1. Introduction
Ectopic eruption of the first permanent maxillary molar (EEFPMM) is an un-frequent local eruption disturbance [
1,
2] generally related to the locking of the permanent molar at the cervical area of the adjacent deciduous molar [
3,
4], resulting in its “premature atypical resorption” [
5].
Generally, the ectopic eruption is defined as reversible when the permanent molar, after a more or less advanced deciduous molar root resorption, erupts into the oral cavity in a functional position within the occlusal plane [
3]; such a pattern was called ′jamp case’ by Young [
6]. Conversely, when the permanent molar remains locked distally under the deciduous, the ectopic eruption becomes irreversible; the term ‘hold’ was used by Young to describe such an irreversible type [
6].
Data emerging from scientific literature showed that permanent molars usually self-corrected by the age of 7 years [
7]. Consequently, a diagnosis of irreversible ectopic eruption could generally be performed starting from this age [
2,
3]. If irreversible ectopic eruption remains un-treated, early loss of the deciduous second molar, space loss, crowding of the corresponding arch segment, and impaction of the second premolars are commonly reported sequelae [
7,
8].
Several investigators have studied the possible etiologic factors of EEFPMM. Small dental arches and lack of bony growth in maxillary tuberosity, [
1] as well large teeth, an abnormal path of eruption of the permanent molar or its premature eruption [
9] have been considered as etiological factors. Also, Pulver [
10] suggested a combination of etiologic factors including the posterior position of the maxilla to the cranial base and the delayed calcification of the permanent first molar in the maxilla.
In addition, the higher prevalence of EEFPMM in children with adjunctive oro-facial or dental anomalies leads us to consider a possible association with genetic factors [
11].
The diagnosis of EEFPMM is essentially based on the clinical and radiographic findings [
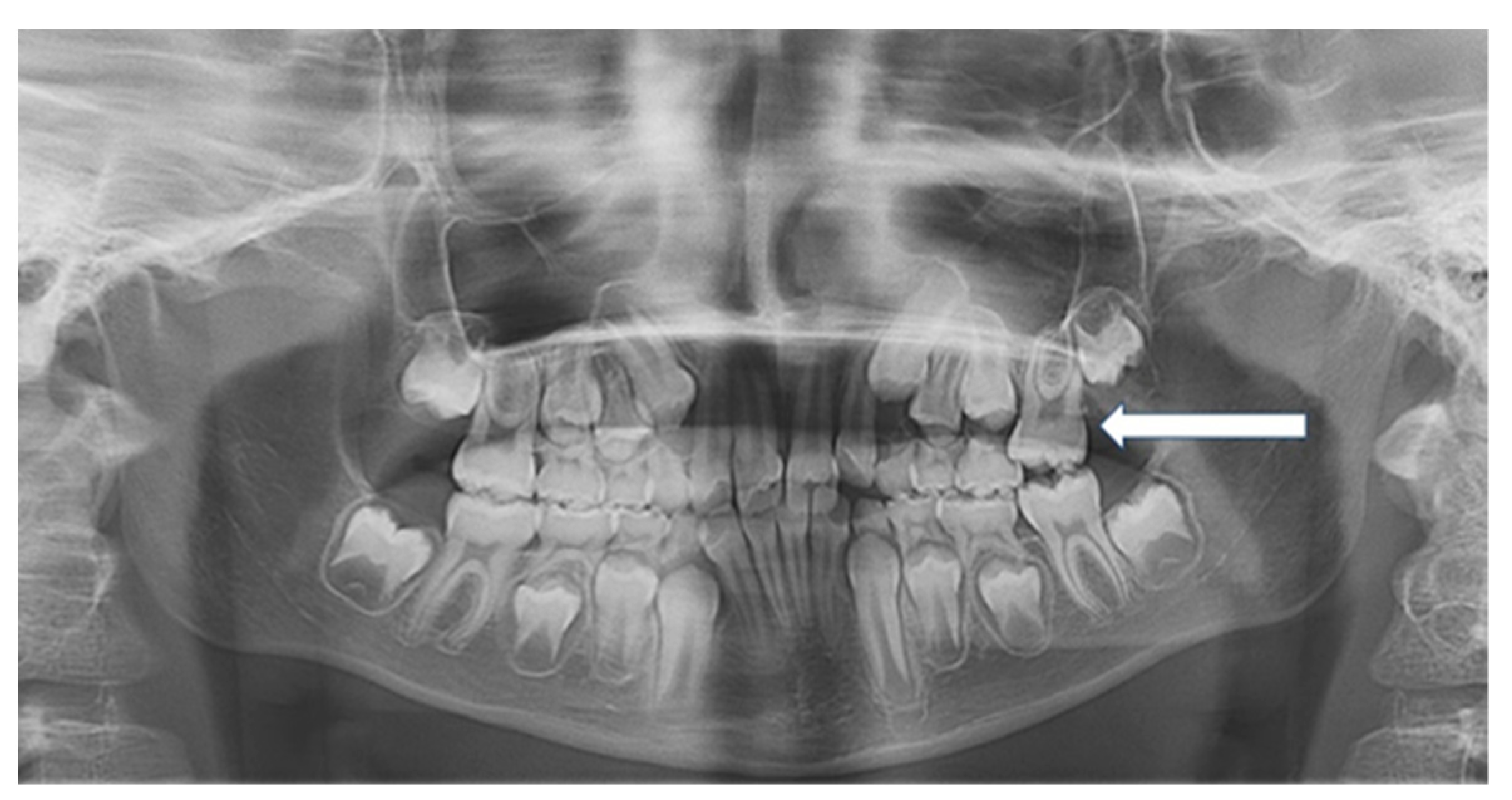
3] identifiable at a routine radiographic examination in a patient clinically missing the permanent first maxillary molar, or with the eruption of the distal cusps exclusively [
12].
Literature reports several staging methods of the severity of EEFPMM, generally based on the width of the impacted marginal ridge [
7,
9], the magnitude of the deciduous second molar distal resorption [
9,
12] or the amount of impaction measured as the distance from the maximum convexity of the permanent molar mesial contour to a tangential plane, to the distal surface of the deciduous one [
12].
The present retrospective study aims to investigate the cephalometric features of patients affected by ectopic eruption of the maxillary permanent first molar compared to a control group.
2. Materials and Methods
From a total of 1935 subjects, that were referred to the Dental Unit of the University-Hospital of the University of Bari “Aldo Moro”, and to a private dental clinic (between 2008 and 2018), a population of orthodontic patients, aged from 6 to 12 years, was screened. Inclusion criteria for the study group were as follows: unilateral or bilateral EEFPMM, no decay on maxillary deciduous second molars, availability of panoramic and lateral teleradiographs to investigate the cephalometric features. A number of 9 patients were excluded from the study because of incomplete or inadequate radiographic material. A total of 13 Caucasian patients (6 males, 7 females) were finally enrolled in the study group.
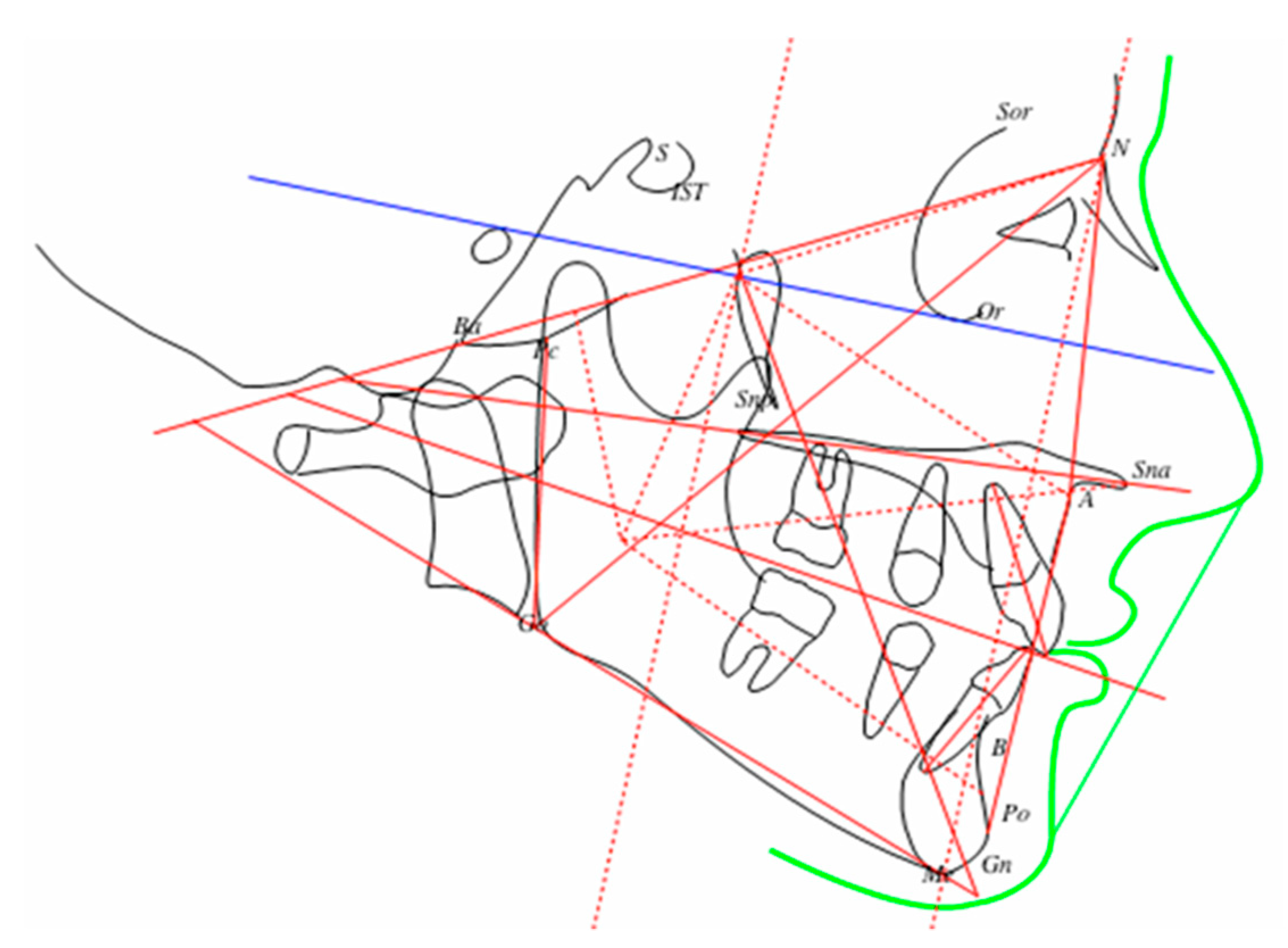
From the initial sample, a group of 26 patients (16 males, 10 females) with the same age range (from 6 to 12 years old) and showing normal eruption of the same tooth was randomly selected as a control group. No patient had received any previous orthodontic treatment. These patients were matched for age and sex with those affected by ectopic eruption. The lateral teleradiographs obtained at the time of diagnosis were scanned. The tracings of all subjects were made using the lines and angles as reported in
Figure 1.
In order to define the intra and inter-investigator reproducibility of measurements, and to evaluate the method error of the study, ten radiographs were traced three separate times by the principal investigator, and ten radiographs were randomly selected to be traced by another two clinicians.
Statistical Package for the Social Sciences (SPSS), version 15.0 (SPSS Inc, Chicago, Il, USA), was used for the statistical analysis. Mean and standard deviations (SDs) were calculated for each variable in both groups. The conventional t-test was used in the method error analysis. Since acceptable t values were found for all cephalometric variables, the error of measurements of this investigation could be considered acceptable. The differences between ectopic and normal eruption groups were compared by a chi-square test and t-test, after having tested the existence of the assumptions through the Shapiro-Wilk test for the normality of the distributions and through the Bartlett test for the equality of variances. A p-value less than 0.05 was set for the rejection of the null hypothesis, i.e., no significant difference in the measurements between groups.
3. Results
The prevalence of maxillary EEFPMM was 1.14% (13 of 1926 subjects). Descriptive statistics were computed for all variables. The means, SDs and the results of tests with the level of significance for each variable are listed in
Table 1.
The mandibular angle (SN-GoMe) was found to be significantly greater in the study group than in the control. The same statistical trend was reported for the inter-maxillary angle (SnaSnp-GoMe). The results showed that the distance Sna-Me was greater in the study group too. Differences among groups were statistically significant for the distances Snp-Sna, Ba-S and SOR-Sna, which were found to be greater in the study group. No statistically significant difference was observed for the remaining cephalometric variables contextually evaluated.
4. Discussion
Data from literature reported that patients with EEFPMM exhibit a tendency to dolichocephaly [
5]. The outcomes of the present investigation seem to be in accordance with such data as the study’s patients showed greater values of
SN-GoMe and
Sna-Snp-GoMe angles compared to the control group.
Conversely, studying the ectopic eruption of the maxillary second molars, Hwang et al. [
13] sustain that no relationships exist between the dolichocephalic pattern or the posterior rotation of the chin and ectopic eruption since molars were disto-bucally infra-occluded, and no opening effect on the posterior occlusion occurred [
13].
Also, it has been previously suggested that maxillary length plays an important role in the etiology of EEFPMM [
1,
5,
10]. A smaller and retro-positioned maxilla was found in affected patients too. Nevertheless, our results do not confirm to this cephalometric feature since the maxillary length was found to be significantly greater in patients of the study group. This finding leads us to assume that local factors, especially the space available for maxillary teeth, would not have a strong influence on ectopic eruption. From this perspective, a greater emphasis could be given to genetic causes rather than local factors in the development of the EEUPFM [
14].
In fact, the importance of genetic factors and their possible link with ectopic eruption was underlined by Kurol and Bjerklin, which reported a prevalence of 19.8% in the siblings of affected children enrolled in their study [
2]. In our study, a pathological eruption occurred in two siblings too.
No analysis regarding the association between ectopic eruption and other dental anomalies was performed in this paper. Becktor et al. postulated that irreversible ectopic eruption could be an early indicator of a canine eruption leading to lateral root resorption [
15]. It would be interesting to explore this association in further studies.
Despite the study group showing a statistically significantly greater Go-Pg distance than the control group, the present investigation does not seem to corroborate a Class III developmental tendency in subjects with ectopic eruption [
13,
16], as demonstrated by
ANB mean values. However, the study group showed a negative mean value of Wits parameter compared to the positive value founded in controls. Such variable difference among groups was not statistically significant.
Early diagnosis of ectopic molar eruption is of great clinical importance since an appropriate treatment is needed in the majority of cases. Data from literature recommends an interceptive treatment after an observation period lasting from 3 to 6 months, if the deciduous tooth resorption is not too severe. Conversely, treatment is mandatory if an irreversible ectopic eruption is diagnosed [
7].
Several orthodontic procedures have been previously proposed [
8,
17]. The majority of our cases were treated using a rapid palatal expander, cemented to the second deciduous molars and modified with a Halterman spring [
18], soldered to the band on the side of the ectopic eruption. An elastic chain was placed from the hook to a bonded button on the occlusal surface of the ectopically erupting permanent molar, as shown in
Figure 2 The use of a palatal expander was justified by a clinically evaluated maxillo-mandibular discrepancy in the posterior-transverse diameter, as already reported in the literature [
17].
No distinction between reversible and irreversible forms of ectopic eruption was made in this study. Moreover, the limitations of the study were related to the sample selection and the small number of subjects included could have influenced the reported results.
5. Conclusions
Ectopic eruption of the maxillary permanent first molar would seem associated with morphogenetic characteristics of patients, especially a dolico-cephalic pattern. The association between ectopic eruption and smaller/retro-positioned maxilla was not confirmed by the outcomes of the current study.
Author Contributions
Conceptualization, D.D.V., A.L., M.C.; methodology, P.L., S.C.; validation, A.L.; investigation, P.L., S.C.; data curation, M.C.; writing—original draft preparation, A.L., D.D.V., S.C.; writing—review and editing, S.C.; supervision, D.D.V., A.L., M.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Bjerklin, K.; Kurol, J. Ectopic eruption of the maxillary first permanent molar: Etiologic factors. Am. J. Orthod. 1983, 84, 147–155. [Google Scholar] [CrossRef]
- Kurol, J.; Bjerklin, K. Ectopic eruption of maxillary first permanent molar: A review. ASDC J. Dent. Child. 1986, 53, 209–214. [Google Scholar] [PubMed]
- Mooney, G.C.; Morgan, A.G.; Rodd, H.D.; North, S. Ectopic eruption of first permanent molars: Presenting features and associations. Eur. Arch. Paediatr. Dent. 2007, 8, 153–157. [Google Scholar] [CrossRef] [PubMed]
- Lee, R.Y.; Artun, J.; Alonzo, T.A. Are dental anomalies risk factors for apical root resorption in orthodontic patients? Am. J. Orthod. Dentofac. Orthop. 1999, 116, 187–195. [Google Scholar] [CrossRef]
- Canut, J.A.; Raga, C. Morphological analysis of cases with ectopic eruption of the maxillary first permanent molar. Eur. J. Orthod. 1983, 5, 249–253. [Google Scholar] [CrossRef] [PubMed]
- Young, D.H. Ectopic eruption of the first permanent molar. J. Dent. Child. 1967, 24, 153–162. [Google Scholar]
- Dabbagh, B.; Sigal, M.J.; Tompson, B.D.; Titley, K.; Andrews, P. Ectopic Eruption of the Permanent Maxillary First Molar: Predictive Factors for Irreversible Outcome. Pediatric Dent. 2017, 39, 215–218. [Google Scholar]
- Kupietzky, A. Correction of ectopic eruption of permanent molars utilizing the brass wire technique. Pediatric Dent. 2000, 22, 408–412. [Google Scholar]
- Chintakanon, K.; Boonpinon, P. Ectopic eruption of the first permanent molars: Prevalence and etiologic factors. Angle Orthod. 1998, 68, 153–160. [Google Scholar] [PubMed]
- Pulver, F. The etiology and prevalence of ectopic eruption of the maxillary first permanent molar. ASDC J. Dent. Child. 1968, 35, 138–146. [Google Scholar] [PubMed]
- Bjerklin, K.; Kurol, J.; Paulin, G. Ectopic eruption of the maxillary first permanent molars in children with cleft lip and/or palate. Eur. J. Orthod. 1993, 15, 535–540. [Google Scholar]
- Barberia-Leache, E.; Suarez-Clúa, M.C.; Saavedra-Ontiveros, D. Ectopic eruption of the maxillary first permanent molar: Characteristics and occurrence in growing children. Angle Orthod. 2005, 75, 610–615. [Google Scholar] [PubMed]
- Hwang, S.; Choi, Y.J.; Lee, J.Y.; Chung, C.; Kim, K.-H. Ectopic eruption of the maxillary second molar: Predictive factors. Angle Orthod. 2017, 87, 583–589. [Google Scholar] [CrossRef] [PubMed]
- Frazier-Bowers, S.A.; Puranik, C.P.; Mahaney, M.C. The etiology of eruption disorder-Further evidence of a “Genetic paradigm”. Semin. Orthod. 2010, 16, 180–185. [Google Scholar] [CrossRef] [PubMed]
- Becktor, K.B.; Steiniche, K.; Kjaer, I. Association between ectopic eruption of maxillary canines and first molars. Eur. J. Orthod. 2005, 27, 186–189. [Google Scholar] [CrossRef] [PubMed]
- Salbach, A.; Schremmer, B.; Grabowski, R.; Stahl de Castrillon, F. Correlation between the frequency of eruption disorders for first permanent molars and the occurrence of malocclusions in early mixed dentition. J. Orofac. Orthop. 2012, 73, 298–306. [Google Scholar] [CrossRef] [PubMed]
- Ambriss, B.; Moukarzel, C.; Noueiri, B. Management of bilateral ectopically erupting maxillary molars: A case report. Int. J. Clin. Pediatr. Dent. 2019, 12, 153–156. [Google Scholar] [PubMed]
- Halterman, C.W. A simple technique for the treatment of ectopically erupting permanent first molars. JADA 1982, 105, 1031–1033. [Google Scholar] [CrossRef] [PubMed][Green Version]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, 




{kind=link}
{kind=link}