
In-Vitro Comparative Adhesion Evaluation of Bioceramic and Dual-Cure Resin Endodontic Sealers Using SEM, AFM, Push-Out and FTIR


 ,
,  ,
, 

 ,
,
Abstract
1. Introduction
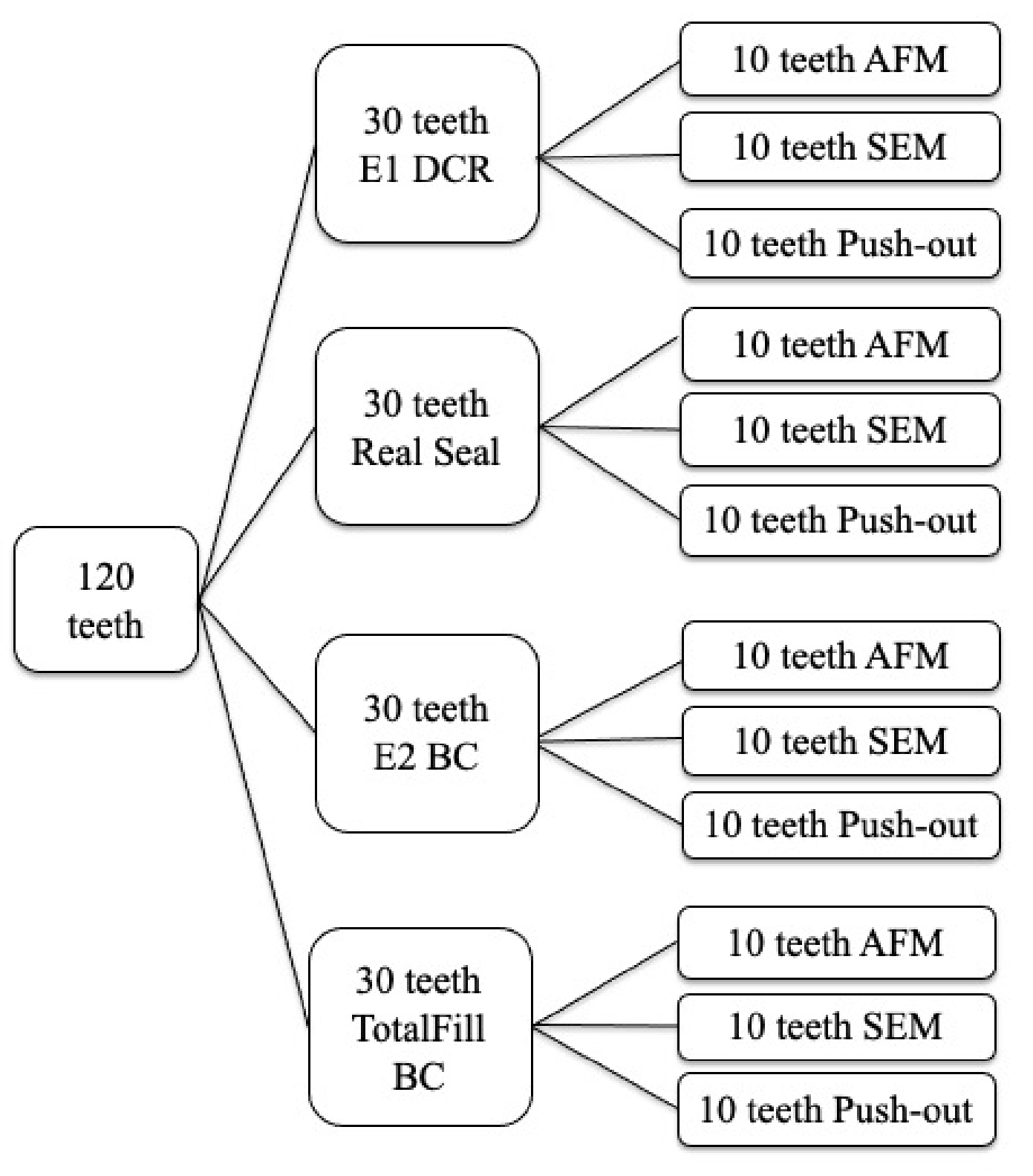
2. Materials and Methods
3. Results
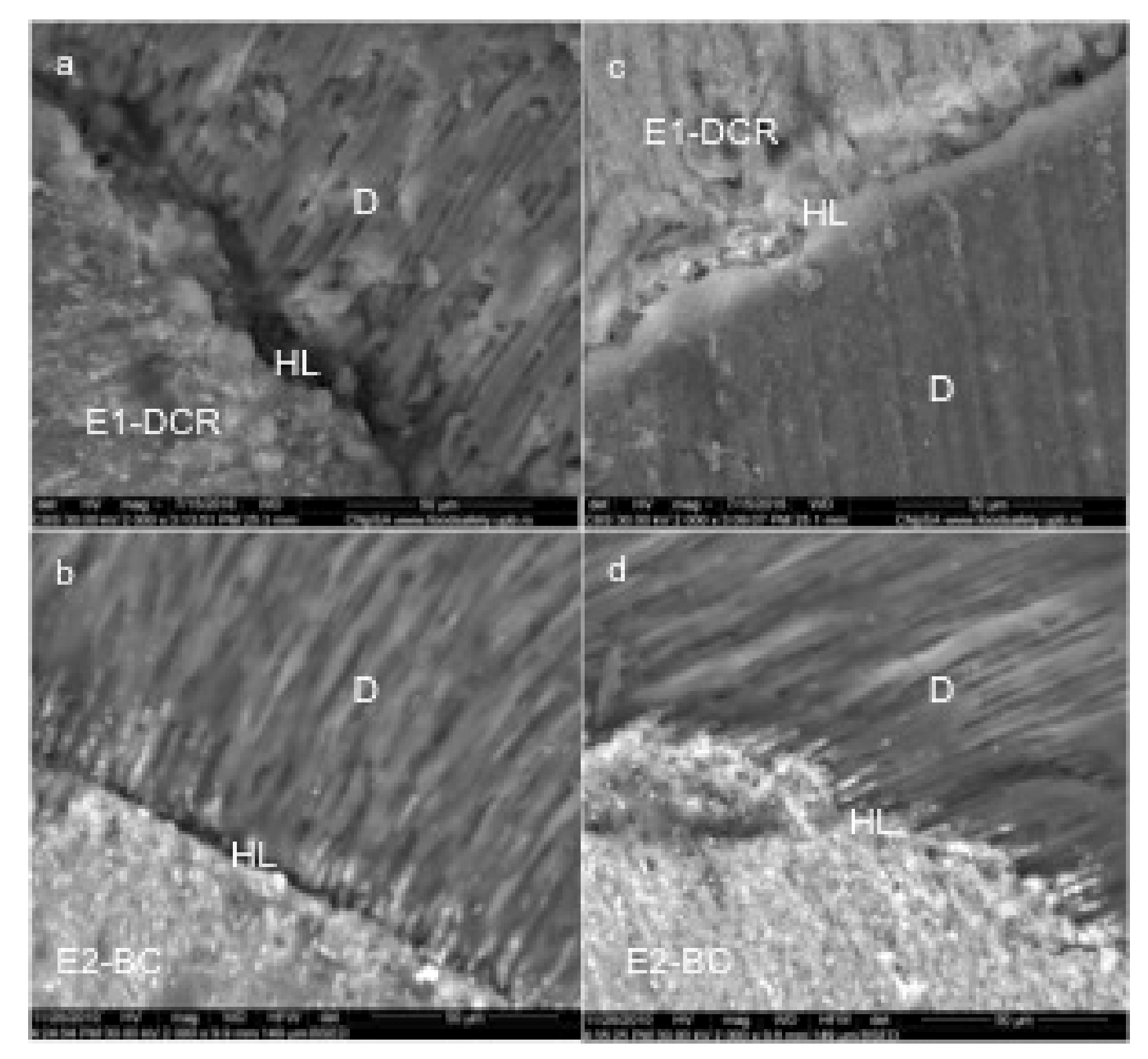
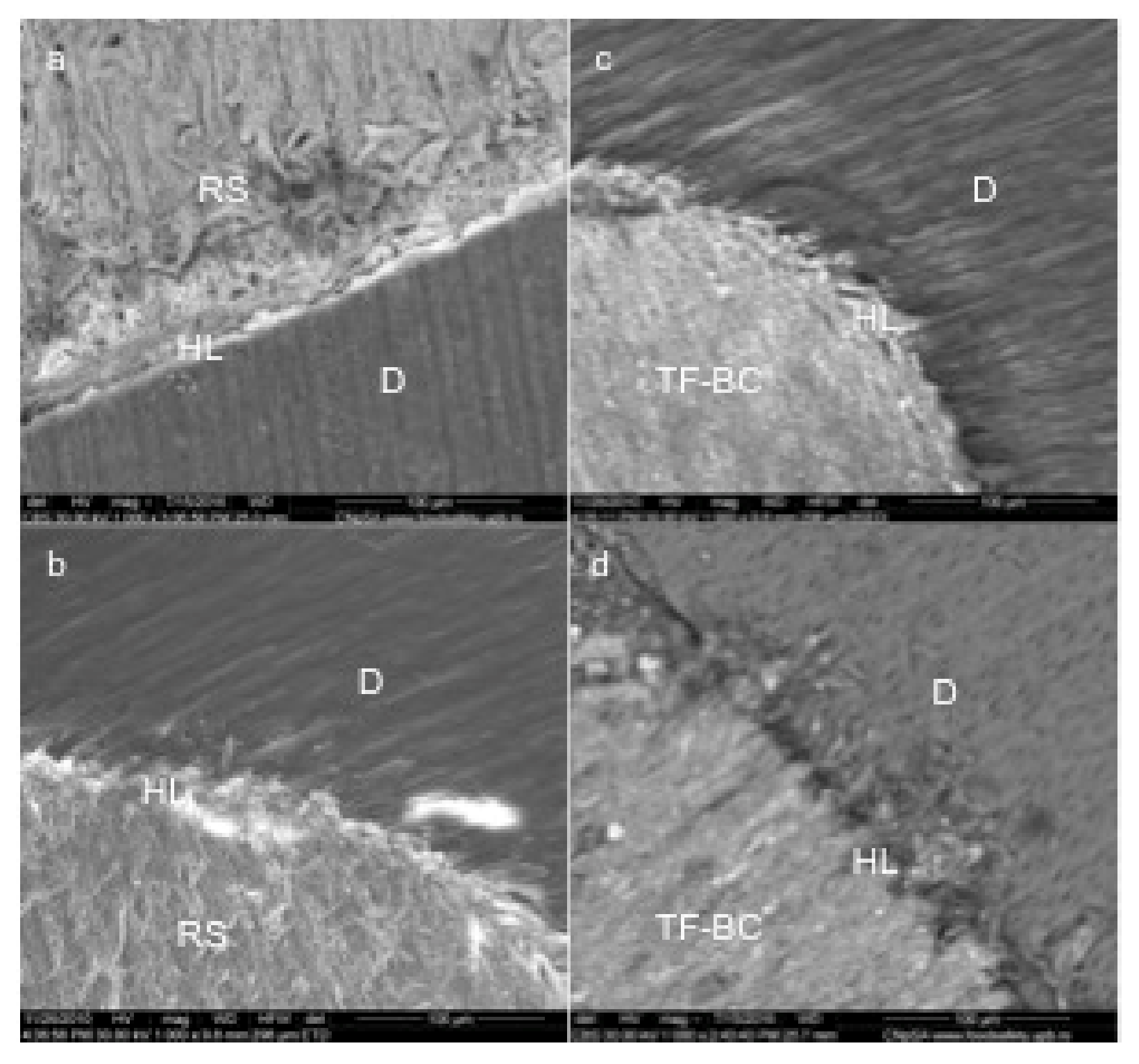
3.1. Scanning Electron Microscopy
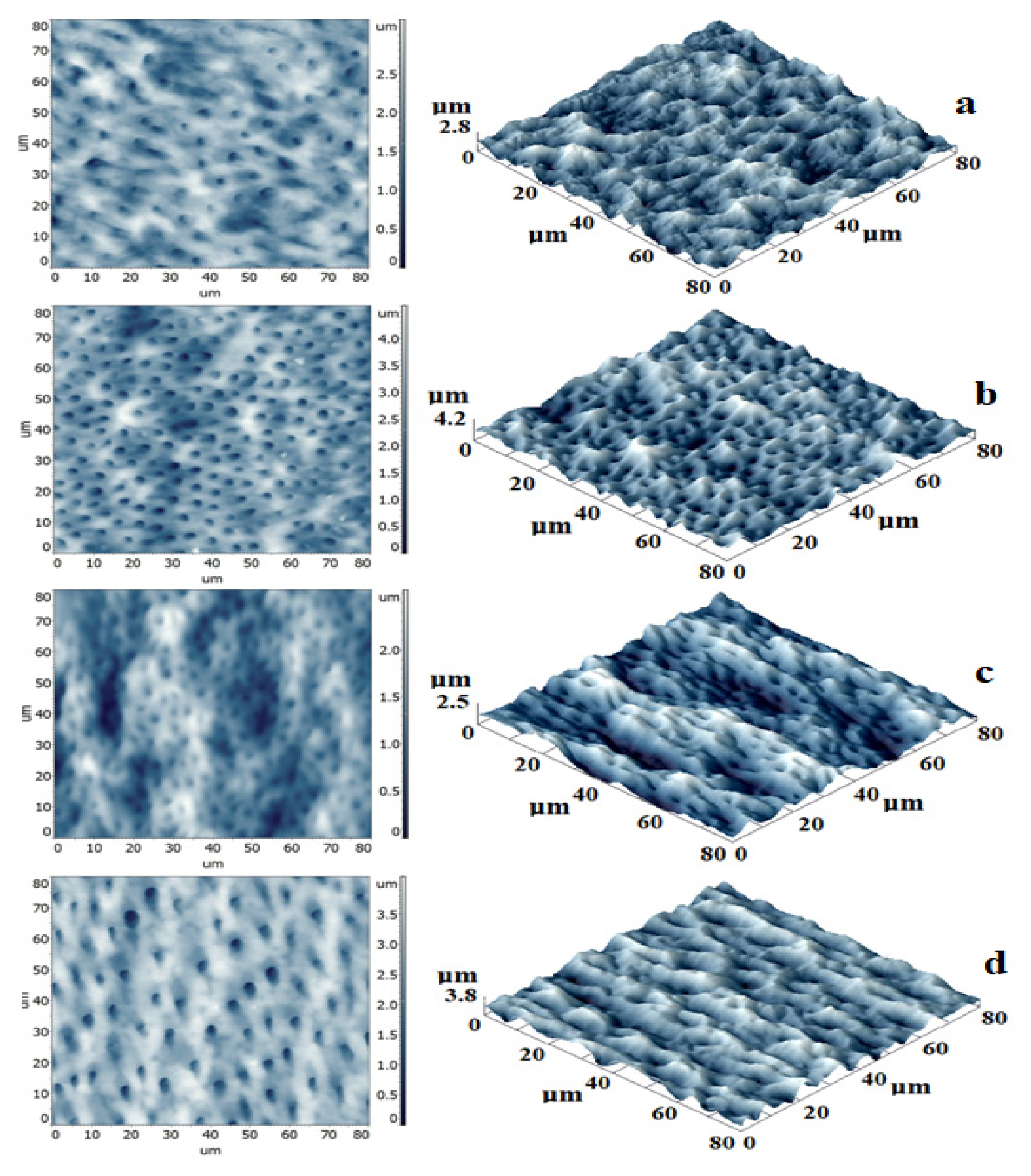
3.2. Atomic Force Microscopy
3.3. FTIR Spectroscopy
3.4. Push-Out Test
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Tay, F.R.; Loushine, R.J.; Lambrechts, P.; Weller, R.N.; Pashley, D.H. Geometric factors affecting dentin bonding in root canals: A theoretical modeling approach. J. Endod. 2005, 31, 584–589. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, R.M.; Pereira, J.C.; Yoshiyama, M.; Pashley, D.H. A review of polymerization contraction: The influence of stress development versus stress relief. Oper. Dent. 1996, 21, 17–24. [Google Scholar] [PubMed]
- Hrab, D.; Pastrav, O.; Chisnoiu, R.; Prodan, D.; Badea, M.E.; Chisnoiu, A. The effectiveness of photodynamic therapy in endodontic sealer adhesion. JOAM 2016, 18, 899–903. [Google Scholar]
- Lohbauer, U.; Nikolaenko, S.A.; Petschelt, A.; Frankenberger, R. Resin tags do not contribute to dentin adhesion in self-etching adhesives. J. Adhes. Dent. 2008, 10, 97–103. [Google Scholar] [PubMed]
- Oliveira, S.S.; Pugach, M.K.; Hilton, J.F.; Watanabe, L.G.; Marshall, S.J.; Marshall, G.W., Jr. The influence of the dentin smear layer on adhesion: A self-etching primer vs. a total-etch system. Dent. Mater. 2003, 19, 758–767. [Google Scholar] [CrossRef]
- Reis, A.; Grandi, V.; Carlotto, L. Effect of smear layer thickness and acidity of selfetching solutions on early and long-term bond strength to dentin. J. Dent. 2005, 33, 549–559. [Google Scholar] [CrossRef] [PubMed]
- Babb, B.R.; Loushine, R.J.; Bryan, T.E. Bonding of self-adhesive (self-etching) root canal sealers to radicular dentin. J. Endod. 2009, 35, 578–582. [Google Scholar] [CrossRef]
- Miyasaka, K.; Nakabayashi, N. Combination of EDTA conditioner and phenyl-P/HEMA self-etching primer for bonding to dentin. Dent. Mater. 1999, 15, 153–157. [Google Scholar] [CrossRef]
- Chisnoiu, R.; Moldovan, M.; Chisnoiu, A.; Hrab, D.; Rotaru, D.; Păstrav, O.; Delean, A. Comparative apical sealing evaluation of two bioceramic endodontic sealers. Med. Pharm Rep. 2019, 92, S55–S60. [Google Scholar] [CrossRef]
- Best, S.M.; Porter, A.E.; Thian, E.S.; Huang, J. Bioceramics: Past, Present and for the Future. J. Eur. Ceram. Soc. 2008, 1, 1319–1327. [Google Scholar] [CrossRef]
- Moldovan, M.; Prejmerean, C.; Colceriu, A.; Tamas, C.; Furtos, G.; Prodan, D.; Trif, M.; Alb, C.; Neamt, S.; Popescu, V. Effect of coupling agents on the local mechanical properties of bioactive dental composites. JOAM 2007, 9, 3415. [Google Scholar]
- Gurgel-Filho, E.D.; Lima, F.C.; Saboia, V.D.P.A.; de Souza Coutinho-Filho, T.; de Almeida Neves, A.; da Silva, E.J. Push-out bond strength of a self-adhesive resin cement used as endodontic sealer. Restor. Dent. Endod. 2014, 39, 282–287. [Google Scholar] [CrossRef]
- Mohammadian, F.; Farahanimastary, F.; Dibaji, F.; Kharazifard, M.J. Scanning Electron Microscopic Evaluation of the Sealer-Dentine Interface of Three Sealers. Iran. Endod. J. 2017, 12, 38–42. [Google Scholar]
- Ballullaya, S.V.; Vinay, V.; Thumu, J.; Devalla, S.; Bollu, I.P.; Balla, S. Stereomicroscopic Dye Leakage Measurement of Six Different Root Canal Sealers. J. Clin. Diagn. Res. 2017, 11, ZC65–ZC68. [Google Scholar] [CrossRef]
- Chisnoiu, R.; Moldovan, M.; Păstrav, O.; Delean, A.; Chisnoiu, A.M. The influence of three endodontic sealers on bone healing: An experimental study. Folia Morphol. 2016, 75, 14–20. [Google Scholar] [CrossRef][Green Version]
- Van Meerbeeck, B.; Vargas, M.; Ionue, S. Microscopy investigations: Techniques, results, limitations. Am. J. Dent. 2000, 13, 3–18. [Google Scholar]
- Zhang, W.; Li, Z.; Peng, B. Assessment of a new root canal sealer’s apical sealing ability. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2009, 107, 79–82. [Google Scholar] [CrossRef]
- Kim, Y.K.; Grandini, S.; Ames, M.; Gu, L.S.; Kim, S.K.; Pashley, D.H.; Gutmann, J.L.; Tay, F.R. Critical Review on Methacrylate Resin-based Root CanalSealers. J. Endod. 2010, 36, 383–399. [Google Scholar] [CrossRef]
- Ayad, M.F.; Bahannan, S.A.; Rosenstiel, S.F. Morphological characteristics of the interface between resin composite and glass-ionomer cement to thin-walled roots; A microscopic investigation. Am. J. Dent. 2010, 23, 103–107. [Google Scholar]
- Trache, A.; Meininger, G.A. Atomic force microscopy (AFM). Curr. Protoc. Microbiol. 2008, 2, C2. [Google Scholar] [CrossRef]
- Mishra, P.; Sharma, A.; Mishra, S.; Gupta, M. Push-out bond strength of different endodontic obturation material at three different sites in-vitro study. J. Clin. Exp. Dent. 2017, 9, e733–e737. [Google Scholar] [CrossRef][Green Version]
- Candeiro, G.T.; Correia, F.C.; Duarte, M.A.; Ribeiro-Siqueira, D.C.; Gavini, G. Evaluation of radiopacity, pH, release of calcium ions, and flow of a bioceramic root canal sealer. J. Endod. 2012, 38, 842–845. [Google Scholar] [CrossRef]
- Chisnoiu, R.; Pastrav, O.; Delean, A.; Prodan, D.; Boboia, S.; Moldovan, M.; Chisnoiu, A. Push-out Bond Strengths of Three Different Endodontic Sealers A comparative study. Mat. Plast. 2015, 6, 239–242. [Google Scholar]
- Yap, W.Y.; Ab Aziz, Z.A.C.; Azami, N.H.; Al-Haddad, A.Y.; Khan, A.A. An in vitro Comparison of Bond Strength of Different Sealers/Obturation Systems to Root Dentin Using the Push-Out Test at 2 Weeks and 3 Months after Obturation. Med. Princ. Pract. 2017, 26, 464–469. [Google Scholar] [CrossRef]
- Monticelli, F.; Osorio, R.; Mazzitelli, C.; Ferrari, M.; Toledano, M. Limited decalcification/ diffusion of self-adhesive cements into dentin. J. Dent. Res. 2008, 87, 74–979. [Google Scholar] [CrossRef]
- Zmener, O.; Pameiher, C.H.; Serrano, S.A.; Vidueira, M.; Macchi, R.L. Significance of moist root canal dentin with the use of methacrylate-based endodontic sealers: An in vitro coronal dye leakage study. J. Endod. 2008, 34, 76–79. [Google Scholar] [CrossRef]
- Steier, L.; Figueiredo, J.A.; Belli, S. Comparison of the interface dentin-endodontic sealer using two SEM magnifications. Rev. Odonto Cienc. 2010, 25, 296–299. [Google Scholar] [CrossRef]
- Mukhtar-Fayyad, D. Cytocompatibility of new bioceramic-based materials on human fibroblast cells (MRC-5). Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2011, 112, e137–e142. [Google Scholar] [CrossRef]
- Zhang, W.; Li, Z.; Peng, B. Ex vivo cytotoxicity of a new calcium silicate-based canal filling material. Int. Endod. J. 2010, 43, 769–774. [Google Scholar] [CrossRef]
- Santos-Junior, A.O.; Tanomaru-Filho, M.; Pinto, J.C.; Tavares, K.I.M.C.; Torres, F.F.E.; Guerreiro-Tanomaru, J.M. Effect of obturation technique using a new bioceramic sealer on the presence of voids in flattened root canals. Braz. Oral Res. 2021, 35, e028. [Google Scholar] [CrossRef]
- Atmeh, A.R.; AlShwaimi, E. The effect of heating time and temperature on epoxy resin and calcium silicate-based endodontic sealers. J. Endod. 2017, 43, 2112–2118. [Google Scholar] [CrossRef] [PubMed]
- Chen, B.; Haapasalo, M.; Mobuchon, C.; Li, X.; Ma, J.; Shen, Y. Cytotoxicity and the effect of temperature on physical properties and chemical composition of a new calcium silicate-based root canal sealer. J. Endod. 2020, 46, 531–538. [Google Scholar]
- Lawson, M.S.; Loushine, B.; Mai, S. Resistance of a 4-META- containing, methacrylate-based sealer to dislocation in root canals. J. Endod. 2008, 34, 833. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.M.; Shen, Y.; Zheng, W.; Zheng, Y.; Haapasalo, M. Physical properties of 5 root canal sealers. J. Endod. 2013, 39, 1281.e6. [Google Scholar] [CrossRef]
- Zoufan, K.; Komabayashi, T.; Safavi, K.E.; Zhu, Q. Cytotoxicity evaluation of Gutta Flow and Endo Sequence BC sealers. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2011, 112, 657–661. [Google Scholar] [CrossRef]
- Al-Bakhsh, B.A.J.; Shafiei, F.; Hashemian, A.; Shekofteh, K.; Bolhari, B.; Behroozibakhsh, M. In-vitro bioactivity evaluation and physical properties of an epoxy-based dental sealer reinforced with synthesized fluorine-substituted hydroxyapatite, hydroxyapatite and bioactive glass nanofillers. Bioact. Mater. 2019, 4, 322–333. [Google Scholar] [CrossRef]
- Lin, X.Y.; Fan, H.S.; Li, X.D.; Tang, M.; Zhang, X.D. Evaluation of bioactivity and cytocompatibility of nano-hydroxyapatite/collagen composite in vitro. Key Eng. Mater. 2005, 284, 553–556. [Google Scholar] [CrossRef]
- Korkut, E.; Torlak, E.; Altunsoy, M. Antimicrobial and mechanical properties of dental resin composite containing bioactive glass. J. Appl. Biomater. Funct. Mater. 2006, 14, e296–e301. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dentinal Tubules Diameter, µm | Sealer Width nm | p | ||||
|---|---|---|---|---|---|---|
| Sample | Minimum | Intermediary | Maximum | Mean | ||
| E1-DCR | 1.45 | 2.90 | 3.87 | 2.47 | 125 | 0.001 |
| E2-BC | 2.03 | 3.05 | 3.39 | 2.82 | 85 | |
| RS | 1.21 | 1.45 | 2.18 | 1.61 | 69 | |
| TF-BC | 1.69 | 3.05 | 3.92 | 2.88 | 55 | |
| Sample | I C = O~1717 cm−1 | I C = C~1636 cm−1 | I Si-O-Si 1040 cm−1 | I C = O/I C = C | I Si-O-Si/I C = C |
|---|---|---|---|---|---|
| E1-DCR hemo | 0.0321 | 0.0076 | 0.12 | 4.223684211 | 15.78947 |
| E1-DCR blood | 0.0362 | 0.0093 | 0.119 | 3.892473118 | 12.7957 |
| E2-BC hemo | 0.1426 | 0.0362 | 0.2991 | 3.939226519 | 8.262431 |
| E2-BC blood | 0.1673 | 0.0207 | 0.2534 | 8.082125604 | 12.24155 |
| Control H | 0.169 | 0.0207 | 0.1965 | 8.164251208 | 9.492754 |
| Control B | 0.2385 | 0.0367 | 0.2743 | 6.498637602 | 7.474114 |
| Mean Bond Strength (MPa) | ||||
|---|---|---|---|---|
| Sample | Median | p | Apical | p |
| E2-BC | 0.9322 ± 0.25 | 0.7 | 1.3096 ± 0.01 | 0.09 |
| RS | 1.0062 ± 0.90 | 0.6524 ± 0.43 | ||
| TF-BC | 1.4367 ± 1.05 | 0.3 | 2.4524 ± 1.15 | 0.01 |
| E1-DCR | 0.8294 ± 0.18 | 0.7177 ± 0.55 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chisnoiu, R.M.; Moldovan, M.; Prodan, D.; Chisnoiu, A.M.; Hrab, D.; Delean, A.G.; Muntean, A.; Rotaru, D.I.; Pastrav, O.; Pastrav, M. In-Vitro Comparative Adhesion Evaluation of Bioceramic and Dual-Cure Resin Endodontic Sealers Using SEM, AFM, Push-Out and FTIR. Appl. Sci. 2021, 11, 4454. https://doi.org/10.3390/app11104454
Chisnoiu RM, Moldovan M, Prodan D, Chisnoiu AM, Hrab D, Delean AG, Muntean A, Rotaru DI, Pastrav O, Pastrav M. In-Vitro Comparative Adhesion Evaluation of Bioceramic and Dual-Cure Resin Endodontic Sealers Using SEM, AFM, Push-Out and FTIR. Applied Sciences. 2021; 11(10):4454. https://doi.org/10.3390/app11104454
Chicago/Turabian StyleChisnoiu, Radu Marcel, Marioara Moldovan, Doina Prodan, Andrea Maria Chisnoiu, Dana Hrab, Ada Gabriela Delean, Alexandrina Muntean, Doina Iulia Rotaru, Ovidiu Pastrav, and Mihaela Pastrav. 2021. "In-Vitro Comparative Adhesion Evaluation of Bioceramic and Dual-Cure Resin Endodontic Sealers Using SEM, AFM, Push-Out and FTIR" Applied Sciences 11, no. 10: 4454. https://doi.org/10.3390/app11104454
APA StyleChisnoiu, R. M., Moldovan, M., Prodan, D., Chisnoiu, A. M., Hrab, D., Delean, A. G., Muntean, A., Rotaru, D. I., Pastrav, O., & Pastrav, M. (2021). In-Vitro Comparative Adhesion Evaluation of Bioceramic and Dual-Cure Resin Endodontic Sealers Using SEM, AFM, Push-Out and FTIR. Applied Sciences, 11(10), 4454. https://doi.org/10.3390/app11104454