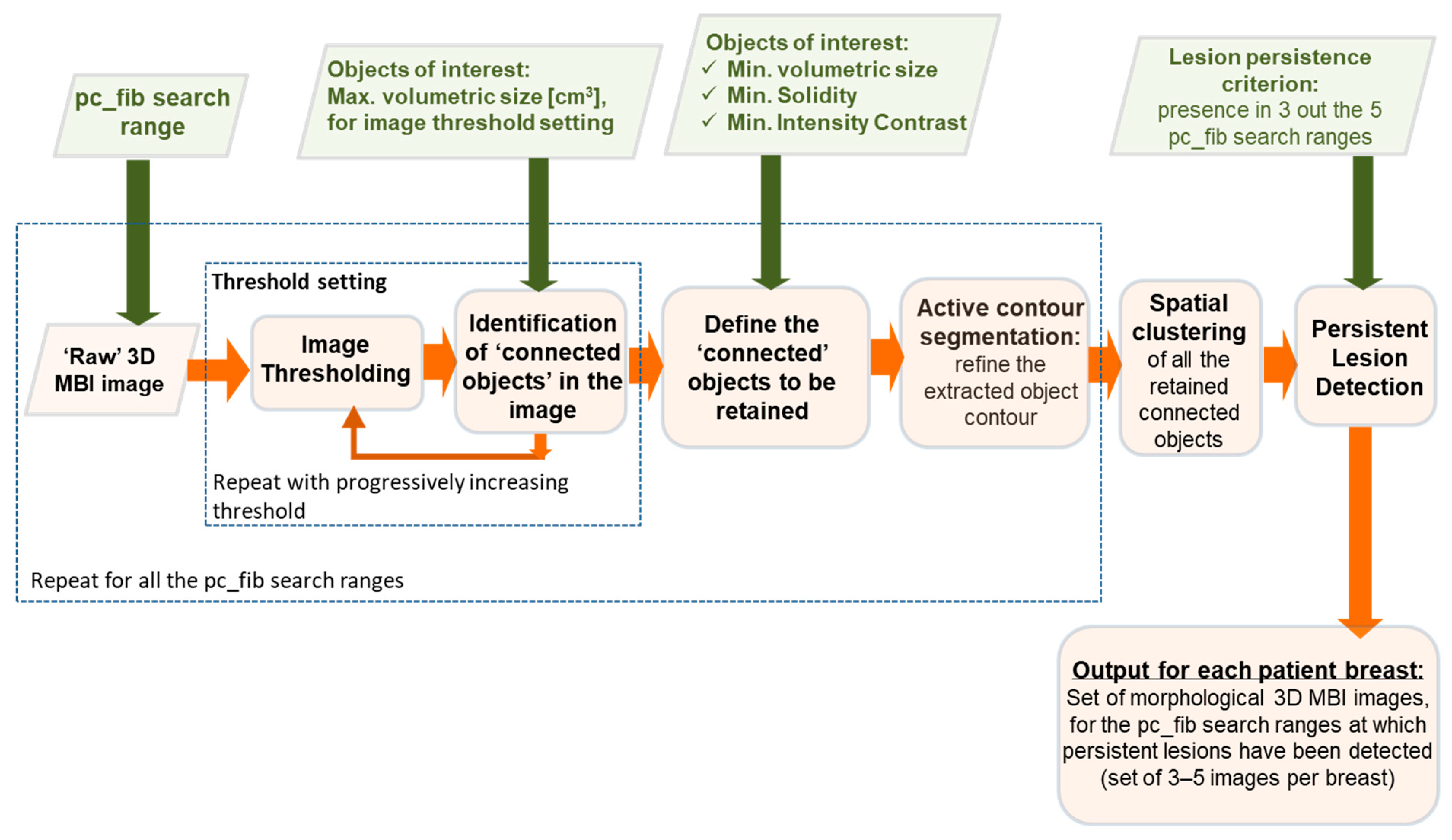
2.2. Morphological MBI Image Post-Processing: Breast Lesion Detection Based on Persistence
- Iterative Image threshold setting: The following operation is first-of-all performed to set a threshold for the raw 3D MBI image, with no a priori available on how normal breast tissue is represented in this type of image:
- Progressive increase in the image threshold, starting from the null threshold,
- At each iteration, identification of the “connected” objects in the thresholded image,
- Threshold setting based on the maximal accepted volumetric size of “connected” objects, potentially defining a breast mass in the image (default value 3 cm3, in this implementation).
- Semi-automated ROI extraction, based on morphological properties: The connected objects to be retained as ROIs, are defined based on a set of user-defined characteristics, including:
- Volumetric size: all the small objects, of volume inferior to 1 cm3, are removed from the FiH clinical data analysis, considering the status of the Wavelia system prototype #1 in terms of minimum size of detectable lesions.
- Solidity: this structural feature measures the density (or convexity) of an object. A measure of solidity can be obtained as a ratio of the volume of the object to the volume of a convex hull of the object. A value of 100% indicates a solid object, and a value less than 100% indicates an object having an irregular boundary or containing holes. All connected objects with solidity >30% have been ultimately retained, for the data analysis of the FiH clinical investigation of Wavelia.
- Intensity Contrast: In case of ambiguity (i.e., multiple connected objects to be retained in a single 3D MBI image, based on the volume and solidity criteria), each connected object is retained as ROI, only if it is associated with the maximal intensity in the image and is minimally contrasted (by at least 5%) against the intensity of all the “competing” connected objects in the image.
- Refinement of the ROI segmentation: An Active Contour segmentation module (Chan-Vese algorithm for segmentation without edges [25]) has been configured and employed to refine the contour of the extracted ROIs, in order to enable a more valid characterization of the lesions in terms of shape and texture, as defined in the following sub-section. This module may have a critical impact, especially in the case of small lesions, which are low contrasted against the background healthy breast tissue.
- Spatial clustering of the ROIs which have been extracted on the set of X MBI images, formed with varying pc_fib search ranges, is performed. In the current implementation of the Wavelia QIF, the Euclidean distance between the centroids of two ROIs is required to be shorter than dR = 1 cm for the ROIs to be associated with the same lesion in the breast.
- Persistence over varying pc-fib search range: Five pc-fib search ranges (2 wide and 3 narrow) are systematically used during the FiH clinical investigation of Wavelia to generate parametric 3D MBI images of each patient’s breast, as earlier stated. Detection of a breast lesion in a minimum number of parametric images (3 out of the 5 pc_fib search ranges) is required for a ROI to be considered persistent and validated.
2.3. Combination of 3D Shape Descriptors and Texture Features for Breast Lesion Characterization with Microwave Breast Imaging (MBI)
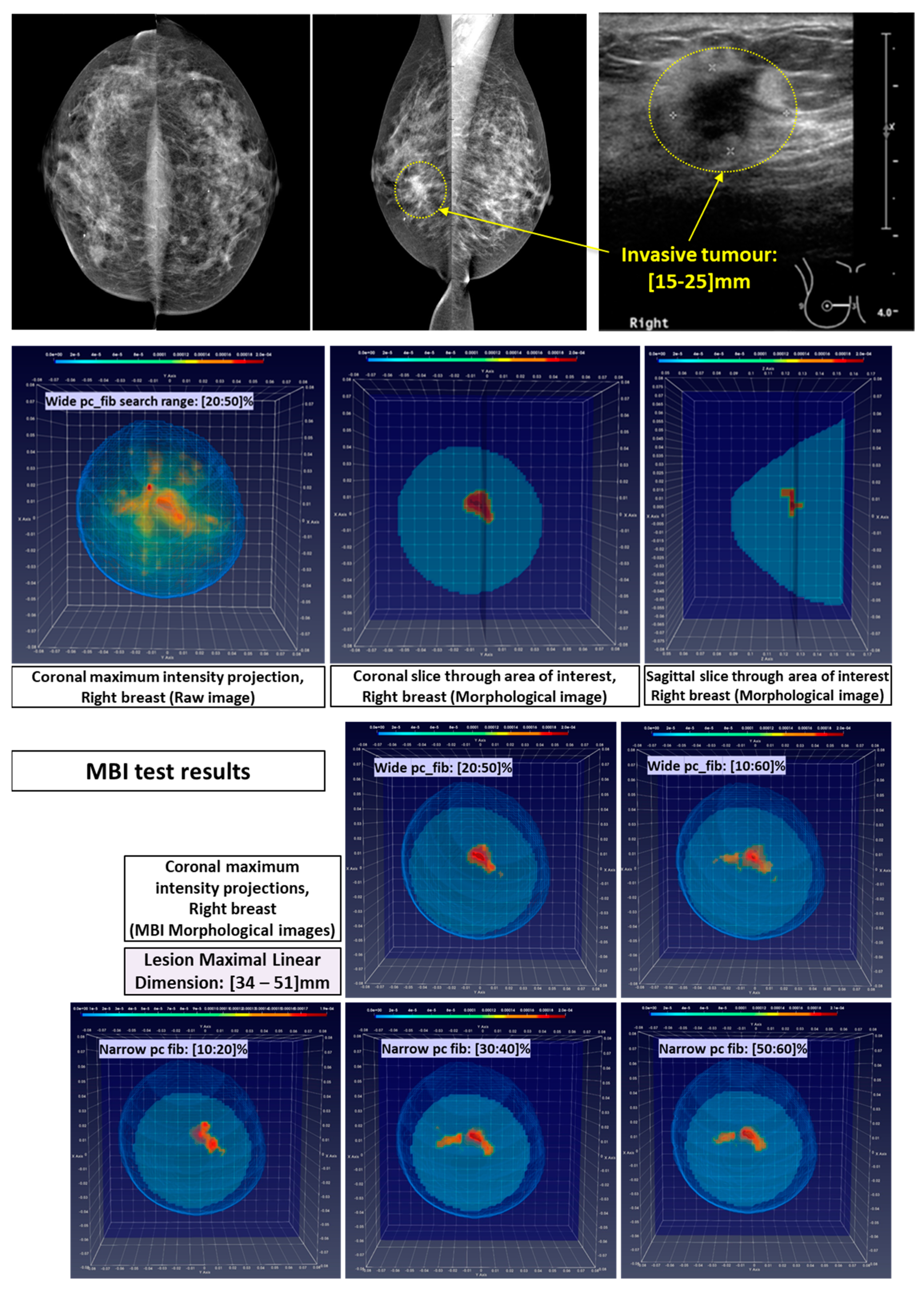
- Breast Lesion sizing: by means of fitting an ellipsoid to the ROI associated with the persistent lesion detection, in the 3D MBI images that have been generated by applying either of the two wide pc_fib search ranges. The greatest linear dimension of the lesion is defined as the length of the longest axis of the fitted ellipsoid. This definition is compatible with the conventional method that is applied for sizing breast abnormalities based on 2D mammography and ultrasound images [24,33]. During the FiH clinical investigation, the Wavelia MBI system showed promise for measuring lesion size with a more favorable linear trend between MBI and post-surgery histological lesion size, compared to the results obtained for conventional imaging [14]. Two challenging patient cases in terms of breast lesion sizing are indicatively discussed in Results Section 3.2, to better highlight the status of the MBI lesion sizing method, as integrated into the current version of the Wavelia QIF.
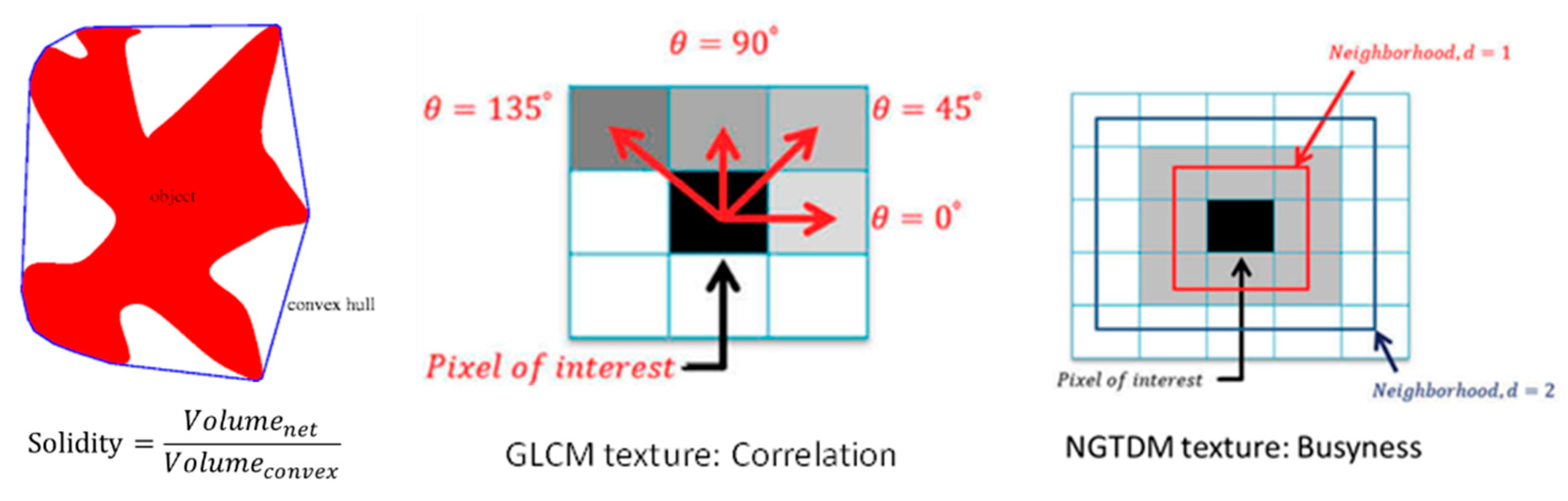
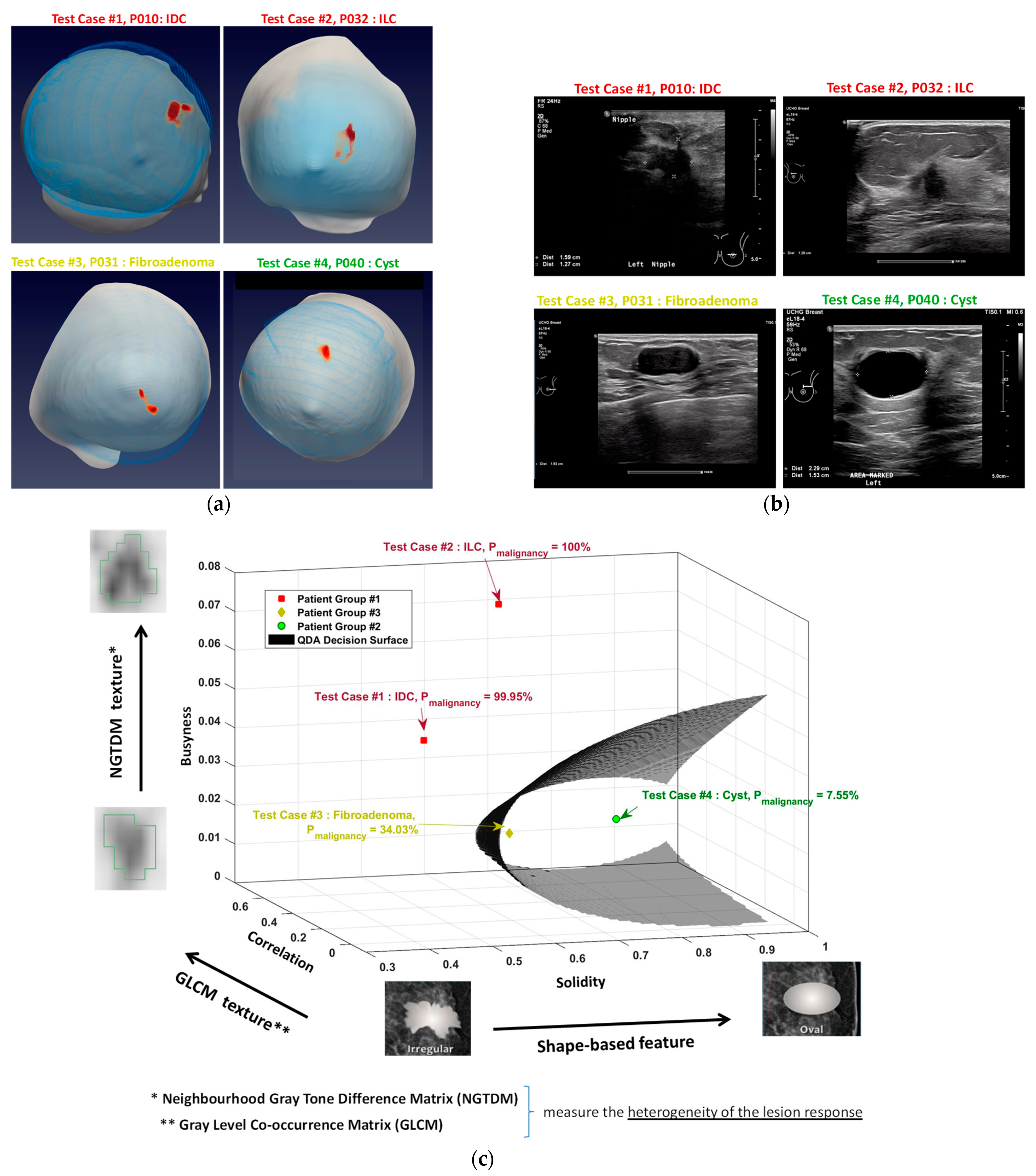
- Malignant-to-benign Breast Lesion labelling is performed in the Wavelia QIF using a combination of 3 features, extracted from morphologically validated ROIs in the MBI images. The selected features include: a shape descriptor [34], a Gray-Level Co-occurrence Matrix (GLCM) texture feature [35] and a Neighborhood Gray Tone Difference Matrix (NGTDM) texture feature [36]. The 3 features which were selected in the Wavelia QIF implementation for the FiH study of the investigational device are more specifically the following:
- ○
- Shape descriptors—Solidity: This feature measures the density, or the convexity, of an object. It is computed as the ratio of the volume of the object to the volume of the convex hull of the object, as illustrated in Figure 3. Breast lesion scoring, in terms of risk for malignancy, is routinely based on visual inspection and evaluation of the shape and margins of the imaged breast lesion, as per BIRADS [24,33]. Shape descriptors have been earlier considered for breast lesion classification with mammography [34,37] and ultrasound [38].
- ○
- GLCM texture—Correlation: The GLCM texture features measure the spatial relationship between pixels per specific directions, thus highlighting the properties of uniformity, homogeneity, randomness, and linear dependency of the image [35]. More specifically, the “correlation” feature varies between 0 (uncorrelated) and 1 (perfectly correlated), showing the linear dependency of gray level values to their respective voxels, as graphically illustrated in Figure 3.
- ○
- NGTDM texture—Busyness: The NGTDM texture features measure the spatial relationship among three or more pixels neighborhood, closely approaching the human perception of the image [36], as graphically illustrated in Figure 3 More specifically, for the “busyness” feature, a high value indicates a “busy” image, with rapid changes of intensity between pixels and its neighborhood.
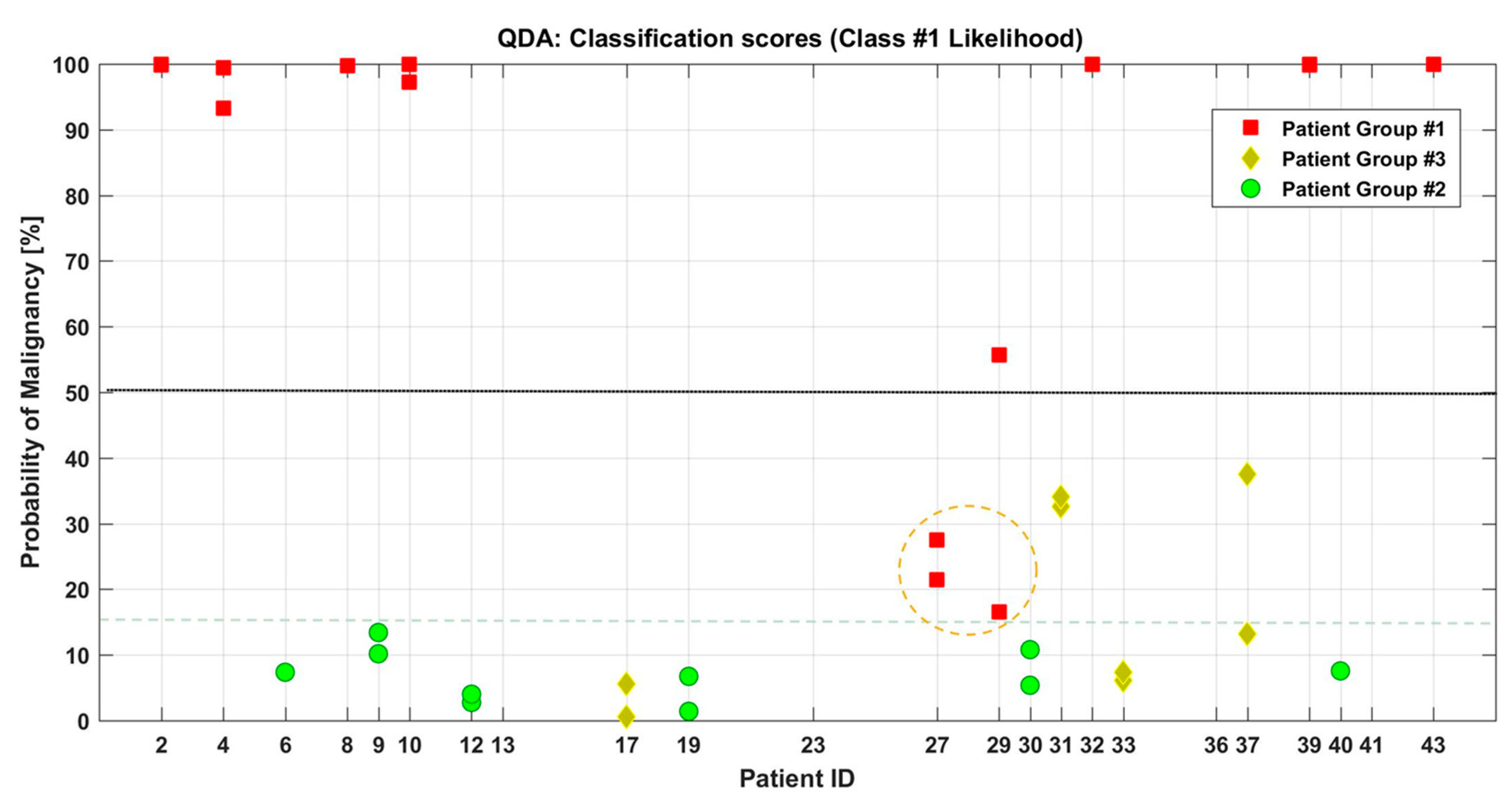
- The Group-1 patient datasets were labelled as Class #1.
- The Group-2 and Group-3 patient datasets were labelled as Class #2.
3. Results
3.1. Semi-Automated Breast Lesion Detection Based on Persistence
- Patient 032: Group-1: 54-years old patient with an Invasive Lobular Carcinoma (ILC) of size 30 mm (MRI data) at the 12 o’clock position of the Right Breast. Breast density: BIRADS Category c, Volumetric Breast Density (VBD) = 13.3%.
- Patient 031: Group 3: 38-years old patient with a Fibroadenoma of size 19 mm (Ultrasound) in the lateral Left Breast. Breast density: BIRADS Category c, VBD = 10.8%.
3.2. Breast Lesion Sizing: Correlation with Conventional Imaging and Post-Surgery Histology
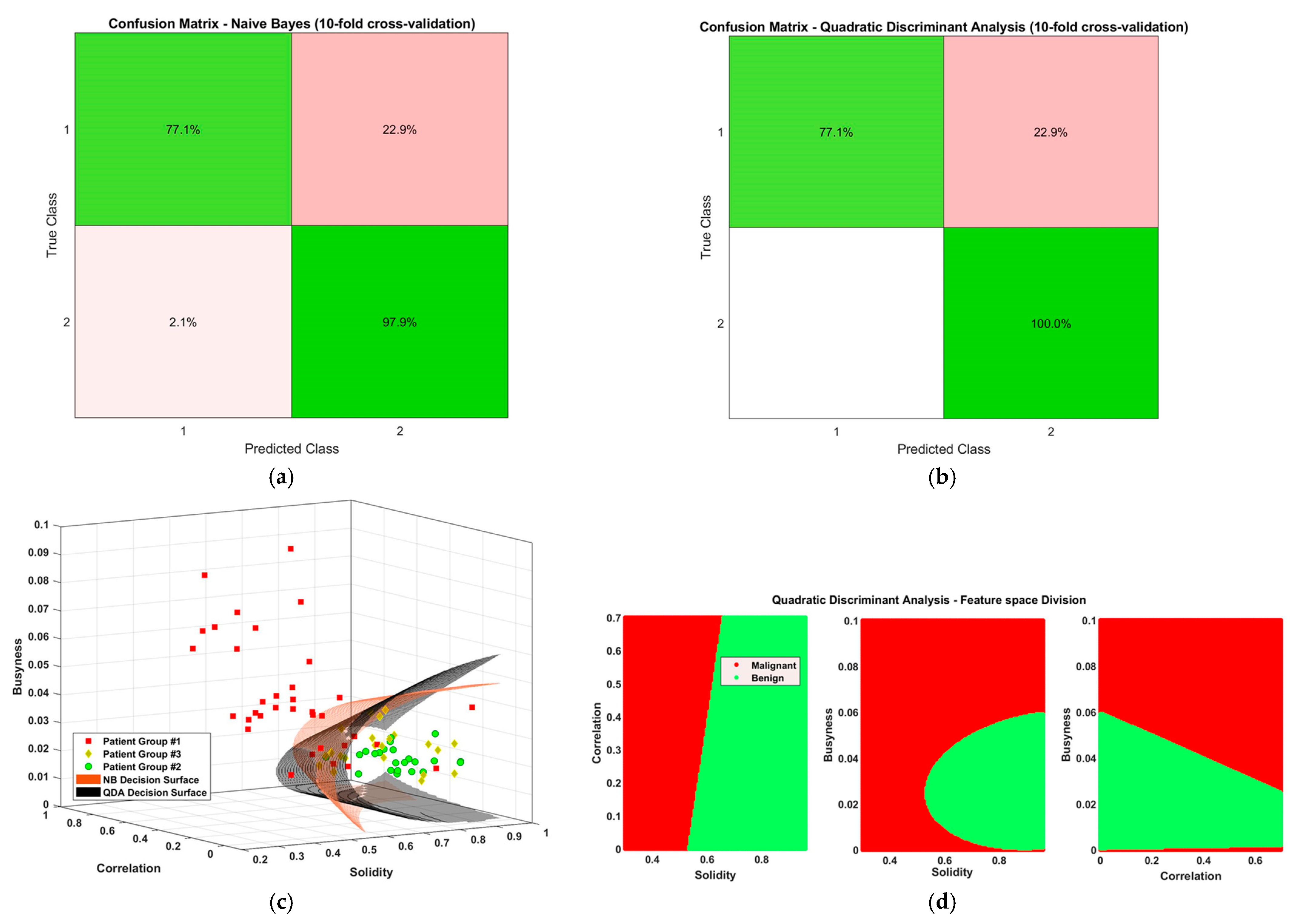
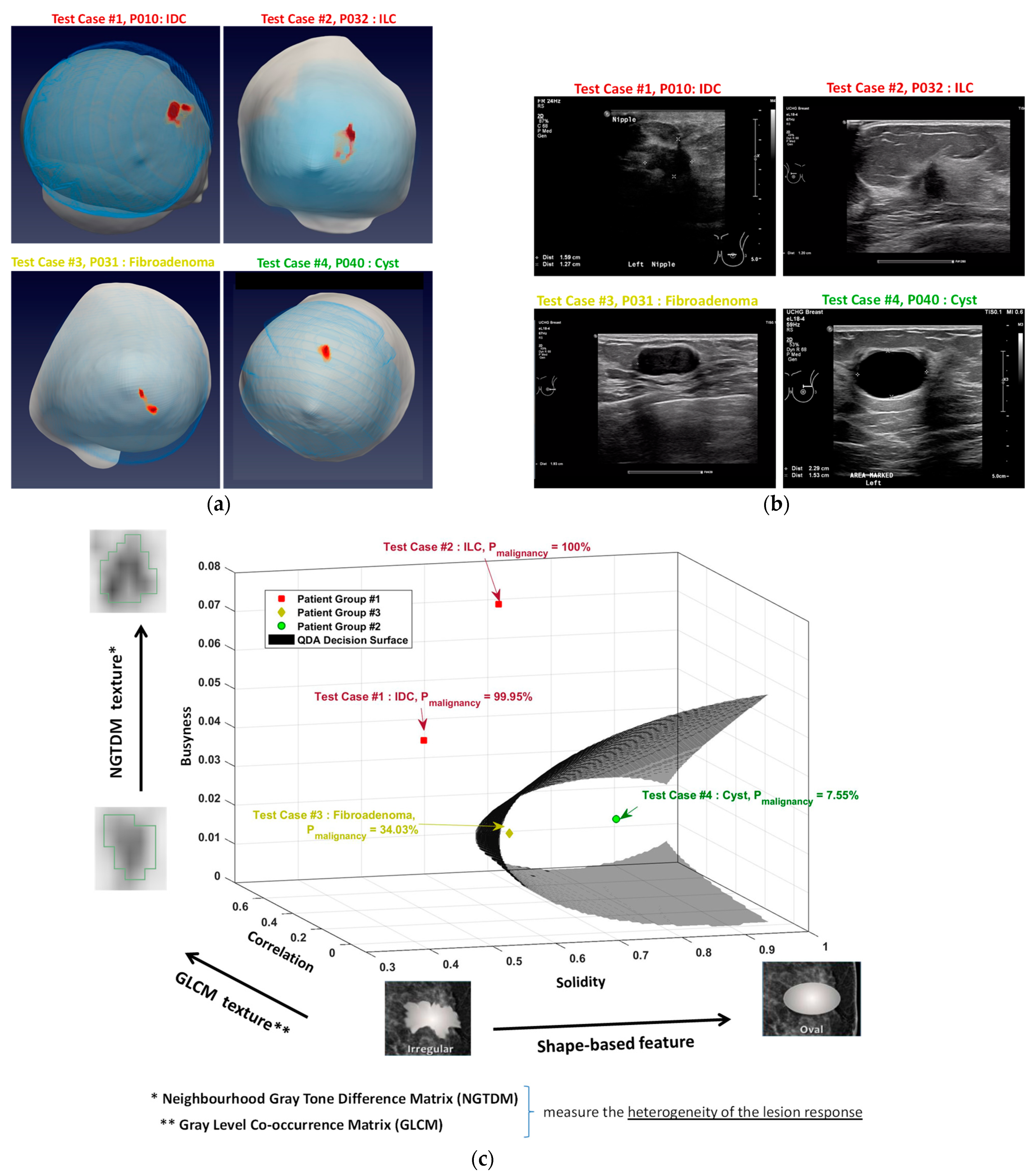
3.3. Discrimination between Malignant and Benign Breast Lesions in a 3-d Feature Space (Shape-Based and Texture-Based Feature Employment)
- the clear differentiability of the simple cyst (Patient 040) in terms of higher solidity,
- the fibroadenoma and the two cancerous lesions had similar solidity levels, however clear distinction was achieved between the benign and the two malignant lesions in terms of texture features,
- both the correlation and the busyness feature values were slightly increased in the case of the malignant lesions, with the increase being more notable on the busyness feature,
- substantially increased busyness value was associated with more heterogeneous lesion patterns, which may be interpretable as being indicative of distributed non-mass like ILC’s, such as in the Patient 032 case.
4. Discussion and Conclusions
5. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Conceição, R.; Mohr, J.; O’Halloran, M. An Introduction to Microwave Imaging for Breast Cancer Detection; Conceição, R.C., Mohr, J.J., O’Halloran, M., Eds.; Biological and Medical Physics, Biomedical Engineering; Springer International Publishing: Cham, Switerland, 2016; ISBN 978-3-319-27865-0. [Google Scholar]
- Gabriel, C. Compilation of the Dielectric Properties of Body Tissues at RF and Microwave Frequencies. Environ. Health 1996. Report N.AL/OE-TR-1996-0037. Available online: http://www.brooks.af.mil/HSC/AL/OE/OER/Title/Title.html (accessed on 18 October 2021).
- Campbell, A.M.; Land, D.V. Dielectric properties of female human breast tissue measured in vitro at 3.2 GHz. Phys. Med. Biol. 1992, 37, 193–210. [Google Scholar] [CrossRef] [PubMed]
- Shere, M.; Lyburn, I.; Sidebottom, R.; Massey, H.; Gillett, C.; Jones, L. MARIA® M5: A multicentre clinical study to evaluate the ability of the Micrima radio-wave radar breast imaging system (MARIA®) to detect lesions in the symptomatic breast. Eur. J. Radiol. 2019, 116, 61–67. [Google Scholar] [CrossRef]
- Sani, L.; Ghavami, N.; Vispa, A.; Paoli, M.; Raspa, G.; Ghavami, M.; Sacchetti, F.; Vannini, E.; Ercolani, S.; Saracini, A.; et al. Novel microwave apparatus for breast lesions detection: Preliminary clinical results. Biomed. Signal Process. Control 2019, 52, 257–263. [Google Scholar] [CrossRef]
- Janjic, A.; Cayoren, M.; Akduman, I.; Yilmaz, T.; Onemli, E.; Bugdayci, O.; Aribal, M.E. SAFE: A Novel Microwave Imaging System Design for Breast Cancer Screening and Early Detection—Clinical Evaluation. Diagnostics 2021, 11, 533. [Google Scholar] [CrossRef]
- Meaney, P.M.; Kaufman, P.A.; Muffly, L.S.; Click, M.; Poplack, S.P.; Wells, W.A.; Schwartz, G.N.; di Florio-Alexander, R.M.; Tosteson, T.D.; Li, Z.; et al. Microwave imaging for neoadjuvant chemotherapy monitoring: Initial clinical experience. Breast Cancer Res. 2013, 15, R35. [Google Scholar] [CrossRef] [Green Version]
- Benny, R.; Anjit, T.A.; Mythili, P. An overview of microwave imaging for breast tumor detection. Prog. Electromagn. Res. B 2020, 87, 61–91. [Google Scholar] [CrossRef]
- Moloney, B.M.; O’Loughlin, D.; Abd Elwahab, S.; Kerin, M.J. Breast Cancer Detection—A Synopsis of Conventional Modalities and the Potential Role of Microwave Imaging. Diagnostics 2020, 10, 103. [Google Scholar] [CrossRef] [Green Version]
- O’Loughlin, D.; O’Halloran, M.; Moloney, B.M.; Glavin, M.; Jones, E.; Elahi, M.A. Microwave Breast Imaging: Clinical Advances and Remaining Challenges. IEEE Trans. Biomed. Eng. 2018, 65, 2580–2590. [Google Scholar] [CrossRef]
- Kwon, S.; Lee, S. Recent Advances in Microwave Imaging for Breast Cancer Detection. Int. J. Biomed. Imaging 2016, 2016, 5054912. [Google Scholar] [CrossRef] [PubMed]
- Moloney, B.M.; McAnena, P.F.; Abd Elwahab, S.M.; Fasoula, A.; Duchesne, L.; Gil Cano, J.D.; Glynn, C.; O’Connell, A.; Ennis, R.; Lowery, A.J.; et al. Microwave Imaging in Breast Cancer—Results from the First-In-Human Clinical Investigation of the Wavelia System. Acad. Radiol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Fasoula, A.; Duchesne, L.; Gil Cano, J.; Lawrence, P.; Robin, G.; Bernard, J.-G. On-Site Validation of a Microwave Breast Imaging System, before First Patient Study. Diagnostics 2018, 8, 53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moloney, B.M.; McAnena, P.F.; Elwahab, S.M.; Fasoula, A.; Duchesne, L.; Gil Cano, J.D.; Glynn, C.; O’Connell, A.; Ennis, R.; Lowery, A.J.; et al. The Wavelia Microwave Breast Imaging system–tumour discriminating features and their clinical usefulness. Br. J. Radiol. 2021. epub ahead of print. [Google Scholar] [CrossRef]
- Fasoula, A.; Moloney, B.M.; Duchesne, L.; Cano, J.D.G.; Oliveira, B.L.; Bernard, J.; Kerin, M.J. Super-resolution radar imaging for breast cancer detection with microwaves: The integrated information selection criteria. In Proceedings of the 41st Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Berlin, Germany, 23–27 July 2019. [Google Scholar]
- Fasoula, A.; Duchesne, L.; Moloney, B.M.; Gil Cano, J.D.; Chenot, C.; Oliveira, B.L.; Bernard, J.-G.; Abd Elwahab, S.M.; Kerin, M.J. Pilot patient study with the Wavelia Microwave Breast Imaging system for breast cancer detection: Clinical feasibility and identified technical challenges. In Proceedings of the 2020 14th European Conference on Antennas and Propagation (EuCAP), Copenhagen, Denmark, 15–20 March 2020. [Google Scholar]
- Devaney, A. Super-resolution processing of multi-static data using time reversal and MUSIC. J. Acoust. Soc. Am. 2000. Available online: https://ece.northeastern.edu/fac-ece/devaney/preprints/paper02n_00.pdf (accessed on 18 October 2021).
- Sugitani, T.; Kubota, S.; Kuroki, S.; Sogo, K.; Arihiro, K.; Okada, M.; Kadoya, T.; Hide, M.; Oda, M.; Kikkawa, T. Complex permittivities of breast tumor tissues obtained from cancer surgeries. Appl. Phys. Lett. 2014, 104, 253702. [Google Scholar] [CrossRef]
- Lazebnik, M.; Popovic, D.; McCartney, L.; Watkins, C.B.; Lindstrom, M.J.; Harter, J.; Sewall, S.; Ogilvie, T.; Magliocco, A.; Breslin, T.M.; et al. A large-scale study of the ultrawideband microwave dielectric properties of normal, benign and malignant breast tissues obtained from cancer surgeries. Phys. Med. Biol. 2007, 52, 6093–6115. [Google Scholar] [CrossRef] [PubMed]
- Martellosio, A.; Bellomi, M.; Pasian, M.; Bozzi, M.; Perregrini, L.; Mazzanti, A.; Svelto, F.; Summers, P.E.; Renne, G.; Preda, L. Dielectric Properties Characterization From 0.5 to 50 GHz of Breast Cancer Tissues. IEEE Trans. Microw. Theory Tech. 2017, 65, 998–1011. [Google Scholar] [CrossRef]
- Summers, P.E.; Vingiani, A.; Di Pietro, S.; Martellosio, A.; Espin-Lopez, P.F.; Di Meo, S.; Pasian, M.; Ghitti, M.; Mangiacotti, M.; Sacchi, R.; et al. Towards mm-wave spectroscopy for dielectric characterization of breast surgical margins. The Breast 2019, 45, 64–69. [Google Scholar] [CrossRef]
- Pertuz, S.; Puig, D.; Garcia, M.A. Analysis of focus measure operators for shape-from-focus. Pattern Recognit. 2013, 46, 1415–1432. [Google Scholar] [CrossRef]
- O’loughlin, D.; Krewer, F.; Glavin, M.; Jones, E.; O’halloran, M. Focal quality metrics for the objective evaluation of confocal microwave images. Int. J. Microw. Wirel. Technol. 2017, 9, 1365–1372. [Google Scholar] [CrossRef] [Green Version]
- Sickles, E.A.; D’Orsi, C.J.; Bassett, L.W.; Appleton, C.M.; Berg, W.A.; Burnside, E.S. Acr Bi-Rads®Mammography. In ACR BI-RADS®Atlas, Breast Imaging Reporting and Data System; American College of Radiology: Reston, VA, USA, 2013; Volume 5. [Google Scholar]
- Chan, T.F.; Vese, L.A. Active contours without edges. IEEE Trans. Image Process. 2001, 10, 266–277. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.; Gunawan, E.; Low, K.S.; Wang, S.C.; Soh, C.B.; Putti, T.C. Effect of Lesion Morphology on Microwave Signature in 2-D Ultra-Wideband Breast Imaging. IEEE Trans. Biomed. Eng. 2008, 55, 2011–2021. [Google Scholar] [CrossRef] [PubMed]
- Davis, S.K.; Van Veen, B.D.; Hagness, S.C.; Kelcz, F. Breast Tumor Characterization Based on Ultrawideband Microwave Backscatter. IEEE Trans. Biomed. Eng. 2008, 55, 237–246. [Google Scholar] [CrossRef]
- Gerazov, B.; Conceicao, R.C. Deep learning for tumour classification in homogeneous breast tissue in medical microwave imaging. In Proceedings of the IEEE EUROCON 2017-17th International Conference on Smart Technologies, Ohrid, Macedonia, 6–8 July 2017; pp. 564–569. [Google Scholar]
- Oliveira, B.; Godinho, D.; O’Halloran, M.; Glavin, M.; Jones, E.; Conceição, R. Diagnosing Breast Cancer with Microwave Technology: Remaining challenges and potential solutions with machine learning. Diagnostics 2018, 8, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conceição, R.C.; Medeiros, H.; Godinho, D.M.; O’Halloran, M.; Rodriguez-Herrera, D.; Flores-Tapia, D.; Pistorius, S. Classification of breast tumor models with a prototype microwave imaging system. Med. Phys. 2020, 47, 1860–1870. [Google Scholar] [CrossRef]
- Doshi, T.; Lyburn, I.; Sidebottom, R.; Gibbins, D. Radio-wave imaging: Frequency response as an aid to lesion characterization. Early concept work. In Proceedings of the Symposium Mammographicum, Liverpool, UK, 8–10 July 2018. [Google Scholar]
- Rana, S.P.; Dey, M.; Tiberi, G.; Sani, L.; Vispa, A.; Raspa, G.; Duranti, M.; Ghavami, M.; Dudley, S. Machine Learning Approaches for Automated Lesion Detection in Microwave Breast Imaging Clinical Data. Sci. Rep. 2019, 9, 10510. [Google Scholar] [CrossRef] [Green Version]
- Mendelson, E.B.; Böhm-Vélez, M.; Berg, W.A. ACR BI-RADS® Ultrasound. In ACR BI-RADS®Atlas, Breast Imaging Reporting and Data System; American College of Radiology: Reston, VA, USA, 2013. [Google Scholar]
- De Brito Silva, T.F.; de Paiva, A.C.; Silva, A.C.; Braz Júnior, G.; de Almeida, J.D.S. Classification of breast masses in mammograms using geometric and topological feature maps and shape distribution. Res. Biomed. Eng. 2020, 36, 225–235. [Google Scholar] [CrossRef]
- Haralick, R.M.; Shanmugam, K.; Dinstein, I. Textural Features for Image Classification. IEEE Trans. Syst. Man. Cybern. 1973, SMC-3, 610–621. [Google Scholar] [CrossRef] [Green Version]
- Amadasun, M.; King, R. Textural features corresponding to textural properties. IEEE Trans. Syst. Man. Cybern. 1989, 19, 1264–1274. [Google Scholar] [CrossRef]
- Safdarian, N.; Hedyezadeh, M. Detection and Classification of Breast Cancer in Mammography Images Using Pattern Recognition Methods. Multidiscip. Cancer Investig. 2019, 3, 13–24. [Google Scholar] [CrossRef]
- Sadad, T.; Hussain, A.; Munir, A.; Habib, M.; Ali Khan, S.; Hussain, S.; Yang, S.; Alawairdhi, M. Identification of Breast Malignancy by Marker-Controlled Watershed Transformation and Hybrid Feature Set for Healthcare. Appl. Sci. 2020, 10, 1900. [Google Scholar] [CrossRef] [Green Version]
- Vallières, M.; Freeman, C.R.; Skamene, S.R.; El Naqa, I. A radiomics model from joint FDG-PET and MRI texture features for the prediction of lung metastases in soft-tissue sarcomas of the extremities. Phys. Med. Biol. 2015, 60, 5471–5496. [Google Scholar] [CrossRef] [PubMed]
- Parekh, V.; Jacobs, M.A. Radiomics: A new application from established techniques. Expert Rev. Precis. Med. Drug Dev. 2016, 1, 207–226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coroller, T.P.; Grossmann, P.; Hou, Y.; Rios Velazquez, E.; Leijenaar, R.T.H.; Hermann, G.; Lambin, P.; Haibe-Kains, B.; Mak, R.H.; Aerts, H.J.W.L. CT-based radiomic signature predicts distant metastasis in lung adenocarcinoma. Radiother. Oncol. 2015, 114, 345–350. [Google Scholar] [CrossRef] [PubMed]
- Parekh, V.S.; Jacobs, M.A. Multiparametric radiomics methods for breast cancer tissue characterization using radiological imaging. Breast Cancer Res. Treat. 2020, 180, 407–421. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient ID | Post-Surgery Histology | MBI | Conventional Imaging | |||||
|---|---|---|---|---|---|---|---|---|
| Invasive Tumor | Total Tumor | W1 | W2 | Max. | Mammography | Ultrasound | Max. | |
| P002 | 20 | 40 | 51 | 34 | 51 | 25 | 15 | 25 |
| P029 | 22 | 35 | 24.5 | 19.8 | 24.5 | 20 | 37 | 37 |
| Patient ID | Lesion Histological Type | Features | Probability of Malignancy [%] | ||
|---|---|---|---|---|---|
| Solidity | Correlation | Busyness | |||
| P010 | Invasive Ductal Carcinoma | 0.529 | 0.496 | 0.041 | 99.95% |
| P032 | Invasive Lobular Carcinoma | 0.661 | 0.556 | 0.074 | 100% |
| P031 | Fibroadenoma | 0.643 | 0.403 | 0.018 | 34.03% |
| P040 | Simple Cyst | 0.816 | 0.422 | 0.02 | 7.55% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fasoula, A.; Duchesne, L.; Gil Cano, J.D.; Moloney, B.M.; Abd Elwahab, S.M.; Kerin, M.J. Automated Breast Lesion Detection and Characterization with the Wavelia Microwave Breast Imaging System: Methodological Proof-of-Concept on First-in-Human Patient Data. Appl. Sci. 2021, 11, 9998. https://doi.org/10.3390/app11219998
Fasoula A, Duchesne L, Gil Cano JD, Moloney BM, Abd Elwahab SM, Kerin MJ. Automated Breast Lesion Detection and Characterization with the Wavelia Microwave Breast Imaging System: Methodological Proof-of-Concept on First-in-Human Patient Data. Applied Sciences. 2021; 11(21):9998. https://doi.org/10.3390/app11219998
Chicago/Turabian StyleFasoula, Angie, Luc Duchesne, Julio Daniel Gil Cano, Brian M. Moloney, Sami M. Abd Elwahab, and Michael J. Kerin. 2021. "Automated Breast Lesion Detection and Characterization with the Wavelia Microwave Breast Imaging System: Methodological Proof-of-Concept on First-in-Human Patient Data" Applied Sciences 11, no. 21: 9998. https://doi.org/10.3390/app11219998
APA StyleFasoula, A., Duchesne, L., Gil Cano, J. D., Moloney, B. M., Abd Elwahab, S. M., & Kerin, M. J. (2021). Automated Breast Lesion Detection and Characterization with the Wavelia Microwave Breast Imaging System: Methodological Proof-of-Concept on First-in-Human Patient Data. Applied Sciences, 11(21), 9998. https://doi.org/10.3390/app11219998