Thermal Comfort Applied in Hospital Environments: A Literature Review



Abstract
1. Introduction
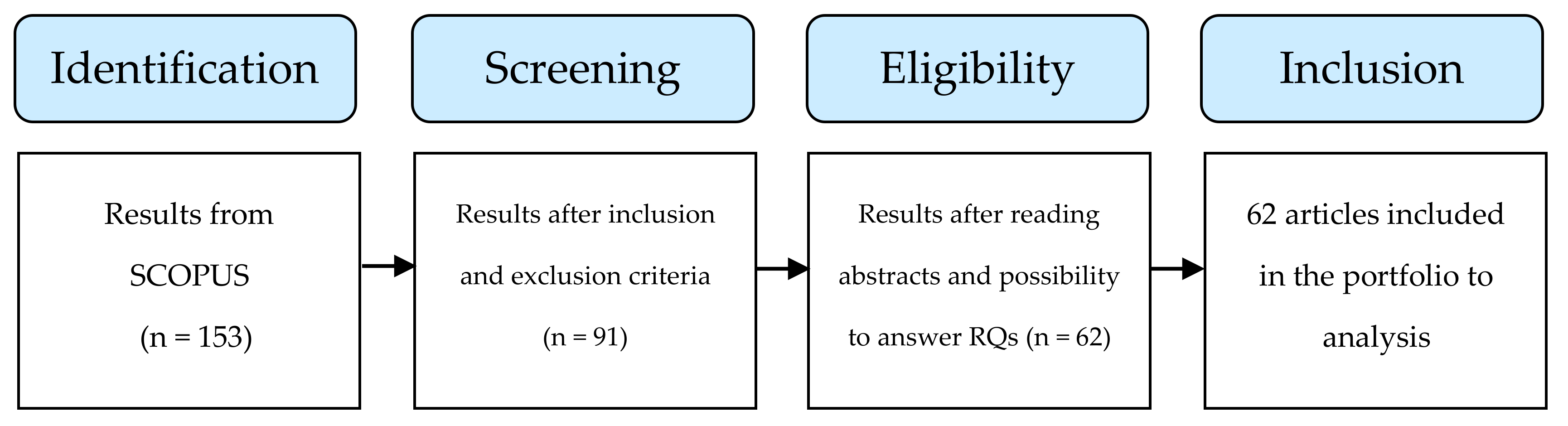
2. Methods
2.1. Research Questions (RQs)
- (a)
- According to Djongyang et al. [23] and de Dear et al. [3], thermal comfort is required in indoor environments because it directly affects people’s perception, in terms of health/wellbeing and productivity. On the other hand, Thapa et al. [24] claim that optimizing the energy used in buildings, whether for heating or for cooling, is a reality today, because there is a need for energy saving. Based on these premises, RQ1 is formulated:RQ1: Considering studies on thermal comfort in hospital environments, what are the main aspects that are taken into account: health/wellbeing, productivity or energy saving?
- (b)
- According to Humphreys and Nicol [25], the PMV model does not consider the adaptive actions that people undertake in indoor environments in order to maintain their comfort, leading PMV to underestimate or overestimate the real thermal sensation felt by people in buildings. Based on this premise, RQ2 is formulated:RQ2: Considering studies on thermal comfort in hospital environments, which relate PMV and real thermal sensation, studies indicate that PMV predicted well, underestimates or overestimates the real thermal sensation?
- (c)
- Different levels of activity require specific environmental conditions for people, in order to achieve thermal comfort. Thus, it is important to define the target group of the research [26]. In addition to this factor, the type of environment in which people are inserted in the hospitals usually has its own standardized environmental requirements, determined by the type of activity to be performed [21]. Based on these premises, RQ3 is formulated:RQ3: Considering studies on thermal comfort in hospital environments, what was the most evaluated group and which area within the hospital was most evaluated?
- (d)
- The hospital environment is complex, since it can change from waiting rooms to operating rooms and intensive care units (ICUs), which demand different requirements for environmental parameters due to the type of activity/care. The concern with planning the environment must go far beyond simply offering thermal comfort to its occupants [27]. Thus, the hospital environment should be prepared to offer a good indoor environmental quality (IEQ). Based on these premises, RQ4 is formulated:RQ4: What other parameters of indoor environmental quality (IEQ) were evaluated, in addition to thermal comfort?
2.2. Method for Bibliographic Search
2.3. Tool for Content Analysis
3. Results
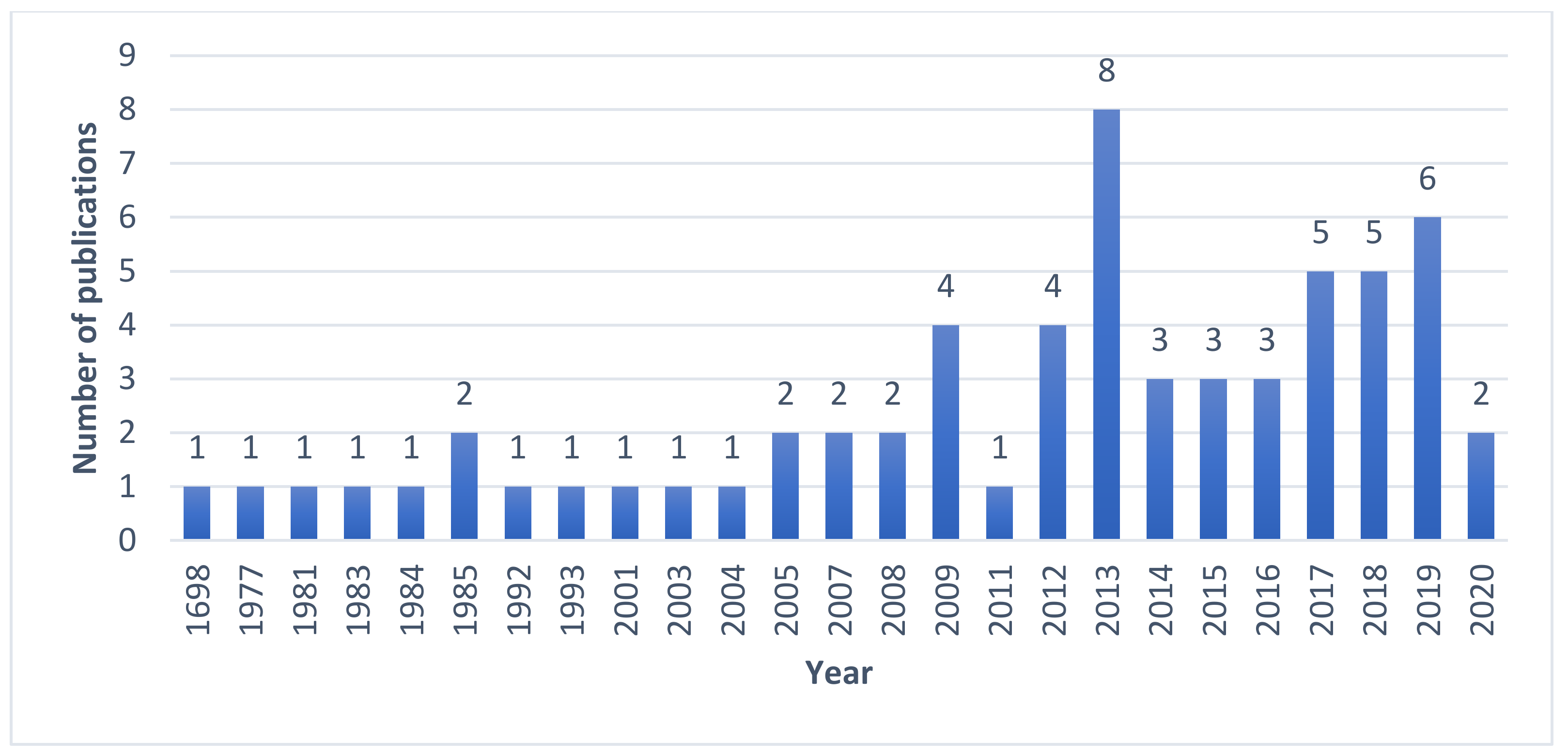
3.1. Preliminary Results
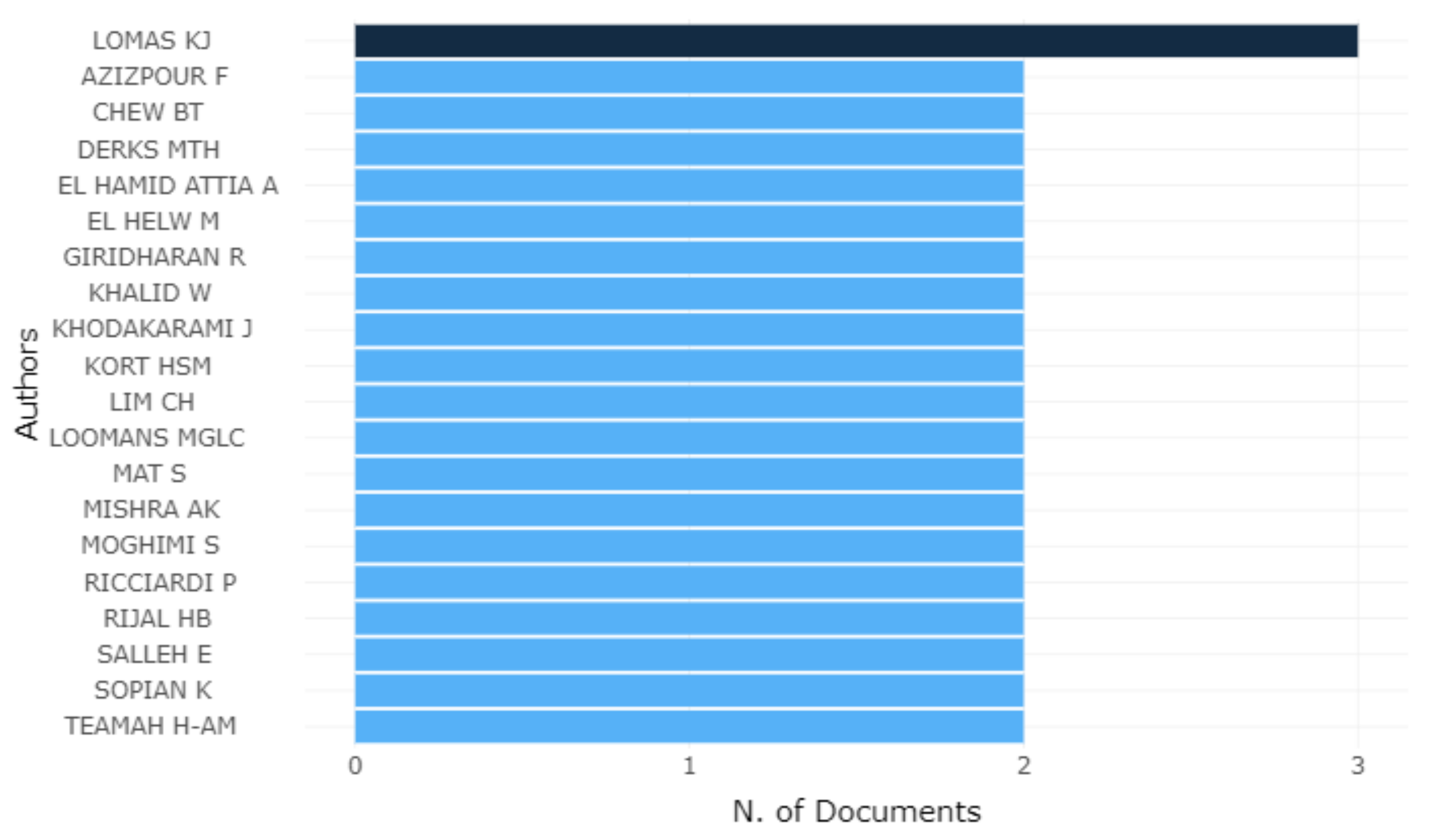
3.2. General Considerations of Studies
4. Discussion
4.1. RQ1: Considering Studies in Thermal Comfort in Hospital Environments, What Are the Main Aspects That Are Taken Into Account: Health/Wellbeing, Productivity or Energy Saving?
4.2. RQ2: Considering Studies of Thermal Comfort in Hospital Environments, Which Relate PMV and Real Thermal Sensation, Studies Indicate That PMV Predicted Well, Underestimates or Overestimates the Real Thermal Sensation?
4.3. RQ3: Considering Studies in Thermal Comfort in Hospital Environments, What Was the Most Evaluated Group and Which Area Within Hospital Was Most Evaluated?
4.4. RQ4: What Other Parameters of Indoor Environmental Quality (IEQ) Were Evaluated, Aside from Thermal Comfort?
5. Final Considerations
6. Study Limitations
Author Contributions
Funding
Conflicts of Interest
References
- Peeters, L.; De Dear, R.; Hensen, J.; D’Haeseleer, W. Thermal comfort in residential buildings: Comfort values and scales for building energy simulation. Appl. Energy 2009, 86, 772–780. [Google Scholar] [CrossRef]
- Fanger, P.O. Thermal Comfort. Analysis and Applications in Environmental Engineering; McGraw-Hill: New York, NY, USA, 1970. [Google Scholar]
- De Dear, R.J.; Akimoto, T.; Arens, E.A.; Brager, G.; Candido, C.; Cheong, K.W.D.; Li, B.; Nishihara, N.; Sekhar, S.C.; Tanabe, S.; et al. Progress in thermal comfort research over the last twenty years. Indoor Air 2013, 23, 442–461. [Google Scholar] [CrossRef] [PubMed]
- Singh, M.K.; Ooka, R.; Rijal, H.B.; Takasu, M. Adaptive thermal comfort in the offices of North-East India in autumn season. Build. Environ. 2017, 124, 14–30. [Google Scholar] [CrossRef]
- Märzinger, T.; Österreicher, D. Supporting the Smart Readiness Indicator—A Methodology to Integrate A Quantitative Assessment of the Load Shifting Potential of Smart Buildings. Energies 2019, 12, 1955. [Google Scholar] [CrossRef]
- Alahmer, A.; Mayyas, A.T.; Mayyas, A.A.; Omar, M.; Shan, D. Vehicular thermal comfort models; a comprehensive review. Appl. Therm. Eng. 2011, 31, 995–1002. [Google Scholar] [CrossRef]
- Jang, M.; Koh, C.; Moon, I. Review of thermal comfort design based on PMV/PPD in cabins of Korean maritime patrol vessels. Build. Environ. 2007, 42, 55–61. [Google Scholar] [CrossRef]
- Srinavin, K.; Mohamed, S. Thermal environment and construction workers’ productivity: Some evidence from Thailand. Build. Environ. 2003, 38, 339–345. [Google Scholar] [CrossRef]
- Kwok, A.G.; Chun, C. Thermal comfort in Japanese schools. Sol. Energy 2003, 74, 245–252. [Google Scholar] [CrossRef]
- Jing, S.; Lei, Y.; Wang, H.; Song, C.; Yan, X. Thermal comfort and energy-saving potential in university classrooms during the heating season. Energy Build. 2019, 202, 109390. [Google Scholar] [CrossRef]
- Wu, J.; Li, X.; Lin, Y.; Yan, Y.; Tu, J.; Yang, L. A PMV-based HVAC control strategy for office rooms subjected to solar radiation. Build. Environ. 2020, 177, 106863. [Google Scholar] [CrossRef]
- Pinto, N.D.M.; Xavier, A.A.D.P.; Hatakeyama, K. Thermal Comfort in Industrial Environment: Conditions and Parameters. Procedia Manuf. 2015, 3, 4999–5006. [Google Scholar] [CrossRef]
- World Health Organization. WHO Announces COVID-19 Outbreak a Pandemic n.d. Available online: http://www.euro.who.int/en/health-topics/health-emergencies/coronavirus covid19/news/news/2020/3/who-announces-covid-19-outbreak-a-pandemic (accessed on 15 June 2020).
- Wyon, D.P.; Lidwell, O.M.; Williams, R.E.O. Thermal comfort during surgical operations. J. Hyg. 1968, 66, 229–248. [Google Scholar] [CrossRef]
- Smith, R.M.; Rae, A. Thermal comfort of patients in hospital ward areas. J. Hyg. 1977, 78, 17–26. [Google Scholar] [CrossRef] [PubMed]
- Berardi, B.M.; Leoni, E. Indoor air climate and microbiological airborne: Contamination in various hospital areas. Zentralblatt Hygiene Umweltmedizin 1993, 194, 405–418. [Google Scholar]
- Del Ferraro, S.; Iavicoli, S.; Russo, S.; Molinaro, V. A field study on thermal comfort in an Italian hospital considering differences in gender and age. Appl. Ergon. 2015, 50, 177–184. [Google Scholar] [CrossRef] [PubMed]
- Fabbri, K.; Gaspari, J.; Vandi, L. Indoor Thermal Comfort of Pregnant Women in Hospital: A Case Study Evidence. Sustainability 2019, 11, 6664. [Google Scholar] [CrossRef]
- Mui, K.W.; Wong, L.T.; Fong, K.N.K.; Wong, W.W.Y. Evaluation of indoor environment quality of elderly centers of Hong Kong. Int. J. Hous. Sci. Appl. 2008, 32, 121–131. [Google Scholar]
- Tartarini, F.; Cooper, P.; Fleming, R. Thermal perceptions, preferences and adaptive behaviours of occupants of nursing homes. Build. Environ. 2018, 132, 57–69. [Google Scholar] [CrossRef]
- Verheyen, J.; Theys, N.; Allonsius, L.; Descamps, F. Thermal comfort of patients: Objective and subjective measurements in patient rooms of a Belgian healthcare facility. Build. Environ. 2011, 46, 1195–1204. [Google Scholar] [CrossRef]
- Khodakarami, J.; Nasrollahi, N. Thermal comfort in hospitals—A literature review. Renew. Sustain. Energy Rev. 2012, 16, 4071–4077. [Google Scholar] [CrossRef]
- Djongyang, N.; Tchinda, R.; Njomo, D. Thermal comfort: A review paper. Renew. Sustain. Energy Rev. 2010, 14, 2626–2640. [Google Scholar] [CrossRef]
- Thapa, S.; Bansal, A.K.; Panda, G.K. Adaptive thermal comfort in the residential buildings of north east India—An effect of difference in elevation. Build. Simul. 2017, 11, 245–267. [Google Scholar] [CrossRef]
- Humphreys, M.A.; Nicol, J.F. The validity of ISO-PMV for predicting comfort votes in every-day thermal environments. Energy Build. 2002, 34, 667–684. [Google Scholar] [CrossRef]
- Khalid, W.; Salim, S.A.Z.S.; Rijal, H.B.; Yakub, F. Investigation of comfort temperature and thermal adaptation for patients and visitors in Malaysian hospitals. Energy Build. 2019, 183, 484–499. [Google Scholar] [CrossRef]
- Cheong, K.; Chong, K.; Cheong, D.K.W. Development and application of an indoor air quality audit to an air-conditioned building in Singapore. Build. Environ. 2001, 36, 181–188. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Broday, E.E.; Xavier, A.A.P. A systematic literature review on thermal response votes (Tsv) and predicted mean vote (pmv). In Occupational Safety and Hygiene VI; Carneiro, P., Cordeiro, P., Costa, N., Arezes, P.M., Baptista, J.S., Perestrelo, G., Melo, R.B., Barroso, M., et al., Eds.; SHO 2018, UTFPR—Federal University of Technology of Paraná; CRC Press/Balkema: Ponta Grossa, Brazil, 2018; pp. 13–17. [Google Scholar]
- Zlatar, T.; Costa, J.T.; Vaz, M.; Baptista, J.S. Influence of severe cold thermal environment on core and skin temperatures: A systematic review. Work 2019, 62, 337–352. [Google Scholar] [CrossRef]
- Aria, M.; Cuccurullo, C. bibliometrix: An R-tool for comprehensive science mapping analysis. J. Inf. 2017, 11, 959–975. [Google Scholar] [CrossRef]
- Critical Appraisal Skills Programme. CASP (Systematic Review) Checklist. 2018. Available online: https://casp-uk.net/wp-content/uploads/2018/01/CASP-Systematic-Review-Checklist_2018.pdf (accessed on 18 August 2020).
- Critical Appraisal Skills Programme CASP (Qualitative) Checklist. 2018. Available online: https://casp-uk.net/wp-content/uploads/2018/01/CASP-Qualitative-Checklist-2018.pdf (accessed on 18 August 2020).
- Gatea, A.A.; Batcha, M.F.M.; Taweekun, J. Energy efficiency and thermal comfort in hospital buildings: A review. Int. J. Integr. Eng. 2020, 12, 33–41. [Google Scholar]
- Matsui, J. A study of thermal comfort conditions of patients—Thermal sensation of patients for thermal environment in hospital wards. J. Showa Med. Assoc. 1981, 41, 271–284. [Google Scholar]
- Wheldon, A.; Hull, D. The thermal environment in the neonatal nursery. Build. Environ. 1983, 18, 163–169. [Google Scholar] [CrossRef]
- Bovenzi, M.; Fiorito, A. Thermal comfort in a hospital. Med. Del. Lav. 1984, 75, 125–132. [Google Scholar]
- Sodha, M.; Sharma, A.; Singh, S.; Bansal, N.; Kumar, A. Evaluation of an earth—Air tunnel system for cooling/heating of a hospital complex. Build. Environ. 1985, 20, 115–122. [Google Scholar] [CrossRef]
- Terzi, R.; Marcaletti, G.; Catenacci, G. [Evaluation of thermal comfort parameters in the operating rooms of a hospital surgical department]. Boll. Della Soc. Ital. Boil. Sper. 1985, 61, 1009–1014. [Google Scholar]
- Chen, Q.; Jiang, Z.; Moser, A. Control of Airborne Particle Concentration and Draught Risk in an Operating Room. Indoor Air 1992, 2, 154–167. [Google Scholar] [CrossRef]
- Chow, T.-T.; Yang, X.-Y. Performance of ventilation system in a non-standard operating room. Build. Environ. 2003, 38, 1401–1411. [Google Scholar] [CrossRef]
- Külpmann, R.; Meierhans, R. New air conditioning concepts for better reduction of air pollution. Anasthesiol. Intensivmed. 2004, 45, 526–528. [Google Scholar]
- Hashiguchi, N.; Hirakawa, M.; Tochihara, Y.; Kaji, Y.; Karaki, C. Thermal Environment and Subjective Responses of Patients and Staff in a Hospital during Winter. J. Physiol. Anthr. Appl. Hum. Sci. 2005, 24, 111–115. [Google Scholar] [CrossRef]
- Skoog, J.; Fransson, N.; Jagemar, L. Thermal environment in Swedish hospitals. Energy Build. 2005, 37, 872–877. [Google Scholar] [CrossRef]
- Hwang, R.-L.; Lin, T.-P.; Cheng, M.-J.; Chien, J.-H. Patient thermal comfort requirement for hospital environments in Taiwan. Build. Environ. 2007, 42, 2980–2987. [Google Scholar] [CrossRef]
- Mazzacane, S.; Giaconia, C.; Costanzo, S.; Cusumano, A. A Survey on the Thermal Conditions Experienced by a Surgical Team. Indoor Built Environ. 2007, 16, 99–109. [Google Scholar] [CrossRef]
- Khodakarami, J.; Knight, I. Required and Current Thermal Conditions for Occupants in Iranian Hospitals. HVAC&R Res. 2008, 14, 175–193. [Google Scholar]
- Ho, S.H.; Rosario, L.; Rahman, M.M. Three-dimensional analysis for hospital operating room thermal comfort and contaminant removal. Appl. Therm. Eng. 2009, 29, 2080–2092. [Google Scholar] [CrossRef]
- Lomas, K.J.; Ji, Y. Resilience of naturally ventilated buildings to climate change: Advanced natural ventilation and hospital wards. Energy Build. 2009, 41, 629–653. [Google Scholar] [CrossRef]
- Masia, M.D.; Dettori, M.; Liperi, G.; Deriu, G.M.; Posadino, S.; Maida, G.; Mura, I. Thermal comfort in perioperatory risk’s evaluation. Ann. Ig. 2009, 21, 251–258. [Google Scholar] [PubMed]
- Thermal comfort study of hospital workers in MalaysiaYau YH, Chew BT. Thermal comfort study of hospital workers in Malaysia. Indoor Air 2009, 19, 500–510. [Google Scholar] [CrossRef]
- Adamu, Z.; Price, A.D.F.; Cook, M. Performance evaluation of natural ventilation strategies for hospital wards—A case study of Great Ormond Street Hospital. Build. Environ. 2012, 56, 211–222. [Google Scholar] [CrossRef]
- Lomas, K.J.; Giridharan, R. Thermal comfort standards, measured internal temperatures and thermal resilience to climate change of free-running buildings: A case-study of hospital wards. Build. Environ. 2012, 55, 57–72. [Google Scholar] [CrossRef]
- Pourshaghaghy, A.; Omidvari, M. Examination of thermal comfort in a hospital using PMV–PPD model. Appl. Ergon. 2012, 43, 1089–1095. [Google Scholar] [CrossRef]
- Ascione, F.; Bianco, N.; De Masi, R.F.; Vanoli, G.P. Rehabilitation of the building envelope of hospitals: Achievable energy savings and microclimatic control on varying the HVAC systems in Mediterranean climates. Energy Build. 2013, 60, 125–138. [Google Scholar] [CrossRef]
- Azizpour, F.; Moghimi, S.; Lim, C.H.; Mat, S.; Salleh, E.; Sopian, K. A Thermal Comfort Investigation of a Facility Department of a Hospital in Hot-Humid Climate: Correlation between Objective and Subjective Measurements. Indoor Built Environ. 2012, 22, 836–845. [Google Scholar] [CrossRef]
- Azizpour, F.; Moghimi, S.; Salleh, E.; Mat, S.; Lim, C.; Sopian, K. Thermal comfort assessment of large-scale hospitals in tropical climates: A case study of University Kebangsaan Malaysia Medical Centre (UKMMC). Energy Build. 2013, 64, 317–322. [Google Scholar] [CrossRef]
- Azmoon, H.; Dehghan, H.; Akbari, J.; Soury, S. The Relationship between Thermal Comfort and Light Intensity with Sleep Quality and Eye Tiredness in Shift Work Nurses. J. Environ. Public Heal. 2013, 2013, 1–5. [Google Scholar] [CrossRef] [PubMed]
- De Giuli, V.; Zecchin, R.; Salmaso, L.; Corain, L.; De Carli, M. Measured and perceived indoor environmental quality: Padua Hospital case study. Build. Environ. 2013, 59, 211–226. [Google Scholar] [CrossRef]
- Giridharan, R.; Lomas, K.J.; Short, C.A.; Fair, A.J. Performance of hospital spaces in summer: A case study of a ’Nucleus’-type hospital in the UK Midlands. Energy Build. 2013, 66, 315–328. [Google Scholar] [CrossRef]
- El Hamid, A.A.; El Helw, M.; Teamah, H.-A.M. Three-dimensional thermal comfort analysis for hospital operating room with the effect of door gradually opened: Part (II) effect on mean age of the air and predicted mean vote distribution. CFD Lett. 2013, 5, 20–31. [Google Scholar]
- El Hamid, A.A.; El Helw, M.; Teamah, H.-A.M. Three-dimensional thermal comfort analysis for hospital operating room with the effect of door gradually opened part (I) effect on velocity and temperature distributions. CFD Lett. 2013, 5, 6–19. [Google Scholar]
- Dovjak, M.; Shukuya, M.; Krainer, A. Individualisation of personal space in hospital environment. Int. J. Exergy 2014, 14, 125–155. [Google Scholar] [CrossRef]
- Van Gaever, R.; Jacobs, V.; Diltoer, M.; Peeters, L.; Vanlanduit, S. Thermal comfort of the surgical staff in the operating room. Build. Environ. 2014, 81, 37–41. [Google Scholar] [CrossRef]
- Yau, Y.H.; Chew, B. Adaptive thermal comfort model for air-conditioned hospitals in Malaysia. Build. Serv. Eng. Res. Technol. 2013, 35, 117–138. [Google Scholar] [CrossRef]
- Rodrigues, N.J.; Oliveira, R.F.; Teixeira, S.; Miguel, A.S.; Teixeira, J.C.; Baptista, J.S. Thermal comfort assessment of a surgical room through computational fluid dynamics using local PMV index. Work 2015, 51, 445–456. [Google Scholar] [CrossRef] [PubMed]
- Uścinowicz, P.; Chludzińska, M.; Bogdan, A. Thermal environment conditions in Polish operating rooms. Build. Environ. 2015, 94, 296–304. [Google Scholar] [CrossRef]
- Cannistraro, G.; Cannistraro, M. Hypothermia Risk, Monitoring and Environment Control in Operating Rooms. Int. J. Heat Technol. 2016, 34, 165–171. [Google Scholar] [CrossRef]
- Carvalhais, C.; Santos, J.; Vieira da Silva, M. Analytical and subjective interpretation of thermal comfort in hospitals: A case study in two sterilization services. J. Toxicol. Environ. Health Part A Curr. Issues 2016, 79, 299–306. [Google Scholar] [CrossRef] [PubMed]
- Jankowski, T.; Młynarczyk, M. An Impact of The Efficient Functioning of the Ventilation and Air-Conditioning System on Thermal Comfort of the Medical Staff in the Operating Room. J. Ecol. Eng. 2016, 17, 114–119. [Google Scholar] [CrossRef]
- Nematchoua, M.K.; Ricciardi, P.; Reiter, S.; Asadi, S.; Demers, C.M. Thermal comfort and comparison of some parameters coming from hospitals and shopping centers under natural ventilation: The case of Madagascar Island. J. Build. Eng. 2017, 13, 196–206. [Google Scholar] [CrossRef]
- Lan, L.; Tushar, W.; Otto, K.; Yuen, C.; Wood, K. Thermal comfort improvement of naturally ventilated patient wards in Singapore. Energy Build. 2017, 154, 499–512. [Google Scholar] [CrossRef]
- Nematchoua, M.K.; Ricciardi, P.; Buratti, C. Statistical analysis of indoor parameters an subjective responses of building occupants in a hot region of Indian ocean; a case of Madagascar island. Appl. Energy 2017, 208, 1562–1575. [Google Scholar] [CrossRef]
- Pirsaheb, M.; Sohrabi, Y.; Yarmohammadi, H. Assessment of Thermal Comfort in Hospital Wards of Kermanshah, Iran, based on the Standards. Indian J. Public Health Res. Dev. 2017, 8, 357. [Google Scholar] [CrossRef]
- Sattayakorn, S.; Ichinose, M.; Sasaki, R. Clarifying thermal comfort of healthcare occupants in tropical region: A case of indoor environment in Thai hospitals. Energy Build. 2017, 149, 45–57. [Google Scholar] [CrossRef]
- Lawrence, I.D.; Jayabal, S.; Thirumal, P. Indoor air quality investigations in hospital patient room. Int. J. Biomed. Eng. Technol. 2018, 27, 124–138. [Google Scholar] [CrossRef]
- Derks, M.; Mishra, A.K.; Loomans, M.; Kort, H. Understanding thermal comfort perception of nurses in a hospital ward work environment. Build. Environ. 2018, 140, 119–127. [Google Scholar] [CrossRef]
- Khalid, W.; Zaki, S.A.; Rijal, H.B.; Yakub, F. Thermal comfort requirements for different occupants in Malaysian hospital in-patient wards. J. Adv. Res. Fluid Mech. Therm. Sci. 2018, 43, 128–140. [Google Scholar]
- Loomans, M.; Mishra, A.K.; Derks, M.; Kraakman, J.; Kort, H. Occupant response to transitions across indoor thermal environments in two different workspaces. Build. Environ. 2018, 144, 402–411. [Google Scholar] [CrossRef]
- Alfa, M.T.; Öztürk, A. Perceived indoor environmental quality of hospital wards and patients’ outcomes: A study of a general hospital, Minna, Nigeria. Appl. Ecol. Environ. Res. 2019, 17, 8235–8259. [Google Scholar] [CrossRef]
- Mora, R.; Meteyer, M. Thermal comfort in health-care settings. ASHRAE J. 2019, 61, 10–19. [Google Scholar]
- Sameh, H.H.; Omar, E.M.; Ezz El-Dein, N.M. Criteria for evaluating the saving and production of energy in hospitals “nursing units”. Int. J. Eng. Res. Technol. 2019, 12, 670–678. [Google Scholar]
- Wu, Y.; Meng, Q.; Li, L.; Mu, J. Interaction between Sound and Thermal Influences on Patient Comfort in the Hospitals of China’s Northern Heating Region. Appl. Sci. 2019, 9, 5551. [Google Scholar] [CrossRef]
- Angelova, R.A.; Velichkova, R. Thermophysiological Comfort of Surgeons and Patient in an Operating Room Based on PMV-PPD and PHS Indexes. Appl. Sci. 2020, 10, 1801. [Google Scholar] [CrossRef]
- Geng, Y.; Ji, W.; Lin, B.; Zhu, Y. The impact of thermal environment on occupant IEQ perception and productivity. Build. Environ. 2017, 121, 158–167. [Google Scholar] [CrossRef]
- Wong, L.; Mui, K.; Tsang, T. An open acceptance model for indoor environmental quality (IEQ). Build. Environ. 2018, 142, 371–378. [Google Scholar] [CrossRef]
- Zakaria Abouleish, M.Y. Indoor Air Quality and Coronavirus Disease (COVID-19) [published online ahead of print, 2020 May 7]. Public Health 2020. [Google Scholar] [CrossRef]
- Correia, G.; Rodrigues, L.; Da Silva, M.G.; Gonçalves, T. Airborne route and bad use of ventilation systems as non-negligible factors in SARS-CoV-2 transmission. Med Hypotheses 2020, 141, 109781. [Google Scholar] [CrossRef] [PubMed]
- Adela Cortina. REHVA Covid19 HVAC Guidance. Eur. Univ. Inst. 2012, 2020, 2–5. [Google Scholar]
- Zhang, J. Integrating IAQ control strategies to reduce the risk of asymptomatic SARS CoV-2 infections in classrooms and open plan offices. Sci. Technol. Built Environ. 2020, 2020, 1–6. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Papers in English | Papers in other languages |
| Articles published until 2020 | Papers that do not provide the complete basic information (author, title, year of publication or source) |
| Papers that focus on the relation of thermal comfort and hospital environments | Papers in thermal comfort, but not in hospital environments |
| Papers that might answer RQ1, RQ2, RQ3, and RQ4 | Repeated papers |
| Search Strategy | Keywords and Combinations | Results |
|---|---|---|
| Database: SCOPUS. Search in: Title, Abstract and Keywords. Type of Article: Review and Article | (“thermal comfort” OR “thermal conditions” OR “predicted mean vote” OR “predicted percentage of dissatisfied”) AND (“hospital” OR “health centers” OR “elderly centers”) | 153 articles |
| Reference | Title | Year | Country | Journal | Citations |
|---|---|---|---|---|---|
| [22] | Thermal comfort in hospitals—A literature review | 2012 | Iran | Renewable and Sustainable Energy Reviews | 109 |
| [34] | Energy efficiency and thermal comfort in hospital buildings: A review | 2020 | Malaysia | International Journal of Integrated Engineering | 0 |
| Authors and References | Title | Year | Country | Journal | Citations | Environment |
|---|---|---|---|---|---|---|
| Wyon, Lidwell and Williams [14] | Thermal comfort during surgical operations | 1968 | United Kingdom | Journal of Hygiene | 58 | Hospital |
| Smith and Rae [15] | Thermal comfort of patients in hospital ward areas | 1977 | United Kingdom | Journal of Hygiene | 13 | Hospital |
| Matsui [35] | A study of thermal comfort conditions of patients—thermal sensation of patients for thermal environment in hospital wards | 1981 | Japan | Journal of the Showa Medical Association | 5 | Hospital |
| Wheldon and Hull [36] | The thermal environment in the neonatal nursery | 1983 | United Kingdom | Building and Environment | 5 | Hospital |
| Bovenzi and Fiorito [37] | Thermal comfort in a hospital | 1984 | Italy | Medicina del lavoro | Not available | Hospital |
| Sodha et al. [38] | Evaluation of an earth-air tunnel system for cooling/heating of a hospital complex | 1985 | India | Building and Environment | 120 | Hospital |
| Terzi, Marcaletti and Catenacci [39] | Evaluation of thermal comfort parameters in the operating rooms of a hospital surgical department | 1985 | Italy | Bollettino della Societa italiana di biologia sperimentale | 0 | Hospital |
| Chen, Jiang and Moser [40] | Control of Airborne Particle Concentration and Draught Risk in an Operating Room | 1992 | Switzerland | Indoor Air | 54 | Hospital |
| Berardi and Leoni [16] | Indoor air climate and microbiological airborne: contamination in various hospital areas. | 1993 | Italy | International journal of hygiene and environmental medicine | 16 | Hospital |
| Cheong and Chong [27] | Development and application of an indoor air quality audit to an air-conditioned building in Singapore | 2001 | Singapore | Building and Environment | 85 | Hospital |
| Chow and Yang [41] | Performance of ventilation system in a non-standard operating room | 2003 | Hong Kong | Building and Environment | 122 | Hospital |
| Külpmann and Meierhans [42] | New air conditioning concepts for better reduction of air pollution | 2004 | Switzerland | Anasthesiologie und Intensivmedizin | 0 | Hospital |
| Hashiguchi et al. [43] | Thermal environment and subjective responses of patients and staff in a hospital during winter | 2005 | Japan | Journal of Physiological Anthropology and Applied Human Science | 25 | Hospital |
| Skoog, Frasson and Jagemar [44] | Thermal environment in Swedish hospitals: Summer and winter measurements | 2005 | Sweden | Energy and Buildings | 88 | Hospital |
| Hwang et al. [45] | Patient thermal comfort requirement for hospital environments in Taiwan | 2007 | China | Building and Environment | 123 | Hospital |
| Mazzacane et al. [46] | A survey on the thermal conditions experienced by a surgical team | 2007 | Italy | Indoor and Built Environment | 18 | Hospital |
| Khodakarami and Knight [47] | Required and current thermal conditions for occupants in Iranian hospitals | 2008 | Iran | HVAC and R Research | 16 | Hospital |
| Mui et al. [19] | Evaluation of indoor environment quality of elderly centers of Hong Kong | 2008 | China | International Journal for Housing Science and Its Applications | 10 | Elderly Center |
| Ho, Rosario and Rahman [48] | Three-dimensional analysis for hospital operating room thermal comfort and contaminant removal | 2009 | United States | Applied Thermal Engineering | 80 | Hospital |
| Lomas and Ji [49] | Resilience of naturally ventilated buildings to climate change: Advanced natural ventilation and hospital wards | 2009 | United Kingdom | Energy and Buildings | 96 | Hospital |
| Masia et al. [50] | Thermal comfort in perioperatory risk’s evaluation | 2009 | Italy | Annali di igiene: medicina preventiva e di comunità | 1 | Hospital |
| Yau and Chew [51] | Thermal comfort study of hospital workers in Malaysia | 2009 | Malaysia | Indoor Air | 65 | Hospital |
| Verheyen et al. [21] | Thermal comfort of patients: Objective and subjective measurements in patient rooms of a Belgian healthcare facility | 2011 | Belgium | Building and Environment | 85 | Health Center |
| Adamu, Price and Cook [52] | Performance evaluation of natural ventilation strategies for hospital wards—A case study of Great Ormond Street Hospital | 2012 | United Kingdom | Building and Environment | 31 | Hospital |
| Lomas and Giridharan [53] | Thermal comfort standards, measured internal temperatures and thermal resilience to climate change of free-running buildings: A case-study of hospital wards | 2012 | United Kingdom | Building and Environment | 124 | Hospital |
| Pourshaghaghy and Omidvari [54] | Examination of thermal comfort in a hospital using PMV-PPD model | 2012 | Iran | Applied Ergonomics | 95 | Hospital |
| Ascione et al. [55] | Rehabilitation of the building envelope of hospitals: Achievable energy savings and microclimatic control on varying the HVAC systems in Mediterranean climates | 2013 | Italy | Energy and Buildings | 74 | Health Center |
| Azizpour et al. [56] | A thermal comfort investigation of a facility department of a hospital in hot-humid climate: Correlation between objective and subjective measurements | 2013 | Malaysia | Indoor and Built Environment | 25 | Hospital |
| Azizpour et al. [57] | Thermal comfort assessment of large-scale hospitals in tropical climates: A case study of University Kebangsaan Malaysia Medical Centre (UKMMC) | 2013 | Malaysia | Energy and Buildings | 58 | Hospital |
| Azmoon et al. [58] | The relationship between thermal comfort and light intensity with sleep quality and eye tiredness in shift work nurses. | 2013 | Iran | Journal of environmental and public health | 45 | Hospital |
| De Giuli et al. [59] | Measured and perceived indoor environmental quality: Padua Hospital case study | 2013 | Italy | Building and Environment | 63 | Hospital |
| Giridharan et al. [60] | Performance of hospital spaces in summer: A case study of a ’Nucleus’-type hospital in the UK Midlands | 2013 | United Kingdom | Energy and Buildings | 25 | Hospital |
| el Hamid Attia, El Helw and Teamah [61] | Three-dimensional thermal comfort analysis for hospital operating room with the effect of door gradually opened: Part (II) effect on mean age of the air and predicted mean vote distribution | 2013 | Egypt | CFD Letters | 2 | Hospital |
| el Hamid Attia, El Helw and Teamah [62] | Three-dimensional thermal comfort analysis for hospital operating room with the effect of door gradually opened part (I) effect on velocity and temperature distributions | 2013 | Egypt | CFD Letters | 2 | Hospital |
| Dovjak, Shukuya and Krainer [63] | Individualisation of personal space in hospital environment | 2014 | Slovenia | International Journal of Exergy | 23 | Hospital |
| Van Gaever et al. [64] | Thermal comfort of the surgical staff in the operating room | 2014 | Belgium | Building and Environment | 54 | Hospital |
| Yau and Chew [65] | Adaptive thermal comfort model for air-conditioned hospitals in Malaysia | 2014 | Malaysia | Building Services Engineering Research and Technology | 21 | Hospital |
| Del Ferraro et al. [17] | A field study on thermal comfort in an Italian hospital considering differences in gender and age | 2015 | Italy | Applied Ergonomics | 51 | Hospital |
| Rodrigues et al. [66] | Thermal comfort assessment of a surgical room through computational fluid dynamics using local PMV index | 2015 | Portugal | Work | 7 | Hospital |
| Uścinowicz, Chludziʼnska and Bogdan [67] | Thermal environment conditions in Polish operating rooms | 2015 | Poland | Building and Environment | 14 | Hospital |
| Cannistraro and Cannistraro [68] | Hypothermia risk, monitoring and environment control in operating rooms | 2016 | Italy | International Journal of Heat and Technology | 25 | Hospital |
| Carvalhais et al. [69] | Analytical and subjective interpretation of thermal comfort in hospitals: A case study in two sterilization services | 2016 | Portugal | Journal of Toxicology and Environmental Health | 2 | Hospital |
| Jankowski and Mlstrokynarczyk [70] | An impact of the efficient functioning of the ventilation and air-conditioning system on thermal comfort of the medical staff in the operating room | 2016 | Poland | Journal of Ecological Engineering | 6 | Hospital |
| Nematchoua et al. [71] | Thermal comfort and comparison of some parameters coming from hospitals and shopping centers under natural ventilation: The case of Madagascar Island | 2017 | Madagascar | Journal of Building Engineering | 20 | Hospital |
| Lan et al. [72] | Thermal comfort improvement of naturally ventilated patient wards in Singapore | 2017 | Singapore | Energy and Buildings | 8 | Hospital |
| Nematchoua, Ricciardi and Buratti [73] | Statistical analysis of indoor parameters an subjective responses of building occupants in a hot region of Indian ocean: a case of Madagascar island | 2017 | Madagascar | Applied Energy | 15 | Hospital |
| Pirsaheb, Sohrabi and Yarmohammadi [74] | Assessment of thermal comfort in hospital wards of Kermanshah, Iran, based on the standards | 2017 | Iran | Indian Journal of Public Health Research and Development | 1 | Hospital |
| Sattayakorn, Ichinose and Sasaki [75] | Clarifying thermal comfort of healthcare occupants in tropical region: A case of indoor environment in Thai hospitals | 2017 | Thailand | Energy and Buildings | 25 | Hospital |
| Lawrence, Jayabal and Thirumal [76] | Indoor air quality investigations in hospital patient room | 2018 | India | International Journal of Biomedical Engineering and Technology | 1 | Hospital |
| Derks et al. [77] | Understanding thermal comfort perception of nurses in a hospital ward work environment | 2018 | Netherlands | Building and Environment | 18 | Hospital |
| Khalid et al. [78] | Thermal comfort requirements for different occupants in Malaysian hospital in-patient wards | 2018 | Malaysia | Journal of Advanced Research in Fluid Mechanics and Thermal Sciences | 7 | Hospital |
| Loomans et al. [79] | Occupant response to transitions across indoor thermal environments in two different workspaces | 2018 | United Kingdom | Building and Environment | 3 | Hospital |
| Tartarini, Cooper and Fleming [20] | Thermal perceptions, preferences and adaptive behaviours of occupants of nursing homes | 2018 | Australia | Building and Environment | 15 | Elderly Center |
| Alfa and Öztürk [80] | Perceived indoor environmental quality of hospital wards and patients’ outcomes: A study of a general hospital, Minna, Nigeria | 2019 | Nigeria | Applied Ecology and Environmental Research | 0 | Hospital |
| Fabbri, Gaspari and Vandi [18] | Indoor thermal comfort of pregnant women in hospital: A case study evidence | 2019 | Italy | Sustainability (Switzerland) | 0 | Hospital |
| Khalid et al. [26] | Investigation of comfort temperature and thermal adaptation for patients and visitors in Malaysian hospitals | 2019 | Malaysia | Energy and Buildings | 18 | Hospital |
| Mora and Meteyer [81] | Thermal comfort in health-care settings | 2019 | Canada | ASHRAE Journal | 0 | Hospital |
| Sameh, Omar and Ezz El-Dein [82] | Criteria for evaluating the saving and production of energy in hospitals “nursing units” | 2019 | Egypt | International Journal of Engineering Research and Technology | 0 | Hospital |
| Wu et al. [83] | Interaction between sound and thermal influences on patient comfort in the hospitals of China’s northern heating region | 2019 | China | Applied Sciences (Switzerland) | 0 | Hospital |
| Angelova and Velichkova [84] | Thermophysiological Comfort of Surgeons and Patient in an Operating Room Based on PMV-PPD and PHS Indexes | 2020 | Bulgaria | Applied Sciences (Switzerland) | 0 | Hospital |
| Words | Occurrences | Words | Occurrences |
|---|---|---|---|
| thermal comfort | 37 | female | 15 |
| hospitals | 33 | male | 15 |
| human | 20 | ventilation | 14 |
| temperature | 19 | air quality | 13 |
| air conditioning | 17 |
| Journal | Articles |
|---|---|
| Building and Environment | 14 |
| Energy and Buildings | 8 |
| Applied Ergonomics | 2 |
| Applied Sciences | 2 |
| Indoor Air | 2 |
| Indoor and Built Environment | 2 |
| Journal of Hygiene | 2 |
| Main Aspect | Articles | Total | % |
|---|---|---|---|
| Health/Wellbeing | [14,15,16,17,18,19,20,21,26,27,35,36,39,40,43,44,45,46,47,48,49,50,51,54,56,57,58,59,61,62,64,65,66,67,68,69,70,71,73,74,75,76,78,79,80,81,83,84] | 48 | 81% |
| Productivity | [77] | 1 | 2% |
| Energy Saving | [38,41,42,52,53,55,60,63,72,82] | 10 | 17% |
| Study | PMV | Season or Period of Data Collection | Sample | |||
|---|---|---|---|---|---|---|
| Predicted Well | Overestimated | Underestimated | Not Suitable for Predict | |||
| [18] | x | November 2017 | 55 pregnant women | |||
| [45] | x | Winter and Spring | 933 respondents | |||
| [51] | x | Summer | 114 occupants | |||
| [21] | x | Winter and Spring | 99 patients | |||
| [56] | x | May and June (2011) | 110 questionnaires | |||
| [57] | x | May 2011 to February 2012 | 188 questionnaires | |||
| [59] | x | 31st March to 7th June 2011 | 55 staff members 35 patients | |||
| [64] | x | Not available | Not available | |||
| [17] | x | October and November, 2011 | 58 subjects interviewed | |||
| [69] | x | Summer | 37 respondents | |||
| [74] | x | July to November, 2015 and March to May 2016 | 451 patients, 331 visitors and 146 medical staff | |||
| [20] | x | Summer and winter | 509 participants | |||
| Reference | Group | Site | Main Findings | ||
|---|---|---|---|---|---|
| Staff | Patients | Visitor | |||
| Wyon, Lidwell and Williams [14] | Surgical Team | Operating rooms | Surgeons and anesthesiologists differ from other professionals in their thermal preferences; surgeons prefer a cooler environment, while anesthesiologists prefer a warmer environment. | ||
| Smith and Rae [15] | * | Wards | The temperature chosen by patients to achieve thermal comfort was 20.5 °C. | ||
| Wheldon and Hull [36] | * | Full-term babies and premature babies | Neonatal nursery | Temperature range of 27–30 °C for nurses and 33–34 °C for patients. | |
| Chen, Jiang and Moser [40] | Surgical Team | * | Operating rooms | In order to achieve thermal comfort, a high air ventilation rate is required. | |
| Berardi and Leoni [16] | * | * | * | Wards, operating rooms, offices, and laboratories | Fanger’s indices were not within the thermal comfort range in most rooms (PPD = 52% in winter and PPD = 62% in summer) |
| Cheong and Chong [27] | Office’s workers | Administration offices | The temperature of the dry air bulb recorded varied between 22.1 and 22.4 °C. This is slightly below the recommended range for acceptable indoor air quality of 22.5–25.5 °C from the local indoor air quality guideline; 49% of respondents complain of feeling cold. | ||
| Hashiguchi et al. [43] | Nurses and nursing assistants | * | Wards | The temperature was found to be between 20 and 23 °C, corresponding to previous studies carried out in Japan. | |
| Skoog, Frasson and Jagemar [44] | Nurses and nursing assistants | * | Wards | Mean Air Temperature in summer and winter were, respectively, 21.5 and 21.8 °C. | |
| Hwang et al. [45] | * | Wards | The neutral temperature observed for a TSV = 0, was 23.2 °C. The variation of the observed percentages of the dissatisfaction model, 20.7–25.4 and 21.8–26.2 °C for winter and summer, respectively, was wider than the predicted percentages of the dissatisfaction model, being 21.9–25.0 and 24.2–26.9 °C for winter and summer, respectively. | ||
| Mazzacane et al. [46] | Surgical Team | Operating rooms | Nurses claim to be comfortable 75% of the time, while assistants experience mild discomfort 90% of the time. | ||
| Khodakarami and Knight [47] | * | * | Patient rooms | Generally, thermal comfort conditions recorded during the measurement period were considered unacceptable. Only in 1% of the time were employees in thermal comfort. In patients, only in 35% of the time in comfort. | |
| Mui et al. [19] | * | Several Departments | The comfort temperature range is 25.4 ± 2.8 °C. | ||
| Ho, Rosario and Rahman [48] | Surgical Team | * | Operating rooms | The comfort temperature range is 22.2–23.6 °C. | |
| Lomas and Ji [49] | * | * | * | Wards | Natural ventilation provided an environment with only 15 hours above 28 °C and 21 h at night above 26 °C. |
| Masia et al. [50] | Surgical Team | * | Operating rooms | The results confirm the existence of a thermal difference between professionals and patients, the latter constantly subjected to cold thermal stress. | |
| Yau and Chew [51] | * | Several Departments | The comfortable temperature range that satisfied 90% of the occupants in the space was in the range of 25.3–28.2 °C. | ||
| Verheyen et al. [21] | * | Wards | No significant difference between the predicted mean vote (PMV), obtained from objective measurements, and the actual mean vote (AMV), obtained subjectively, for all different wards, except for neurology department. | ||
| Pourshaghaghy and Omidvari [54] | * | * | * | Wards and operating rooms | PPD in men is higher than one verified in women in both winter and summer seasons, although the PPD difference is less than 5%. |
| Azizpour et al. [56] | * | * | * | Facility Department | When analyzing the linear regression between TSV and PMV, neutrality was found around +0.75 instead of 0, as given in the Fanger model. The neutral temperature found was 26.8 °C, 1.8 °C higher than that calculated by the Fanger model (25 °C). |
| Azizpour et al. [57] | * | Lobby, office, praying room, kindergarten, and catering area | The new PMV limit corresponding to the neutrality range in this field study was −0.22 and +1.73 as opposed to −1 and +1 in the PMV model, and the operative temperature was 26.8 °C. | ||
| Azmoon et al. [58] | Nurses | Nursing workstation | The mean of the WBGT indicator, for all hospital workstations, was 20.67 °C (range 19.60–22.20 °C). | ||
| De Giuli et al. [59] | * | * | Wards | The maximum temperatures of the places where the patients were exceeded 29 °C, while the average values were around 26–27 °C. | |
| Van Gaever et al. [64] | Surgical Team | Operating rooms | PPD = 100% for anesthesiologists and PPD = 63% for nurses. | ||
| Yau and Chew [65] | * | Staff rooms, nurse counters, and the working space of the hospital personnel | Acceptable internal neutral temperatures are in the range of 23.3–26.5 ℃ | ||
| Del Ferraro et al. [17] | Doctors | * | Wards | The PMV best correlation with the AMV values among the male medical team under 65 years old. | |
| Rodrigues et al. [66] | Surgical Team | Operating rooms | The PMV index does not provide a correct and sufficient descriptive assessment of the thermal environment of the operating room. | ||
| Uścinowicz, Chludziʼnska and Bogdan [67] | Surgical Team | Operating rooms | Anesthesiologists wearing surgical clothing consider thermal comfort to be satisfactory in about 90% of operating rooms, while surgeon assistants and nurses 30% of ORs. Surgeons, as they have a higher metabolic rate, perceive thermal comfort in only 5% of ORs. | ||
| Carvalhais et al. [69] | * | Sterilization services (SS) | The results for PMV/PPD varied from 0.77/17.6% (morning) to 1.08/29.8% (afternoon) in SS1 and from 1/26.1% (morning) to 1.18/34.4% (afternoon) in SS2. | ||
| Jankowski and Mlstrokynarczyk [70] | Doctors | Operating rooms | The individual thermal sensations reported by the medical team pointed to the lack of thermal comfort. | ||
| Nematchoua et al. [71] | * | N/A | 90% of patients reported a comfortable temperature range of 24.5–26.2 °C. | ||
| Nematchoua, Ricciardi and Buratti [73] | * | N/A | 80% of patients reported a comfortable temperature range of 22.9–27.2 °C. | ||
| Pirsaheb, Sohrabi and Yarmohammadi [74] | * | Wards | The results show that the mean and the standard deviation of temperature was 29.9 ± 4.4 °C. Less than 50% of individuals felt discomfort in 87.1% of wards. | ||
| Sattayakorn, Ichinose and Sasaki [75] | * | * | * | Outpatient department | The acceptable temperature range for patients, visitors, and medical staff is 21.8–27.9, 22.0–27.1, and 24.1–25.6 °C, respectively. |
| Derks et al. [77] | Nurses | Wards | The mean thermal sensation vote (TSV) was 1.1, obtained with an air temperature of 23.3 °C. | ||
| Khalid et al. [78] | * | * | * | Wards | Ideal temperatures for patients, visitors, and nurses are, respectively, 25.7, 25.5, and 23.5 °C. |
| Loomans et al. [79] | Nurses | Wards | For temperature variations within ±2 °C, the thermal perception is minimally affected. | ||
| Tartarini, Cooper and Fleming [20] | * | * | * | All hospital | The estimated comfort range was between 19.1 and 26.2 °C. |
| Alfa and Öztürk [80] | * | Wards | A correlation of 0.357 between thermal comfort and perceived indoor environmental quality was found. | ||
| Fabbri, Gaspari and Vandi [18] | Pregnant women | Wards | The values reported were: TSV = 0.97, while PMV = −0.85. | ||
| Khalid et al. [26] | * | * | Patient rooms | Mean air temperature in patient rooms of 23.5 and 23.2 °C for patients and visitors, respectively. | |
| Wu et al. [83] | * | Wards | Research participants reported that the thermal sensation was “comfortable” (62.3%) and “very comfortable” (25%), indicating good thermal comfort conditions. | ||
| Angelova and Velichkova [84] | Surgeons | * | Operating rooms | The temperature of 28 °C can satisfy the thermal comfort of both the patient and the surgeon. | |
| Reference | Parameter | Main Findings |
|---|---|---|
| Chen, Jiang and Moser [40] | Particle concentration | Particle concentration between 2 and 2.55 m (particles/m3). Very small particle concentration in the operating room. |
| Berardi and Leoni [16] | Microbiological irborne contamination and CO2 concentration | Air microbial amount was higher in the wards and operating rooms than in the hospital offices. |
| Cheong and Chong [27] | Indoor air quality (IAQ) | CO2 = 450–700 ppm; CO = 0.05–0.7 ppm; Formaldehyde = 0.1–0.3 ppm. |
| Skoog, Frasson and Jagemar [44] | CO2 concentration Dust concentration | The maximum values measured during the winter were 576 ppm for CO2 concentration and 6.1 × 10−6 g/m3 for dust concentration. |
| Mui et al. [19] | Indoor environmental quality (IEQ) | CO2 concentration ranged from 970 ± 460 ppm, illumination levels ranged from 490 ± 460 lux and equivalent sound pressure levels ranged from 69 ± 8 dBA. |
| Ho, Rosario and Rahman [48] | Contaminant removal effectiveness (CRE) and the mean contaminant concentration | The parameters were used to evaluate the ventilation performance of the room through simulation. |
| Azmoon et al. [58] | Light intensity | The average light intensity for all hospital workstations was 296 lux. |
| De Giuli et al. [59] | Indoor environmental quality (IEQ) | Medium illuminance values have been established. Employees complained about lack of privacy, size of rooms, and acoustic discomfort. |
| Lawrence, Jayabal and Thirumal [76] | Indoor air quality (IAQ) | A patient room was studied. By monitoring the air quality system, it was demonstrated how different types of ventilations systems might benefit patients. |
| Alfa and Öztürk [80] | Indoor environmental quality (IEQ) | Maximum values for illumination, sound pressure level, and CO2 concentration are, respectively: 420 lux, 46.2 dBA, and 517 ppm. |
| Wu et al. [83] | Sound pressure level (LAeq) and acoustic satisfaction | The mean value of the equivalent continuous A-weighted sound pressure level in the wards was 59.2 dB, this being a satisfactory value. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pereira, P.F.d.C.; Broday, E.E.; Xavier, A.A.d.P. Thermal Comfort Applied in Hospital Environments: A Literature Review. Appl. Sci. 2020, 10, 7030. https://doi.org/10.3390/app10207030
Pereira PFdC, Broday EE, Xavier AAdP. Thermal Comfort Applied in Hospital Environments: A Literature Review. Applied Sciences. 2020; 10(20):7030. https://doi.org/10.3390/app10207030
Chicago/Turabian StylePereira, Pedro Filipe da Conceição, Evandro Eduardo Broday, and Antonio Augusto de Paula Xavier. 2020. "Thermal Comfort Applied in Hospital Environments: A Literature Review" Applied Sciences 10, no. 20: 7030. https://doi.org/10.3390/app10207030
APA StylePereira, P. F. d. C., Broday, E. E., & Xavier, A. A. d. P. (2020). Thermal Comfort Applied in Hospital Environments: A Literature Review. Applied Sciences, 10(20), 7030. https://doi.org/10.3390/app10207030