
Multi-Organ Protective Effects of Curcumin Nanoparticles on Drug-Induced Acute Myocardial Infarction in Rats with Type 1 Diabetes Mellitus

 ,
, 


 ,
,  , , , and
, , , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethics Statement
2.2. Animals
2.3. Chemicals and Reagents
2.4. Diabetes Mellitus Induction
2.5. Acute Myocardial Infarction Induction
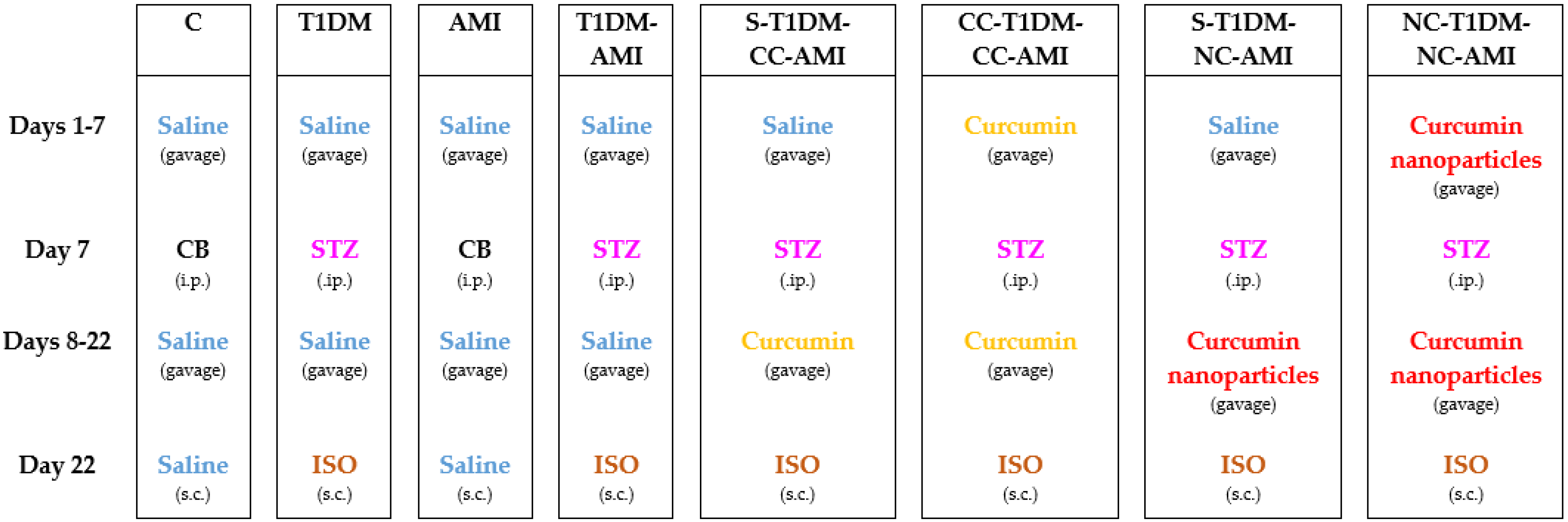
2.6. Study Groups
2.7. Electrocardiographic Monitoring
2.8. Biochemical Analysis
2.9. Histopathological Examination
2.10. Statistical Analysis
3. Results
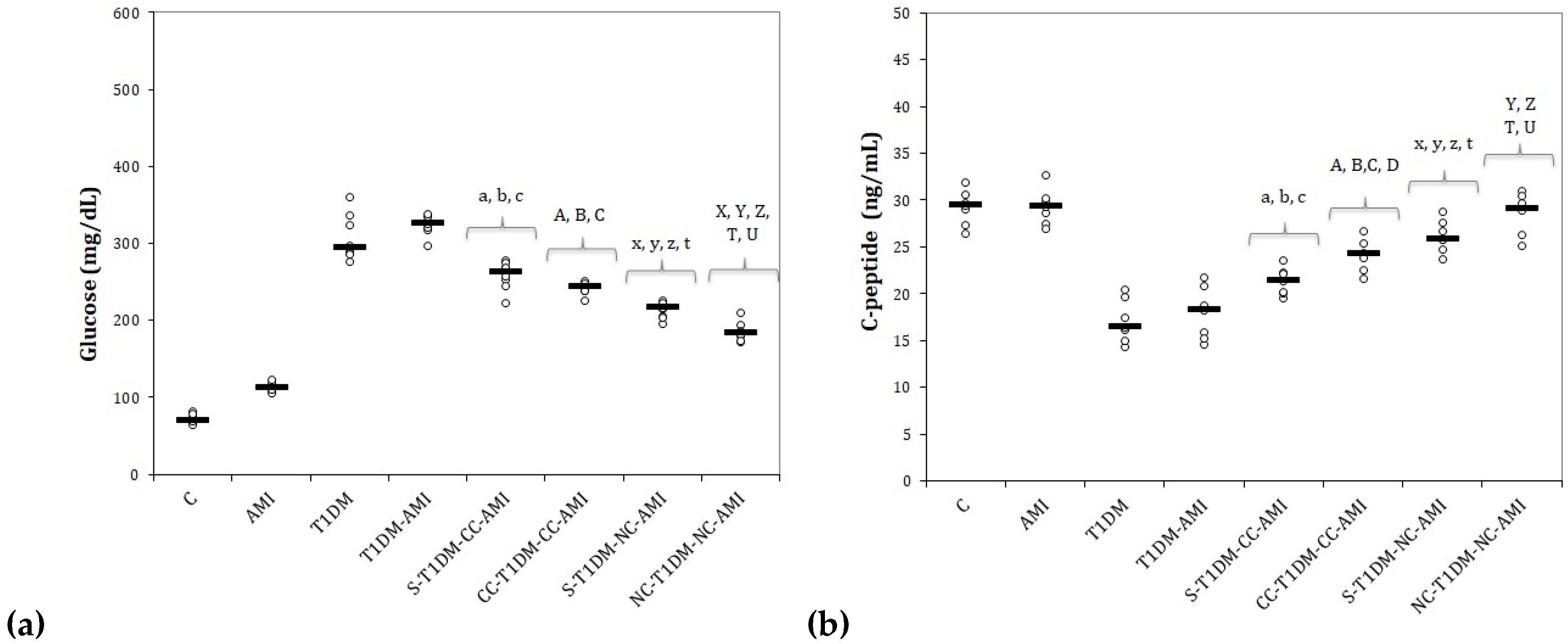
3.1. Serum Levels of Glucose and C-Peptide
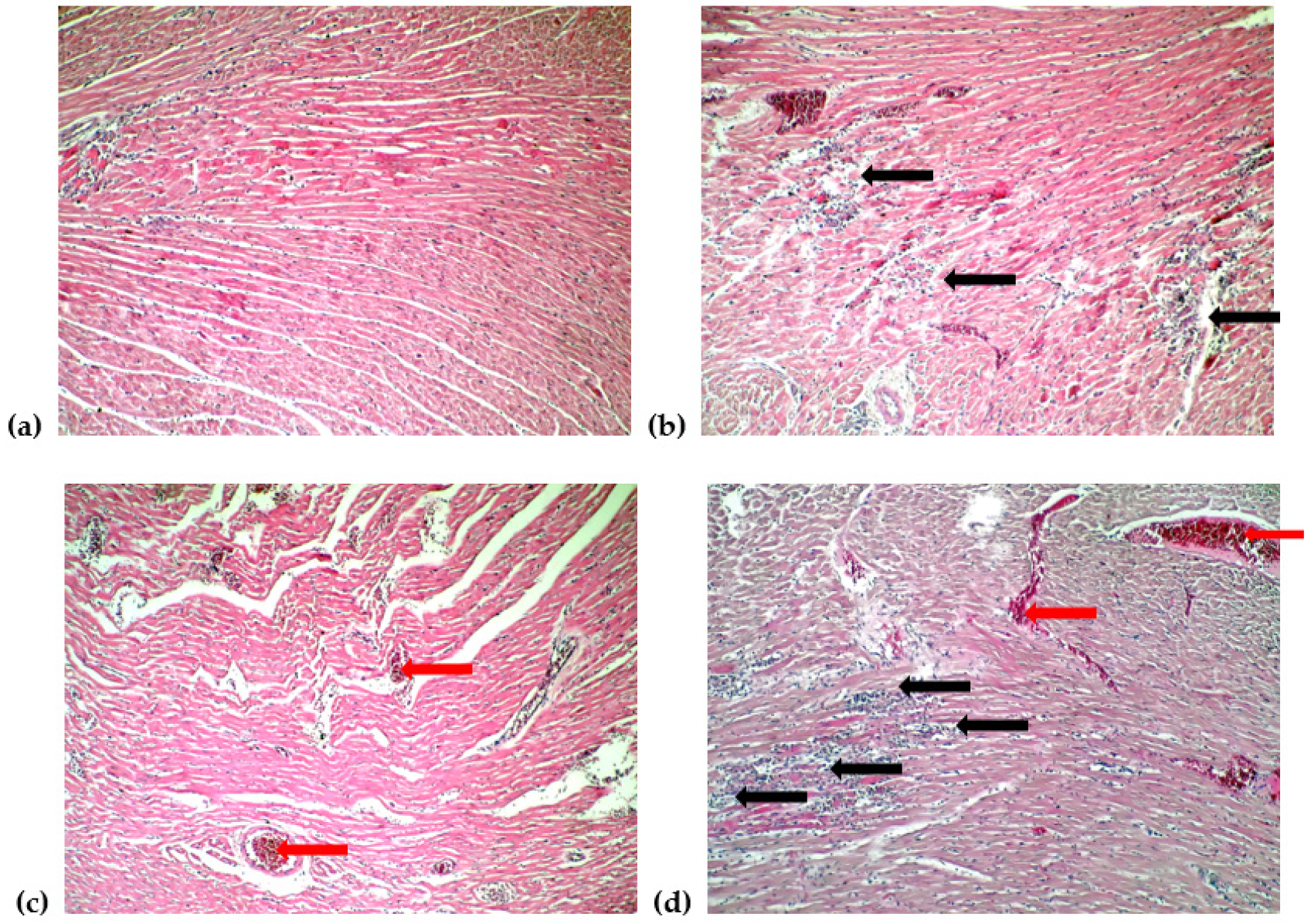
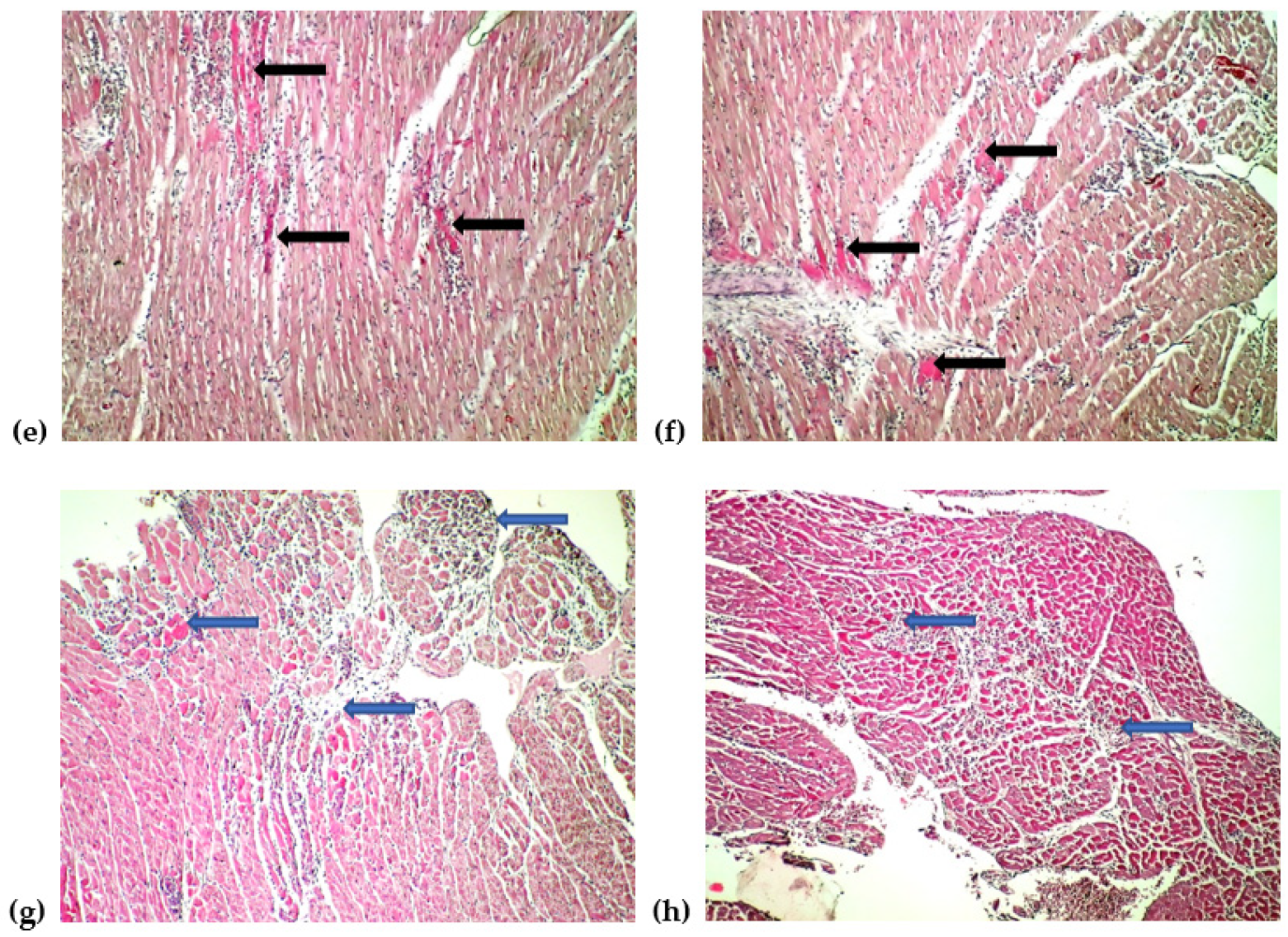
3.2. Electrocardiogram Monitoring and Histological Changes of the Heart
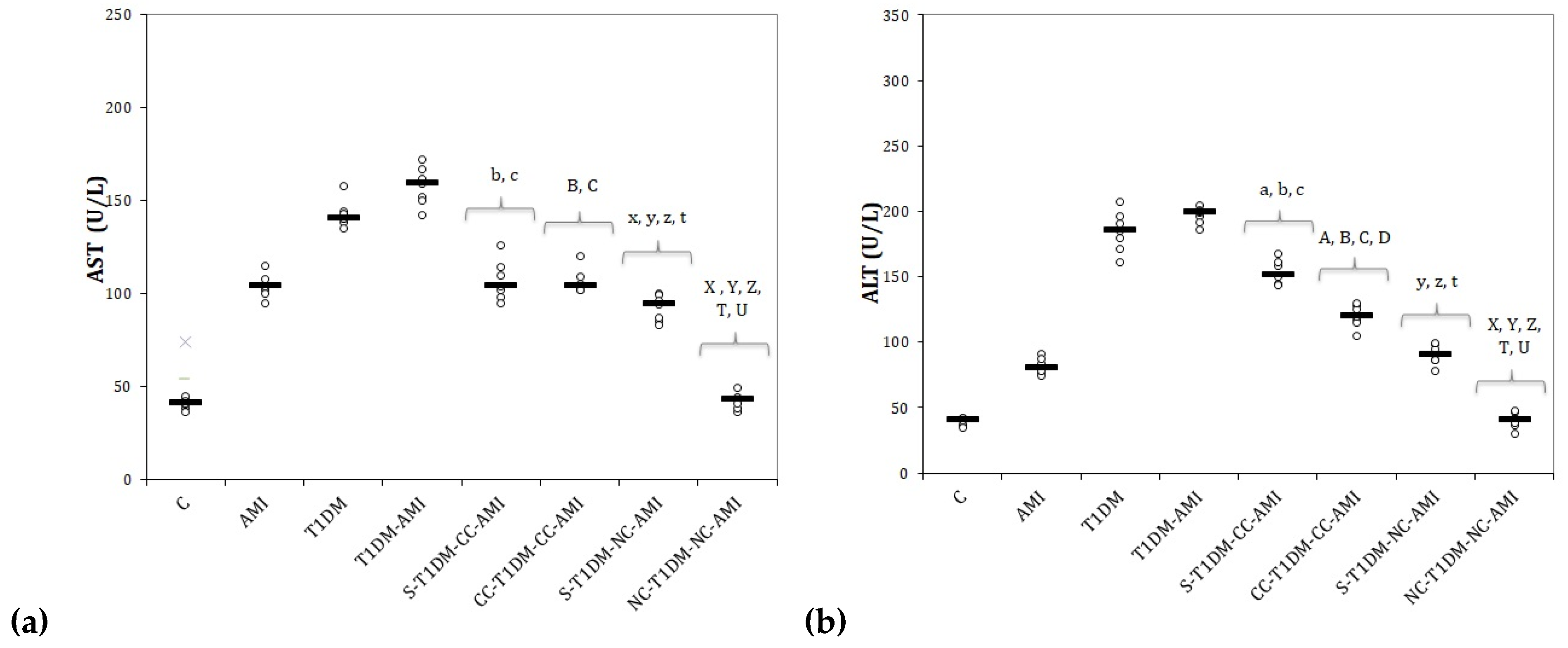
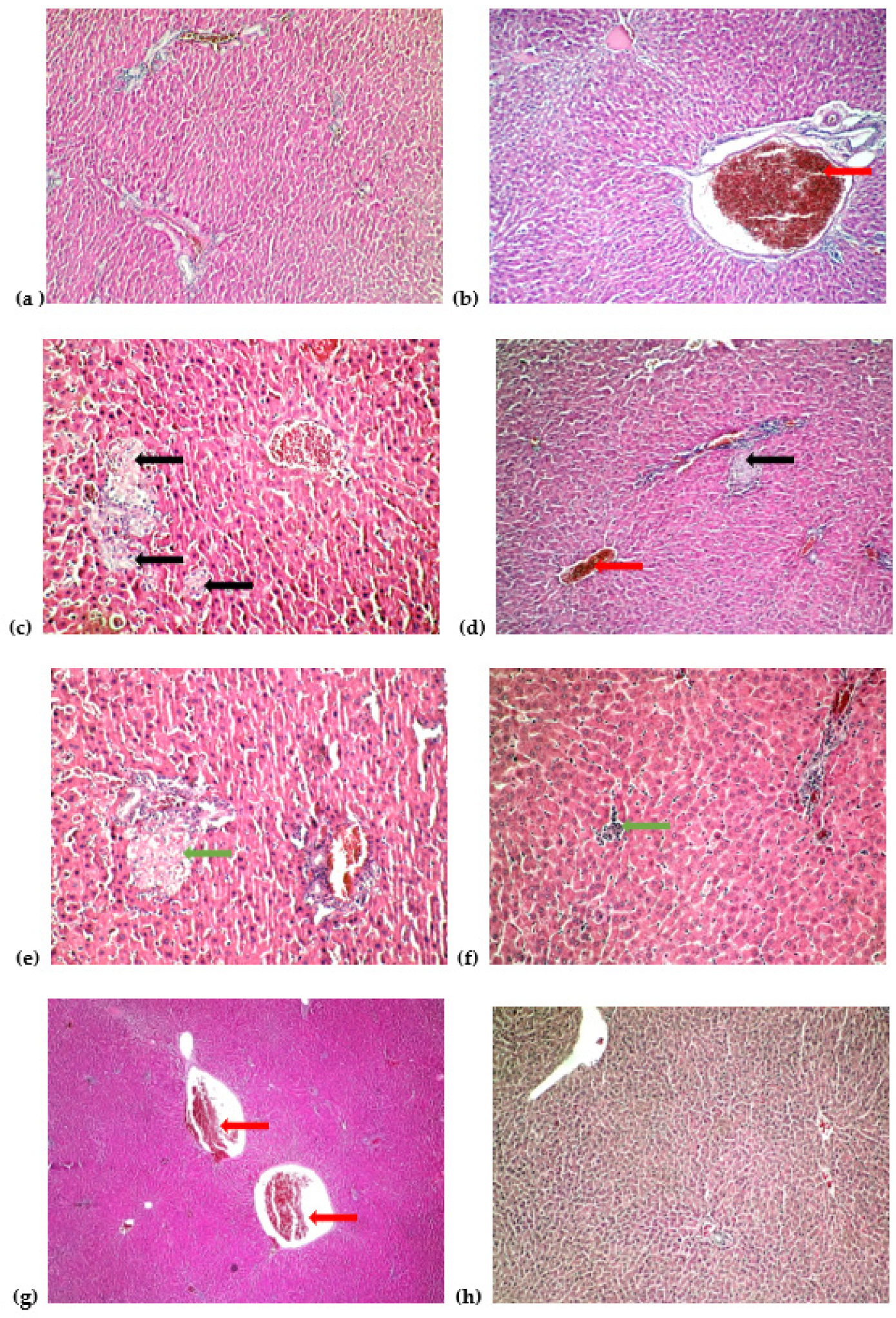
3.3. Serum Levels of Liver Function Parameters and Liver Histopathological Changes
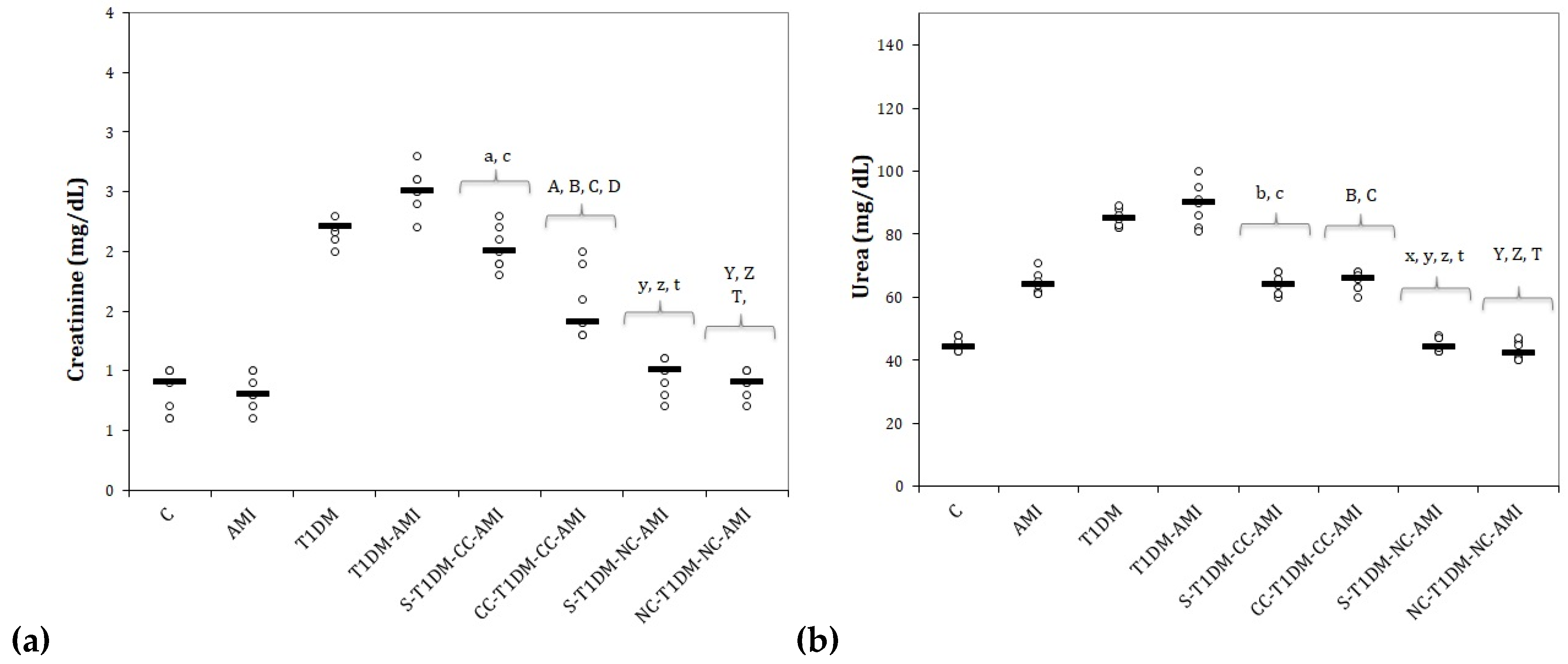
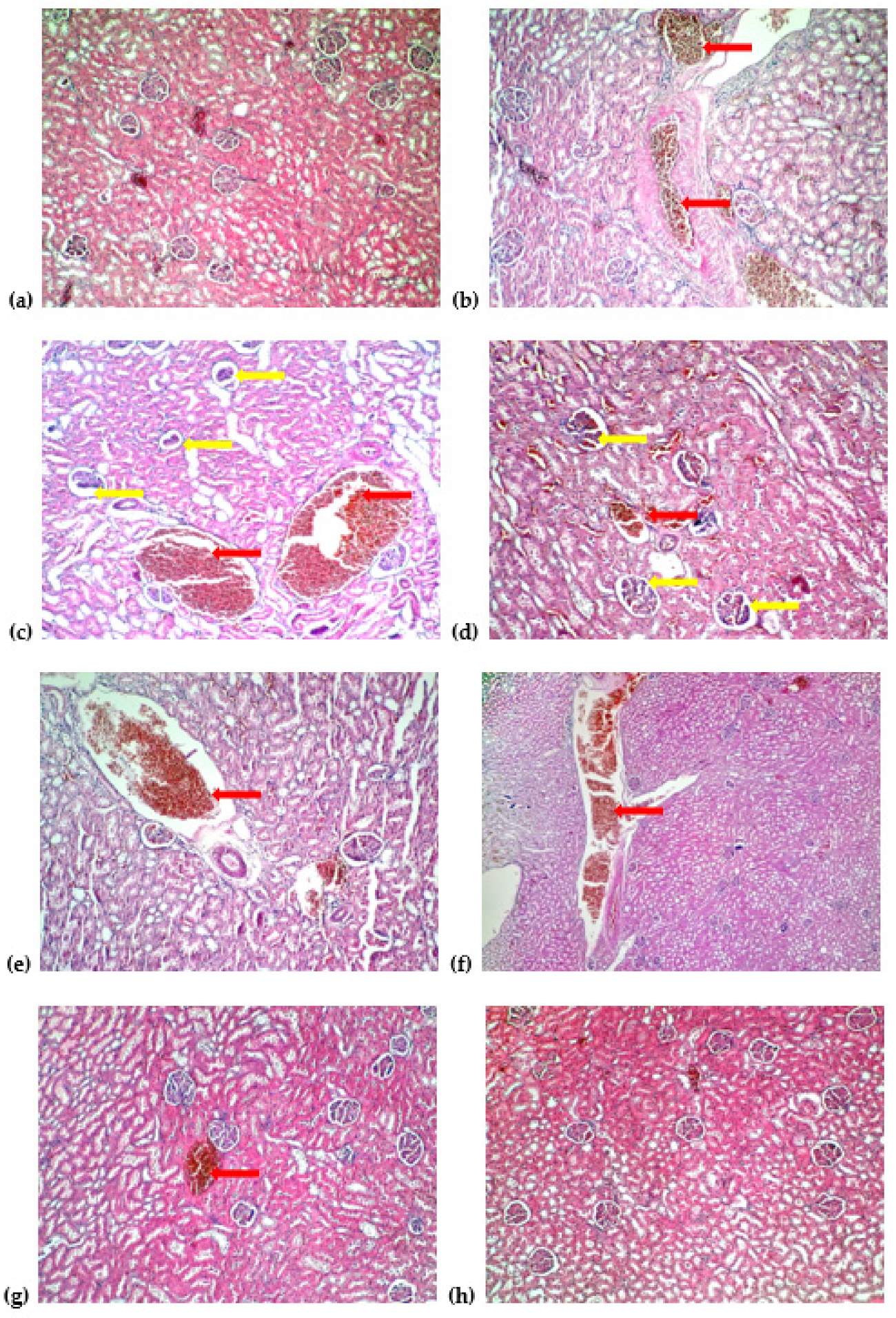
3.4. Serum Levels of Kidney Function Parameters and Kidney Histopathological Changes
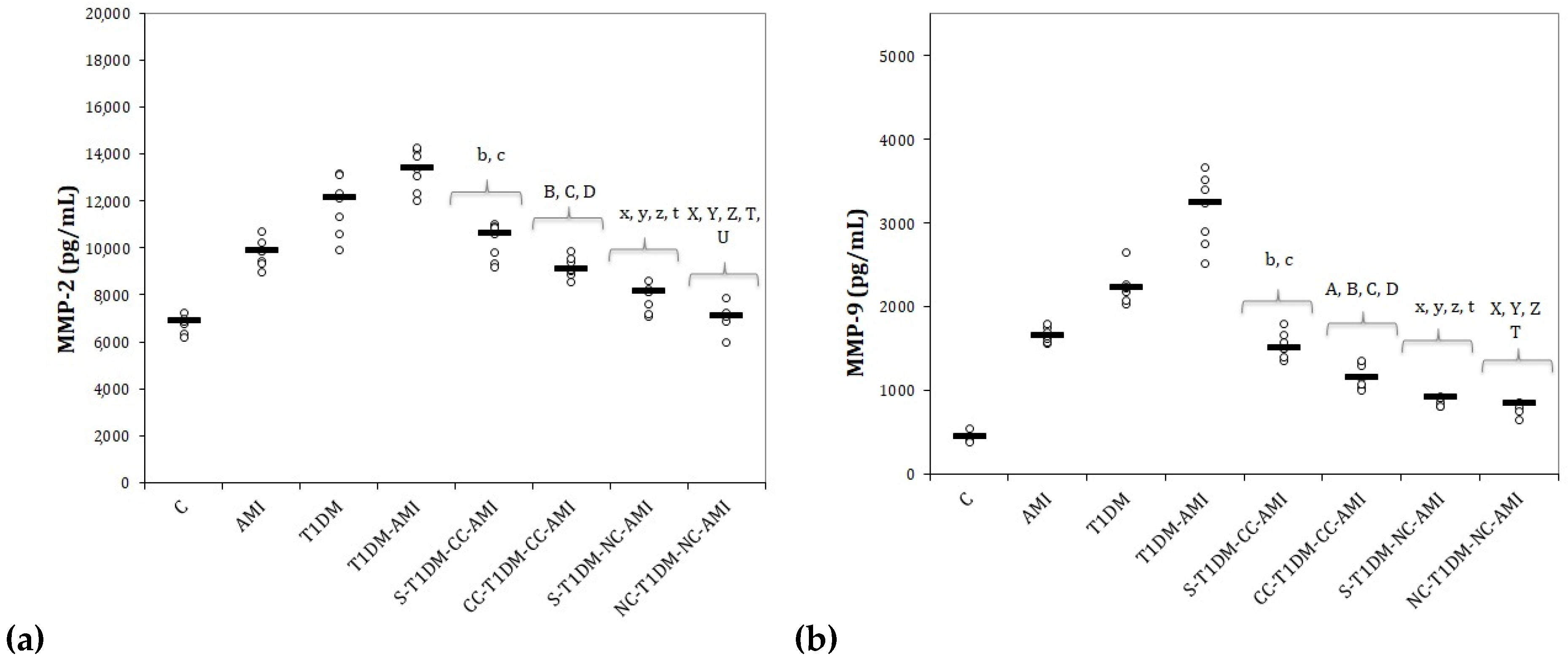
3.5. Serum Levels of Matrix Metalloproteinases
4. Discussion
4.1. Serum Levels of Glucose and C-Peptide
4.2. Electrocardiogram Monitoring and Histological Changes of the Heart
4.3. Serum Levels of Liver Function Parameters and Liver Histopathological Changes
4.4. Serum Levels of Kidney Function and Kidney Histopathological Changes
4.5. Serum Levels of Matrix Metalloproteinases
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Allender, S.; Scarborough, P.; Peto, V.; Rayner, M. European Cardiovascular Disease Statistics 2008; British Heart Foundation: London, UK, 2008. [Google Scholar]
- Luo, M.; Guan, X.; Luczak, E.D.; Lang, D.; Kutschke, W.; Gao, Z.; Yang, J.; Glynn, P.; Sossalla, S.; Swaminathan, P.D.; et al. Diabetes increases mortality after myocardial infarction by oxidizing CaMKII. J. Clin. Investig. 2013, 123, 1262–1274. [Google Scholar] [CrossRef] [PubMed]
- Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes. 2019. Available online: https://care.diabetesjournals.org/content/diacare/42/Supplement_1/S13.full.pdf (accessed on 21 March 2021).
- King, A.J.F. The use of animal models in diabetes research. Br. J. Pharmacol. 2012, 166, 877–894. [Google Scholar] [CrossRef] [PubMed]
- Szkudelski, T. The mechanism of alloxan and streptozotocin action in B cells of the rat pancreas. Physiol. Res. 2001, 50, 537–546. [Google Scholar]
- Rona, G. Catecholamine cardiotoxicity. J. Mol. Cell. Cardiol. 1985, 17, 291–306. [Google Scholar] [CrossRef]
- Abd Halim, S.A.S.; Ghafar, N.A.; Jubri, Z.; Das, S. Induction of myocardial infarction in experimental animals: A review. J. Clin. Diagn. Res. 2018, 12, 1–5. [Google Scholar] [CrossRef]
- Upaganlawar, A.; Gandhi, H.; Balaraman, R. Isoproterenol induced myocardial infarction: Protective role of natural products. J. Pharmacol. Toxicol. 2011, 6, 1–17. [Google Scholar] [CrossRef]
- Mirzaei, H.; Shakeri, A.; Rashidi, B.; Jalili, A.; Banikazemi, Z.; Sahebkar, A. Phytosomal curcumin: A review of pharmacokinetic, experimental and clinical studies. Biomed. Pharmacother. 2017, 85, 102–112. [Google Scholar] [CrossRef]
- Noorafshan, A.; Ashkani-Esfahani, S. A Review of Therapeutic Effects of Curcumin. Curr. Pharm. Des. 2013, 19, 2032–2046. [Google Scholar] [CrossRef]
- Nelson, K.M.; Dahlin, J.L.; Bisson, J.; Graham, J.; Pauli, G.F.; Walters, M.A. The Essential Medicinal Chemistry of Curcumin. J. Med. Chem. 2017, 60, 1620–1637. [Google Scholar] [CrossRef]
- Shang, L.; Nienhaus, K.; Nienhaus, G.U. Engineered nanoparticles interacting with cells: Size matters. J. Nanobiotechnology 2014, 12, 5. [Google Scholar] [CrossRef]
- Hu, L.; Jia, Y.; Niu, F.; Jia, Z.; Yang, X.; Jiao, K. Preparation and Enhancement of Oral Bioavailability of Curcumin Using Microemulsions Vehicle. J. Agric. Food Chem. 2012, 60, 7137–7141. [Google Scholar] [CrossRef]
- Panda, S.P.; Haldar, P.K.; Bera, S.; Adhikary, S.; Kandar, C.C. Antidiabetic and antioxidant activity of Swietenia mahagoni in streptozotocin-induced diabetic rats. Pharm. Biol. 2010, 48, 974–979. [Google Scholar] [CrossRef]
- Bhandari, U.; Ansari, M.N. Ameliorative effect of an ethanol extract of Embelia ribes fruits on isoproterenol-induced cardiotoxicity in diabetic rats. Pharm. Biol. 2009, 47, 669–674. [Google Scholar] [CrossRef][Green Version]
- Boarescu, P.-M.; Boarescu, I.; Bocșan, I.C.; Gheban, D.; Bulboacă, A.E.; Nicula, C.; Pop, R.M.; Râjnoveanu, R.-M.; Bolboacă, S.D. Antioxidant and Anti-Inflammatory Effects of Curcumin Nanoparticles on Drug-Induced Acute Myocardial Infarction in Diabetic Rats. Antioxidants 2019, 8, 504. [Google Scholar] [CrossRef]
- Dogaru, G.; Bulboaca, A.; Stanescu, I.; Rus, V.; Gyorgy, B.; Ciumarnean, L.; Munteanu, C.; Boarescu, P.M.; Neagos, A.; Festila, D. The effect of carbonated natural mineral water on oxidative stress in experimental myocardial ischemia. Rev. Chim. 2019, 70, 2677–2680. [Google Scholar] [CrossRef]
- Konopelski, P.; Ufnal, M. Electrocardiography in rats: A comparison to human. Physiol. Res. 2016, 65, 717–725. [Google Scholar] [CrossRef]
- Weissgerber, T.L.; Milic, N.M.; Winham, S.J.; Garovic, V.D. Beyond bar and line graphs: Time for a new data presentation paradigm. PLoS Biol. 2015, 13, e1002128. [Google Scholar] [CrossRef]
- Ishihara, M. Acute hyperglycemia in patients with acute myocardial infarction. Circ. J. 2012, 76, 563–571. [Google Scholar] [CrossRef]
- Ceriello, A. Acute hyperglycaemia, a ‘new’ risk factor during myocardial infarction. Eur. Heart J. 2004, 26, 328–331. [Google Scholar] [CrossRef] [PubMed]
- Leighton, E.; Sainsbury, C.A.; Jones, G.C. A practical review of C-peptide testing in diabetes. Diabetes Ther. 2017, 8, 475–487. [Google Scholar] [CrossRef]
- Wahren, J.; Kallas, A.; Sima, A.A.F. The Clinical Potential of C-Peptide Replacement in Type 1 Diabetes. Diabetes 2012, 61, 761–772. [Google Scholar] [CrossRef] [PubMed]
- Kusari, J.; Zhou, S.X.; Padillo, E.; Clarke, K.G.; Gil, D.W. Inhibition of vitreoretinal VEGF elevation and blood–retinal barrier breakdown in streptozotocin-induced diabetic rats by brimonidine. Investig. Ophthalmol. Vis. Sci. 2010, 51, 1044–1051. [Google Scholar] [CrossRef] [PubMed]
- Wickenberg, J.; Ingemansson, S.L.; Hlebowicz, J. Effects of Curcuma longa (turmeric) on postprandial plasma glucose and insulin in healthy subjects. Nutr. J. 2010, 9, 43. [Google Scholar] [CrossRef]
- Ganugula, R.; Arora, M.; Jaisamut, P.; Wiwattanapatapee, R.; Jørgensen, H.G.; Venkatpurwar, V.P.; Zhou, B.; Hoffmann, A.R.; Basu, R.; Guo, S.; et al. Nano-curcumin safely prevents streptozotocin-induced inflammation and apoptosis in pancreatic beta cells for effective management of Type 1 diabetes mellitus. Br. J. Pharmacol. 2017, 174, 2074–2084. [Google Scholar] [CrossRef]
- Fang, M.; Jin, Y.; Bao, W.; Gao, H.; Xu, M.; Wang, D.; Wang, X.; Yao, P.; Liu, L. In vitro characterization and in vivo evaluation of nanostructured lipid curcumin carriers for intragastric administration. Int. J. Nanomed. 2012, 7, 5395–5404. [Google Scholar] [CrossRef]
- Choi, K.M.; Zhong, Y.; Hoit, B.D.; Grupp, I.L.; Hahn, H.; Dilly, K.W.; Guatimosim, S.; Lederer, W.J.; Matlib, M.A. Defective intracellular Ca2+ signaling contributes to cardiomyopathy in Type 1 diabetic rats. Am. J. Physiol. Heart Circ. Physiol. 2002, 283, H1398–H1408. [Google Scholar] [CrossRef]
- Howarth, F.C.; Jacobson, M.; Shafiullah, M.; Adeghate, E. Long-term effects of streptozotocin-induced diabetes on the electrocardiogram, physical activity and body temperature in rats. Exp. Physiol. 2005, 90, 827–835. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Parratt, J.R.; Beastall, G.H.; Pyne, N.J.; Furman, B.L. Streptozotocin diabetes protects against arrhythmiasin rat isolated hearts: Role of hypothyroidism. Eur. J. Pharmacol. 2002, 435, 269–276. [Google Scholar] [CrossRef]
- Veglio, M.; Chinaglia, A.; Cavallo-Perin, P. QT interval, cardiovascular risk factors and risk of death in diabetes. J. Endocrinol. Investig. 2004, 27, 175–181. [Google Scholar] [CrossRef]
- Balea, Ş.S.; Pârvu, A.E.; Pop, N.; Marín, F.Z.; Pârvu, M. Polyphenolic Compounds; Antioxidant; and Cardioprotective Effects of Pomace Extracts from Fetească Neagră Cultivar. Oxid. Med. Cell. Longev. 2018, 2018, 8194721. [Google Scholar] [CrossRef] [PubMed]
- Králová, E.; Mokran, T.; Murin, J.; Stankovicova, T. Electrocardiography in two models of isoproterenol-induced left ventricular remodeling. Physiol. Res. 2008, 57, S83–S89. [Google Scholar]
- Soraya, H.; Khorrami, A.; Garjani, A.; Maleki-Dizaji, N.; Garjani, A. Acute treatment with metformin improves cardiac function following isoproterenol induced myocardial infarction in rats. Pharmacol. Rep. 2012, 64, 1476–1484. [Google Scholar] [CrossRef]
- Boarescu, P.-M.; Boarescu, I.; Bocșan, I.C.; Pop, R.M.; Gheban, D.; Bulboacă, A.E.; Nicula, C.; Râjnoveanu, R.-M.; Bolboacă, S.D. Curcumin Nanoparticles Protect against Isoproterenol Induced Myocardial Infarction by Alleviating Myocardial Tissue Oxidative Stress, Electrocardiogram, and Biological Changes. Molecules 2019, 24, 2802. [Google Scholar] [CrossRef]
- Nirmala, C.; Puvanakrishnan, R. Protective role of curcumin against isoproterenol induced myocardial infarction in rats. Mol. Cell. Biochem. 1996, 159, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Boarescu, P.M.; Chirilă, I.; Bulboacă, A.E.; Bocșan, I.C.; Pop, R.M.; Gheban, D.; Bolboacă, S.D. Effects of curcumin nanoparticles in isoproterenol-induced myocardial infarction. Oxid. Med. Cell. Longev. 2019, 2019, 7847142. [Google Scholar] [CrossRef]
- Ranjan, A.P.; Mukerjee, A.; Helson, L.; Vishwanatha, J.K. Mitigating prolonged QT interval in canCer nanodrug development for accelerated clinical translation. J. Nanobiotechnol. 2013, 11, 40. [Google Scholar] [CrossRef]
- Helson, L.; Shopp, G.; Bouchard, A.; Majeed, M. Liposome mitigation of curcumin inhibition of cardiac potassium delayed-rectifier current. J. Recept. Ligand Channel Res. 2012, 11, 1–8. [Google Scholar] [CrossRef][Green Version]
- Dogaru, G.; Bulboaca, A.E.; Gheban, D.; Boarescu, P.M.; Rus, V.; Festila, D.; Sitar-Taut, A.V.; Stanescu, I. Effect of liposomal curcumin on acetaminophen hepatotoxicity by down-regulation of oxidative stress and matrix metalloproteinases. In Vivo 2020, 34, 569–582. [Google Scholar] [CrossRef]
- GezginCi-Oktayoglu, S.; Basaraner, H.; Yanardag, R.; Bolkent, S. The effects of combined treatment of antioxidants on the liver injury in STZ diabetic rats. Dig. Dis. Sci. 2009, 54, 538–546. [Google Scholar] [CrossRef] [PubMed]
- Filho, H.G.L.; Ferreira, N.L.; De Sousa, R.B.; De Carvalho, E.R.; Lobo, P.L.D.; Filho, J.G.L. Experimental model of myocardial infarction induced by isoproterenol in rats. Braz. J. Cardiovasc. Surg. 2011, 26, 469–476. [Google Scholar] [CrossRef]
- Buonomo, A.R.; Scotto, R.; Nappa, S.; Arcopinto, M.; Salzano, A.; Marra, A.M.; D’Assante, R.; Zappulo, E.; Borgia, G.; Gentile, I. The role of curcumin in liver diseases. Arch. Med. Sci. 2019, 15, 1608–1620. [Google Scholar] [CrossRef] [PubMed]
- Trujillo, J.; Chirino, Y.I.; Molina-Jijón, E.; Andérica-Romero, A.C.; Tapia, E.; Pedraza-Chaverrí, J. Renoprotective effect of the antioxidant curcumin: Recent findings. Redox Biol. 2013, 1, 448–456. [Google Scholar] [CrossRef] [PubMed]
- Lewandowski, K.C.; Banach, E.; Bieńkiewicz, M.; Lewiński, A. Matrix metalloproteinases in type 2 diabetes and non-diabetic controls: Effects of short-term and chronic hyperglycaemia. Arch. Med. Sci. 2011, 7, 294–303. [Google Scholar] [CrossRef] [PubMed]
- Thompson, M.M.; Squire, I.B. Matrix metalloproteinase-9 expression after myocardial infarction: Physiological or pathological? Cardiovasc. Res. 2002, 54, 495–498. [Google Scholar] [CrossRef]
- Sawicki, G.; Leon, H.; Sawicka, J.; Sariahmetoglu, M.; Schulze, C.J.; Scott, P.G.; Szczesna-Cordary, D.; Schulz, R. Degradation of myosin light chain in isolated rat hearts subjected to ischemia-reperfusion injury: A new intracellular target for matrix metalloproteinase. Circulation 2005, 112, 544–552. [Google Scholar] [CrossRef]
- Yabluchanskiy, A.; Ma, Y.; Iyer, R.P.; Hall, M.E.; Lindsey, M.L. Matrix metalloproteinase-9: Many shades of function in cardiovascular disease. Physiology 2013, 28, 391–403. [Google Scholar] [CrossRef] [PubMed]
- Kowluru, R.A.; Mohammad, G.; Dos Santos, J.M.; Zhong, Q. Abrogation of MMP-9 gene protects against the development of retinopathy in diabetic mice by preventing mitochondrial damage. Diabetes 2011, 60, 3023–3033. [Google Scholar] [CrossRef] [PubMed]
- Fouad, M.; Boraie, M. Matrix metalloproteinase-2 as potential marker of early nephropathy in type 1 diabetes. Am. J. Intern. Med. 2015, 3, 1–5. [Google Scholar] [CrossRef]
- Uemura, S.; Matsushita, H.; Li, W.; Glassford, A.J.; Asagami, T.; Lee, K.H.; Harrison, D.G.; Tsao, P.S. Diabetes mellitus enhances vascular matrix metalloproteinase activity: Role of oxidative stress. Circ. Res. 2001, 88, 1291–1298. [Google Scholar] [CrossRef]
- Signorelli, S.S.; Malaponte, G.; Libra, M.; Di Pino, L.; Celotta, G.; Bevelacqua, V.; Petrina, M.; Nicotra, G.S.; Indelicato, M.; Navolanic, P.M.; et al. Plasma levels and zymographic activities of matrix metalloproteinases 2 and 9 in type II diabetics with peripheral arterial disease. Vasc. Med. 2005, 10, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Hayashidani, S.; Tsutsui, H.; Ikeuchi, M.; Shiomi, T.; Matsusaka, H.; Kubota, T.; Imanaka-Yoshida, K.; Itoh, T.; Takeshita, A. Targeted deletion of MMP-2 attenuates early LV rupture and late remodeling after experimental myocardial infarction. Am. J. Physiol. Heart Circ. Physiol. 2003, 285, H1229–H1235. [Google Scholar] [CrossRef] [PubMed]
- Ducharme, A.; Frantz, S.; Aikawa, M.; Rabkin, E.; Lindsey, M.; Rohde, L.E.; Schoen, F.J.; Kelly, R.A.; Werb, Z.; Libby, P.; et al. Targeted deletion of matrix metalloproteinase-9 attenuates left ventricular enlargement and collagen accumulation after experimental myocardial infarction. J. Clin. Invest. 2000, 106, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Wang, N.P.; Wang, Z.F.; Tootle, S.; Philip, T.; Zhao, Z.Q. Curcumin promotes cardiac repair and ameliorates cardiac dysfunction following myocardial infarction. Br. J. Pharmacol. 2012, 167, 1550–1562. [Google Scholar] [CrossRef]
- Bulboacă, A.E.; Porfire, A.S.; Tefas, L.R.; Boarescu, P.M.; Bolboacă, S.D.; Stănescu, I.C.; Bulboacă, A.C.; Dogaru, G. Liposomal Curcumin is Better than Curcumin to Alleviate Complications in Experimental Diabetic Mellitus. Molecules 2019, 24, 846. [Google Scholar] [CrossRef] [PubMed]
- Nabofa, W.E.E.; Alashe, O.O.; Oyeyemi, O.T.; Attah, A.F.; Oyagbemi, A.A.; Omobowale, T.O.; Adedapo, A.A.; Alada, A.R.A. Cardioprotective Effects of Curcumin-Nisin Based Poly Lactic Acid Nanoparticle on Myocardial Infarction in Guinea Pigs. Sci. Rep. 2018, 8, 16649. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Abbreviation | RR(ms) | HR(b/min) | PR(ms) | QRS(ms) | QT(ms) | QTc(ms) | R(mV) | ST(mV) |
|---|---|---|---|---|---|---|---|---|
| C | 209 (7.0) | 287 (9.6) | 44 (2.1) | 35 (2.2) | 75 (4.4) | 64 (3.7) | 3 (0.11) | 0.00 (0.00) |
| AMI | 180 (3.1) | 333 (5.7) | 45 (2.2) | 53 (2.3) | 103 (3.6) | 94 (3.0) | 1.3 (0.10) | 0.09 (0.01) |
| T1DM | 239 (8.7) | 252 (9.4) | 43 (1.7) | 42 (1.3) | 85 (3.6) | 68 (2.4) | 2.1 (0.13) | 0.00 (0.00) |
| T1DM-AMI | 191 (3.0) | 314 (5.0) | 44 (2.6) | 57 (2.0) | 113 (3.0) | 100 (2.7) | 1.2 (0.08) | 0.10 (0.02) |
| S-T1DM-CC- AMI | 223 (3.6) | 269 (4.3) | 43 (1.5) | 42 (2.2) | 99 (2.5) | 81 (1.6) | 1.2 (0.13) | 0.08 (0.01) |
| CC-T1DM-CC-AMI | 226 (6.6) | 266 (7.7) | 43 (1.5) | 40 (1.3) | 94 (2.9) | 76 (3.1) | 1.4 (0.13) | 0.08 (0.02) |
| S-T1DM-NC-AMI | 249 (6.1) | 241 (5.8) | 44 (1.7) | 37 (1.7) | 88 (1.7) | 68 (1.2) | 1.7 (0.17) | 0.05 (0.01) |
| NC-T1DM-NC-AMI | 250 (3.4) | 240 (3.4) | 44 (1.4) | 37 (1.6) | 87 (2.7) | 67 (2.1) | 2.1 (0.17) | 0.02 (0.01) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boarescu, P.-M.; Boarescu, I.; Bulboacă, A.E.; Bocșan, I.C.; Pop, R.M.; Gheban, D.; Râjnoveanu, R.-M.; Râjnoveanu, A.; Roşian, Ş.H.; Buzoianu, A.D.; et al. Multi-Organ Protective Effects of Curcumin Nanoparticles on Drug-Induced Acute Myocardial Infarction in Rats with Type 1 Diabetes Mellitus. Appl. Sci. 2021, 11, 5497. https://doi.org/10.3390/app11125497
Boarescu P-M, Boarescu I, Bulboacă AE, Bocșan IC, Pop RM, Gheban D, Râjnoveanu R-M, Râjnoveanu A, Roşian ŞH, Buzoianu AD, et al. Multi-Organ Protective Effects of Curcumin Nanoparticles on Drug-Induced Acute Myocardial Infarction in Rats with Type 1 Diabetes Mellitus. Applied Sciences. 2021; 11(12):5497. https://doi.org/10.3390/app11125497
Chicago/Turabian StyleBoarescu, Paul-Mihai, Ioana Boarescu, Adriana Elena Bulboacă, Ioana Corina Bocșan, Raluca Maria Pop, Dan Gheban, Ruxandra-Mioara Râjnoveanu, Armand Râjnoveanu, Ştefan Horia Roşian, Anca Dana Buzoianu, and et al. 2021. "Multi-Organ Protective Effects of Curcumin Nanoparticles on Drug-Induced Acute Myocardial Infarction in Rats with Type 1 Diabetes Mellitus" Applied Sciences 11, no. 12: 5497. https://doi.org/10.3390/app11125497
APA StyleBoarescu, P.-M., Boarescu, I., Bulboacă, A. E., Bocșan, I. C., Pop, R. M., Gheban, D., Râjnoveanu, R.-M., Râjnoveanu, A., Roşian, Ş. H., Buzoianu, A. D., & Bolboacă, S. D. (2021). Multi-Organ Protective Effects of Curcumin Nanoparticles on Drug-Induced Acute Myocardial Infarction in Rats with Type 1 Diabetes Mellitus. Applied Sciences, 11(12), 5497. https://doi.org/10.3390/app11125497