
Laser Therapy in the Treatment of Peri-Implantitis: State-of-the-Art, Literature Review and Meta-Analysis





 and
and
Abstract
Featured Application
Abstract
1. Introduction
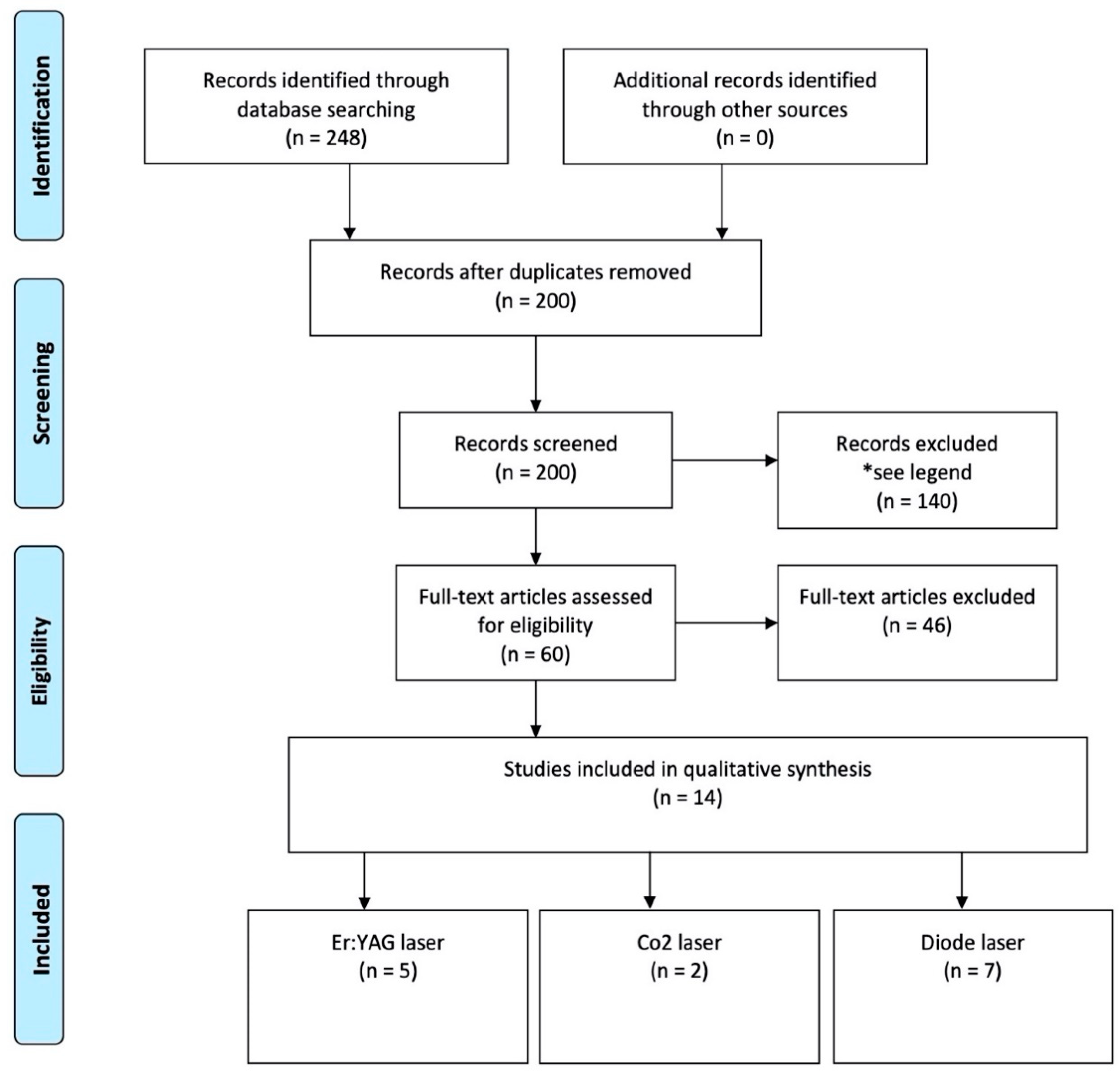
2. Materials and Methods
2.1. Eligibility Criteria
- •
- Inclusion criteria:
- o
- Population: Implants affected by mucositis and peri-implantitis in human;
- o
- Study design: Randomized-controlled trial, case-control studies, cases series with a minimum of 3 patients, meta-analysis conducted on “in vivo” studies;
- o
- Language: Papers written in English language only;
- o
- Time of publication: Paper published in the last 15 years;
- o
- Treatment: Any laser-aided treatment;
- o
- Follow-up: Studies followed by an observational period of at least 3 months.
- •
- Exclusion criteria:
- o
- Studies assessing the effectiveness of laser treatment using only radiographs;
- o
- Studies evaluating the effectiveness of lasers in peri-implantitis treatment in vitro only.
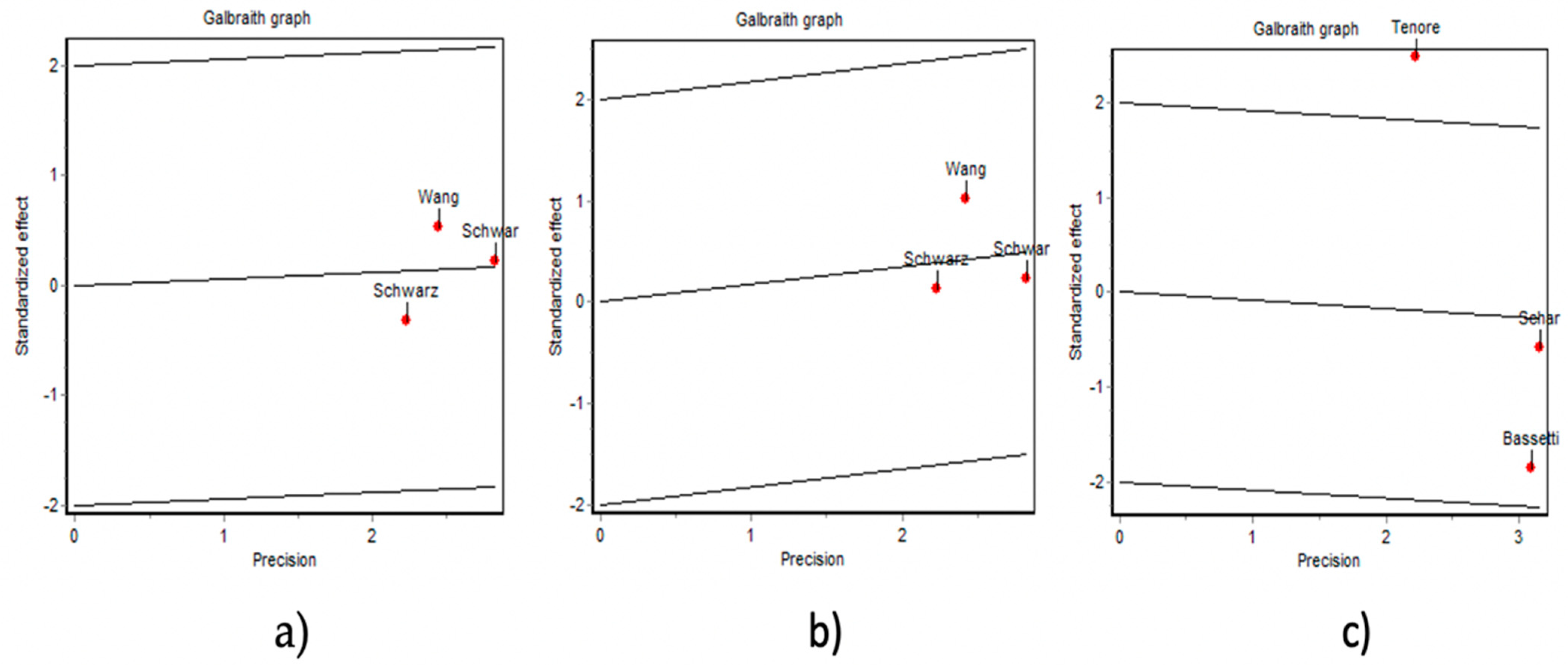
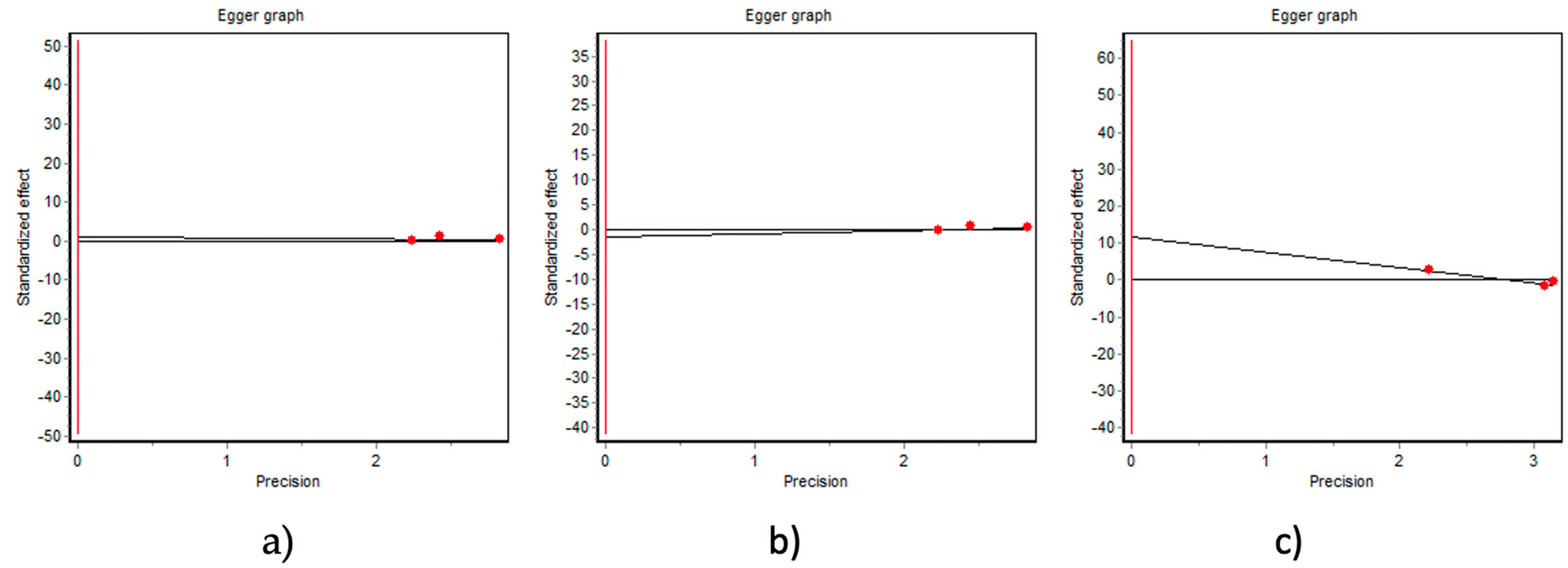
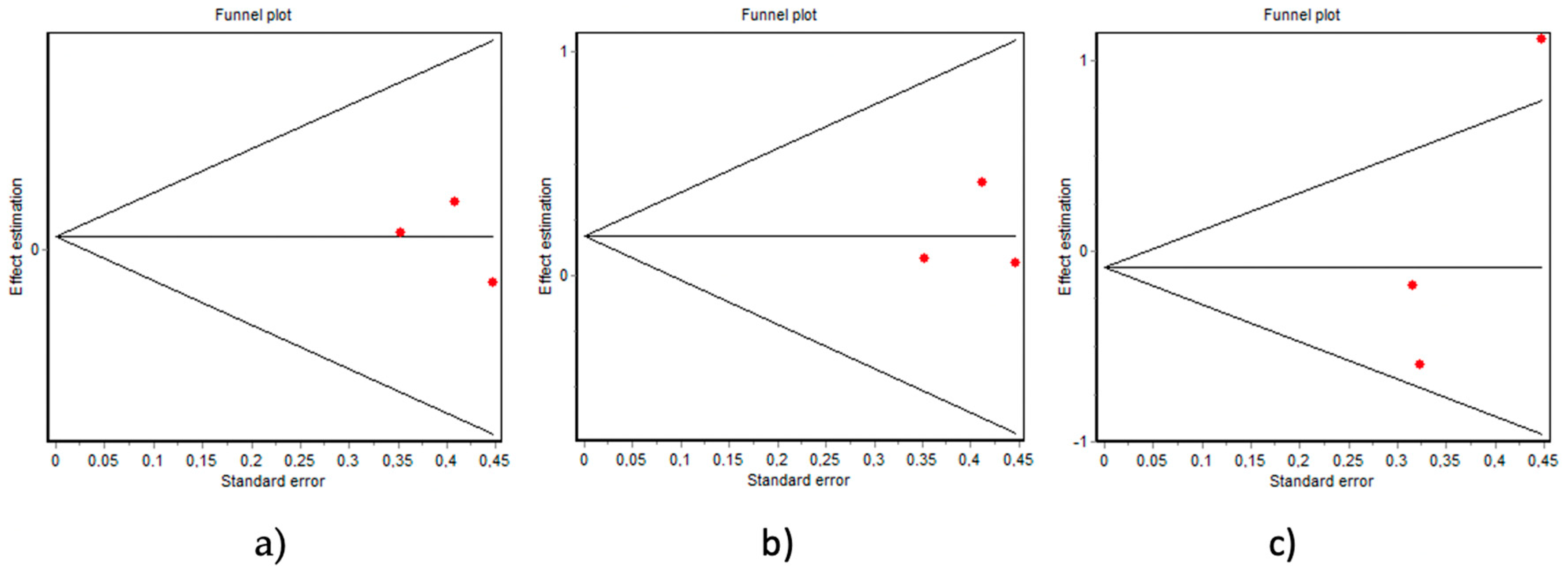
2.2. Data Analysis
3. Results
3.1. Group 1—Use of Er:YAG Laser in Peri-Implantitis Treatment (Table 1)
3.2. Group 2—Use of CO2 Laser in Peri-Implantitis Treatment (Table 2)
3.3. Group 3—Use of Diode Laser in Peri-Implantitis Treatment (Table 3)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sánchez-Gárces, M.A.; Gay-Escoda, C. Periimplantitis. Med. Oral Patol. Oral Cir. Bucal. 2004, 9, 69–74; 63–69. [Google Scholar]
- López-Cerero, L. [Dental implant-related infections]. Enferm. Infecc. Microbiol. Clin. 2008, 26, 589–592. [Google Scholar] [CrossRef] [PubMed]
- Algraffee, H.; Borumandi, F.; Cascarini, L. Peri-Implantitis. Br. J. Oral Maxillofac. Surg. 2012, 50, 689–694. [Google Scholar] [CrossRef]
- Salmeron, S.; Rezende, M.L.R.; Consolaro, A.; Sant’ana, A.C.P.; Damante, C.A.; Greghi, S.L.A.; Passanezi, E. Laser Therapy as an Effective Method for Implant Surface Decontamination: A Histomorphometric Study in Rats. J. Periodontol. 2013, 84, 641–649. [Google Scholar] [CrossRef] [PubMed]
- Lindhe, J.; Meyle, J. Group D of European Workshop on Periodontology Peri-Implant Diseases: Consensus Report of the Sixth European Workshop on Periodontology. J. Clin. Periodontol. 2008, 35, 282–285. [Google Scholar] [CrossRef]
- Renvert, S.; Hirooka, H.; Polyzois, I.; Kelekis-Cholakis, A.; Wang, H.-L. Working Group 3 Diagnosis and Non-Surgical Treatment of Peri-Implant Diseases and Maintenance Care of Patients with Dental Implants—Consensus Report of Working Group 3. Int. Dent. J. 2019, 69 (Suppl. 2), 12–17. [Google Scholar] [CrossRef] [PubMed]
- Frisch, E.; Ziebolz, D.; Ratka-Krüger, P.; Rinke, S. Double Crown-Retained Maxillary Overdentures: 5-Year Follow-Up. Clin. Implant. Dent. Relat. Res. 2015, 17, 22–31. [Google Scholar] [CrossRef] [PubMed]
- Mombelli, A.; Müller, N.; Cionca, N. The Epidemiology of Peri-Implantitis. Clin. Oral Implant. Res. 2012, 23 (Suppl. 6), 67–76. [Google Scholar] [CrossRef]
- Heitz-Mayfield, L.J.A.; Mombelli, A. The Therapy of Peri-Implantitis: A Systematic Review. Int. J. Oral Maxillofac. Implant. 2014, 29, 325–345. [Google Scholar] [CrossRef] [PubMed]
- Ashnagar, S.; Nowzari, H.; Nokhbatolfoghahaei, H.; Yaghoub Zadeh, B.; Chiniforush, N.; Choukhachi Zadeh, N. Laser Treatment of Peri-Implantitis: A Literature Review. J. Lasers Med. Sci. 2014, 5, 153–162. [Google Scholar] [PubMed]
- Tosun, E.; Tasar, F.; Strauss, R.; Kıvanc, D.G.; Ungor, C. Comparative Evaluation of Antimicrobial Effects of Er:YAG, Diode, and CO₂ Lasers on Titanium Discs: An Experimental Study. J. Oral Maxillofac. Surg. 2012, 70, 1064–1069. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, F.; Sculean, A.; Rothamel, D.; Schwenzer, K.; Georg, T.; Becker, J. Clinical Evaluation of an Er:YAG Laser for Nonsurgical Treatment of Peri-Implantitis: A Pilot Study. Clin. Ora.l Implant. Res. 2005, 16, 44–52. [Google Scholar] [CrossRef] [PubMed]
- Renvert, S.; Lindahl, C.; Roos Jansåker, A.-M.; Persson, G.R. Treatment of Peri-Implantitis Using an Er:YAG Laser or an Air-Abrasive Device: A Randomized Clinical Trial. J. Clin. Periodontol. 2011, 38, 65–73. [Google Scholar] [CrossRef]
- Schwarz, F.; Hegewald, A.; John, G.; Sahm, N.; Becker, J. Four-Year Follow-up of Combined Surgical Therapy of Advanced Peri-Implantitis Evaluating Two Methods of Surface Decontamination. J. Clin. Periodontol. 2013, 40, 962–967. [Google Scholar] [CrossRef] [PubMed]
- Pommer, B.; Haas, R.; Mailath-Pokorny, G.; Fürhauser, R.; Watzek, G.; Busenlechner, D.; Müller-Kern, M.; Kloodt, C. Periimplantitis Treatment: Long-Term Comparison of Laser Decontamination and Implantoplasty Surgery. Implant. Dent. 2016, 25, 646–649. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.-W.; Ashnagar, S.; Gianflippo, R.D.; Arnett, M.; Kinney, J.; Wang, H.-L. Laser-Assisted Regenerative Surgical Therapy for Peri-Implantitis: A Randomized Controlled Clinical Trial. J. Periodontol. 2020. [Google Scholar] [CrossRef]
- Romanos, G.E.; Nentwig, G.H. Regenerative Therapy of Deep Peri-Implant Infrabony Defects after CO2 Laser Implant Surface Decontamination. Int J. Periodontics Restor. Dent. 2008, 28, 245–255. [Google Scholar]
- Deppe, H.; Horch, H.-H.; Neff, A. Conventional versus CO2 Laser-Assisted Treatment of Peri-Implant Defects with the Concomitant Use of Pure-Phase Beta-Tricalcium Phosphate: A 5-Year Clinical Report. Int. J. Oral Maxillofac. Implant. 2007, 22, 79–86. [Google Scholar]
- Schär, D.; Ramseier, C.A.; Eick, S.; Arweiler, N.B.; Sculean, A.; Salvi, G.E. Anti-Infective Therapy of Peri-Implantitis with Adjunctive Local Drug Delivery or Photodynamic Therapy: Six-Month Outcomes of a Prospective Randomized Clinical Trial. Clin. Oral Implant. Res. 2013, 24, 104–110. [Google Scholar] [CrossRef]
- Bassetti, M.; Schär, D.; Wicki, B.; Eick, S.; Ramseier, C.A.; Arweiler, N.B.; Sculean, A.; Salvi, G.E. Anti-Infective Therapy of Peri-Implantitis with Adjunctive Local Drug Delivery or Photodynamic Therapy: 12-Month Outcomes of a Randomized Controlled Clinical Trial. Clin. Oral Implant. Res. 2014, 25, 279–287. [Google Scholar] [CrossRef]
- Deppe, H.; Mücke, T.; Wagenpfeil, S.; Kesting, M.; Sculean, A. Nonsurgical Antimicrobial Photodynamic Therapy in Moderate vs Severe Peri-Implant Defects: A Clinical Pilot Study. Quintessence Int. 2013, 44, 609–618. [Google Scholar] [CrossRef]
- Bombeccari, G.P.; Guzzi, G.; Gualini, F.; Gualini, S.; Santoro, F.; Spadari, F. Photodynamic Therapy to Treat Periimplantitis. Implant. Dent. 2013, 22, 631–638. [Google Scholar] [CrossRef] [PubMed]
- Papadopoulos, C.A.; Vouros, I.; Menexes, G.; Konstantinidis, A. The Utilization of a Diode Laser in the Surgical Treatment of Peri-Implantitis. A Randomized Clinical Trial. Clin. Oral Investig. 2015, 19, 1851–1860. [Google Scholar] [CrossRef] [PubMed]
- Tenore, G.; Montori, A.; Mohsen, A.; Mattarelli, G.; Palaia, G.; Romeo, U. Evaluation of Adjunctive Efficacy of Diode Laser in the Treatment of Peri-Implant Mucositis: A Randomized Clinical Trial. Lasers Med. Sci. 2020, 35, 1411–1417. [Google Scholar] [CrossRef]
- Mettraux, G.R.; Sculean, A.; Bürgin, W.B.; Salvi, G.E. Two-Year Clinical Outcomes Following Non-Surgical Mechanical Therapy of Peri-Implantitis with Adjunctive Diode Laser Application. Clin. Oral Implant. Res. 2016, 27, 845–849. [Google Scholar] [CrossRef]
- Kotsovilis, S.; Karoussis, I.K.; Trianti, M.; Fourmousis, I. Therapy of Peri-Implantitis: A Systematic Review. J. Clin. Periodontol. 2008, 35, 621–629. [Google Scholar] [CrossRef] [PubMed]
- Giannelli, M.; Lasagni, M.; Bani, D. Thermal Effects of λ = 808 Nm GaAlAs Diode Laser Irradiation on Different Titanium Surfaces. Lasers Med. Sci. 2015, 30, 2341–2352. [Google Scholar] [CrossRef]
- Kreisler, M.; Götz, H.; Duschner, H. Effect of Nd:YAG, Ho:YAG, Er:YAG, CO2, and GaAIAs Laser Irradiation on Surface Properties of Endosseous Dental Implants. Int. J. Oral Maxillofac. Implant. 2002, 17, 202–211. [Google Scholar]
- Ganz, C.H. Evaluation of the Safety of the Carbon Dioxide Laser Used in Conjunction with Root Form Implants: A Pilot Study. J. Prosthet. Dent. 1994, 71, 27–30. [Google Scholar] [CrossRef]
- Matsuyama, T.; Aoki, A.; Oda, S.; Yoneyama, T.; Ishikawa, I. Effects of the Er:YAG Laser Irradiation on Titanium Implant Materials and Contaminated Implant Abutment Surfaces. J. Clin. Laser Med. Surg. 2003, 21, 7–17. [Google Scholar] [CrossRef] [PubMed]
- Taniguchi, Y.; Aoki, A.; Mizutani, K.; Takeuchi, Y.; Ichinose, S.; Takasaki, A.A.; Schwarz, F.; Izumi, Y. Optimal Er:YAG Laser Irradiation Parameters for Debridement of Microstructured Fixture Surfaces of Titanium Dental Implants. Lasers Med. Sci. 2013, 28, 1057–1068. [Google Scholar] [CrossRef] [PubMed]
- Aoki, A.; Mizutani, K.; Schwarz, F.; Sculean, A.; Yukna, R.A.; Takasaki, A.A.; Romanos, G.E.; Taniguchi, Y.; Sasaki, K.M.; Zeredo, J.L.; et al. Periodontal and Peri-Implant Wound Healing Following Laser Therapy. Periodontology 2000 2015, 68, 217–269. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.-W.; Renvert, S.; Wang, H.-L. Nonsurgical Treatment of Periimplantitis. Implant. Dent. 2019, 28, 155–160. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author-Year | Type of Laser | Laser Settings | No. of Patients | Study Design | Follow-Up Duration | Results Obtained at the End of the Follow-Up | Conclusions |
|---|---|---|---|---|---|---|---|
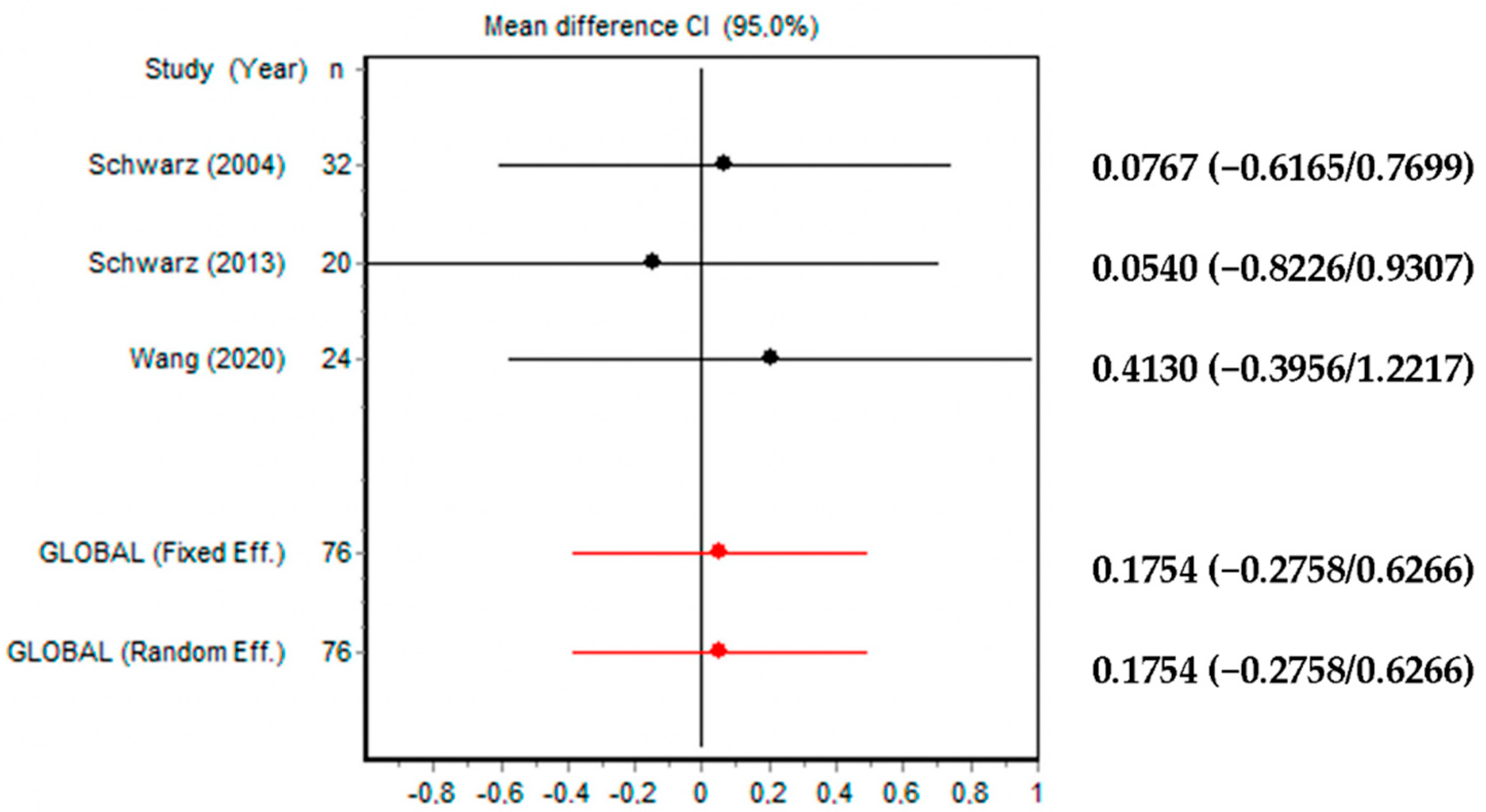
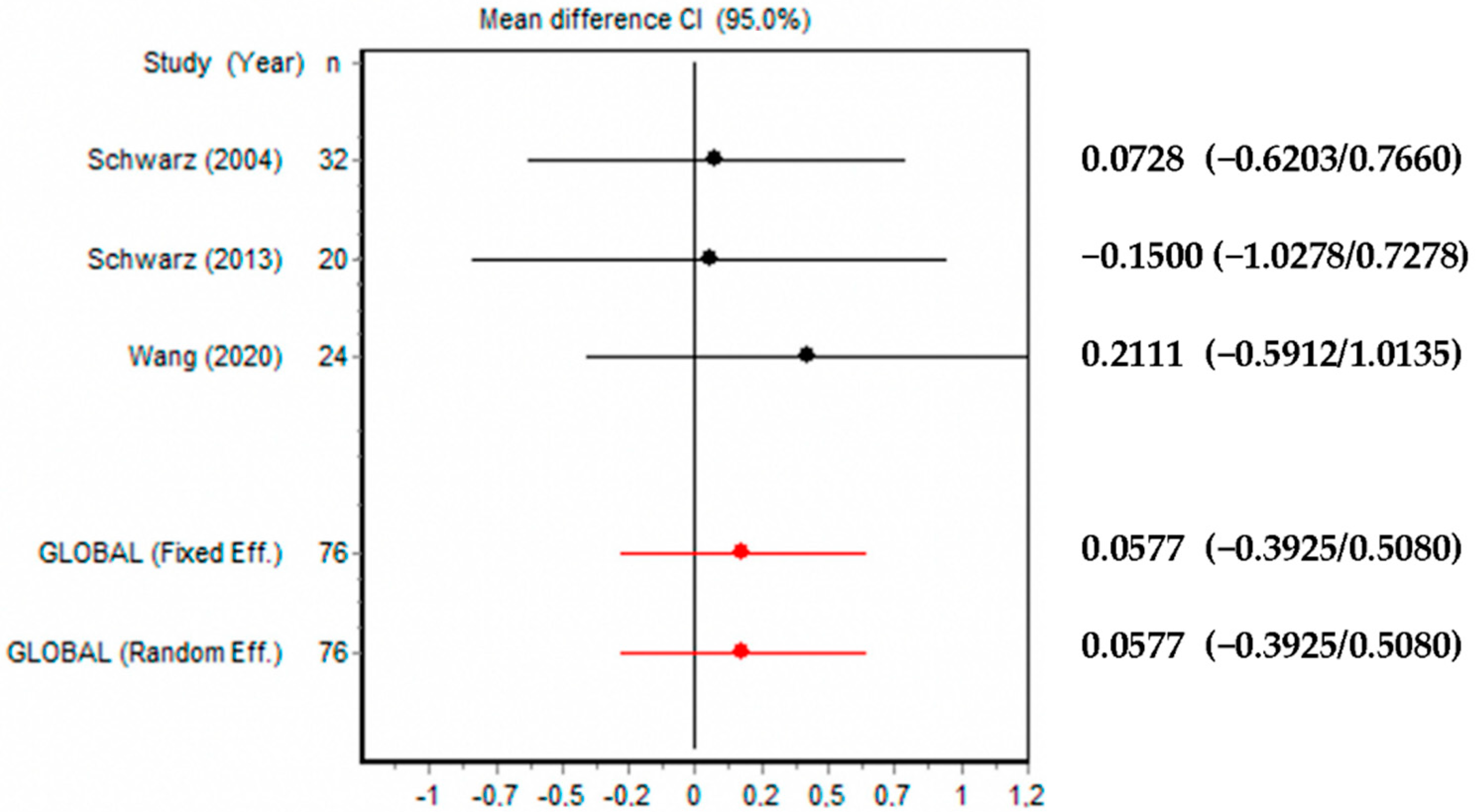
| Schwarz et al., 2005 [12] | Er:YAG | Wavelength 2.94 nm at 100 mJ/pulse | 20 patients with a total of 32 dental implants. Test group: 16 implants; Control group: 16 implants | Pilot study. Test group: Er: YAG laser instrumentation. Control group: mechanical debridement using plastic curettes and antiseptic therapy with chlorhexidine digluconate (0.2%) | 6 months | Test group: mean value of BOP decreased from 83% at baseline to 31% after 6 months. A mean CAL change from 5.8 ± 1 mm at baseline to 5.1 ± 1.1 mm after 6 months. Control group: mean value of BOP decreased from 80% at baseline to 58% after 6 months. A mean CAL change from 6.2 ± 1.5 mm at baseline to 5.6 ± 1.6 mm after 6 months | After 6 months, the difference in CAL gain between the two groups was statistically not significant (p > 0.05). A statistically significant higher reduction of BOP than in control group was achieved in the test group |
| Renvert et al., 2011 [13] | Er:YAG | 100 mJ/pulse | 42 patients. Test group: 21 patients; Control group: 21 patients | Randomized controlled trial. Test group: implants were treated with Er:YAG laser instrumentation. Control group: implants were treated with air-polishing used in the pocket around the implant | 6 months | The mean probing depth (PPD) reductions in the control and test groups were 0.9 mm and 0.8 mm, with mean bone-level changes (loss) of −0.1 mm and −0.3 mm, respectively | No statistically different results were achieved between control and test group after 6 months |
| Schwarz et al., 2013 [14] | Er:YAG | Wavelength 2.94 nm at 100 mJ/pulse | 17 patients. Test group: 7 patients; Control group: 10 patients | Randomized controlled trial. In both groups surgical therapy to obtain a complete granulation tissue remotion and implantoplasty at exposed fixtures parts were performed. Subsequently, implants were treated with Er:YAG laser in the test group, while only with plastic curettes in the control group | 48 months | In control group a higher reduction in mean BOP (control: 85.2 ± 16.4% versus test: 71.6 ± 24.9%) and better CAL values (control: 1.5 ± 2.0 mm versus test: 1.2 ± 2.0 mm) was obtained when compared with the test group | Implants surfaces decontaminations methods did not influence clinical outcome obtained with surgical therapy in the treatment of advanced peri-implantitis disease |
| Pommer et al., 2016 [15] | Er:YAG | Wavelength 2.94 nm | 142 patients. Group 1: 72 patients, Group 2: 47 patients; Group 3: 23 patients | Comparative study. Group 1: laser decontamination; Group 2: implantoplasty; Group 3: laser decontamination + implantoplasty | 9 years | Success rate / implant failure after 9-years of follow-up. Laser therapy: 91.9% success rate; Implantoplasty: 87.2% success rate; Combination of both technique: 82.6% success rate | No statistically difference was found by the authors after 9 years of follow-up between 3 groups |
| Wang et al., 2020 [16] | Er:YAG | 50 mJ/pulse, 25 pulse/s | 24 patients. Test group: 12 patients; Control group: 12 patients | Randomized controlled clinical trial. Control group: surgical regenerative therapy, involving mechanical debridement and GBR. Test group: adjunctive laser irradiation in addition to mechanical debridement prior to bone grafting | 6 months | PD reductions was higher in test group vs. control. No statistical differences were found in CAL gain (1.90 ± 2.28 vs. 1.47 ± 1.76 mm; test vs. control), GI reduction (−1.14 ± 1.15 vs. −1.04 ± 0.89; test vs. control), radiographic linear bone gain (1.27 ± 1.14 vs. 1.08 ± 1.04 mm; test vs. control) or proportional defect size reduction (−24.46 ± 19.00% vs. −15.19 ± 23.56%; test vs. control) | The use of Er:YAG laser was effective in PPD reduction |
| First Author-Year | Type of Laser | Laser Settings | No. of Patients | Study Design | Follow-Up Duration | Results Obtained at the End of the Follow-Up | Conclusions |
|---|---|---|---|---|---|---|---|
| Romanos et al., 2008 [17] | CO2 | Wavelength 10.6 nm at 2.8 W | 15 patients | Case series. Surgical therapy of peri-implant infrabony defects through CO2 laser irradiation + bone augmentation | Mean post-operative observational period 27.10 ± 17.83 months | Clinical parameters such as sulcus bleeding index (2.76 ± 0.35 vs. 1.03 ± 0.85 after surgery) and probing depth (6.0 ± 2 mm vs. 2.48 ± 0.63 mm after surgery) presented a significant reduction during the examination period. Complete bone filling was radiologically observed in all defects. | In this study, CO2 laser decontamination associated with regenerative surgery was effective in the treatment of peri-implantitis. |
| Deppe et al., 2007 [18] | CO2 | Wavelength 10.6 nm at 7 W | 73 implants. Group 1: 19 implants; Group 2: 15 implants; Group 3: 22 implants; Group 4: 17 implants | Clinical Report. Group 1: Conventional decontamination + soft tissue resection. Group 2: Conventional decontamination + bone augmentation. Group 3: Laser decontamination + soft tissue resection. Group 4: Laser decontamination + bone augmentation | 4 (T1) and 59 (T2) months | Group 1 vs. Group 3: Group 3 showed better results in terms of CAL mean values (5.5 mm ± 0.9 mm) vs. Group 1 (6.3 mm ± 1.1 mm) at T1 and (6.6 mm ± 0.7 mm for Group 3 vs. 7.0 mm ± 0.9 mm for Group 1) at T2. A shorter distance from implant shoulder to the first bone contact was observed in Group 3 (6.8 mm ± 0.9 mm) versus Group 1 (7.9 mm ± 1.3 mm) at T2; no statistically significant differences were found between the two groups (6.9 mm ± 1.4 mm for Group 3 vs. 7.2 mm ± 1.9 mm for Group 1) at T1. Group 2 vs. Group 4: Group 4 showed better results in terms of clinical attachment level (CAL) mean values (1.6 mm ± 1.5 mm) with respect to Group 2 (3.5 mm ± 1.2 mm) at T1; no statistically significant differences were observed between the two groups (3.6 mm ± 1.4 mm for Group 4 vs. 3.8 mm ± 0.5 mm for Group 2) at T2. A shorter distance from implant shoulder to the first bone contact was observed in Group 4 (2.3 mm ± 0.9 mm) versus Group 2 (4.1 mm ± 0.9 mm) at T1; no statistically significant differences were observed between the two groups (4.5 mm ± 1.2 mm for Group 4 vs. 4.7 mm ± 1.1 mm for Group 2) at T2. | CO2 laser decontamination may be more efficacious than conventional decontamination in deep, narrow bony defects and especially when combined with soft tissue resection. |
| First Author-Year | Type of Laser | Laser Settings | No. of Patients | Study Design | Follow-Up Duration | Results Obtained at the End of the Follow-Up | Conclusions |
|---|---|---|---|---|---|---|---|
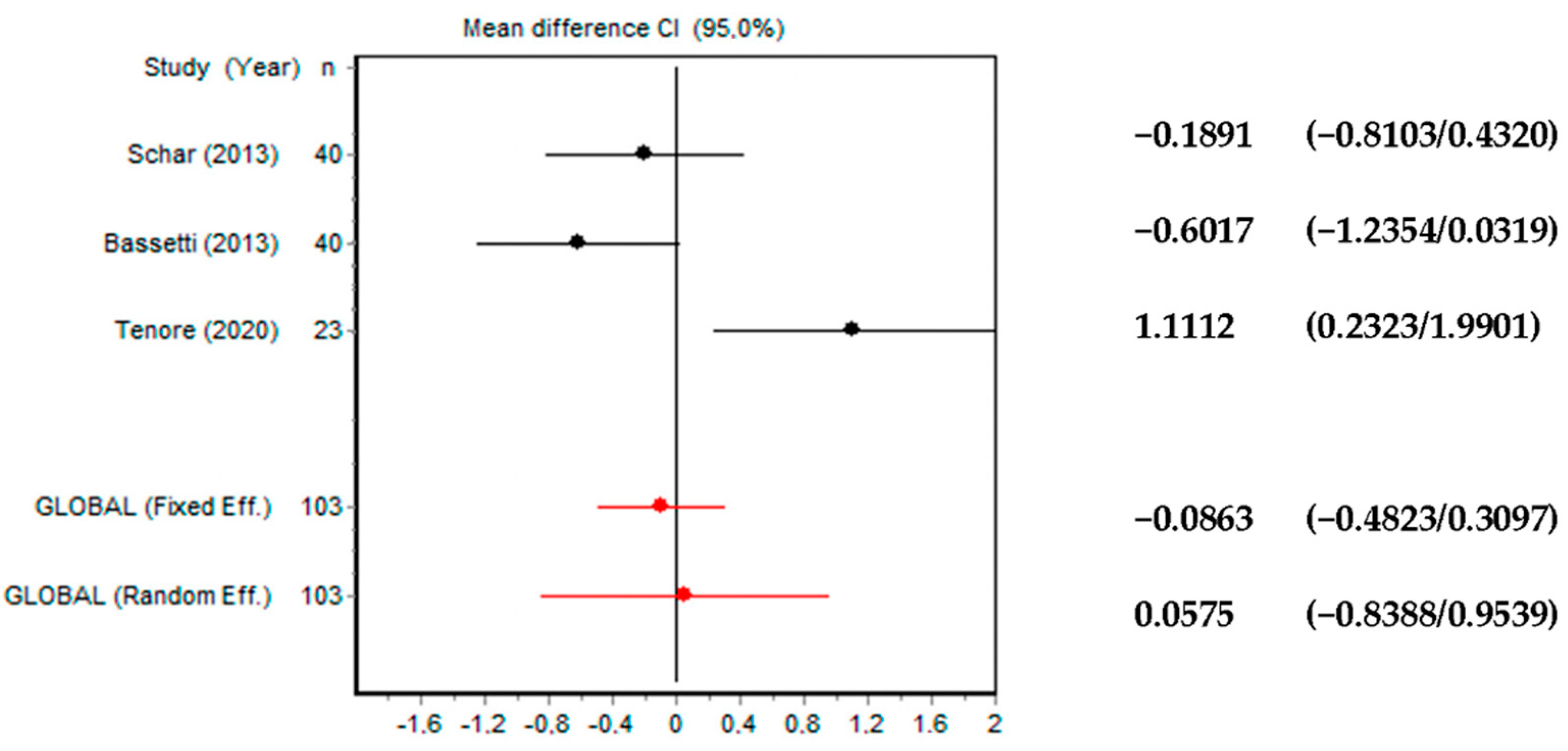
| Schar et al., 2013 [19] | Diode laser + dye phenothiazine chloride | Wavelength of 660 nm; Power density of 100 mW | 40 patients. Test group: 20 patients Control group: 20 patients | Prospective randomized clinical trial. All implants were mechanically debrided with titanium curettes and with a glycine-based powder air-polishing system. Implants in the test group received adjunctive photodynamic therapy (PDT), whereas minocycline microspheres were locally delivered into the peri-implant pockets of control implants | 6 months | Complete resolution of mucosal inflammation was obtained in 15% of the implants in the control group and in 30% of the implants in the test group (p = 0.16). Periodontal probing depth (PPD), mucosal recession, plaque index (PI) and clinical attachment level (CAL) measurements did not yield statistically significant changes (p > 0.05) in both groups | Adjunctive PDT may represent an alternative treatment modality in the non-surgical management of initial peri-implantitis |
| Bassetti et al., 2014 [20] | Diode laser + dye phenothiazine chloride | Wavelength of 660 nm; Power density of 100 mW | 40 patients. Test group: 20 patients Control group: 20 patients | Prospective randomized clinical trial. All implants were mechanically debrided with titanium curettes and with a glycine-based powder air-polishing system. Implants in the test group received adjunctive PDT, whereas minocycline microspheres were locally delivered into the peri-implant pockets of control implants | 12 months | Complete resolution of mucosal inflammation was obtained in 35% of the implants in the control group and in 41.1% of the implants in the test group (p = 0.16). PPD, mucosal recession, PI and CAL measurements did not yield statistically significant changes (p > 0.05) in both groups | Adjunctive PDT may represent an alternative treatment modality in the non-surgical management of initial peri-implantitis |
| Deppe et al., 2013 [21] | Diode laser + phenothiazine chloride | Wavelength of 660 nm; Power density of 60 mW | 16 patients with a total of 18 dental implant. Group 1: 10 implants. Group 2: 8 implants | Clinical Pilot Study. Group 1: <5 mm bone loss around the implant. Group 2: >5 mm bone loss around the implant. Each group was treated by photodynamic therapy (PDT) | 3 months and 6 months | 3 months after therapy, in both groups, sulcus bleeding index and CAL decreased significantly. In contrast, after 6 months, CAL and radiographic evaluation of distance from implant to bone (DIB) increased significantly in Group 2, not in Group 1. However, distance from implant shoulder to marginal mucosa were not statistically different 6 months after therapy in both groups | Nonsurgical PDT could stop bone resorption in moderate peri-implant defects. (<5 mm) but not in severe defects (>5 mm) |
| Bombeccari et al., 2013 [22] | Diode laser | Wavelength of 810 nm and a continuous wave mode of 1 W | 40 patients. Test group: 20 patients. Control group: 20 patients | Randomized comparative case-control study. The aim of this study was to compare the efficacy of antimicrobial PDT in the test group (N = 20) versus conventionally surgical therapy in the control group (N = 20), in patients with peri-implantitis | 6 months | Total anaerobic counts of bacteria did not differ significantly between the two groups (test group, 95.2%; control group 80.85%). Bleeding on probing (BOP) at 6 months after treatment was observed in adult periodontally compromised patients in both groups. Changes in PPD were recorded in the PDT group only | Treatment with PDT in patients with peri-implantitis was not associated with major reduction of total anaerobic bacteria on the rough surfaces of dental implants as compared with surgical therapy |
| Papadopoulos et al., 2015 [23] | Diode laser | Wavelength of 980 nm 0.8 W in pulsed mode | 19 patients. Test group: 9. Control group: 10 | Randomized comparative case-control study. Control group: mucoperiosteal flaps, implant surface debridement with plastic curettes and sterilized gauzes soaked in saline. Test group: was treated similarly but with additional irradiation using a diode laser | 6 months | 3 months after treatment, a mean PPD reduction of 1.19 mm for the control group and 1.38 mm for the test group was recorded. The corresponding BOP changes were 72.9 and 66.7%, respectively. These changes were significant and remained at the same levels at the 6-month examination (p < 0.05). | Surgical treatment of peri-implantitis by access flaps leads to improvement of all clinical parameters studied while the additional use of diode laser does not seem to have an extra beneficiary effect |
| Tenore et al., 2020 [24] | Diode laser | Wavelength 980 nm, at power of 1W in pulsed mode | 23 patients with a total of 23 dental implants. Test group: 11 implants. Control group: 12 implants | Randomized Controlled Trial. For both groups, full mouth mechanical debridement was per- formed through the use of ultrasonic piezoelectric scaler and manual instruments. In test group the peri-implant sulcus of each implant was irradiated immediately after the mechanical debridement with laser | 3 months | The average of PPD value for test group was 4.04 ± 0.54 mm at baseline and it was 2.98 ± 0.7 mm after 3 months. In the control group, the average was 3.8 ± 1.24 mm at baseline and was 3.54 ± 0.35 mm after 3 months. A greater decrease in both clinical parameters was detected for subjects treated with lasers (test group) | Diode laser may be considered an adjunct to the conventional non-surgical treatments of peri-implants mucositis and initial peri-implantitis |
| Mettraux et al., 2016 [25] | Diode laser | Wavelength 810 nm, 2.5 W, 50 Hz, 10 ms | 15 patients with a total of 23 dental implants. | Retrospective case series study. The implant surfaces were debrided under local anesthesia using carbon fiber curettes, and the inflamed peri-implant soft tissue wall was curetted with sharp metal curettes. Adjunctive diode laser was applied | 2 years | The deepest PPD decreased from 7.5 ± 2.6 mm to 3.6 ± 0.7 mm at buccal (p < 0.0001) and from 7.7 ± 2.1 mm to 3.8 ± 0.9 mm at oral sites (p < 0.0001), respectively. The % of implants with ≥1 site with BoP decreased from 100% at BL to 43% after 2 years (p = 0.0002). The % of implants with suppuration decreased from 87% at BL to 0% after 2 years (p < 0.0001) | Non-surgical mechanical therapy of PI with adjunctive repeated application of a diode laser yielded significant clinical improvements after an observation period of at least 2 years |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pisano, M.; Amato, A.; Sammartino, P.; Iandolo, A.; Martina, S.; Caggiano, M. Laser Therapy in the Treatment of Peri-Implantitis: State-of-the-Art, Literature Review and Meta-Analysis. Appl. Sci. 2021, 11, 5290. https://doi.org/10.3390/app11115290
Pisano M, Amato A, Sammartino P, Iandolo A, Martina S, Caggiano M. Laser Therapy in the Treatment of Peri-Implantitis: State-of-the-Art, Literature Review and Meta-Analysis. Applied Sciences. 2021; 11(11):5290. https://doi.org/10.3390/app11115290
Chicago/Turabian StylePisano, Massimo, Alessandra Amato, Pasquale Sammartino, Alfredo Iandolo, Stefano Martina, and Mario Caggiano. 2021. "Laser Therapy in the Treatment of Peri-Implantitis: State-of-the-Art, Literature Review and Meta-Analysis" Applied Sciences 11, no. 11: 5290. https://doi.org/10.3390/app11115290
APA StylePisano, M., Amato, A., Sammartino, P., Iandolo, A., Martina, S., & Caggiano, M. (2021). Laser Therapy in the Treatment of Peri-Implantitis: State-of-the-Art, Literature Review and Meta-Analysis. Applied Sciences, 11(11), 5290. https://doi.org/10.3390/app11115290