Feature Assessment of Toe Area Activity during Walking of Elderly People with Stumbling Experiences through Wearable Clog-Integrated Plantar Visualization System


Abstract
1. Introduction
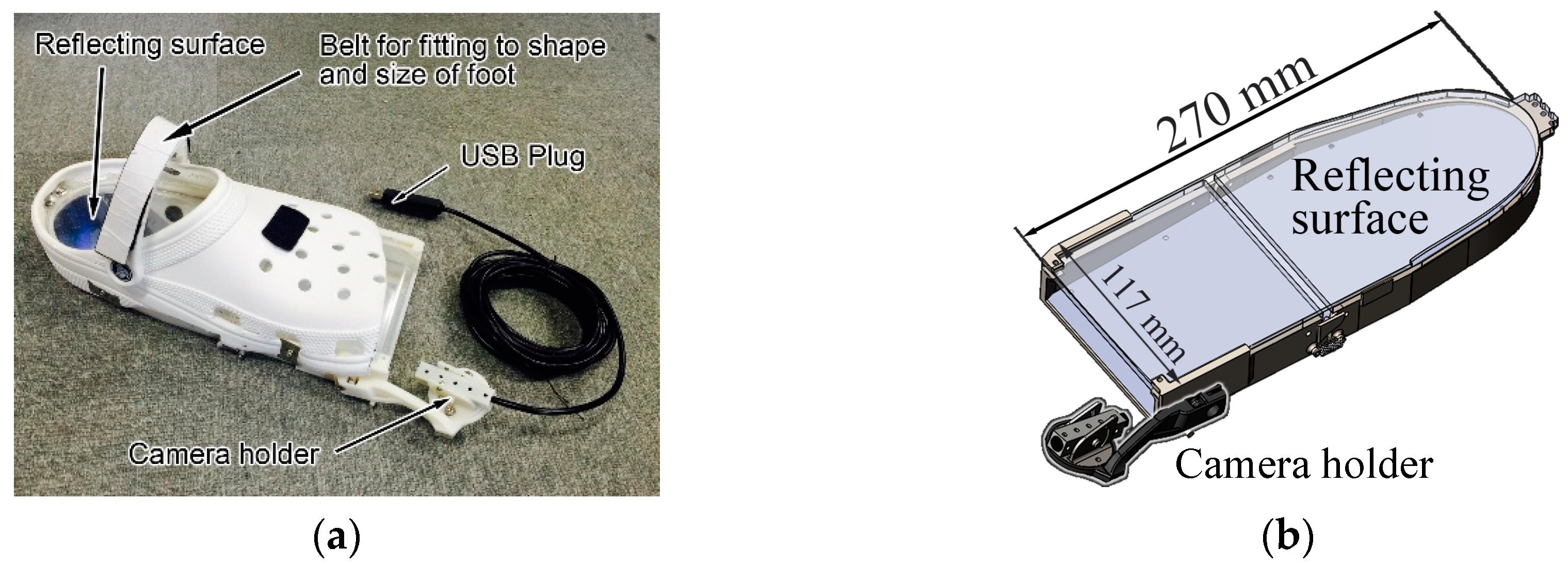
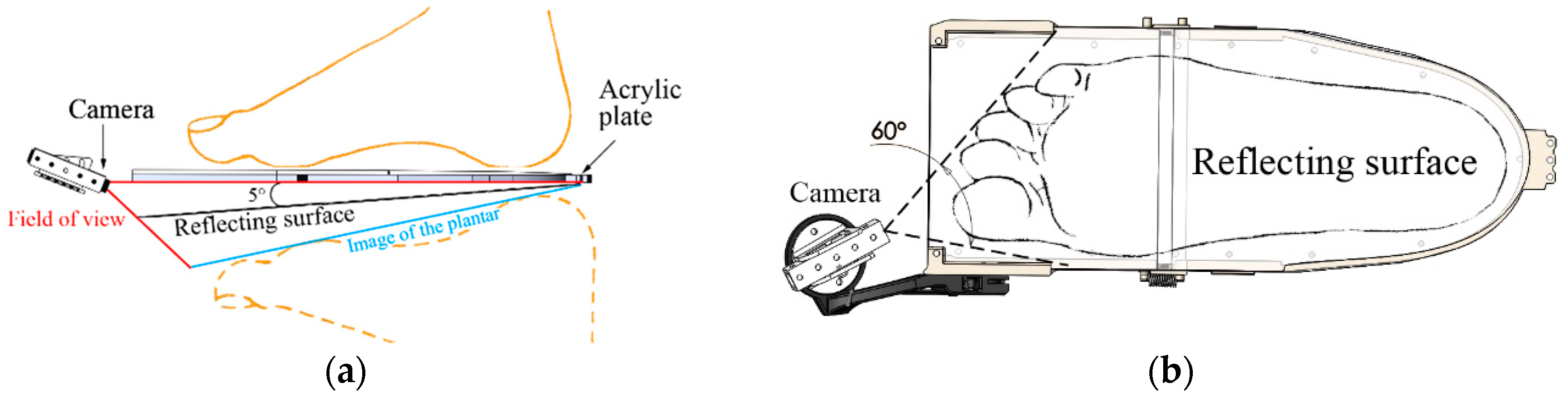
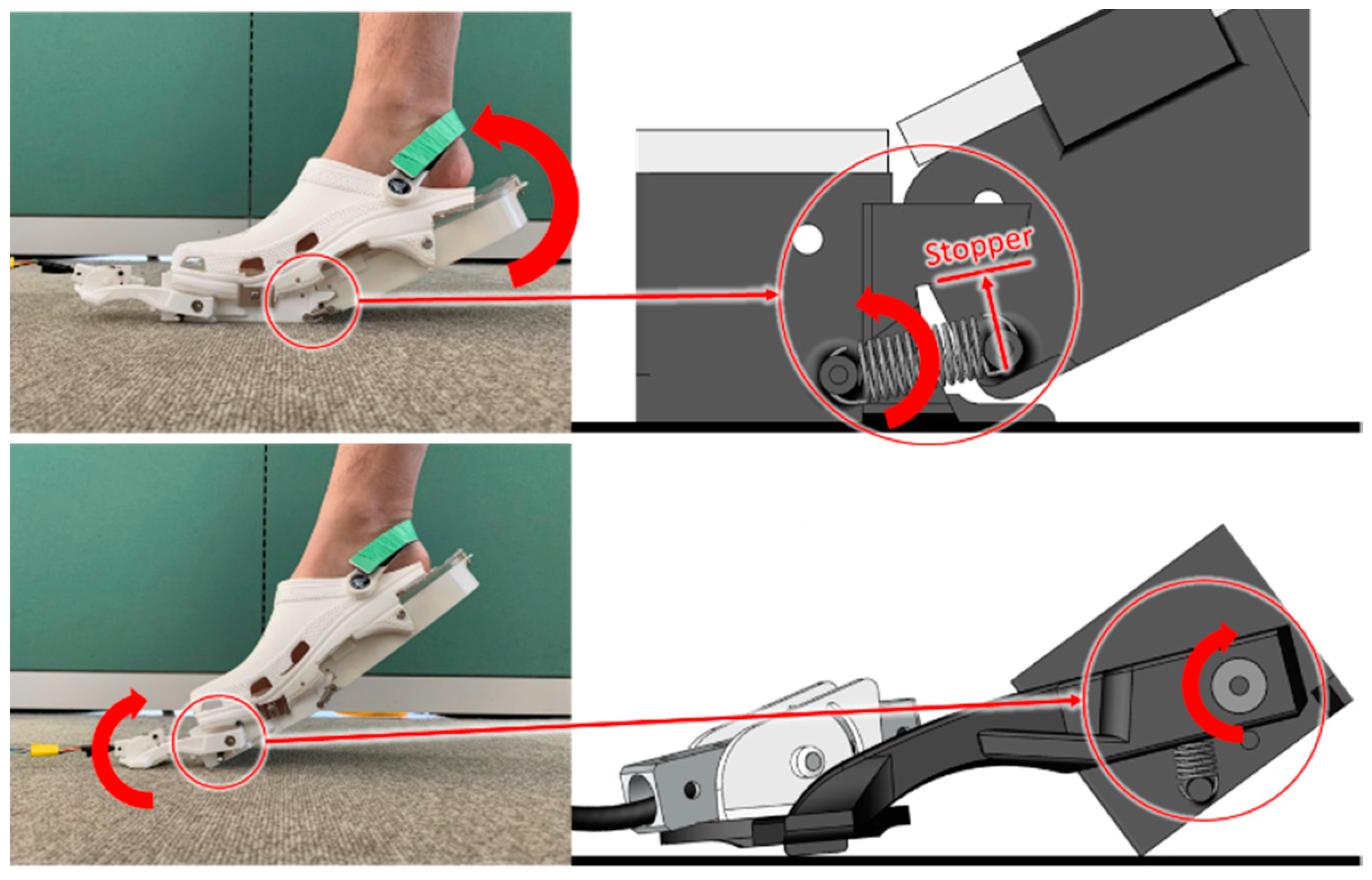
2. Clog-Integrated Plantar Visualization System
Overview of the System
3. Methods
3.1. Participants
3.2. Procedure
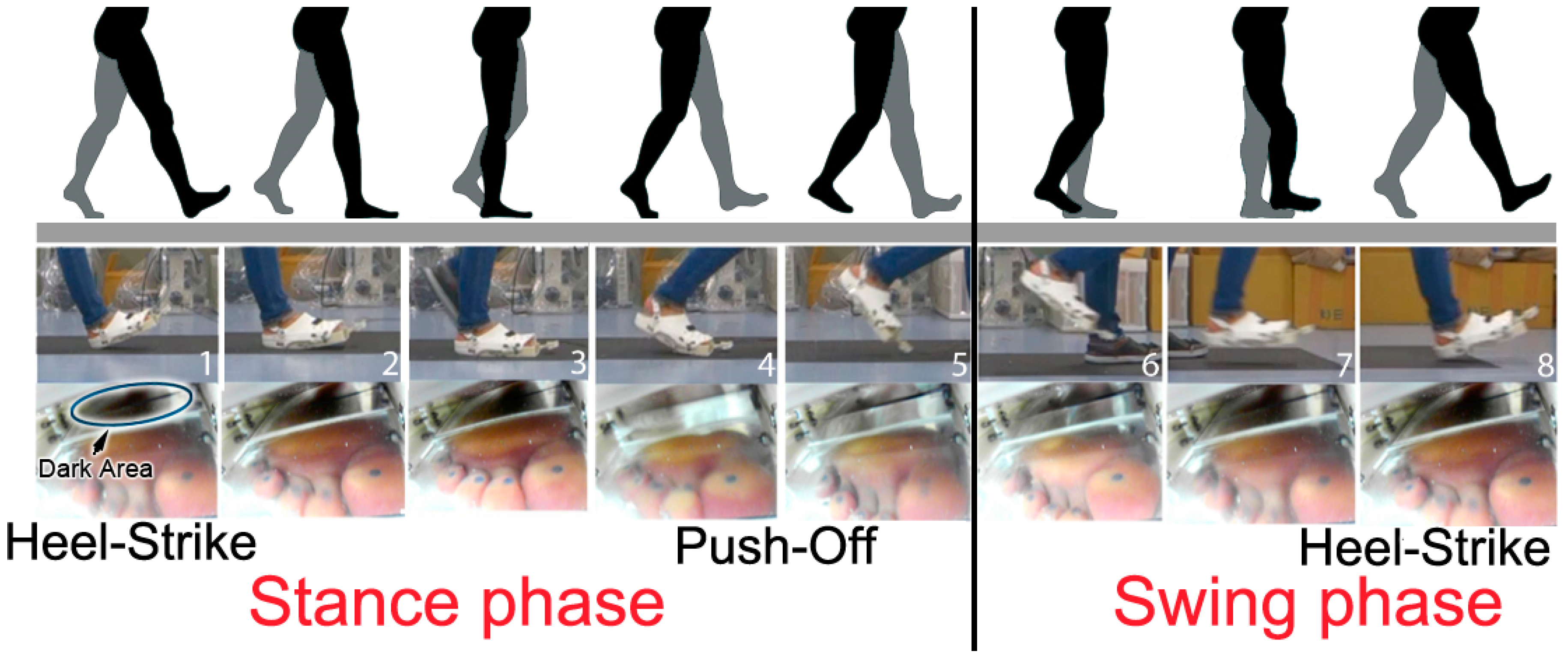
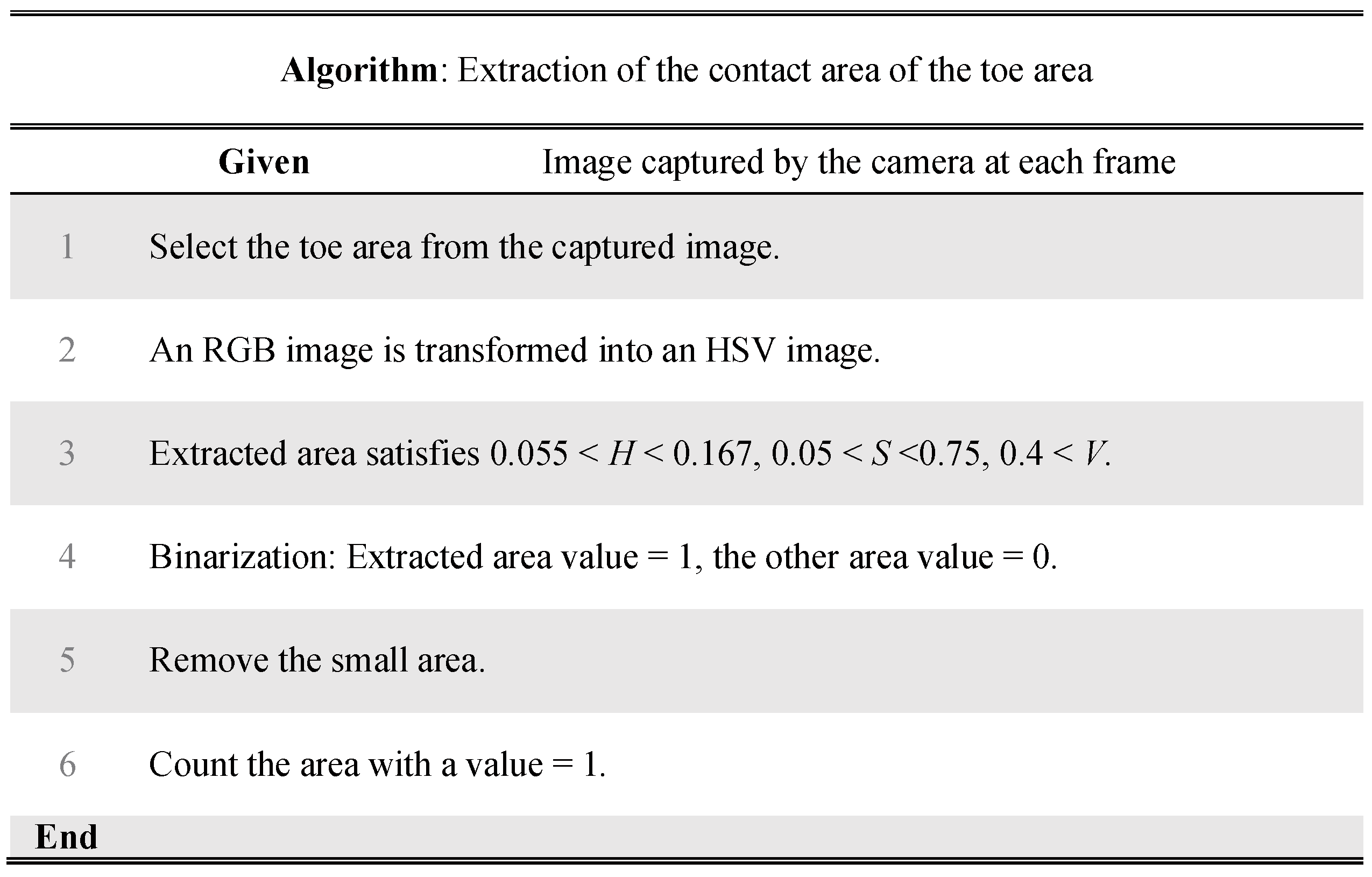
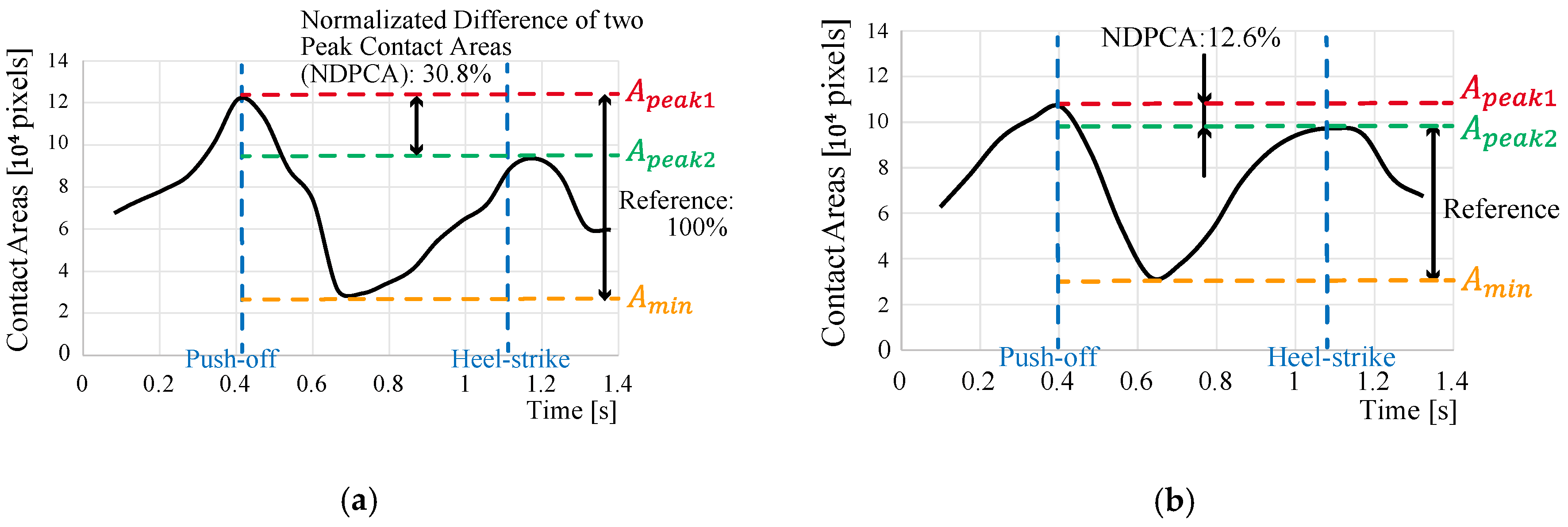
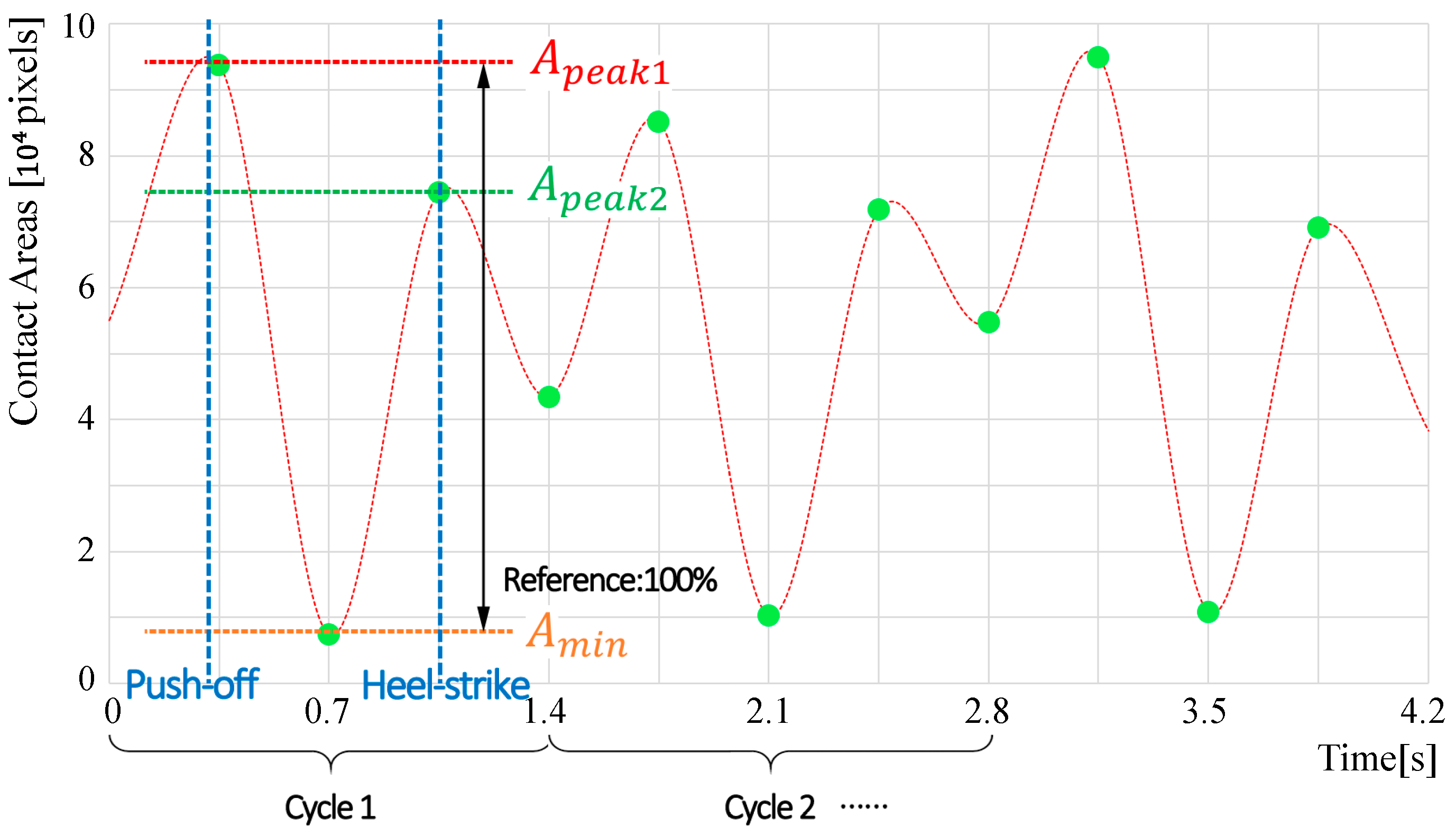
3.3. Data Analysis: Toe-Area Activity
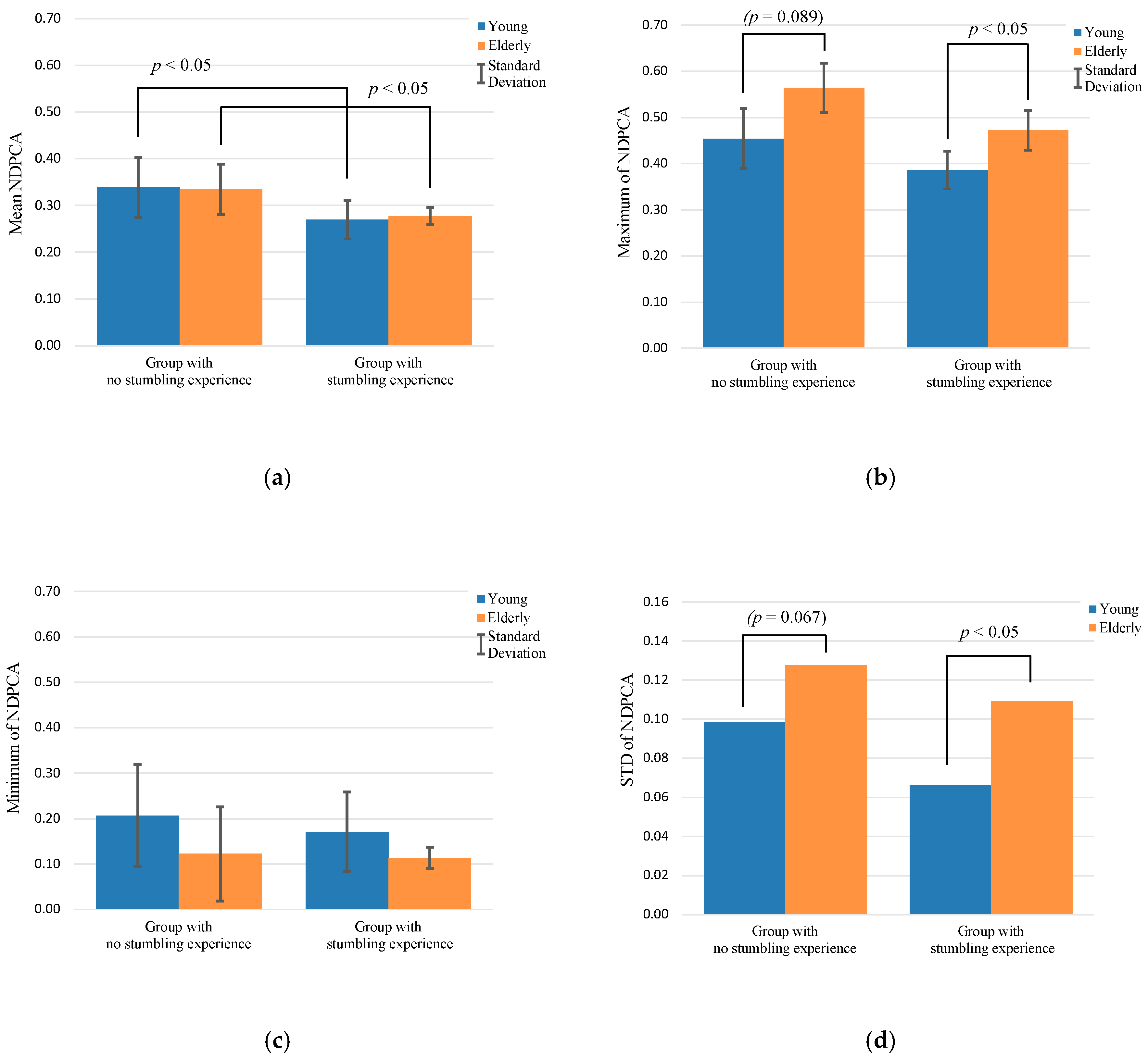
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A
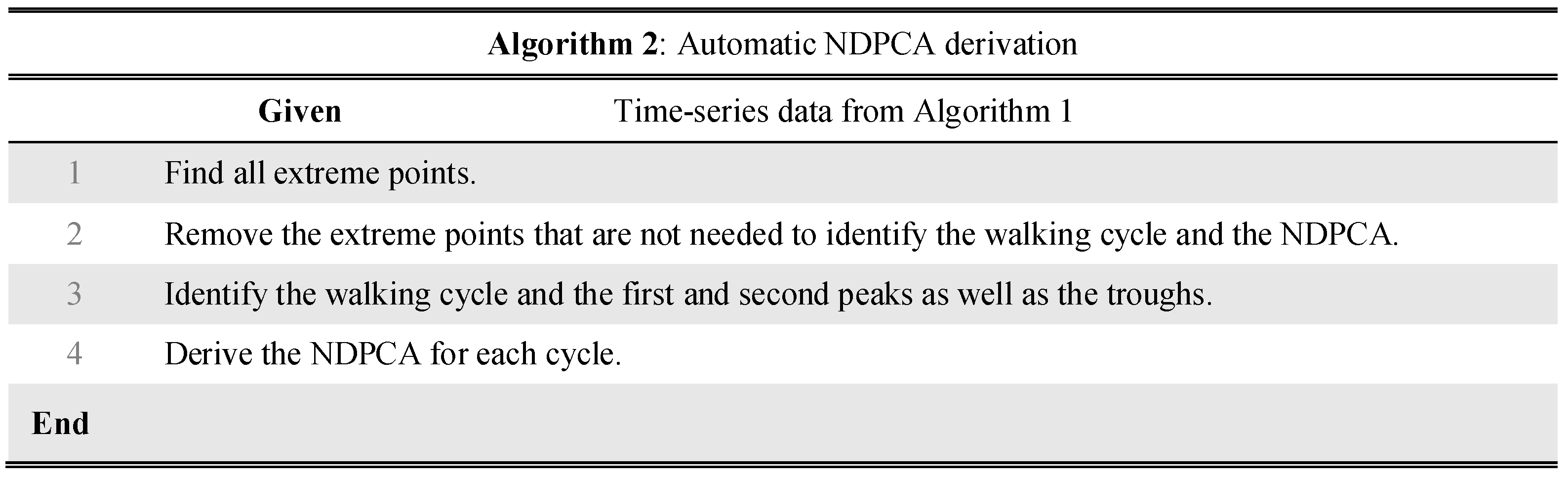
Automatic Deviation of NDPCA



References
- Cabinet Office, Government of Japan. Annual Report on the Aging Society. 2016. Available online: https://www8.cao.go.jp/kourei/english/annualreport/2016/2016pdf_e.html (accessed on 15 January 2020).
- Oliver, D.; Daly, F.; Martin, F.C.; McMurdo, M.E.T. Risk factors and risk assessment tools for falls in hospital in-patients: A systematic review. Age Ageing 2004, 33, 122–130. [Google Scholar] [CrossRef]
- Taylor, A.J.; Menz, H.B.; Keenan, A.-M. The influence of walking speed on plantar pressure measurements using the two-step gait initiation protocol. Foot 2004, 14, 49–55. [Google Scholar] [CrossRef]
- Burnfield, J.M.; Few, C.D.; Mohamed, O.S.; Perry, J. The influence of walking speed and footwear on plantar pressures in older adults. Clin. Biomech. 2004, 19, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Preis, S.; Klemms, A.; Müller, K. Gait analysis by measuring ground reaction forces in children: Changes to an adaptive gait pattern between the ages of one and five years. Dev. Med. Child Neurol. 2008, 39, 228–233. [Google Scholar] [CrossRef] [PubMed]
- Chuckpaiwong, B.; Nunley, J.A.; Mall, N.A.; Queen, R.M. The effect of foot type on in-shoe plantar pressure during walking and running. Gait Posture 2008, 28, 405–411. [Google Scholar] [CrossRef]
- Majumder, A.J.A.; Zerin, I.; Uddin, M.; Ahamed, S.I.; Smith, R.O. Smartprediction: A Real-time Smartphone-based Fall Risk Prediction and Prevention System. In Proceedings of the 2013 Research in Adaptive and Convergent Systems, Montreal, OC, Canada, 1–4 October 2013; pp. 434–439. [Google Scholar]
- Ayena, J.C.; Otis, M.J.D.; Menelas, B.A.J. An efficient home-based risk of falling assessment test based on Smartphone and instrumented insole. In Proceedings of the 2015 IEEE International Symposium on Medical Measurements and Applications (MeMeA) Proceedings, Turin, Italy, 7–9 May 2015; pp. 416–421. [Google Scholar]
- Yu, H.; Wang, D.; Yang, C.-J.; Lee, K.-M. A walking monitoring shoe system for simultaneous plantar-force measurement and gait-phase detection. In Proceedings of the 2010 IEEE/ASME International Conference on Advanced Intelligent Mechatronics, Montreal, ON, Canada, 6–9 July 2010; pp. 207–212. [Google Scholar]
- Crea, S.; Donati, M.; De Rossi, S.M.M.; Oddo, C.M.; Vitiello, N. A wireless flexible sensorized insole for gait analysis. Sensors 2014, 14, 1073–1093. [Google Scholar] [CrossRef]
- Yang, S.; Li, Q. Inertial sensor-based methods in walking speed estimation: A systematic review. Sensors 2012, 12, 6102–6116. [Google Scholar] [CrossRef]
- Hung, T.N.; Suh, Y.S. Inertial sensor-based two feet motion tracking for gait analysis. Sensors 2013, 13, 5614–5629. [Google Scholar] [CrossRef]
- Do, T.N.; Suh, Y.S. Gait Analysis Using Floor Markers and Inertial Sensors. Sensors 2012, 12, 1594–1611. [Google Scholar] [CrossRef]
- Foxlin, E. Pedestrian Tracking with Shoe-Mounted Inertial Sensors. IEEE Comput. Graph. Appl. 2005, 25, 38–46. [Google Scholar] [CrossRef]
- Sim, S.Y.; Jeon, H.S.; Chung, G.S.; Kim, S.K.; Kwon, S.J.; Lee, W.K.; Park, K.S. Fall detection algorithm for the elderly using acceleration sensors on the shoes. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, EMBS, Boston, MA, USA, 30 August–3 September 2011; pp. 4935–4938. [Google Scholar]
- Rampp, A.; Barth, J.; Schülein, S.; Gaßmann, K.G.; Klucken, J.; Eskofier, B.M. Inertial Sensor-Based Stride Parameter Calculation from Gait Sequences in Geriatric Patients. IEEE Trans. Biomed. Eng. 2015, 62, 1089–1097. [Google Scholar] [CrossRef]
- Mariani, B.; Hoskovec, C.; Rochat, S.; Büla, C.; Penders, J.; Aminian, K. 3D gait assessment in young and elderly subjects using foot-worn inertial sensors. J. Biomech. 2010, 43, 2999–3006. [Google Scholar] [CrossRef]
- Schepers, H.M.; Koopman, H.F.J.M.; Veltink, P.H. Ambulatory assessment of ankle and foot dynamics. IEEE Trans. Biomed. Eng. 2007, 54, 895–902. [Google Scholar] [CrossRef] [PubMed]
- Bamberg, S.J.M.; Benbasat, A.Y.; Scarborough, D.M.; Krebs, D.E.; Paradiso, J. A Gait analysis using a shoe-integrated wireless sensor system. IEEE Trans. Inf. Technol. Biomed. 2008, 12, 413–423. [Google Scholar] [CrossRef] [PubMed]
- Bebek, Ö.; Suster, M.A.; Rajgopal, S.; Fu, M.J.; Huang, X.; Cavusoglu, M.C.; Young, D.J.; Mehregany, M.; van den Bogert, A.J.; Mastrangelo, C.H. Personal Navigation via High-Resolution Gait-Corrected Inertial Measurement Units. IEEE Trans. Instrum. Meas. 2010, 59, 3018–3027. [Google Scholar] [CrossRef]
- Chen, M.; Huang, B.; Xu, Y. Intelligent shoes for abnormal gait detection. In Proceedings of the IEEE International Conference on Robotics and Automation, Pasadena, CA, USA, 19–23 May 2008; pp. 2019–2024. [Google Scholar]
- Hegde, N.; Sazonov, E.S. SmartStep 2.0—A completely wireless, versatile insole monitoring system. In Proceedings of the 2015 IEEE International Conference on Bioinformatics and Biomedicine (BIBM), Washington, DC, USA, 9–12 November 2015; pp. 746–749. [Google Scholar]
- Kawsar, F.; Hasan, M.K.; Love, R.; Ahamed, S.I. A Novel Activity Detection System Using Plantar Pressure Sensors and Smartphone. In Proceedings of the IEEE 39th Annual Computer Software and Applications Conference, Taichung, Taiwan, 1–5 July 2015; pp. 44–49. [Google Scholar]
- Tsuyuguchi, R.; Kurose, S.; Seto, T.; Takao, N.; Tagashira, S.; Tsutsumi, H.; Otsuki, S.; Kimura, Y. Toe grip strength in middle-aged individuals as a risk factor for falls. J. Sports Med. Phys. Fit. 2018, 58, 1325–1330. [Google Scholar]
- Kim, Y.-W.; Kwon, O.-Y.; Cynn, H.-S.; Weon, J.-H.; Yi, C.-H.; Kim, T.-H. Comparison of Toe Plantar Flexors Strength and Balancing Ability between Elderly Fallers and Non-fallers. J. Phys. Ther. Sci. 2011, 23, 127–132. [Google Scholar] [CrossRef][Green Version]
- Mickle, K.J.; Munro, B.J.; Lord, S.R.; Menz, H.B.; Steele, J.R. ISB Clinical Biomechanics Award 2009. Clin. Biomech. 2009, 24, 787–791. [Google Scholar] [CrossRef] [PubMed]
- Hiura, M.; Nemoto, H.; Nishisaka, K.; Higashi, K.; Katoh, T. The Association Between Walking Ability and Falls in Elderly Japanese Living in the Community Using a Path Analysis. J. Community Health 2012, 37, 957–962. [Google Scholar] [CrossRef] [PubMed]
- Uritani, D.; Fukumoto, T.; Matsumoto, D.; Shima, M. The Relationship Between Toe Grip Strength and Dynamic Balance or Functional Mobility Among Community-Dwelling Japanese Older Adults: A Cross-Sectional Study. J. Aging Phys. Act. 2016, 24, 459–464. [Google Scholar] [CrossRef] [PubMed]
- Branthwaite, H.; Grabtree, G.; Chockalingam, N.; Greenhalgh, A. The Effect of Toe Flexion Exercises on Grip. J. Am. Podiatr. Med. Assoc. 2018, 108, 355–361. [Google Scholar] [CrossRef]
- Takatori, K.; Matsumoto, D. Relationships Between Simple Toe Elevation Angle in the Standing Position and Dynamic Balance and Fall Risk Among Community-Dwelling Older Adults. PM&R 2015, 7, 1059–1063. [Google Scholar]
- Bus, S.A.; Maas, M.; de Lange, A.; Michels, R.P.J.; Levi, M. Elevated plantar pressures in neuropathic diabetic patients with claw/hammer toe deformity. J. Biomech. 2005, 38, 1918–1925. [Google Scholar] [CrossRef] [PubMed]
- Morag, E.; Cavanagh, P.R. Structural and functional predictors of regional peak pressures under the foot during walking. J. Biomech. 1999, 32, 359–370. [Google Scholar] [CrossRef]
- Payne, C.; Turner, D.; Miller, K. Determinants of plantar pressures in the diabetic foot. J. Diabetes Complicat. 2002, 16, 277–283. [Google Scholar] [CrossRef]
- Buldt, A.K.; Forghany, S.; Landorf, K.B.; Levinger, P.; Murley, G.S.; Menz, H.B. Foot posture is associated with plantar pressure during gait: A comparison of normal, planus and cavus feet. Gait Posture 2018, 62, 235–240. [Google Scholar] [CrossRef]
- Jin, Y.; Shogenji, M.; Watanabe, T. Clog-integrated plantar visualization system for evaluating activity during walking. In Proceedings of the 2017 IEEE International Conference on Advanced Intelligent Mechatronics (AIM), Munich, Germany, 3–7 July 2017; pp. 862–867. [Google Scholar]
- Byju, A.G.; Nussbaum, M.A.; Madigan, M.L. Alternative measures of toe trajectory more accurately predict the probability of tripping than minimum toe clearance. J. Biomech. 2016, 49, 4016–4021. [Google Scholar] [CrossRef]
- Santhiranayagam, B.K.; Sparrow, W.A.; Lai, D.T.H.; Begg, R.K. Non-MTC gait cycles: An adaptive toe trajectory control strategy in older adults. Gait Posture 2017, 53, 73–79. [Google Scholar] [CrossRef]
- Zhang, J.; Si, Y.; Zhang, Y.; Liu, Y. The effects of restricting the flexion–extension motion of the first metatarsophalangeal joint on human walking gait. Biomed. Mater. Eng. 2014, 24, 2577–2584. [Google Scholar] [CrossRef]
- Kurihara, T.; Yamauchi, J.; Otsuka, M.; Tottori, N.; Hashimoto, T.; Isaka, T. Maximum toe flexor muscle strength and quantitative analysis of human plantar intrinsic and extrinsic muscles by a magnetic resonance imaging technique. J. Foot Ankle Res. 2014, 7, 26. [Google Scholar] [CrossRef]
- Guillén-Rogel, P.; San Emeterio, C.; Marín, P.J. Associations between ankle dorsiflexion range of motion and foot and ankle strength in young adults. J. Phys. Ther. Sci. 2017, 29, 1363–1367. [Google Scholar] [CrossRef] [PubMed]
- Mecagni, C.; Smith, J.P.; Roberts, K.E.; O’Sullivan, S.B. Balance and ankle range of motion in community-dwelling women aged 64 to 87 years: A correlational study. Phys. Ther. 2000, 80, 1004–1011. [Google Scholar] [CrossRef] [PubMed]
- Moosabhoy, M.A.; Gard, S.A. Methodology for determining the sensitivity of swing leg toe clearance and leg length to swing leg joint angles during gait. Gait Posture 2006, 24, 493–501. [Google Scholar] [CrossRef] [PubMed]
- Menz, H.B.; Zammit, G.V.; Munteanu, S.E. Plantar pressures are higher under callused regions of the foot in older people. Clin. Exp. Dermatol. 2007, 32, 375–380. [Google Scholar] [CrossRef]
- Fox, J.; Docherty, C.L.; Schrader, J.; Applegate, T. Eccentric plantar-flexor torque deficits in participants with functional ankle instability. J. Athl. Train. 2008, 43, 51–54. [Google Scholar] [CrossRef]
- Mueller, M.J.; Hastings, M.; Commean, P.K.; Smith, K.E.; Pilgram, T.K.; Robertson, D.; Johnson, J. Forefoot structural predictors of plantar pressures during walking in people with diabetes and peripheral neuropathy. J. Biomech. 2003, 36, 1009–1017. [Google Scholar] [CrossRef]
- Verlinden, V.J.A.; van der Geest, J.N.; Hoogendam, Y.Y.; Hofman, A.; Breteler, M.M.B.; Ikram, M.A. Gait patterns in a community-dwelling population aged 50 years and older. Gait Posture 2013, 37, 500–505. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Young | Elderly | |
|---|---|---|
| Number of participants | 13 (M:9 F:4) | 9 (M:5 F:4) |
| Without stumbling experience | 8 (M:5 F:3) | 5 (M:3 F:2) |
| With stumbling experience | 5 (M:4 F:1) | 4 (M:2 F:2) |
| Information of participants | ||
| Age | ||
| Weight | ||
| Height | ||
| Foot Size |
| NDPCA (Mean ± Std.) | Male | Female | p-Value * |
|---|---|---|---|
| Young | 0.536 | ||
| Elderly | 0.690 |
| Young | Elderly | p-Value | |
|---|---|---|---|
| Mean NDPCA | |||
| Without stumbling experience | 0.451 | ||
| With stumbling experience | 0.348 | ||
| p-value | 0.020 * | 0.039 * | / |
| Maximum NDPCA | |||
| Without stumbling experience | 0.012 * | ||
| With stumbling experience | 0.038 * | ||
| p-value | 0.089 | 0.017 * | / |
| Minimum NDPCA | |||
| Without stumbling experience | 0.101 | ||
| With stumbling experience | 0.110 | ||
| p-value | 0.268 | 0.572 | / |
| NDPCA Standard Deviation | |||
| Without stumbling experience | 0.067 | ||
| With stumbling experience | 0.048 * | ||
| p-value | 0.096 | 0.151 | / |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jin, Y.; Shogenji, M.; Watanabe, T. Feature Assessment of Toe Area Activity during Walking of Elderly People with Stumbling Experiences through Wearable Clog-Integrated Plantar Visualization System. Appl. Sci. 2020, 10, 1359. https://doi.org/10.3390/app10041359
Jin Y, Shogenji M, Watanabe T. Feature Assessment of Toe Area Activity during Walking of Elderly People with Stumbling Experiences through Wearable Clog-Integrated Plantar Visualization System. Applied Sciences. 2020; 10(4):1359. https://doi.org/10.3390/app10041359
Chicago/Turabian StyleJin, Yingjie, Miho Shogenji, and Tetsuyou Watanabe. 2020. "Feature Assessment of Toe Area Activity during Walking of Elderly People with Stumbling Experiences through Wearable Clog-Integrated Plantar Visualization System" Applied Sciences 10, no. 4: 1359. https://doi.org/10.3390/app10041359
APA StyleJin, Y., Shogenji, M., & Watanabe, T. (2020). Feature Assessment of Toe Area Activity during Walking of Elderly People with Stumbling Experiences through Wearable Clog-Integrated Plantar Visualization System. Applied Sciences, 10(4), 1359. https://doi.org/10.3390/app10041359