
Intra- and Inter-Rater Reliability of a Well-Used and a Less-Used IsoMed 2000 Dynamometer for Knee Flexion and Extension Peak Torque Measurements in a Concentric Test in Athletes

 , ,
, ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Design
2.3. Procedures
2.4. Outcome Variables
2.5. Statistical Analysis
3. Results
3.1. Intra-Rater Reliability
3.2. Trial Effect
3.3. Inter-Rater Reliability
3.4. Dynamometer Effect
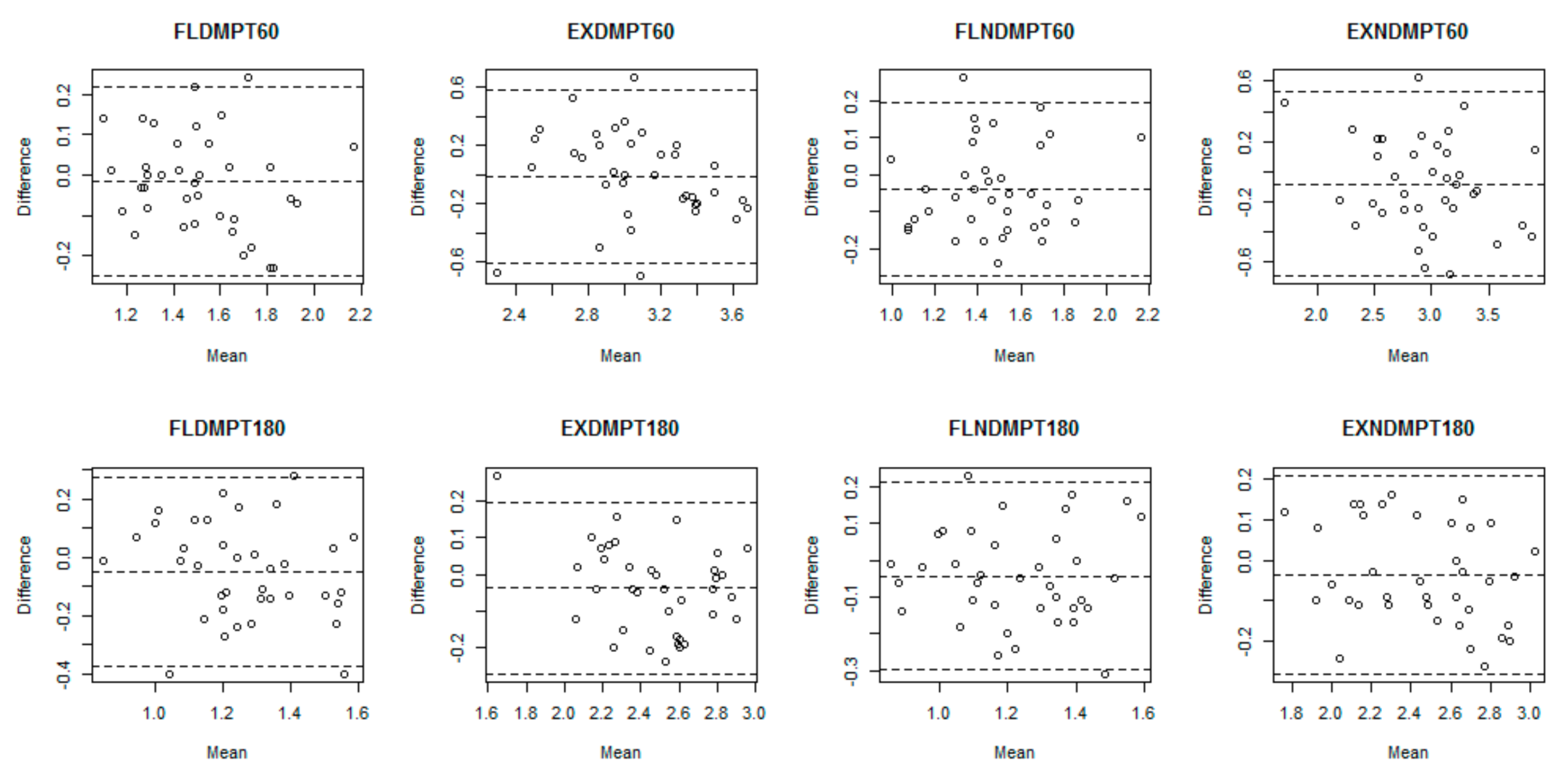
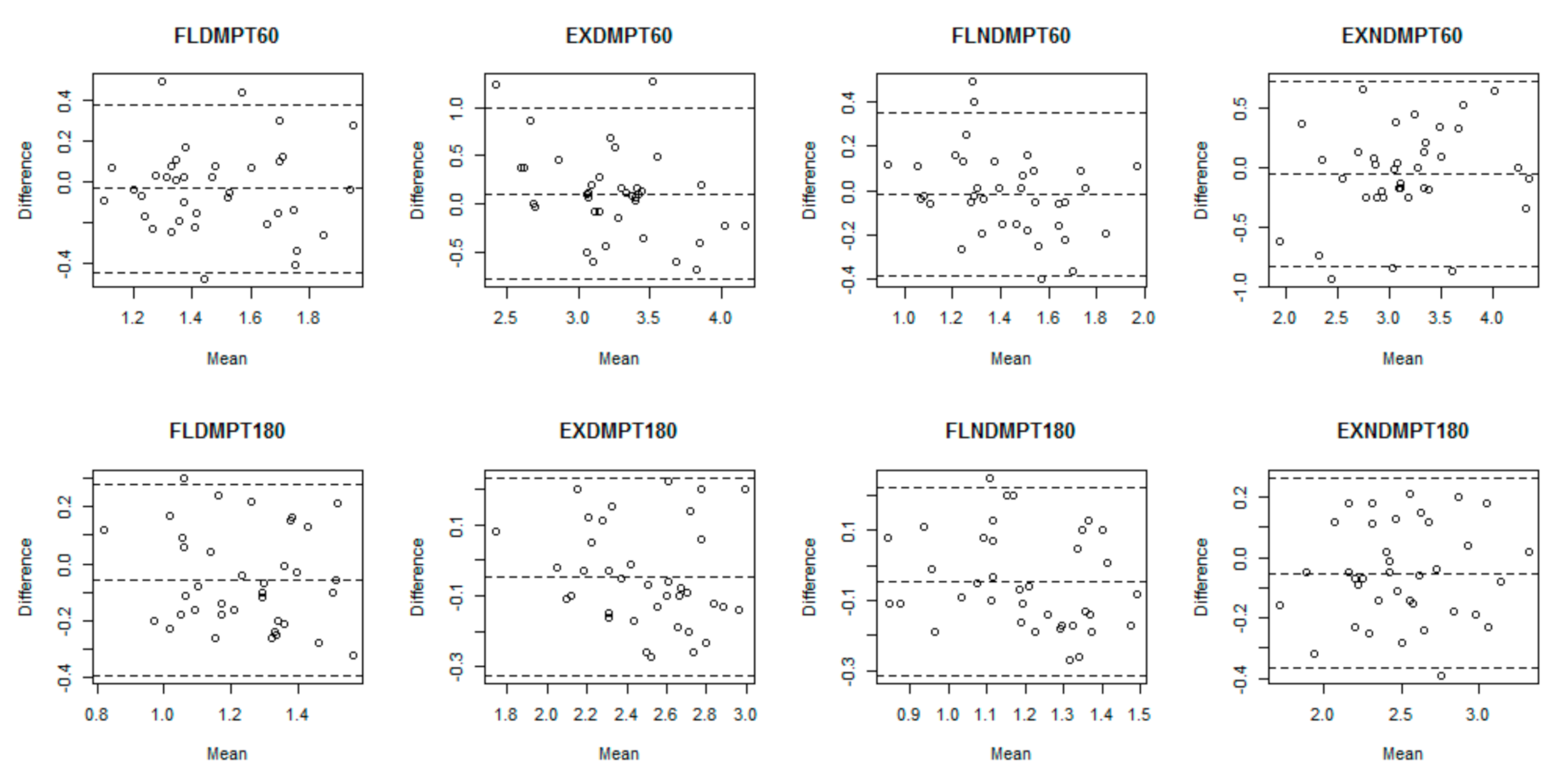
3.5. Bland-Altman Analysis
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Achenbach, L.; Laver, L.; Walter, S.S.; Zeman, F.; Kuhr, M.; Krutsch, W. Decreased external rotation strength is a risk factor for overuse shoulder injury in youth elite handball athletes. Knee Surg. Sports Traumatol. Arthrosc. 2019, 28, 1–10. [Google Scholar]
- Faigenbaum, A.D.; Lloyd, R.S.; MacDonald, J.; Myer, G.D. Citius, Altius, Fortius: Beneficial effects of resistance training for young athletes: Narrative review. Br. J. Sports Med. 2016, 50, 3–7. [Google Scholar] [CrossRef]
- Alvares, J.B.A.R.; Rodrigues, R.; de Azevedo Franke, R.; da Silva, B.G.C.; Pinto, R.S.; Vaz, M.A.; Baroni, B.M. Inter-machine reliability of the Biodex and Cybex isokinetic dynamometers for knee flexor/extensor isometric, concentric and eccentric tests. Phys. Ther. Sports 2015, 16, 59–65. [Google Scholar] [CrossRef]
- Forthomme, B.; Croisier, J.-L.; Delvaux, F.; Kaux, J.-F.; Crielaard, J.-M.; Gleizes-Cervera, S. Preseason strength assessment of the rotator muscles and shoulder injury in handball players. J. Athl. Train. 2018, 53, 174–180. [Google Scholar] [CrossRef] [PubMed]
- Willigenburg, N.W.; McNally, M.P.; Hewett, T.E. Quadriceps and hamstrings strength in athletes. In Hamstring and Quadriceps Injuries in Athletes; Springer: New York, NY, USA, 2014; pp. 15–28. [Google Scholar]
- Kolber, M.J.; Cleland, J.A. Strength testing using hand-held dynamometry. Phys. Ther. Rev. 2005, 10, 99–112. [Google Scholar] [CrossRef]
- Jackson, S.M.; Cheng, M.S.; Smith, A.R., Jr.; Kolber, M.J. Intrarater reliability of hand held dynamometry in measuring lower extremity isometric strength using a portable stabilization device. Musculoskelet. Sci. Pract. 2017, 27, 137–141. [Google Scholar] [CrossRef]
- Sung, K.-S.; Yi, Y.G.; Shin, H.-I. Reliability and validity of knee extensor strength measurements using a portable dynamometer anchoring system in a supine position. BMC Musculoskelet. Disord. 2019, 20, 320. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, R.; Araújo, J.P.; Barreira, P.; Loureiro, N.; Diesel, W. Preseason Evaluation. In Injuries and Health Problems in Football; Springer: Berlin/Heidelberg, Germany, 2017; pp. 493–514. [Google Scholar]
- Baltzopoulos, B.; King, M.; Gleeson, N.; De Ste Croix, M. The BASES expert statement on measurement of muscle strength with isokinetic dynamometry. Sport Exerc. Sci. 2012, 31, 12–13. [Google Scholar]
- Dirnberger, J.; Wiesinger, H.-P.; Stöggl, T.; Kösters, A.; Müller, E. Absolute und relative Kraftausdauer der Kniebeuge-und-streckmuskulatur: Eine Reliabilitätsstudie unter Verwendung des IsoMed 2000-Dynamometers. Sportverletz. Sportsc. 2012, 26, 142–147. [Google Scholar] [CrossRef] [PubMed]
- Maffiuletti, N.A.; Bizzini, M.; Desbrosses, K.; Babault, N.; Munzinger, U. Reliability of knee extension and flexion measurements using the Con-Trex isokinetic dynamometer. Clin. Physiol. Funct. Imaging 2007, 27, 346–353. [Google Scholar] [CrossRef] [PubMed]
- Dirnberger, J.; Kösters, A.; Müller, E. Concentric and eccentric isokinetic knee extension: A reproducibility study using the IsoMed 2000-dynamometer. Isokinet. Exerc. Sci. 2012, 20, 31–35. [Google Scholar] [CrossRef]
- Lund, H.; Søndergaard, K.; Zachariassen, T.; Christensen, R.; Bülow, P.; Henriksen, M.; Bartels, E.; Danneskiold-Samsøe, B.; Bliddal, H. Learning effect of isokinetic measurements in healthy subjects, and reliability and comparability of Biodex and Lido dynamometers. Clin. Physiol. Funct. Imaging 2005, 25, 75–82. [Google Scholar] [CrossRef]
- Jenkins, N.D.; Palmer, T.B.; Cramer, J.T. Comparisons of voluntary and evoked rate of torque development and rate of velocity development during isokinetic muscle actions. Isokinet. Exerc. Sci. 2013, 21, 253–261. [Google Scholar] [CrossRef]
- Guilhem, G.; Giroux, C.; Couturier, A.; Maffiuletti, N.A. Validity of trunk extensor and flexor torque measurements using isokinetic dynamometry. J. Electromyogr. Kinesiol. 2014, 24, 986–993. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge Academic: New York, NY, USA, 1988. [Google Scholar]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.-G. Statistical power analyses using G* Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef]
- Lehnert, B. Package ‘BlandAltmanLeh’. Available online: https://cloud.r-project.org/web/packages/BlandAltmanLeh/BlandAltmanLeh.pdf (accessed on 23 December 2015).
- Shrout, P.E.; Fleiss, J.L. Intraclass correlations: Uses in assessing rater reliability. Psychol. Bull. 1979, 86, 420. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Portney, L.G.; Watkins, M.P. Foundations of Clinical Research: Applications to Practice; Pearson/Prentice Hall: Upper Saddle River, NJ, USA, 2009; Volume 892. [Google Scholar]
- Weir, J.P. Quantifying test-retest reliability using the intraclass correlation coefficient and the SEM. J. Strength Cond. Res. 2005, 19, 231–240. [Google Scholar] [PubMed]
- Lee, P.; Liu, C.-H.; Fan, C.-W.; Lu, C.-P.; Lu, W.-S.; Hsieh, C.-L. The test–retest reliability and the minimal detectable change of the Purdue Pegboard Test in schizophrenia. J. Formos. Med. Assoc. 2013, 112, 332–337. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 327, 307–310. [Google Scholar] [CrossRef]
- Vargas, V.Z.; Motta, C.; Peres, B.; Vancini, R.L.; Andre Barbosa De Lira, C.; Andrade, M.S. Knee isokinetic muscle strength and balance ratio in female soccer players of different age groups: A cross-sectional study. Phys. Sportsmed. 2020, 48, 105–109. [Google Scholar] [CrossRef]
- Muñoz-Bermejo, L.; Pérez-Gómez, J.; Manzano, F.; Collado-Mateo, D.; Villafaina, S.; Adsuar, J.C. Reliability of isokinetic knee strength measurements in children: A systematic review and meta-analysis. PLoS ONE 2019, 14, e0226274. [Google Scholar] [CrossRef] [PubMed]
- Sole, G.; Hamrén, J.; Milosavljevic, S.; Nicholson, H.; Sullivan, S.J. Test-retest reliability of isokinetic knee extension and flexion. Arch. Phys. Med. Rehabil. 2007, 88, 626–631. [Google Scholar] [CrossRef]
- Thompson, M.C.; Shingleton, L.G.; Kegerreis, S.T. Comparison of values generated during testing of the knee using the Cybex II Plus® and Biodex Model B-2000® isokinetic dynamometers. J. Orthop. Sports Phys. Ther. 1989, 11, 108–115. [Google Scholar] [CrossRef]
- Gross, M.T.; Huffman, G.M.; Phillips, C.N.; Wray, J.A. Intramachine and intermachine reliability of the Biodex and Cybex® II for knee flexion and extension peak torque and angular work. J. Orthop. Sports Phys. Ther. 1991, 13, 329–335. [Google Scholar] [CrossRef]
- Keilani, M.; Posch, M.; Zorn, C.; Knötig, M.; Pircher, M.; Quittan, M.; Fialka-Moser, V.; Jirasek, U.; Crevenna, R. Comparison of values generated during isokinetic-testing of the knee extensor and flexor muscles using the cybex 6000 and biodex 3 isokinetic dynamometer. Phys. Med. Rehab. Kuror. 2007, 17, 327–333. [Google Scholar] [CrossRef]
- Bandy, W.D.; McLaughlin, S. Intramachine and intermachine reliability for selected dynamic muscle performance tests. J. Orthop. Sports Phys. Ther. 1993, 18, 609–613. [Google Scholar] [CrossRef] [PubMed]
- Harbo, T.; Brincks, J.; Andersen, H. Maximal isokinetic and isometric muscle strength of major muscle groups related to age, body mass, height, and sex in 178 healthy subjects. Eur. J. Appl. Physiol. 2012, 112, 267–275. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Mean | SD | Median | Range [Min-Max] |
|---|---|---|---|---|
| Age (years) | 16.7 | 0.8 | 17.0 | 4.0 [15.0–19.0] |
| Body Mass (kg) | 66.3 | 10.1 | 66.1 | 43.1 [48.4–91.5] |
| Height (m) | 1.65 | 0.07 | 1.67 | 0.26 [1.51–1.78] |
| Experience (year) | 4.8 | 1.4 | 5.0 | 5.0 [3.0–8.0] |
| First Evaluation | Second Evaluation | Third Evaluation | Forth Evaluation | |
|---|---|---|---|---|
| First Group (n = 18) | New Dynamometer | Old Dynamometer | Old Dynamometer | New Dynamometer |
| Second Group (n = 19) | Old Dynamometer | New Dynamometer | New Dynamometer | Old Dynamometer |
| Measures (N/W) | Trial 1 | Trial 2 | Bland-Altman | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | MDa | SD | 95% LoA | ICC | 95% CI | SEM | SDC95 | SDC% | |
| FLDMPT60 | 1.51 | 0.24 | 1.52 | 0.26 | –0.02 | 0.12 | –0.26 + 0.22 | 0.888 | 0.794;0.940 | 0.08 | 0.24 | 15.52 |
| EXDMPT60 | 3.06 | 0.34 | 3.07 | 0.40 | –0.01 | 0.28 | –0.55 + 0.54 | 0.681 | 0.459;0.822 | 0.20 | 0.59 | 17.91 |
| FLNDMPT60 | 1.45 | 0.26 | 1.49 | 0.25 | –0.04 | 0.12 | –0.28 + 0.20 | 0.883 | 0.779;0.939 | 0.08 | 0.24 | 16.00 |
| EXNDMPT60 | 2.91 | 0.45 | 3.00 | 0.53 | –0.08 | 0.31 | –0.69 + 0.53 | 0.788 | 0.627;0.885 | 0.22 | 0.61 | 20.56 |
| FLDMPT180 | 1.24 | 0.19 | 1.29 | 0.22 | –0.05 | 0.16 | –0.36 + 0.26 | 0.659 | 0.431;0.808 | 0.11 | 0.31 | 24.79 |
| EXDMPT180 | 2.46 | 0.27 | 2.49 | 0.31 | –0.04 | 0.12 | –0.28 + 0.20 | 0.911 | 0.831;0.954 | 0.08 | 0.24 | 9.50 |
| FLNDMPT180 | 1.21 | 0.20 | 1.25 | 0.21 | –0.04 | 0.13 | –0.29 + 0.21 | 0.785 | 0.616;0.884 | 0.09 | 0.25 | 20.72 |
| EXNDMPT180 | 2.44 | 0.32 | 2.47 | 0.35 | –0.04 | 0.12 | –0.28 + 0.20 | 0.928 | 0.864;0.963 | 0.08 | 0.24 | 9.58 |
| Measures (N/W) | Trial 1 | Trial 2 | Bland-Altman | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | MDa | SD | 95% LoA | ICC | 95% CI | SEM | SDC95 | SDC% | |
| FLDMPT60 | 1.46 | 0.25 | 1.50 | 0.25 | –0.02 | 0.12 | –0.26 + 0.22 | 0.640 | 0.404;0.796 | 0.08 | 0.24 | 15.89 |
| EXDMPT60 | 3.30 | 0.37 | 3.20 | 0.54 | 0.01 | 0.30 | –0.58 + 0.60 | 0.516 | 0.241;0.716 | 0.21 | 0.59 | 18.09 |
| FLNDMPT60 | 1.42 | 0.23 | 1.43 | 0.28 | –0.01 | 0.19 | –0.38 + 0.36 | 0.734 | 0.438;0.813 | 0.13 | 0.37 | 26.13 |
| EXNDMPT60 | 3.10 | 0.64 | 3.16 | 0.55 | –0.06 | 0.39 | –0.82 + 0.70 | 0.786 | 0.624;0.883 | 0.28 | 0.76 | 24.42 |
| FLDMPT180 | 1.21 | 0.18 | 1.27 | 0.21 | –0.06 | 0.17 | –0.39 + 0.27 | 0.601 | 0.349;0.772 | 0.12 | 0.33 | 26.87 |
| EXDMPT180 | 2.47 | 0.28 | 2.52 | 0.31 | –0.05 | 0.14 | –0.32 + 0.22 | 0.876 | 0.767;0.935 | 0.10 | 0.27 | 11.00 |
| FLNDMPT180 | 1.17 | 0.17 | 1.22 | 0.20 | –0.05 | 0.14 | –0.32 + 0.22 | 0.721 | 0.517;0.846 | 0.10 | 0.27 | 22.96 |
| EXNDMPT180 | 2.48 | 0.38 | 2.53 | 0.37 | –0.05 | 0.16 | –0.36 + 0.26 | 0.901 | 0.813;0.949 | 0.11 | 0.31 | 12.52 |
| Measures (N/W) | Old | New | Bland-Altman | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | MDa | SD | 95% LoA | ICC | 95% CI | SEM | SDC95 | SDC% | |
| FLDMPT60 | 1.51 | 0.24 | 1.46 | 0.25 | 0.04 | 0.14 | –0.24 + 0.32 | 0.818 | 0.672;0.903 | 0.10 | 0.28 | 18.82 |
| EXDMPT60 | 3.06 | 0.34 | 3.30 | 0.37 | –0.24 ** | 0.31 | –0.84 + 0.37 | 0.519 | 0.102;0.754 | 0.22 | 0.60 | 19.00 |
| FLNDMPT60 | 1.45 | 0.26 | 1.42 | 0.23 | 0.04 | 0.13 | –0.21 + 0.29 | 0.849 | 0.726;0.919 | 0.08 | 0.25 | 17.76 |
| EXNDMPT60 | 2.91 | 0.45 | 3.10 | 0.64 | –0.19 ** | 0.41 | –0.99 + 0.61 | 0.688 | 0.438.833 | 0.22 | 0.80 | 26.74 |
| FLDMPT180 | 1.24 | 0.19 | 1.21 | 0.18 | 0.03 | 0.15 | –0.26 + 0.32 | 0.668 | 0.445.813 | 0.11 | 0.29 | 24.00 |
| EXDMPT180 | 2.46 | 0.27 | 2.47 | 0.28 | –0.01 | 0.11 | –0.23 + 0.21 | 0.915 | 0.842;0.955 | 0.08 | 0.22 | 8.75 |
| FLNDMPT180 | 1.21 | 0.20 | 1.17 | 0.17 | 0.03 | 0.14 | –0.24 + 0.30 | 0.727 | 0.532;0.849 | 0.09 | 0.27 | 23.06 |
| EXNDMPT180 | 2.44 | 0.32 | 2.48 | 0.38 | –0.04 | 0.18 | –0.39 + 0.31 | 0.868 | 0.759;0.929 | 0.08 | 0.35 | 14.34 |
| Measures (N/W) | Old | New | Bland-Altman | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | MDa | SD | 95% LoA | ICC | 95% CI | SEM | SDC95 | SDC% | |
| FLDMPT60 | 1.52 | 0.26 | 1.50 | 0.25 | 0.03 | 0.20 | –0.36 + 0.41 | 0.712 | 0.509;0.840 | 0.14 | 0.38 | 25.37 |
| EXDMPT60 | 3.08 | 0.40 | 3.20 | 0.54 | –0.12 | 0.42 | –0.94 + 0.69 | 0.603 | 0.354;0.773 | 0.29 | 0.81 | 25.92 |
| FLNDMPT60 | 1.49 | 0.25 | 1.43 | 0.28 | 0.06 | 0.20 | –0.33 + 0.45 | 0.715 | 0.511;0.843 | 0.14 | 0.39 | 26.85 |
| EXNDMPT60 | 3.00 | 0.53 | 3.16 | 0.55 | –0.17 ** | 0.36 | –0.88 + 0.54 | 0.740 | 0.514;0.864 | 0.25 | 0.71 | 22.91 |
| FLDMPT180 | 1.29 | 0.22 | 1.27 | 0.21 | 0.02 | 0.16 | –0.29 + 0.33 | 0.723 | 0.536;0.847 | 0.11 | 0.31 | 24.50 |
| EXDMPT180 | 2.49 | 0.31 | 2.52 | 0.31 | –0.02 | 0.13 | –0.27 + 0.23 | 0.909 | 0.831;0.952 | 0.09 | 0.25 | 10.17 |
| FLNDMPT180 | 1.25 | 0.21 | 1.22 | 0.20 | 0.03 | 0.14 | –0.24 + 0.30 | 0.774 | 0.606;0.877 | 0.10 | 0.27 | 22.22 |
| EXNDMPT180 | 2.47 | 0.35 | 2.53 | 0.37 | –0.06 * | 0.16 | –0.37 + 0.25 | 0.891 | 0.790;0.943 | 0.11 | 0.31 | 12.54 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kocahan, T.; Akınoğlu, B.; Yilmaz, A.E.; Rosemann, T.; Knechtle, B. Intra- and Inter-Rater Reliability of a Well-Used and a Less-Used IsoMed 2000 Dynamometer for Knee Flexion and Extension Peak Torque Measurements in a Concentric Test in Athletes. Appl. Sci. 2021, 11, 4951. https://doi.org/10.3390/app11114951
Kocahan T, Akınoğlu B, Yilmaz AE, Rosemann T, Knechtle B. Intra- and Inter-Rater Reliability of a Well-Used and a Less-Used IsoMed 2000 Dynamometer for Knee Flexion and Extension Peak Torque Measurements in a Concentric Test in Athletes. Applied Sciences. 2021; 11(11):4951. https://doi.org/10.3390/app11114951
Chicago/Turabian StyleKocahan, Tuğba, Bihter Akınoğlu, Ayfer Ezgi Yilmaz, Thomas Rosemann, and Beat Knechtle. 2021. "Intra- and Inter-Rater Reliability of a Well-Used and a Less-Used IsoMed 2000 Dynamometer for Knee Flexion and Extension Peak Torque Measurements in a Concentric Test in Athletes" Applied Sciences 11, no. 11: 4951. https://doi.org/10.3390/app11114951
APA StyleKocahan, T., Akınoğlu, B., Yilmaz, A. E., Rosemann, T., & Knechtle, B. (2021). Intra- and Inter-Rater Reliability of a Well-Used and a Less-Used IsoMed 2000 Dynamometer for Knee Flexion and Extension Peak Torque Measurements in a Concentric Test in Athletes. Applied Sciences, 11(11), 4951. https://doi.org/10.3390/app11114951