Assessing the Energy Demand Reduction in a Surgical Suite by Optimizing the HVAC Operation During Off-Use Periods

 , ,
, ,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
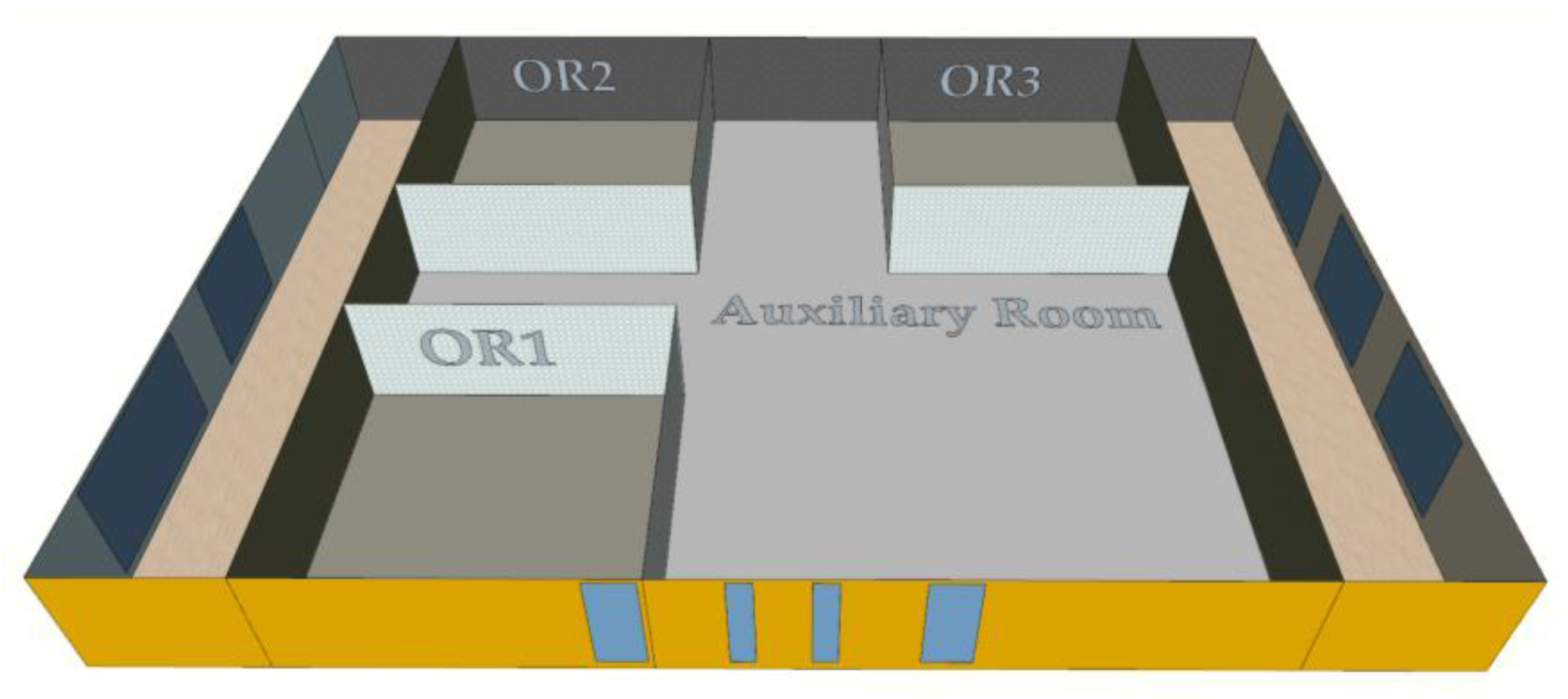
2.1. Description of the Surgical Suite and the Experimental Procedure
2.1.1. The Surgical Suite and Its HVAC System
2.1.2. Experimental Tests
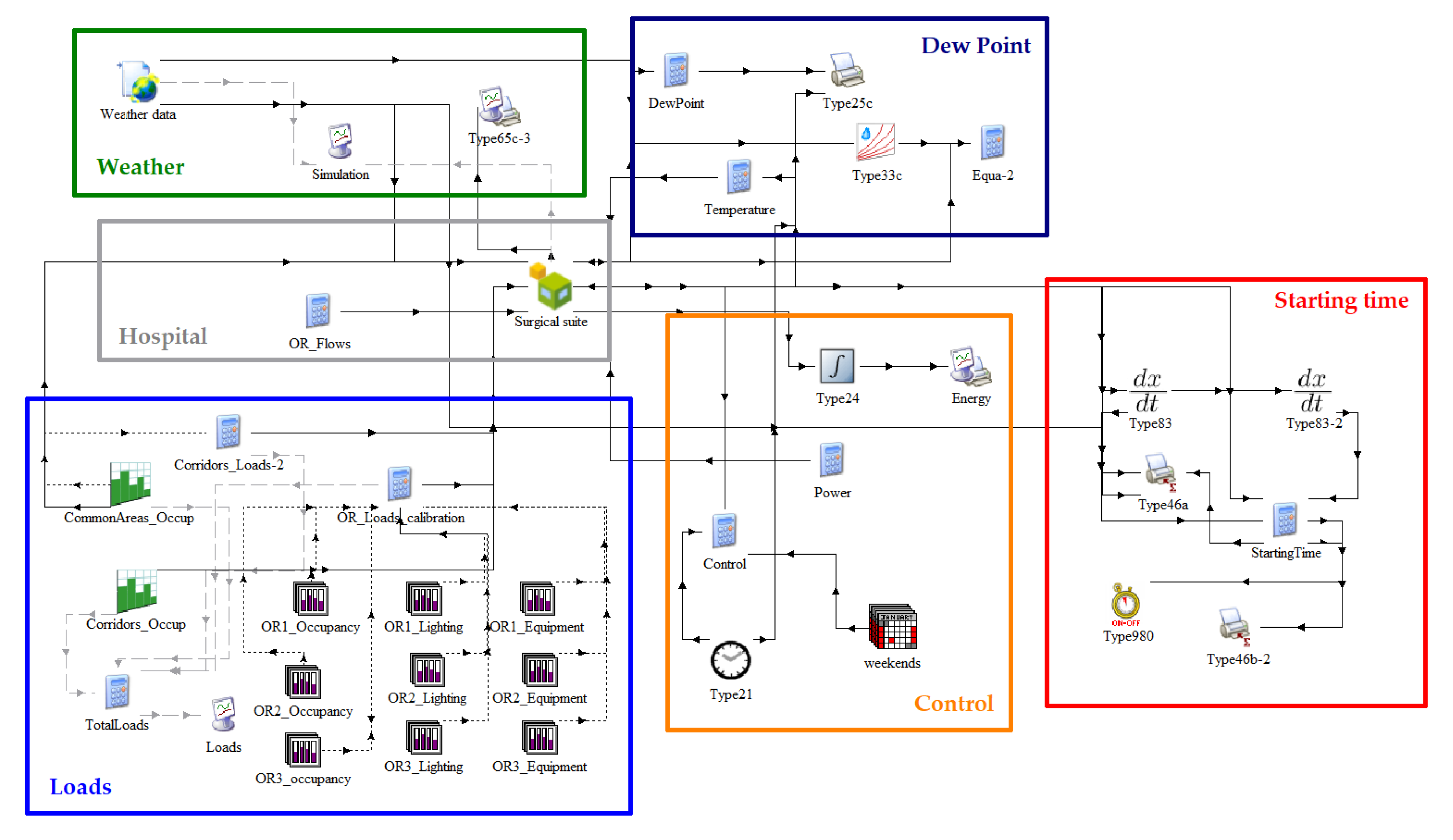
2.2. Simulation Procedure
2.2.1. Dynamic Thermal Model
2.2.2. Calibration and Contrasting
- mean of measured values.
- number of measured data points.
- measured value.
- simulated value.
2.2.3. Simulation of Different Scenarios
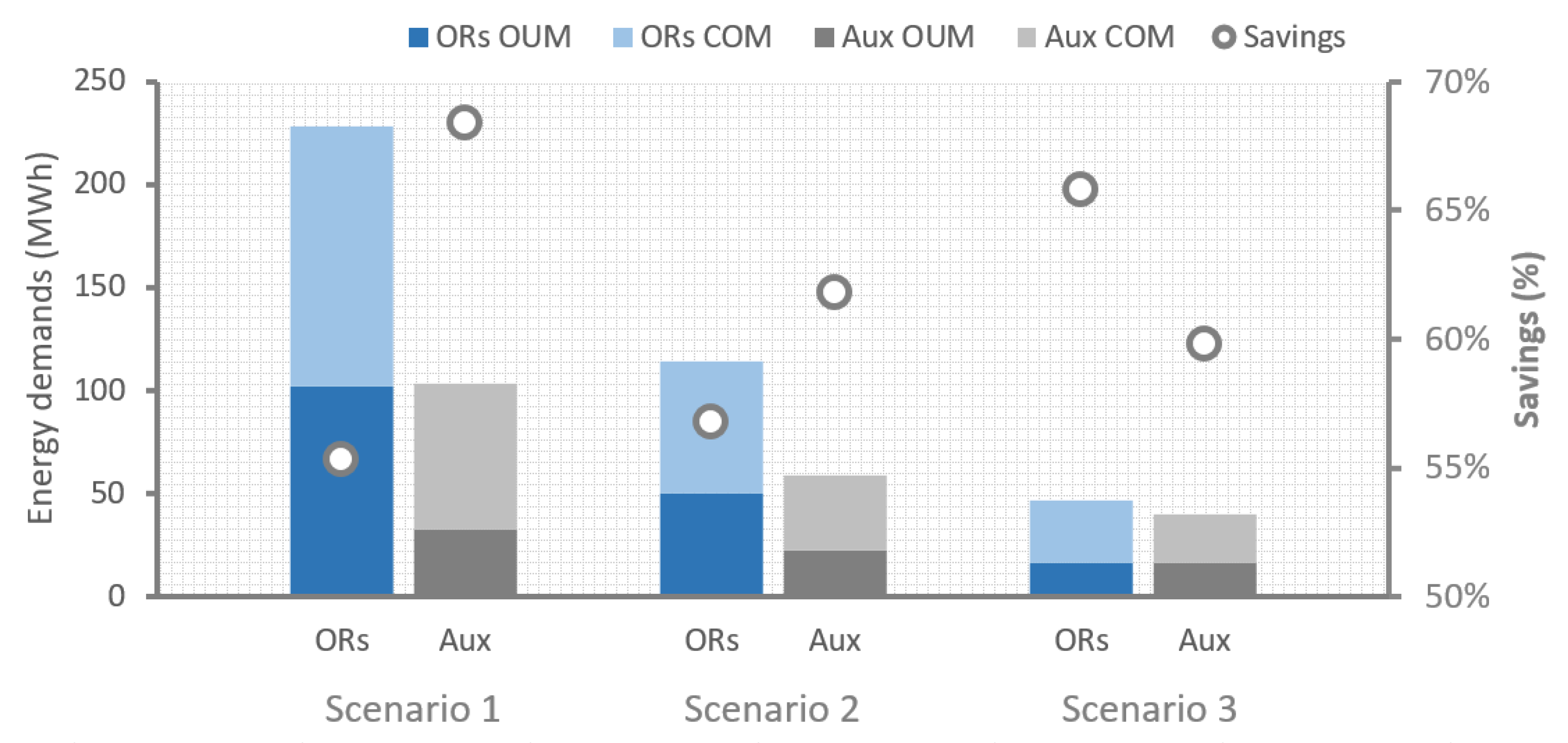
- Scenario 1. Considering the actual design operation rates. This means 21.5 ACH in the ORs and 6 ACH in the ancillary rooms, with 100% outdoor fresh air intake in both cases.
- Scenario 2. Considering a reduction of the 50% of outdoor fresh air. This means 21.5 ACH in the ORs, 6 ACH in the ancillary rooms, but with an air recirculation rate of 50% in both cases.
- Scenario 3. Considering the American standard requirements for ventilation [42]. This means 20 ACH in the ORs with a total fresh air intake of 4 ACH, and 6 ACH in the ancillary rooms with 2 ACH of fresh air.
3. Results and Discussion
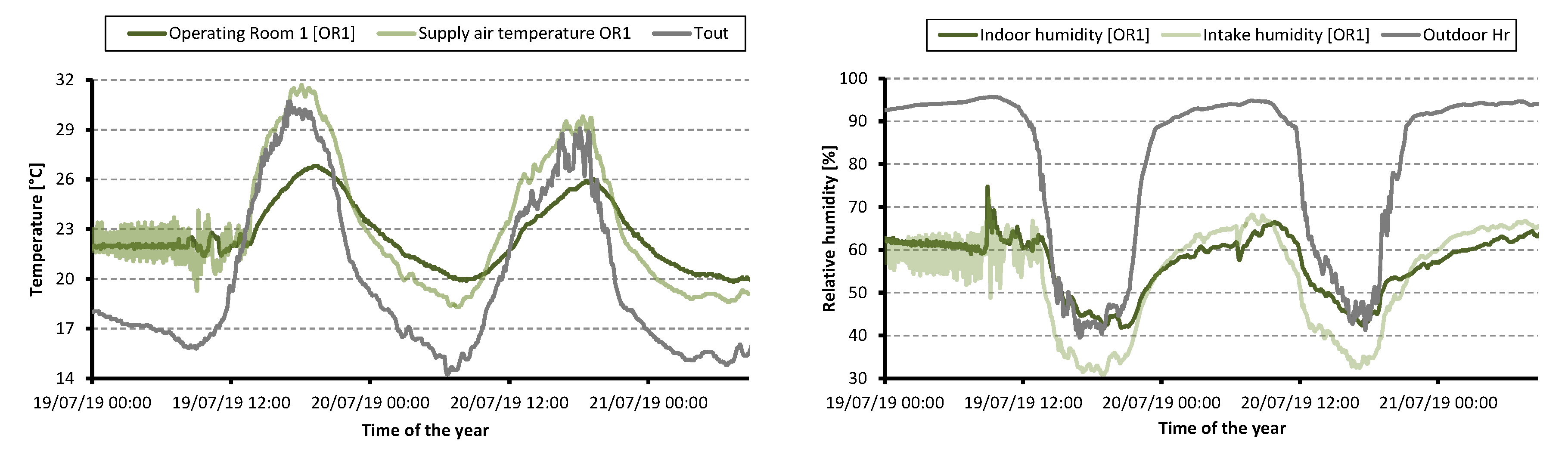
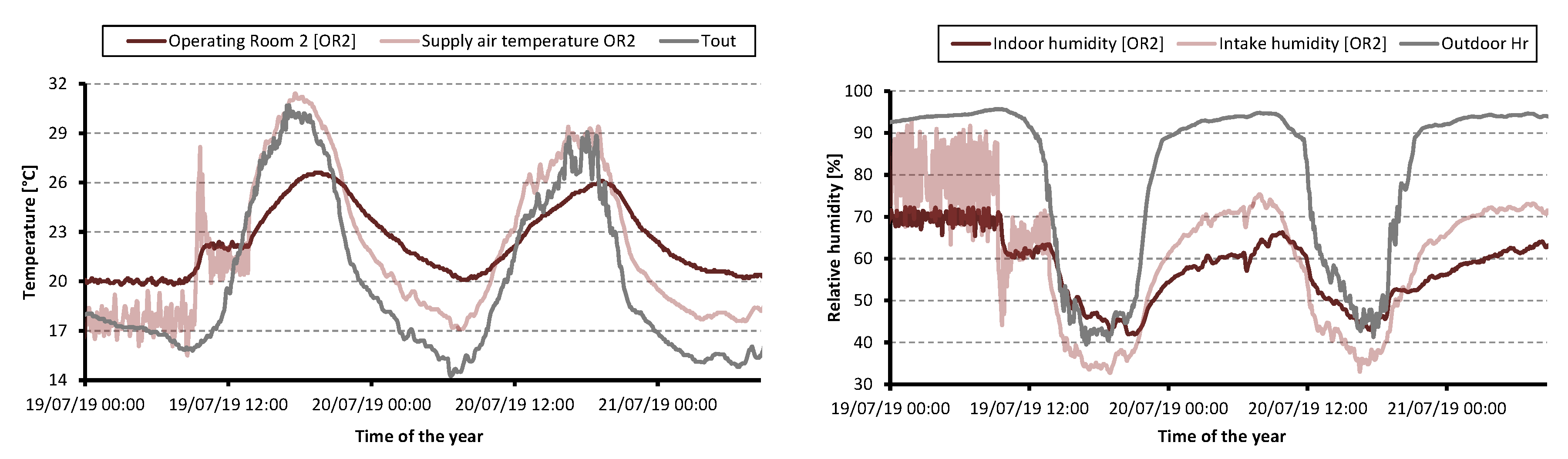
3.1. Assessment of the Experimental Results
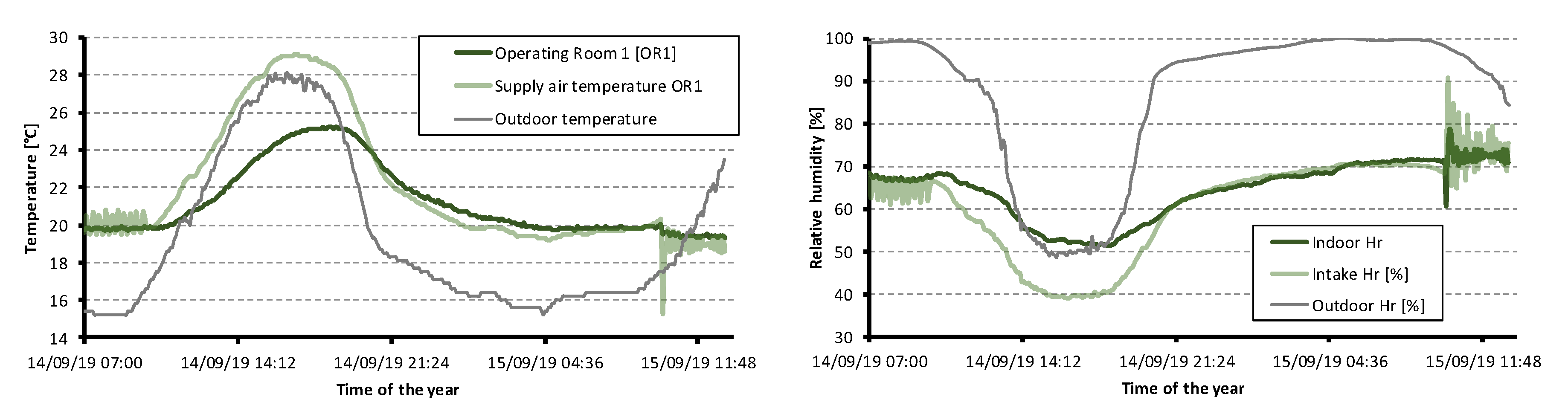
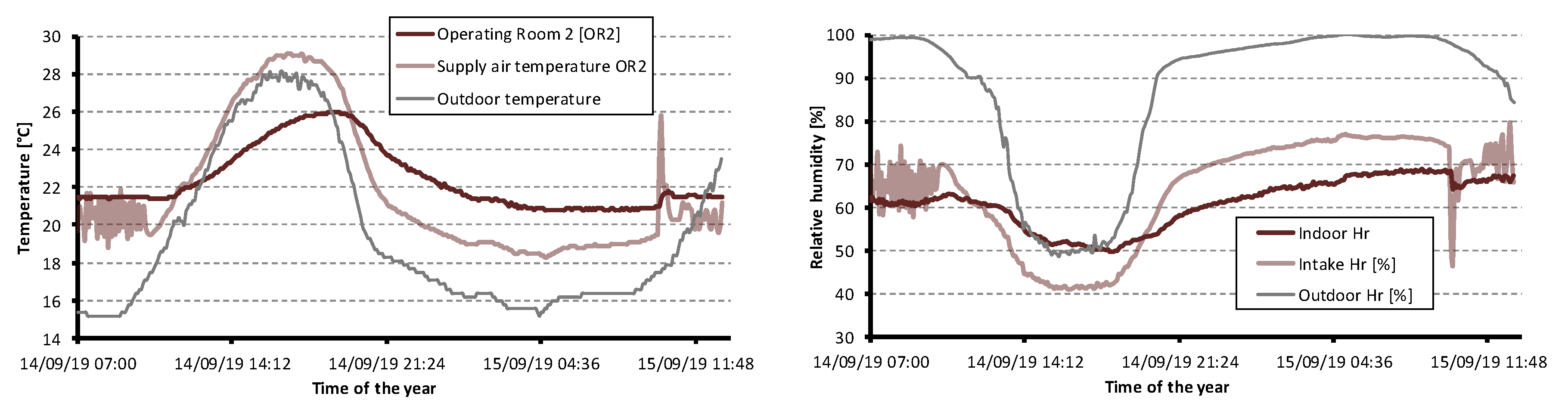
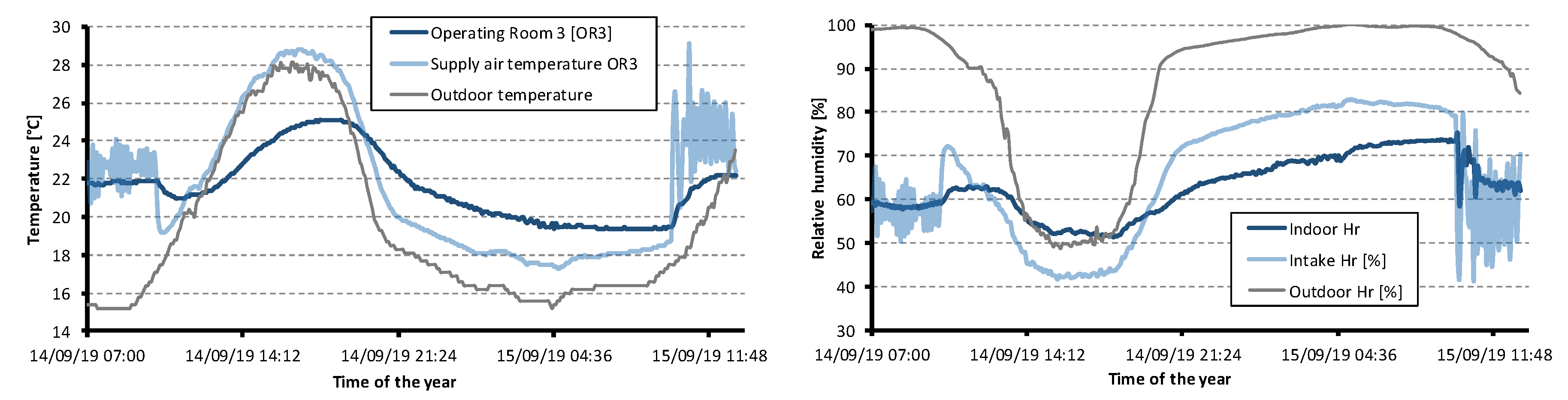
3.1.1. First Data Collection Period
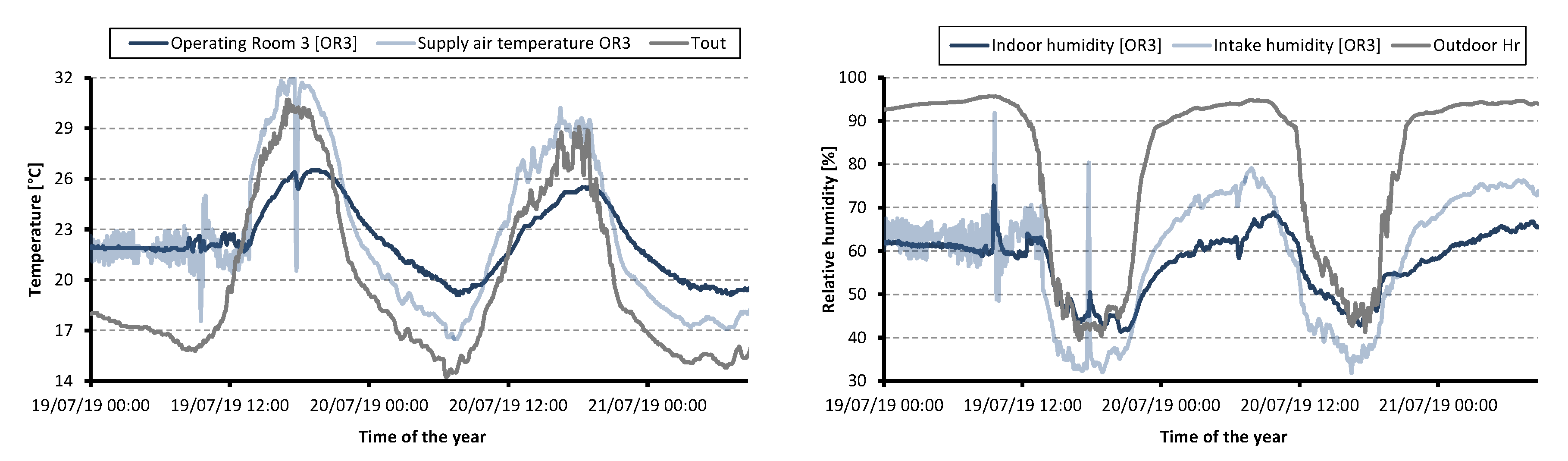
3.1.2. Second Data Collection Period
3.2. Simulation Results of the Calibrated Model
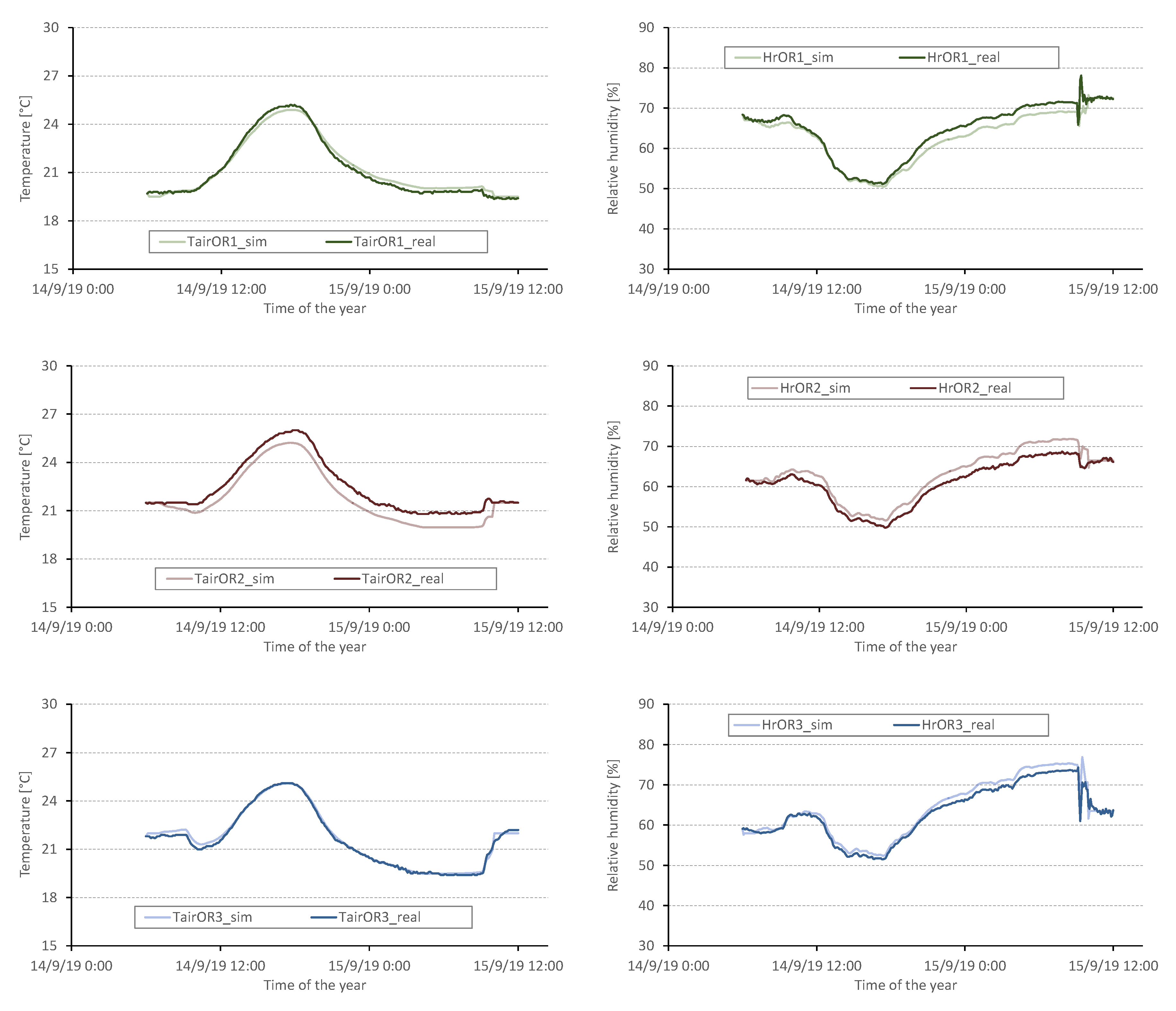
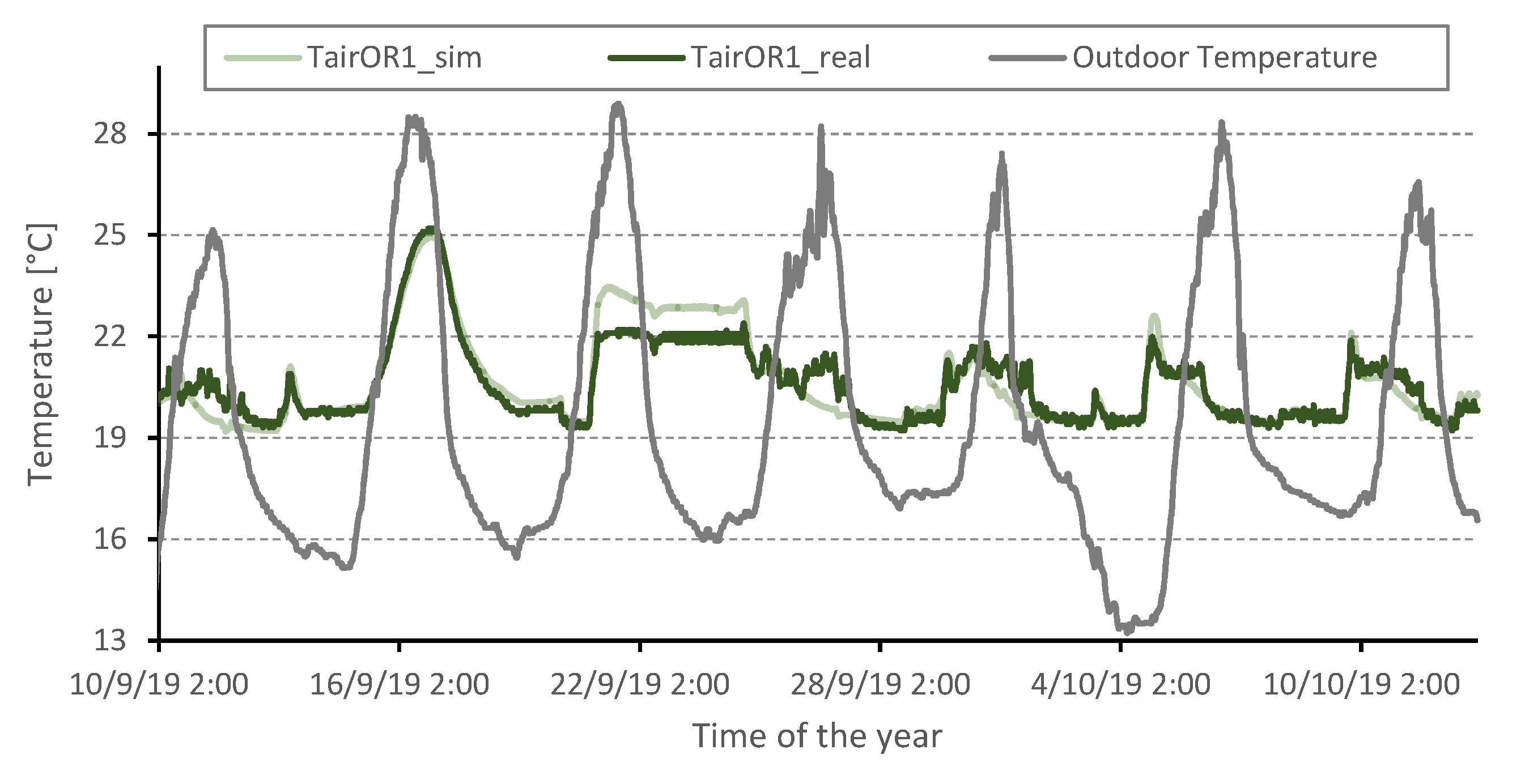
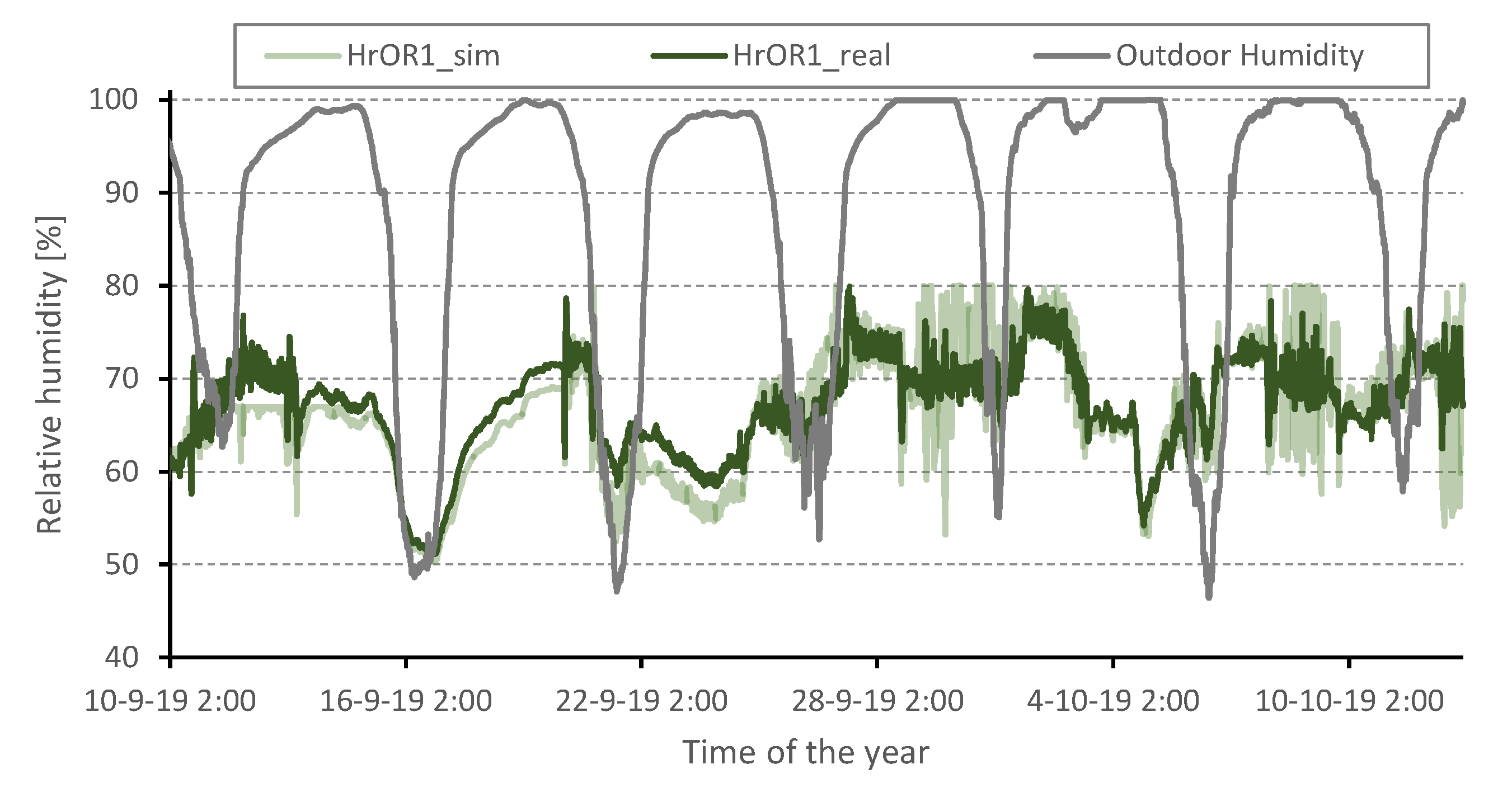
3.2.1. Validation of the Calibrated Model
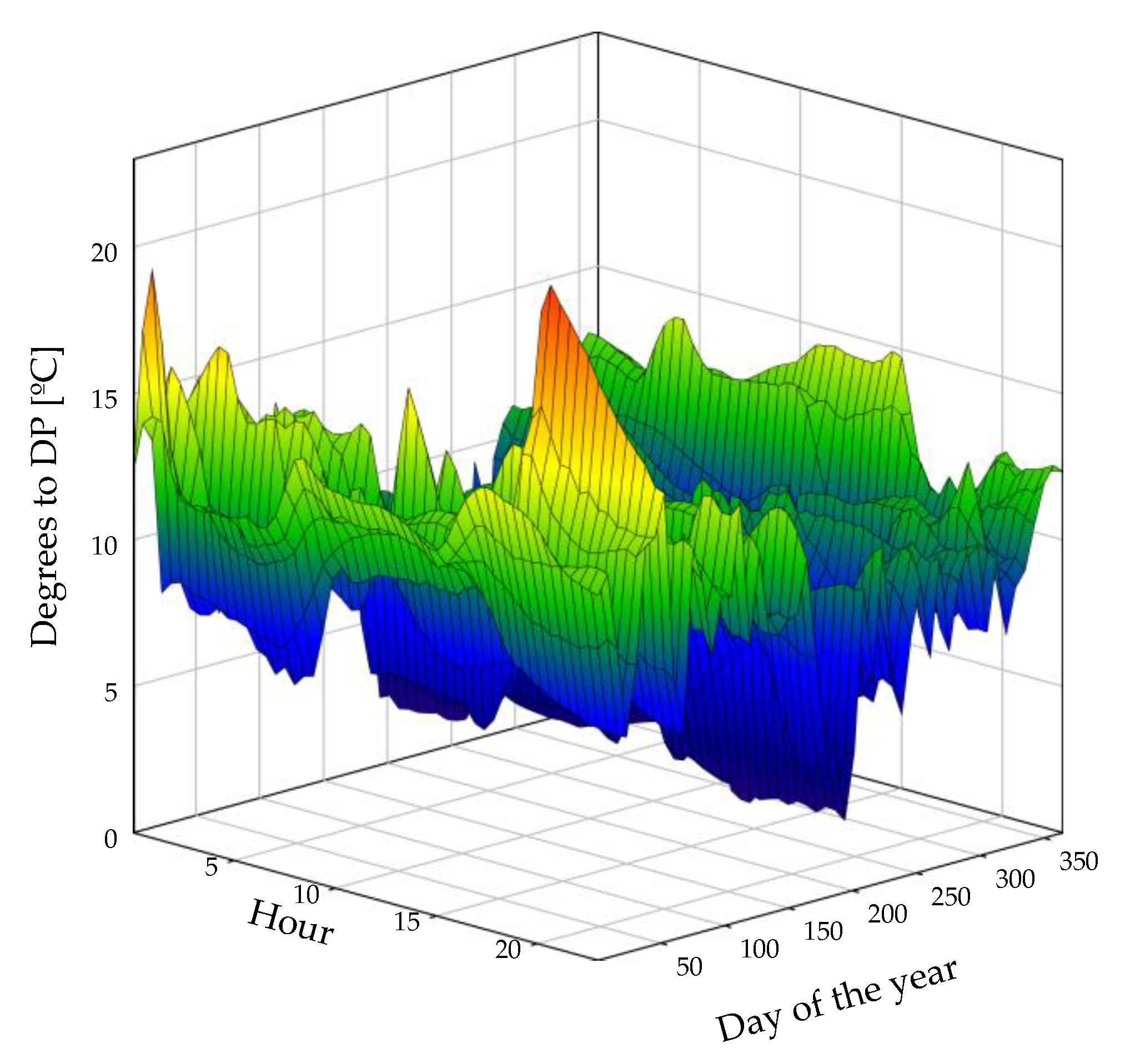
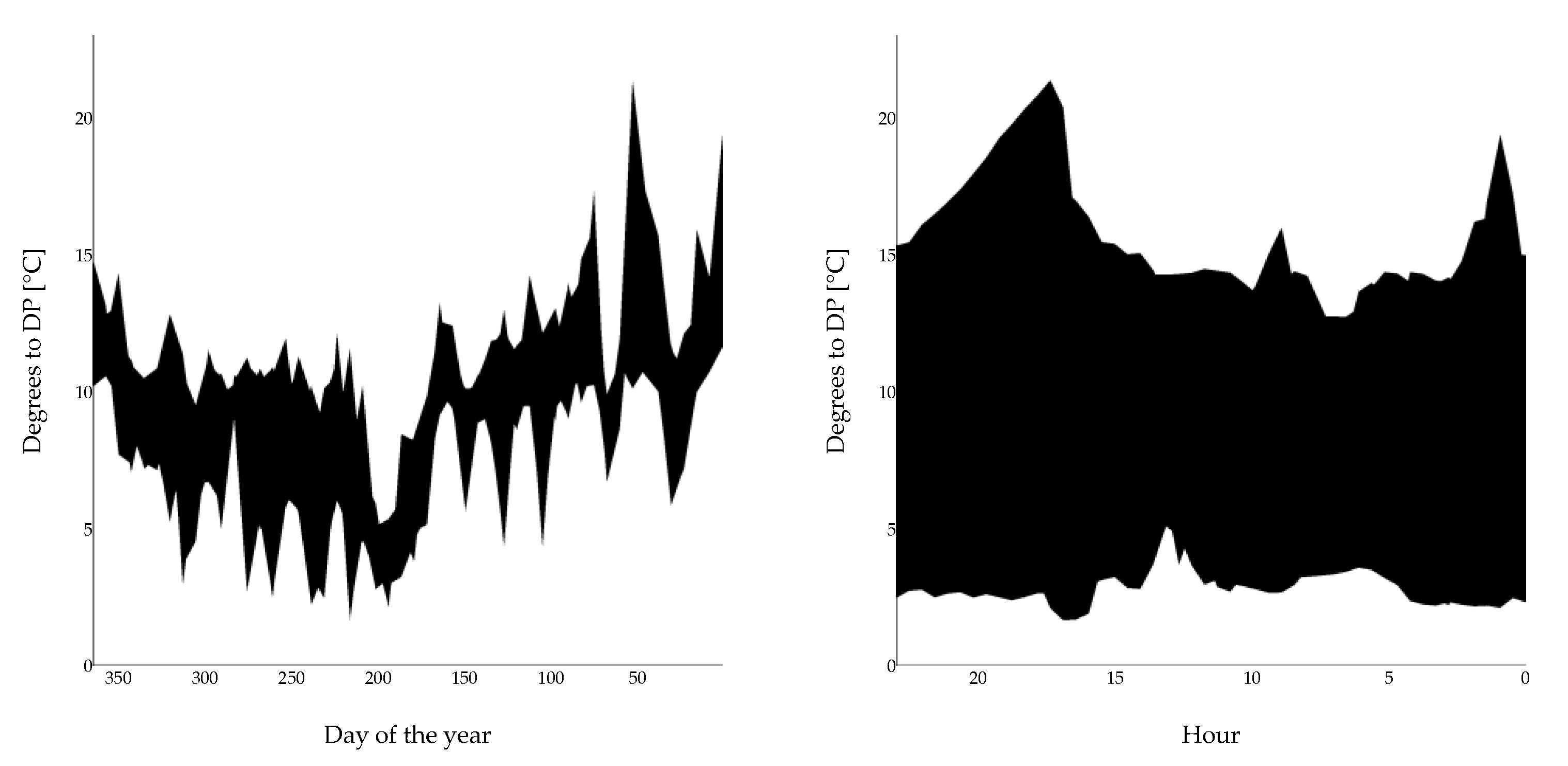
3.2.2. Analysis of the Moisture Condensation Risk
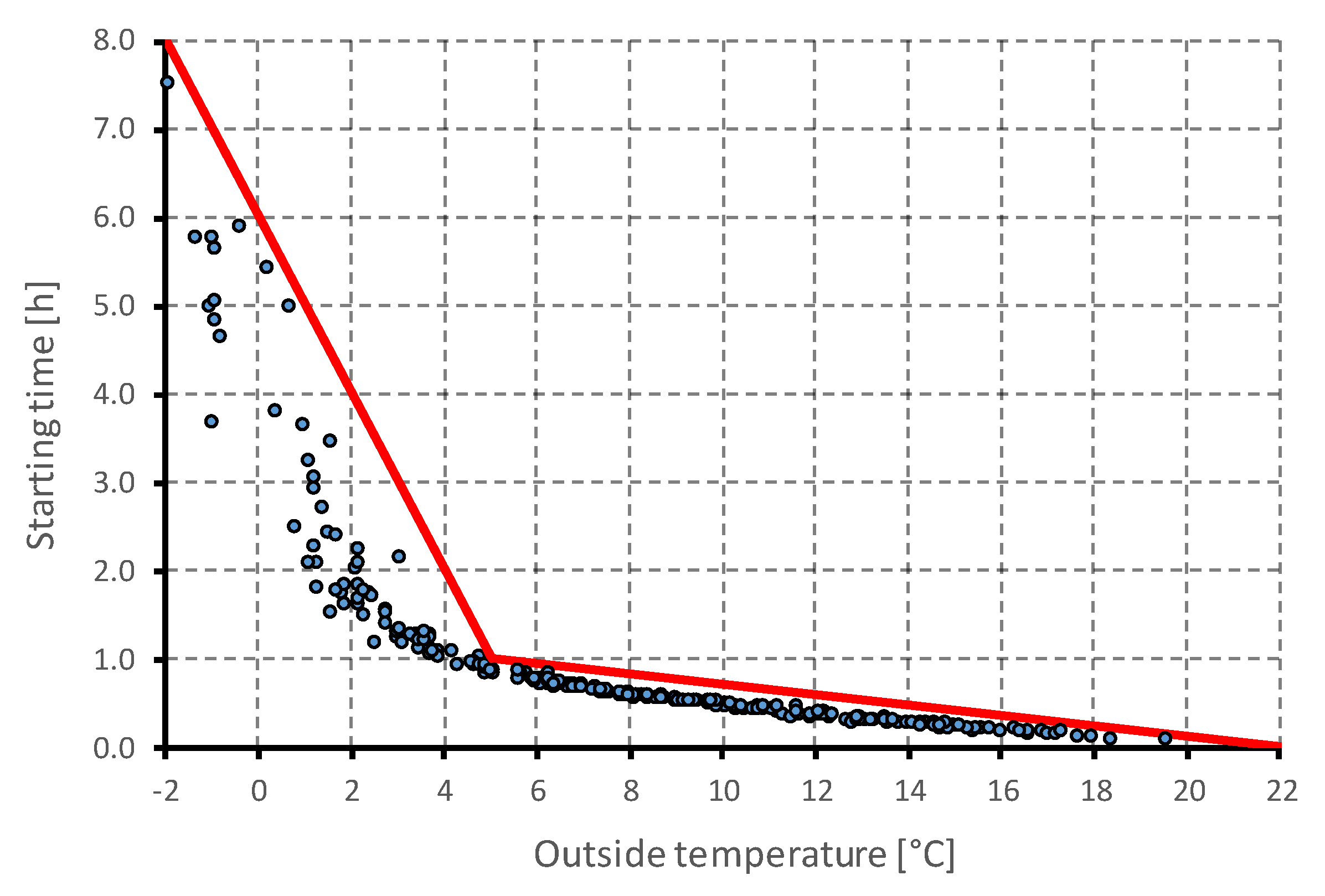
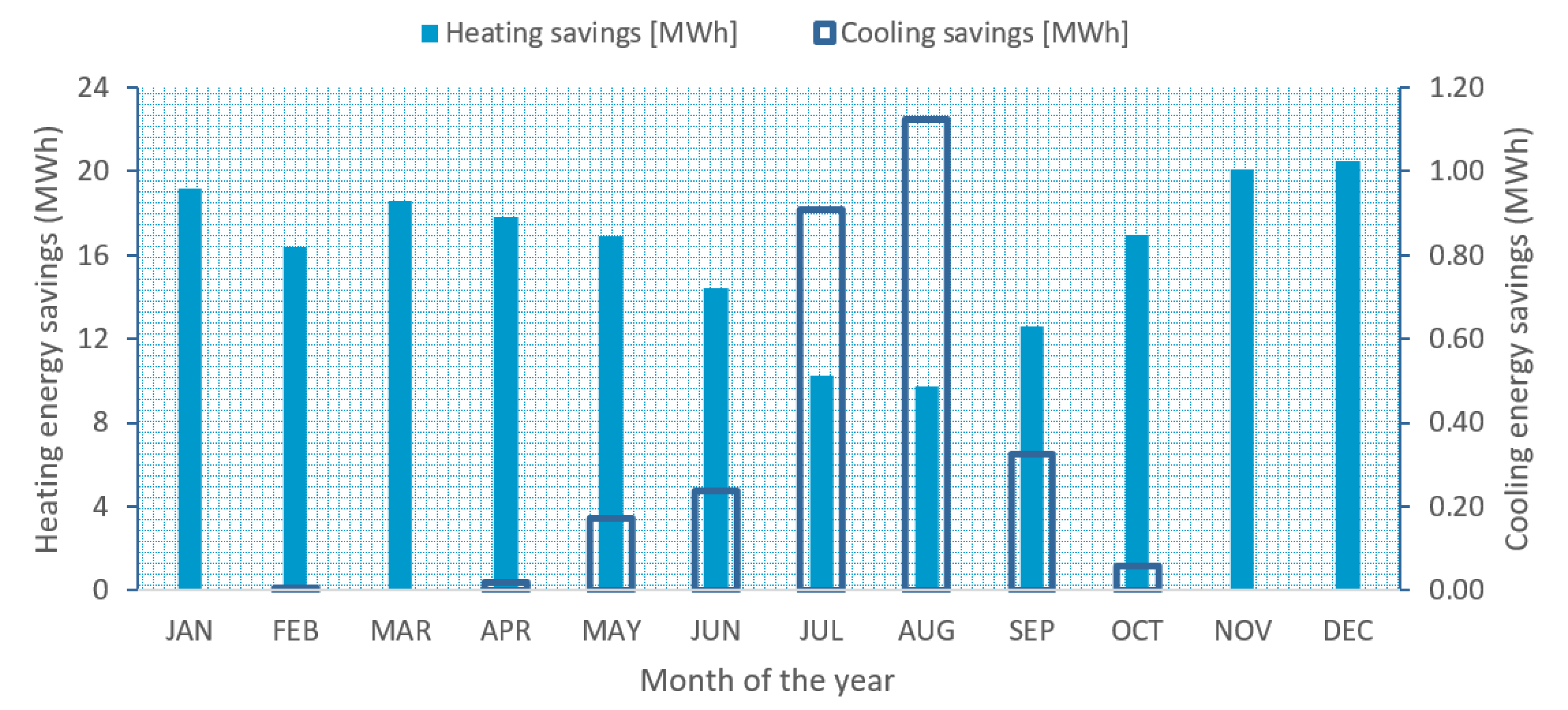
3.2.3. Study of the Air-Conditioned Starting Time
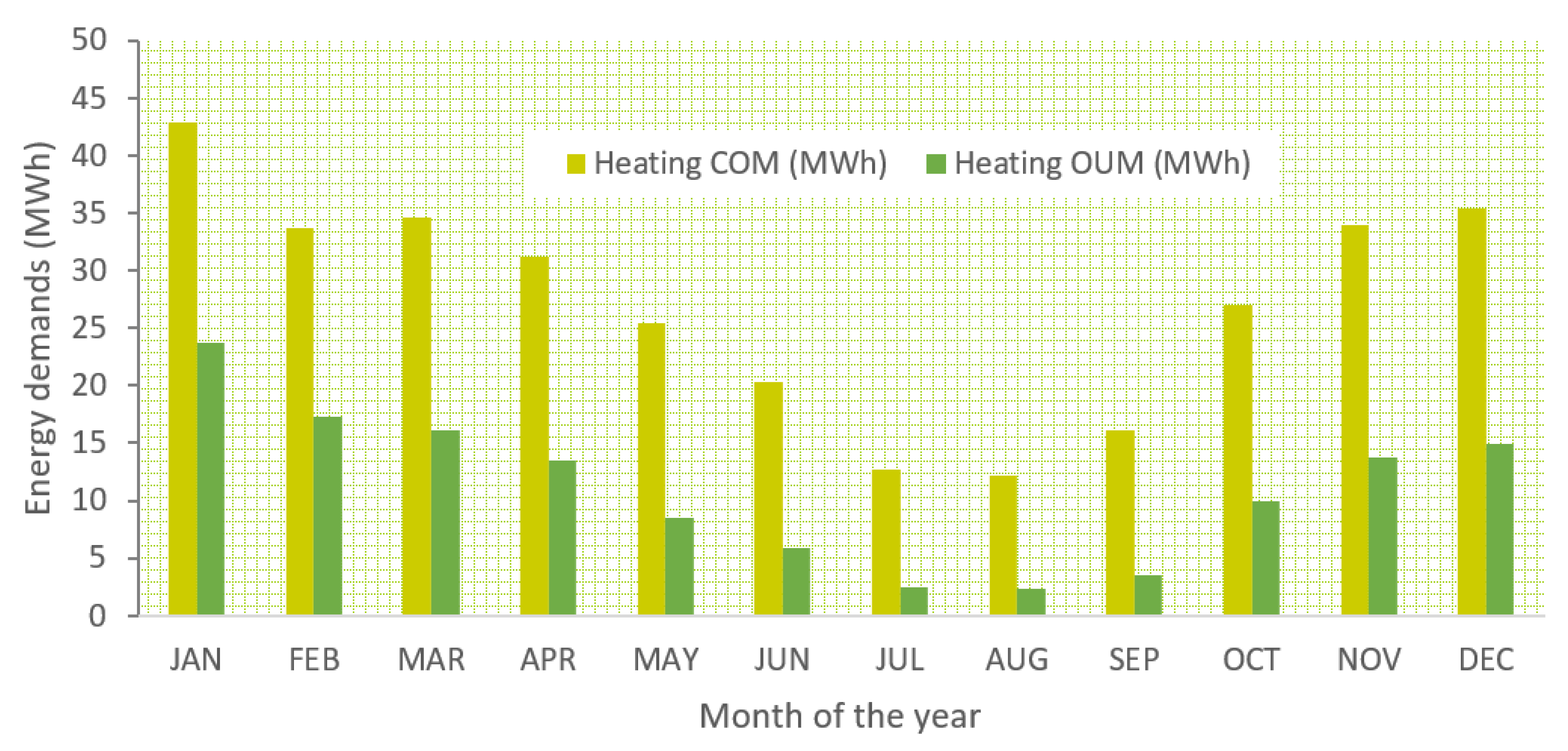
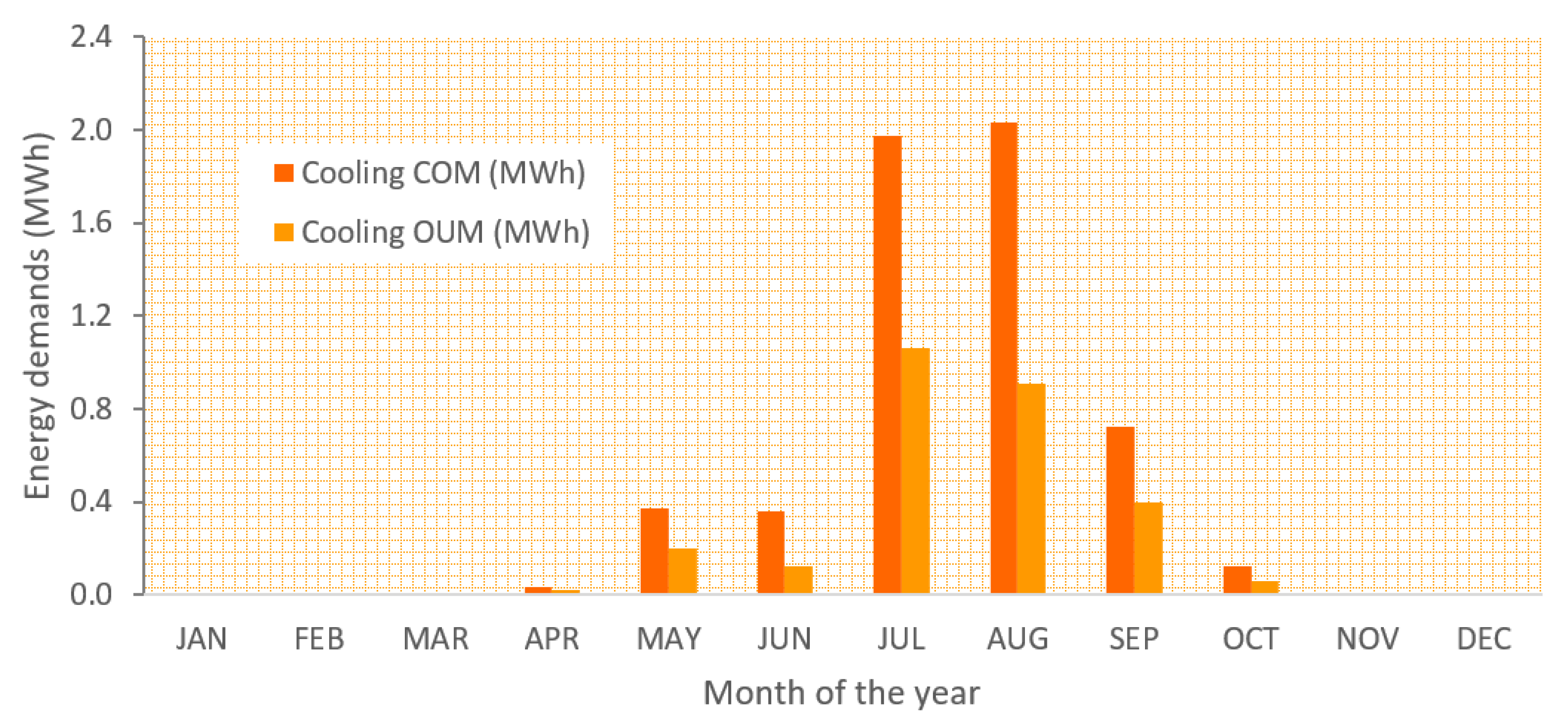
3.2.4. Potential Energy Savings of the Different Ventilation Scenarios
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bawaneh, K.; Nezami, F.G.; Rasheduzzaman, M.; Deken, B. Energy consumption analysis and characterization of healthcare facilities in the United States. Energies 2019, 12, 3775. [Google Scholar] [CrossRef]
- Choudhary, R. Energy analysis of the non-domestic building stock of greater london. Build. Environ. 2012, 51, 243–254. [Google Scholar] [CrossRef]
- González, A.G.; García-Sanz-Calcedo, J.; Salgado, D.R. Evaluation of energy consumption in german hospitals: Benchmarking in the public sector. Energies 2018, 11, 2279. [Google Scholar] [CrossRef]
- González González, A.; García-Sanz-Calcedo, J.; Salgado, D.R. A quantitative analysis of final energy consumption in hospitals in spain. Sustain. Cities Soc. 2018, 36, 169–175. [Google Scholar] [CrossRef]
- García-Sanz-calcedo, J. Study of CO2 emissions from energy consumption in Spanish hospitals. Vibroengineering Procedia 2019, 26, 46–51. [Google Scholar] [CrossRef]
- Capozzoli, A.; Piscitelli, M.S.; Neri, F.; Grassi, D.; Serale, G. A novel methodology for energy performance benchmarking of buildings by means of linear mixed effect model: The case of space and dhw heating of out-patient healthcare centres. Appl. Energy 2016, 171, 592–607. [Google Scholar] [CrossRef]
- Teke, A.; Timur, O. Assessing the energy efficiency improvement potentials of hvac systems considering economic and environmental aspects at the hospitals. Renew. Sustain. Energy Rev. 2014, 33, 224–235. [Google Scholar] [CrossRef]
- Čongradac, V.; Prebiračević, B.; Jorgovanović, N.; Stanišić, D. Assessing the energy consumption for heating and cooling in hospitals. Energy Build. 2012, 48, 146–154. [Google Scholar] [CrossRef]
- Ahmed, T.M.F.; Rajagopalan, P.; Fuller, R. A classification of healthcare facilities: Toward the development of energy performance benchmarks for day surgery centers in australia. Health Environ. Res. Des. J. 2015, 8, 139–157. [Google Scholar] [CrossRef]
- Ji, R.; Qu, S. Investigation and evaluation of energy consumption performance for hospital buildings in china. Sustainability 2019, 11, 1724. [Google Scholar] [CrossRef]
- Ascione, F.; Bianco, N.; De Masi, R.F.; Vanoli, G.P. Rehabilitation of the building envelope of hospitals: Achievable energy savings and microclimatic control on varying the hvac systems in mediterranean climates. Energy Build. 2013, 60, 125–138. [Google Scholar] [CrossRef]
- Buonomano, A.; Calise, F.; Ferruzzi, G.; Palombo, A. Dynamic energy performance analysis: Case study for energy efficiency retrofits of hospital buildings. Energy 2014, 78, 555–572. [Google Scholar] [CrossRef]
- Vaziri, S.M.; Rezaee, B.; Monirian, M.A. Utilizing renewable energy sources efficiently in hospitals using demand dispatch. Renew. Energy 2019, 151, 551–562. [Google Scholar] [CrossRef]
- Bujak, J.W. Production of waste energy and heat in hospital facilities. Energy 2015, 91, 350–362. [Google Scholar] [CrossRef]
- Bakaimis, B.; Papanikolaou, I. Electrical energy saving policies, initiatives, results, challenges and lessons learned for the grevena hospital. Procedia Environ. Sci. 2017, 38, 882–889. [Google Scholar] [CrossRef]
- García-Sanz-Calcedo, J.; Al-Kassir, A.; Yusaf, T. Economic and environmental impact of energy saving in healthcare buildings. Appl. Sci. 2018, 8, 440. [Google Scholar] [CrossRef]
- Gaspari, J.; Fabbri, K.; Gabrielli, L. A study on parametric design application to hospital retrofitting for improving energy savings and comfort conditions. Buildings 2019, 9, 220. [Google Scholar] [CrossRef]
- Wyssusek, K.H.; Keys, M.T.; van Zundert, A.A.J. Operating room greening initiatives – the old, the new, and the way forward: A narrative review. Waste Manag. Res. 2019, 37, 3–19. [Google Scholar] [CrossRef]
- Wang, T.; Li, X.; Liao, P.-C.; Fang, D. Building energy efficiency for public hospitals and healthcare facilities in china: Barriers and drivers. Energy 2016, 103, 588–597. [Google Scholar] [CrossRef]
- Kolokotsa, D.; Tsoutsos, T.; Papantoniou, S. Energy conservation techniques for hospital buildings. Adv. Build. Energy Res. 2012, 6, 159–172. [Google Scholar] [CrossRef]
- González-Gil, A.; López-González, J.L.; Fernández, M.; Eguía, P.; Erkoreka, A.; Granada, E. Thermal energy demand and potential energy savings in a spanish surgical suite through calibrated simulations. Energy Build. 2018, 174, 513–526. [Google Scholar] [CrossRef]
- Ho, S.H.; Rosario, L.; Rahman, M.M. Three-dimensional analysis for hospital operating room thermal comfort and contaminant removal. Appl. Therm. Eng. 2009, 29, 2080–2092. [Google Scholar] [CrossRef]
- Chow, T.T.; Yang, X.Y. Ventilation performance in operating theatres against airborne infection: Review of research activities and practical guidance. J. Hosp. Infect. 2004, 56, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Chow, T.T.; Yang, X.Y. Ventilation performance in the operating theatre against airborne infection: Numerical study on an ultra-clean system. J. Hosp. Infect. 2005, 59, 138–147. [Google Scholar] [CrossRef]
- Rui, Z.; Guangbei, T.; Jihong, L. Study on biological contaminant control strategies under different ventilation models in hospital operating room. Build. Environ. 2008, 43, 793–803. [Google Scholar] [CrossRef]
- Yau, Y.H.; Ding, L.C. A comprehensive computational fluid dynamics simulation on the air distribution in an operating room at university of malaya medical centre malaysia. Indoor Built Environ. 2015, 24, 355–369. [Google Scholar] [CrossRef]
- Mora, R.; English, M.J.M.; Athienitis, A.K. Assessment of Thermal Comfort during Surgical Operations; ASHRAE Winter Meeting CD, Technical and Symposium Papers; ASHRAE: Houston, TX, USA, 2001; pp. 65–74. [Google Scholar]
- Khodakarami, J.; Nasrollahi, N. Thermal comfort in hospitals—A literature review. Renew. Sustain. Energy Rev. 2012, 16, 4071–4077. [Google Scholar] [CrossRef]
- Van Gaever, R.; Jacobs, V.A.; Diltoer, M.; Peeters, L.; Vanlanduit, S. Thermal comfort of the surgical staff in the operating room. Build. Environ. 2014, 81, 37–41. [Google Scholar] [CrossRef]
- Sánchez-Barroso, G.; Sanz-Calcedo, J.G. Evaluation of hvac design parameters in high-performance hospital operating theatres. Sustainability 2019, 11, 1493. [Google Scholar] [CrossRef]
- Balaras, C.A.; Dascalaki, E.; Gaglia, A. Hvac and indoor thermal conditions in hospital operating rooms. Energy Build. 2007, 39, 454–470. [Google Scholar] [CrossRef]
- Melhado, M.A.; Hensen, J.; Loomans, M.G.L.C.; Forejt, L. Review of Operating Room Ventilation Standards; STP-Society of Environmental Engineering: Prague, Czech Republic, 2019. [Google Scholar]
- Yau, Y.H. The use of a double heat pipe heat exchanger system for reducing energy consumption of treating ventilation air in an operating theatre—A full year energy consumption model simulation. Energy Build. 2008, 40, 917–925. [Google Scholar] [CrossRef]
- Noie-Baghban, S.H.; Majideian, G.R. Waste heat recovery using heat pipe heat exchanger (hphe) for surgery rooms in hospitals. Appl. Therm. Eng. 2000, 20, 1271–1282. [Google Scholar] [CrossRef]
- Ozyogurtcu, G.; Mobedi, M.; Ozerdem, B. Economical assessment of different hvac systems for an operating room: Case study for different turkish climate regions. Energy Build. 2011, 43, 1536–1543. [Google Scholar] [CrossRef]
- Wang, C.; Holmberg, S.; Sadrizadeh, S. Numerical study of temperature-controlled airflow in comparison with turbulent mixing and laminar airflow for operating room ventilation. Build. Environ. 2018, 144, 45–56. [Google Scholar] [CrossRef]
- Alsved, M.; Civilis, A.; Ekolind, P.; Tammelin, A.; Andersson, A.E.; Jakobsson, J.; Svensson, T.; Ramstorp, M.; Sadrizadeh, S.; Larsson, P.A.; et al. Temperature-controlled airflow ventilation in operating rooms compared with laminar airflow and turbulent mixed airflow. J. Hosp. Infect. 2018, 98, 181–190. [Google Scholar] [CrossRef]
- Febrero Garrido, L.; López, G.; Eguía, O.; Granada, Á. Development of a calibrated simulation method for airborne particles to optimize energy consumption in operating rooms. Energies 2019, 12, 2433. [Google Scholar] [CrossRef]
- Cannistraro, G.; Cannistraro, M.; Galvagno, A.; Trovato, G. Analysis and measures for energy savings in operating theaters. Int. J. Heat Technol. 2017, 35, S422–S448. [Google Scholar] [CrossRef]
- Sánchez-Barroso Moreno, G.; García-Sanz Calcedo, J.; González, A.G.; Salgado, D.R. Sustainable Solutions for Thermal Energy Saving in Hospital Operating Theatres; E3S Web of Conferences; EENVIRO 2018: Cluj Napoca, Romania, 2019. [Google Scholar]
- AENOR. Une 100713:2005 Instalaciones de Acondicionamiento de Aire en Hospitals; AENOR: Madrid, España, 2005. [Google Scholar]
- ASHRAE. Ansi/Ashrae/Ashe Standard 170-2017 Ventilation of Health Care Facilities; AHSRAE: Atlanta, GA, USA, 2017. [Google Scholar]
- Chow, T.-T.; Yang, X.-Y. Performance of ventilation system in a non-standard operating room. Build. Environ. 2003, 38, 1401–1411. [Google Scholar] [CrossRef]
- Loomans, M.G.L.C.; Molenaar, P.C.A.; Kort, H.S.M.; Joosten, P.H.J. Energy demand reduction in pharmaceutical cleanrooms through optimization of ventilation. Energy Build. 2019, 202, 109346. [Google Scholar] [CrossRef]
- Porowski, M. Energy optimization of hvac system from a holistic perspective: Operating theater application. Energy Convers. Manag. 2019, 182, 461–496. [Google Scholar] [CrossRef]
- AFNOR. Nf s90-351 Établissements de Santé—Zones à Environnement Maîtrisé—Exigences Relatives à la Maîtrise de la Contamination Aéroportée; AFNOR: Paris, France, 2013. [Google Scholar]
- Wisconsin-Madison, S.E.L.U.O. Trnsys 17, a Transient System Simulation Program User Manual; University of Wisconsin: Madison, MI, USA, 2012. [Google Scholar]
- ISO. 7730:2005. Ergonomics of the Thermal Environment—Analytical Determination and Interpretation of Thermal Comfort Using Calculation of the PMV and PPD Indices and Local Thermal Comfort Criteria; ISO: Geneva, Switzerland, 2005. [Google Scholar]
- Laboratory, L.B.N. Genopt Generic Optimization Program; Lawrence Berkeley National Laboratory: Berkeley, CA, USA, 2016. [Google Scholar]
- Ruiz, G.R.; Bandera, C.F. Validation of calibrated energy models: Common errors. Energies 2017, 10, 1587. [Google Scholar] [CrossRef]




















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Lighting | Electrical Equipment | ||
|---|---|---|---|
| Space | Power (W) | Space | Power (W) |
| ORs | 3300 | ORs | 31,500 1 |
| Ancillary rooms | 1500 | Ancillary rooms | - |
| Corridors | 1000 | Corridors | - |
| Total | 5800 | Total | 31,500 |
| Sensor Number | Model | Zone | Variable | Uncertainty |
|---|---|---|---|---|
| 1 | Siemens QFA2060 | OR1 | Temperature | ±0.7 °C, at 15 °C…35 °C ±1 °C, at −35 °C…50 °C |
| 2 | OR2 | |||
| 3 | OR3 | RH | ±5%, at 0%…95% ±3%, at 30%…70% | |
| 4 | Siemens QFM2160 | Ancillary rooms | Temperature | ±0.8 °C, at 15 °C…35 °C ±1 °C, at −35 °C…50 °C |
| 5 | Entrance corridor | |||
| 6 | Exit corridor | RH | ±5%, at 0%…95% ±3%, at 30%…70% |
| Parameters | Zone | SCENARIO 1 | SCENARIO 2 | SCENARIO 3 |
|---|---|---|---|---|
| Total air intake | ORs | 21.5 ACH | 21.5 ACH | 20 ACH |
| Anc. rooms | 6 ACH | 6 ACH | 6 ACH | |
| Outside air intake | ORs | 21.5 ACH | 10.8 ACH | 4 ACH |
| Anc. rooms | 6 ACH | 3 ACH | 2 ACH | |
| Working period 1 hygrothermal conditions | ORs | T = 22 °C, 45–55% RH | ||
| Anc. rooms | T = 23.5 °C, 45–55% RH | |||
| Off-use period hygrothermal conditions | ORs | 15–30 °CNon-controlled RH | ||
| Anc. rooms | ||||
| OR1 | OR2 | OR3 | ||||
|---|---|---|---|---|---|---|
| Intake Air | Indoor Air | Intake Air | Indoor Air | Intake Air | Indoor Air | |
| Maximum RH [%] | 68.2 | 66.5 | 75.4 | 66.3 | 79.7 | 68.9 |
| Average RH [%] | 52.4 | 55.1 | 56.9 | 54.9 | 58.2 | 56.1 |
| Minimum RH [%] | 30.8 | 41.8 | 32.8 | 41.9 | 31.8 | 41.4 |
| Maximum T [°C] | 31.7 | 26.8 | 31.4 | 26.6 | 32.4 | 26.5 |
| Average T [°C] | 23.5 | 22.8 | 22.8 | 23.0 | 22.8 | 22.4 |
| Minimum T [°C] | 18.3 | 19.8 | 17.1 | 20.1 | 16.5 | 19.1 |
| First Data Collection Period | Second Data Collection Period | |||||
|---|---|---|---|---|---|---|
| Error | OR1 | OR2 | OR3 | OR1 | OR2 | OR3 |
| CV(RMSE) Temperatures | 1.02% | 2.63% | 0.64% | 1.12% | 3.16% | 0.73% |
| CV(RMSE) RH | 3.98% | 3.26% | 2.54% | 2.96% | 3.75% | 2.31% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cacabelos-Reyes, A.; López-González, J.L.; González-Gil, A.; Febrero-Garrido, L.; Eguía-Oller, P.; Granada-Álvarez, E. Assessing the Energy Demand Reduction in a Surgical Suite by Optimizing the HVAC Operation During Off-Use Periods. Appl. Sci. 2020, 10, 2233. https://doi.org/10.3390/app10072233
Cacabelos-Reyes A, López-González JL, González-Gil A, Febrero-Garrido L, Eguía-Oller P, Granada-Álvarez E. Assessing the Energy Demand Reduction in a Surgical Suite by Optimizing the HVAC Operation During Off-Use Periods. Applied Sciences. 2020; 10(7):2233. https://doi.org/10.3390/app10072233
Chicago/Turabian StyleCacabelos-Reyes, Antón, José Luis López-González, Arturo González-Gil, Lara Febrero-Garrido, Pablo Eguía-Oller, and Enrique Granada-Álvarez. 2020. "Assessing the Energy Demand Reduction in a Surgical Suite by Optimizing the HVAC Operation During Off-Use Periods" Applied Sciences 10, no. 7: 2233. https://doi.org/10.3390/app10072233
APA StyleCacabelos-Reyes, A., López-González, J. L., González-Gil, A., Febrero-Garrido, L., Eguía-Oller, P., & Granada-Álvarez, E. (2020). Assessing the Energy Demand Reduction in a Surgical Suite by Optimizing the HVAC Operation During Off-Use Periods. Applied Sciences, 10(7), 2233. https://doi.org/10.3390/app10072233