A Unified Framework for Automatic Detection of Wound Infection with Artificial Intelligence

 , ,
, ,
Abstract
1. Introduction
Objectives
2. Materials and Methods
2.1. Application for Collection of Wound Images
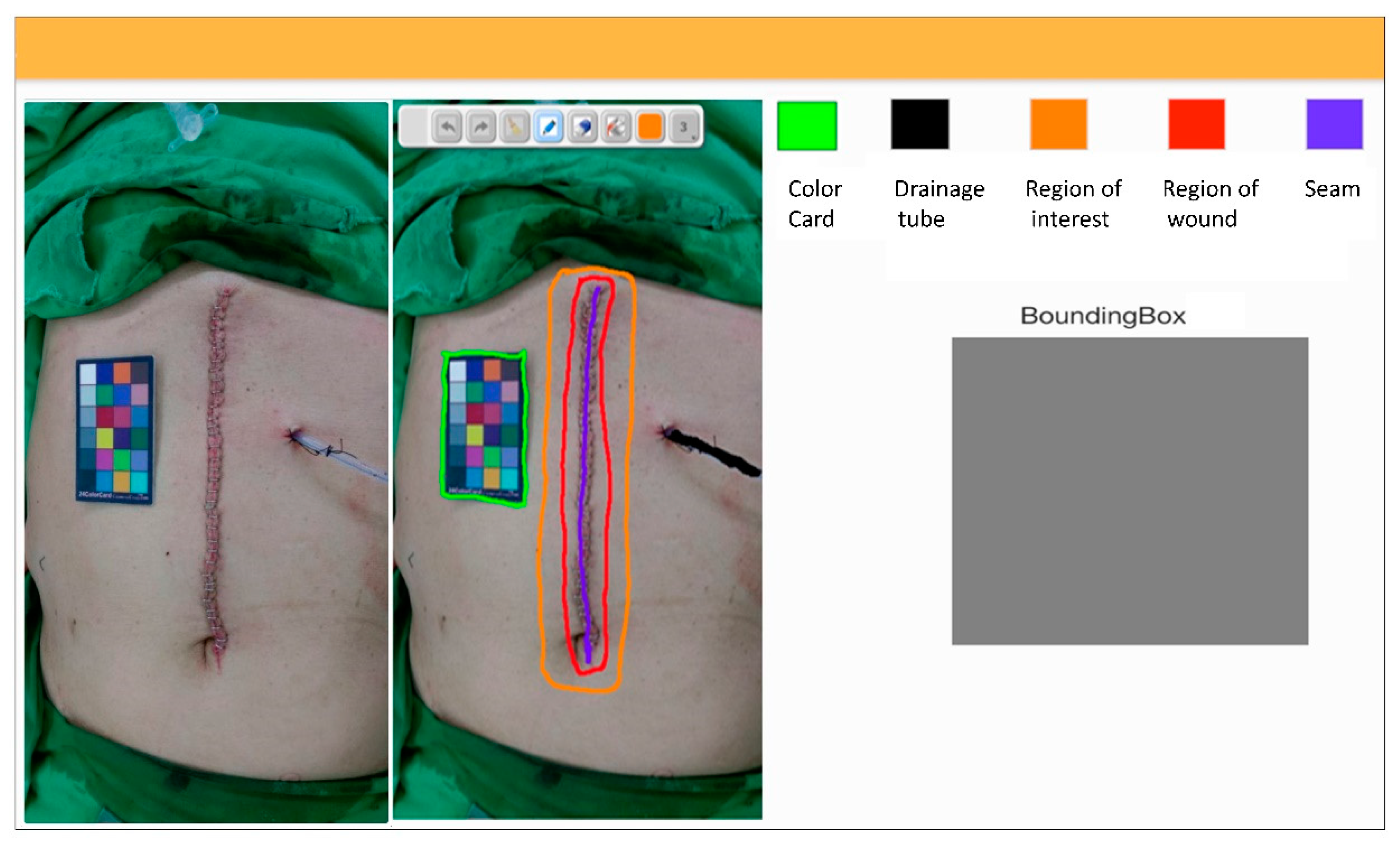
2.2. Interface of Wound Annotation
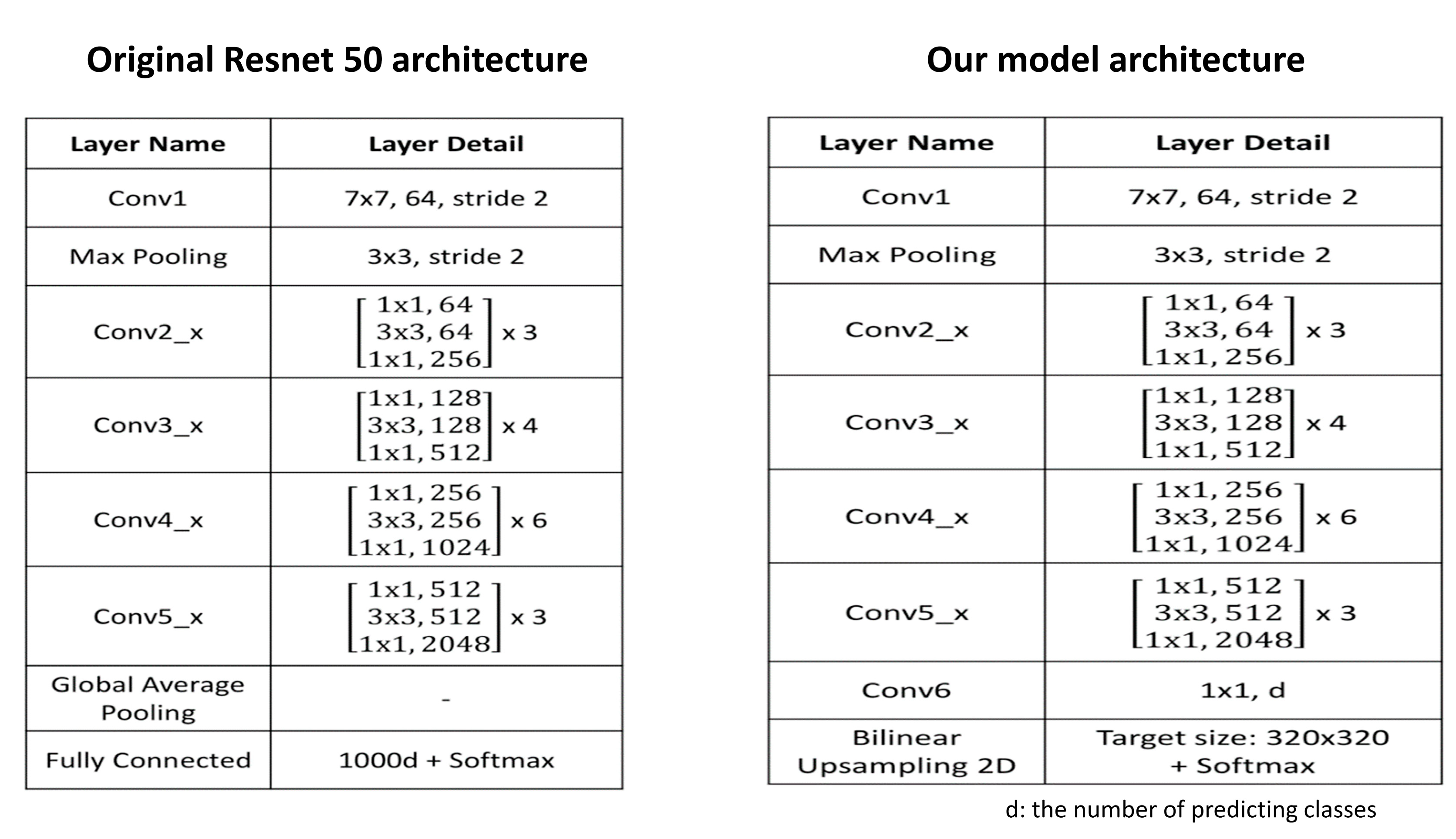
2.3. Model Development
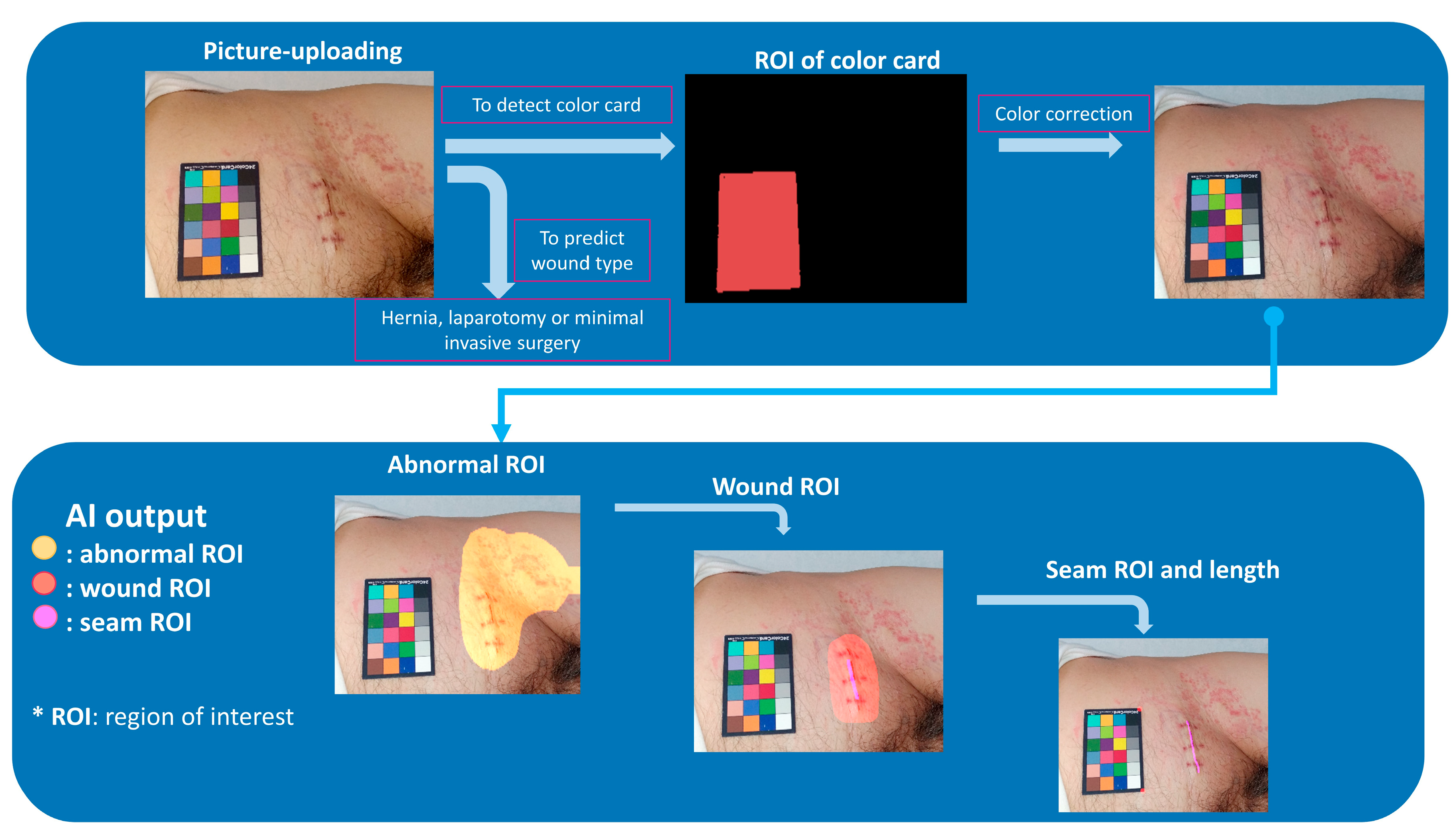
2.4. Detection of Color Card and ROI
2.5. Image Processing and Color Correction
2.6. Detection of Wound Infection
2.7. Experimental Setup
3. Results
3.1. Detection of Color Card and Wound ROI
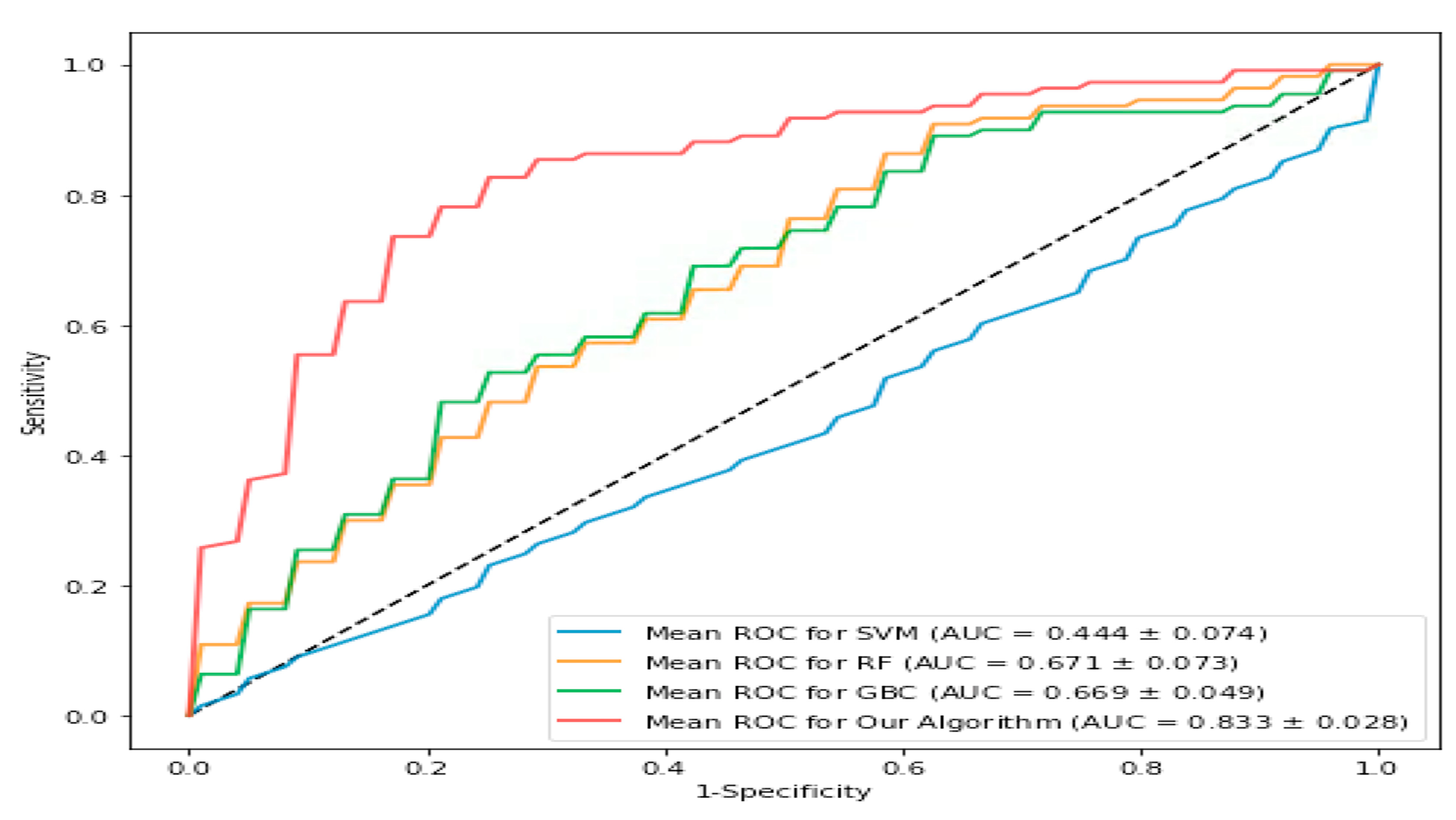
3.2. Detection of Wound Infection
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Lewis, S.S.; Moehring, R.W.; Chen, L.F.; Sexton, D.J.; Anderson, D.J. Assessing the relative burden of hospital-acquired infections in a network of community hospitals. Infect. Control. Hosp. Epidemiol. 2013, 34, 1229–1230. [Google Scholar] [CrossRef]
- Wiseman, J.T.; Guzman, A.M.; Fernandes-Taylor, S.; Engelbert, T.L.; Saunders, R.S.; Kent, K.C. General and vascular surgery readmissions: A systematic review. J. Am. Coll. Surg. 2014, 219, 552–569. [Google Scholar] [CrossRef] [PubMed]
- Young, P.Y.; Khadaroo, R.G. Surgical site infections. Surg. Clin. North Am. 2014, 94, 1245–1264. [Google Scholar] [CrossRef] [PubMed]
- Ljungqvist, O.; Scott, M.; Fearon, K.C. Enhanced Recovery After Surgery: A Review. JAMA Surg. 2017, 152, 292–298. [Google Scholar] [CrossRef] [PubMed]
- Gunter, R.L.; Fernandes-Taylor, S.; Rahman, S.; Awoyinka, L.; Bennett, K.M.; Weber, S.M.; Greenberg, C.C.; Kent, K.C. Feasibility of an Image-Based Mobile Health Protocol for Postoperative Wound Monitoring. J. Am. Coll. Surg. 2018, 226, 277–286. [Google Scholar] [CrossRef] [PubMed]
- Symer, M.M.; Abelson, J.S.; Milsom, J.; McClure, B.; Yeo, H.L. A Mobile Health Application to Track Patients After Gastrointestinal Surgery: Results from a Pilot Study. J. Gastrointest. Surg. 2017, 21, 1500–1505. [Google Scholar] [CrossRef]
- Fernandes-Taylor, S.; Gunter, R.L.; Bennett, K.M.; Awoyinka, L.; Rahman, S.; Greenberg, C.C.; Kent, K.C. Feasibility of Implementing a Patient-Centered Postoperative Wound Monitoring Program Using Smartphone Images: A Pilot Protocol. JMIR Res. Protoc. 2017, 6, e26. [Google Scholar] [CrossRef]
- Wu, J.M.; Ho, T.W.; Chang, Y.T.; Hsu, C.; Tsai, C.J.; Lai, F.; Lin, M.T. Wearable-Based Mobile Health App in Gastric Cancer Patients for Postoperative Physical Activity Monitoring: Focus Group Study. JMIR mHealth uHealth 2019, 7, e11989. [Google Scholar] [CrossRef]
- Wiseman, J.T.; Fernandes-Taylor, S.; Gunter, R.; Barnes, M.L.; Saunders, R.S.; Rathouz, P.J.; Yamanouchi, D.; Kent, K.C. Inter-rater agreement and checklist validation for postoperative wound assessment using smartphone images in vascular surgery. J. Vasc. Surg. Venous Lymphat. Disord. 2016, 4, 320–328. [Google Scholar] [CrossRef]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. arXiv 2015, arXiv:1512.03385. [Google Scholar]
- Everingham, M.; Van Gool, L.; Williams, C.K.I.; Winn, J.; Zisserman, A. The Pascal Visual Object Classes (VOC) Challenge. Intern. J. Comput. V. 2010, 88, 303–338. [Google Scholar] [CrossRef]
- Bay, H.; Tuyteelars, T.; Van Gool, L. SURF: Speeded Up Robust Features. In Proceedings of the 9th European Conference on Computer Vision, Graz, Austria, 7–13 May 2006; Leonardis, A., Bischof, H., Pinz, A., Eds.; Springer: Berlin/Heidelberg, Germany, 2006; Volume 3951. [Google Scholar]
- Lowe, D.G.; Muja, M. Fast Approximate Nearest Neighbors with Automatic Algorithm Configuration. In Proceedings of the Fourth International Conference on Computer Vision Theory and Applications, Lisbon, Portugal, 5–8 February 2009; pp. 331–340. [Google Scholar]
- Berger, R.L.; Hsu, J.C.; Hauck, W.W.; Anderson, S.; Meredith, M.P.; Heise, M.A.; Liu, J.-P.; Chow, S.-C.; Schuirmann, D.J.; Hwang, J.T.G.; et al. Bioequivalence trials, intersection-union tests and equivalence confidence: Comment. Stat. Sci. 1996, 11, 283–319. [Google Scholar] [CrossRef]
- Chollet, F. Xception: Deep learning with depthwise separable convolutions. arXiv 2016, arXiv:1610.02357v3. [Google Scholar]
- Chang, C.C.; Lin, C.J. Training nu-support vector classifiers: Theory and algorithms. Neural Comput. 2001, 13, 2119–2147. [Google Scholar] [CrossRef] [PubMed]
- Breiman, L. Random Forests. Mach. Learn. 2001, 45, 5–32. [Google Scholar] [CrossRef]
- Natekin, A.; Knoll, A. Gradient boosting machines, a tutorial. Front. Neurorobot. 2013, 7, 21. [Google Scholar] [CrossRef]
- Wang, C.; Yan, X.; Smith, M.; Kochhar, K.; Rubin, M.; Warren, S.M.; Wrobel, J.; Lee, H. A Unified Framework for Automatic Wound Segmentation and Analysis with Deep Convolutional Neural Networks. In Proceedings of the 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Milan, Italy, 25–29 August 2015; pp. 2415–2418. [Google Scholar] [CrossRef]
- Zhang, J.Q.; Curran, T.; McCallum, J.C.; Wang, L.; Wyers, M.C.; Hamdan, A.D.; Guzman, R.J.; Schermerhorn, M.L. Risk factors for readmission after lower extremity bypass in the American College of Surgeons National Surgery Quality Improvement Program. J. Vasc. Surg. 2014, 59, 1331–1339. [Google Scholar] [CrossRef]
- Fiordelli, M.; Diviani, N.; Schulz, P.J. Mapping mHealth research: A decade of evolution. J. Med. Internet Res. 2013, 15, e95. [Google Scholar] [CrossRef]
- Wayne, N.; Ritvo, P. Smartphone-Enabled Health Coach Intervention for People With Diabetes From a Modest Socioeconomic Strata Community: Single-Arm Longitudinal Feasibility Study. J. Med. Internet Res. 2014, 16, e149. [Google Scholar] [CrossRef]
- Kim, B.Y.; Lee, J. Smart Devices for Older Adults Managing Chronic Disease: A Scoping Review. JMIR Mhealth Uhealth 2017, 5, e69. [Google Scholar] [CrossRef]
- Gunter, R.L.; Chouinard, S.; Fernandes-Taylor, S.; Wiseman, J.T.; Clarkson, S.; Bennett, K.; Greenberg, C.C.; Kent, K.C. Current Use of Telemedicine for Post-Discharge Surgical Care: A Systematic Review. J. Am. Coll. Surg. 2016, 222, 915–927. [Google Scholar] [CrossRef] [PubMed]
- Kummerow Broman, K.; Gaskill, C.E.; Faqih, A.; Feng, M.; Phillips, S.E.; Lober, W.B.; Pierce, R.A.; Holzman, M.D.; Evans, H.L.; Poulose, B.K. Evaluation of Wound Photography for Remote Postoperative Assessment of Surgical Site Infections. JAMA Surg. 2018, 154, 117–124. [Google Scholar] [CrossRef] [PubMed]
- Gunter, R.; Fernandes-Taylor, S.; Mahnke, A.; Awoyinka, L.; Schroeder, C.; Wiseman, J.; Sullivan, S.; Bennett, K.; Greenberg, C.; Kent, K.C. Evaluating Patient Usability of an Image-Based Mobile Health Platform for Postoperative Wound Monitoring. JMIR mHealth uHealth 2016, 4, e113. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.M.; Yu, H.J.; Ho, T.W.; Su, X.Y.; Lin, M.T.; Lai, F. Tablet PC-enabled application intervention for patients with gastric cancer undergoing gastrectomy. Comput. Methods Progr. Biomed. 2015, 119, 101–109. [Google Scholar] [CrossRef] [PubMed]
- Luo, G.; Stone, B.L.; Johnson, M.D.; Tarczy-Hornoch, P.; Wilcox, A.B.; Mooney, S.D.; Sheng, X.; Haug, P.J.; Nkoy, F.L. Automating Construction of Machine Learning Models With Clinical Big Data: Proposal Rationale and Methods. JMIR Res. Protoc. 2017, 6, e175. [Google Scholar] [CrossRef]
- Philbrick, K.A.; Weston, A.D.; Akkus, Z.; Kline, T.L.; Korfiatis, P.; Sakinis, T.; Kostandy, P.; Boonrod, A.; Zeinoddini, A.; Takahashi, N.; et al. RIL-Contour: A Medical Imaging Dataset Annotation Tool for and with Deep Learning. J. Digit. Imaging 2019, 32, 571–581. [Google Scholar] [CrossRef]
- Trajman, A.; Luiz, R.R. McNemar χ2 test revisited: Comparing sensitivity and specificity of diagnostic examinations. Scand. J. Clin. Lab. Investig. 2008, 68, 77–80. [Google Scholar] [CrossRef]
- Wang, L.; Pedersen, P.C.; Strong, D.M.; Tulu, B.; Agu, E.; Ignotz, R. Smartphone-based wound assessment system for patients with diabetes. IEEE Trans. Biomed. Eng. 2015, 62, 477–488. [Google Scholar] [CrossRef]
- Wang, L.; Pedersen, P.C.; Agu, E.; Strong, D.M.; Tulu, B. Area Determination of Diabetic Foot Ulcer Images Using a Cascaded Two-Stage SVM-Based Classification. IEEE Trans. Biomed. Eng 2017, 64, 2098–2109. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Model | Accuracy | Recall | Precision | F1 Score | Specificity | False Positive | False Negative | AUC |
|---|---|---|---|---|---|---|---|---|
| Our model | 79.5% ± 4.2% | 77.1% ± 6.1% | 82.7% ± 7.8% | 79.4% ± 3.9% | 82.2% ± 3.5% | 17.8% ± 6.5% | 22.9% ± 6.0% | 83.3% ± 2.8% |
| Kernel support vector machines | 41.1% ± 2.1% | 40.8% ± 8.7% | 48.2% ± 3.3% | 38.3% ± 3.5% | 56.2% ± 2.6% | 43.8% ± 7.3% | 59.2% ± 8.8% | 44.4% ± 4.5% |
| Random forest | 58.6% ± 5.9% | 64.8% ± 12.4% | 44.5% ± 13.6% | 43.1% ± 11.4% | 19.2% ± 7.5% | 80.8% ± 2.5% | 35.2% ± 12.3% | 67.1% ± 7.3% |
| Gradient boosting classifier | 63.4% ± 4.2% | 65.2% ± 7.4% | 54.5% ± 6.4% | 58.7% ± 3.3% | 65.2% ± 5.3% | 34.8% ± 4.6% | 34.8% ± 7.4% | 66.9% ± 4.9% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, J.-M.; Tsai, C.-J.; Ho, T.-W.; Lai, F.; Tai, H.-C.; Lin, M.-T. A Unified Framework for Automatic Detection of Wound Infection with Artificial Intelligence. Appl. Sci. 2020, 10, 5353. https://doi.org/10.3390/app10155353
Wu J-M, Tsai C-J, Ho T-W, Lai F, Tai H-C, Lin M-T. A Unified Framework for Automatic Detection of Wound Infection with Artificial Intelligence. Applied Sciences. 2020; 10(15):5353. https://doi.org/10.3390/app10155353
Chicago/Turabian StyleWu, Jin-Ming, Chia-Jui Tsai, Te-Wei Ho, Feipei Lai, Hao-Chih Tai, and Ming-Tsan Lin. 2020. "A Unified Framework for Automatic Detection of Wound Infection with Artificial Intelligence" Applied Sciences 10, no. 15: 5353. https://doi.org/10.3390/app10155353
APA StyleWu, J.-M., Tsai, C.-J., Ho, T.-W., Lai, F., Tai, H.-C., & Lin, M.-T. (2020). A Unified Framework for Automatic Detection of Wound Infection with Artificial Intelligence. Applied Sciences, 10(15), 5353. https://doi.org/10.3390/app10155353