Familiarization and Reliability of the Isometric Knee Extension Test for Rapid Force Production Assessment

 ,
,  ,
, 
Abstract
Featured Application
Abstract
1. Introduction
2. Materials and Methods
2.1. Experimental Design
2.2. Participants
2.3. Rapid Isometric Contraction of the Knee Extensors
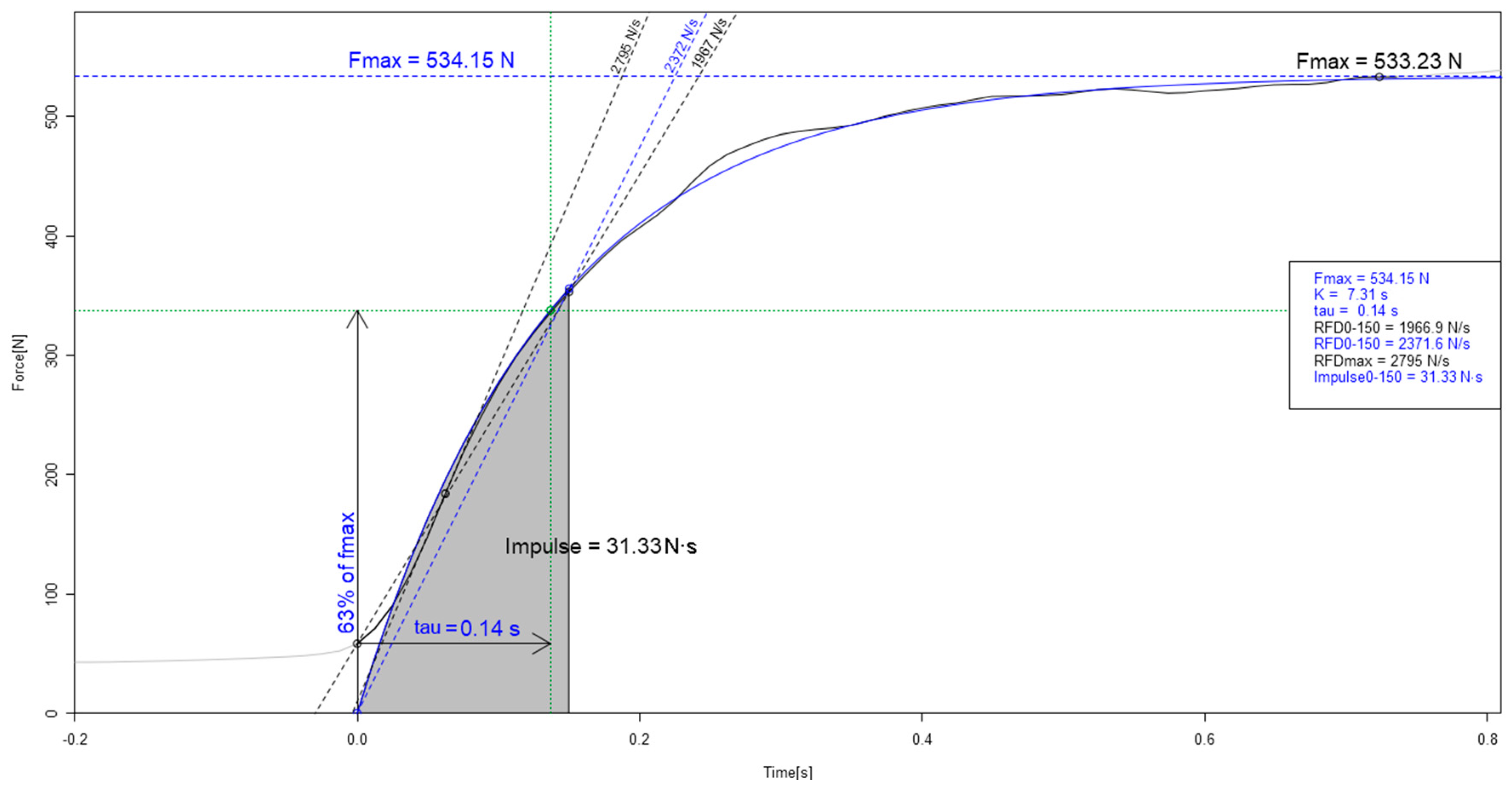
2.4. Force Variables
- Maximal voluntary contraction force (MVC): instantaneous maximal isometric muscle strength in Newtons (N).
- Rate of force development (RFD): the contractile RFD was obtained from the slope of the force-time curve (ΔForce/Δtime) expressed in N·s−1; thus, the instantaneous RFD peak (RFDmax) was the highest slope of the curve [17]. Average RFD was calculated for three overlapping periods in milliseconds to collect measures in three different phases of the contraction: 0–50 ms (RFD0–50), 0–150 ms (RFD0–150) and 0–250 ms (RFD0–250) [9,27].
- Impulse: the impulse was calculated through integration of force over time (i.e., cumulated area under the force-time curve) expressed in N·s [17]. Average impulse was calculated for the same three overlapping RFD periods in milliseconds (Impulse0–50, Impulse0–150 and Impulse0–250)
2.5. Statistical Analysis
3. Results
3.1. Intra-Session Reliability
3.2. Test-Retest Reliability
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- De Ruiter, C.J.; Van Leeuwen, D.; Heijblom, A.; Bobbert, M.F.; De Haan, A. Fast unilateral isometric knee extension torque development and bilateral jump height. Med. Sci. Sports Exerc. 2006, 38, 1843–1852. [Google Scholar] [CrossRef]
- Requena, B.; González-Badillo, J.J.; Saez De Villareal, E.S.; Ereline, J.; García, I.; Gapeyeva, H.; Pääsuke, M. Functional performance, maximal strength, and power characteristics in isometric and dynamic actions of lower extremities in soccer players. J. Strength Cond. Res. 2009, 23, 1391–1401. [Google Scholar] [CrossRef]
- Bojsen-Møller, J.; Magnusson, S.P.; Rasmussen, L.R.; Kjaer, M.; Aagaard, P. Muscle performance during maximal isometric and dynamic contractions is influenced by the stiffness of the tendinous structures. J. Appl. Physiol. 2005, 99, 986–994. [Google Scholar] [CrossRef]
- Maffiuletti, N.A.; Bizzini, M.; Widler, K.; Munzinger, U. Asymmetry in quadriceps rate of force development as a functional outcome measure in TKA. Clin. Orthop. Relat. Res. 2010, 468, 191–198. [Google Scholar] [CrossRef]
- Gapeyeva, H.; Buht, N.; Peterson, K.; Ereline, J.; Haviko, T.; Pääsuke, M. Quadriceps femoris muscle voluntary isometric force production and relaxation characteristics before and 6 months after unilateral total knee arthroplasty in women. Knee Surg. Sports Traumatol. Arthrosc. 2007, 15, 202–211. [Google Scholar] [CrossRef]
- Blazevich, A.J.; Wilson, C.J.; Alcaraz, P.E.; Rubio, J.A. Effects of Resistance Training Movement Pattern and Velocity on Isometric Muscular Rate of Force Development: A Systematic Review with Meta-analysis and Meta-regression. Sports Med. 2020, 50, 943–963. [Google Scholar] [CrossRef]
- Oranchuk, D.J.; Storey, A.G.; Nelson, A.R.; Cronin, J.B. Isometric training and long-term adaptations: Effects of muscle length, intensity, and intent: A systematic review. Scand. J. Med. Sci. Sports 2019, 29, 484–503. [Google Scholar] [CrossRef]
- Folland, J.P.; Buckthorpe, M.W.; Hannah, R. Human capacity for explosive force production: Neural and contractile determinants. Scand. J. Med. Sci. Sports 2014, 24, 894–906. [Google Scholar] [CrossRef]
- Maffiuletti, N.A.; Aagaard, P.; Blazevich, A.J.; Folland, J.; Tillin, N.; Duchateau, J. Rate of force development: Physiological and methodological considerations. Eur. J. Appl. Physiol. 2016, 116, 1091–1116. [Google Scholar] [CrossRef]
- Rodríguez-Rosell, D.; Pareja-Blanco, F.; Aagaard, P.; González-Badillo, J.J. Physiological and methodological aspects of rate of force development assessment in human skeletal muscle. Clin. Physiol. Funct. Imaging 2018, 38, 743–762. [Google Scholar] [CrossRef]
- McGuigan, M. Testing and Evaluation of Strength and Power; Routledge: Abingdon, UK, 2019; ISBN 0429647956. [Google Scholar]
- Dideriksen, J.L.; Del Vecchio, A.; Farina, D. Neural and muscular determinants of maximal rate of force development. J. Neurophysiol. 2020, 123, 149–157. [Google Scholar] [CrossRef]
- Andersen, L.L.; Aagaard, P. Influence of maximal muscle strength and intrinsic muscle contractile properties on contractile rate of force development. Eur. J. Appl. Physiol. 2006, 96, 46–52. [Google Scholar] [CrossRef]
- Toonstra, J.; Mattacola, C.G. Test-retest reliability and validity of isometric knee-flexion and -extension measurement using 3 methods of assessing muscle strength. J. Sport Rehabil. 2013, 22, 1–5. [Google Scholar] [CrossRef]
- Ruschel, C.; Haupenthal, A.; Jacomel, G.F.; de Fontana, H.B.; dos Santos, D.P.; Scoz, R.D.; Roesler, H. Validity and reliability of an instrumented leg-extension machine for measuring isometric muscle strength of the knee extensors. J. Sport Rehabil. 2015, 24, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Aagaard, P.; Simonsen, E.B.; Andersen, J.L.; Magnusson, P.; Dyhre-Poulsen, P. Increased rate of force development and neural drive of human skeletal muscle following resistance training. J. Appl. Physiol. 2002, 93, 1318–1326. [Google Scholar] [CrossRef] [PubMed]
- Aagaard, P.; Simonsen, E.B.; Andersen, J.L.; Magnusson, P.; Dyhre-Poulsen, P. Neural adaptation to resistance training: Changes in evoked V-wave and H-reflex responses. J. Appl. Physiol. 2002, 92, 2309–2318. [Google Scholar] [CrossRef] [PubMed]
- Dello Iacono, A.; Valentin, S.; Sanderson, M.; Halperin, I. The Isometric Horizontal Push Test: Test–Retest Reliability and Validation Study. Int. J. Sports Physiol. Perform. 2019, 15, 581–584. [Google Scholar] [CrossRef]
- Moir, G.L.; Getz, A.; Davis, S.E.; Marques, M.; Witmer, C.A. The Inter-Session Reliability of Isometric Force-Time Variables and the Effects of Filtering and Starting Force. J. Hum. Kinet. 2019, 66, 43–55. [Google Scholar] [CrossRef]
- Brady, C.J.; Harrison, A.J.; Flanagan, E.P.; Gregory Haff, G.; Comyns, T.M. A comparison of the isometric midthigh pull and isometric squat: Intraday reliability, usefulness, and the magnitude of difference between tests. Int. J. Sports Physiol. Perform. 2018, 13, 844–852. [Google Scholar] [CrossRef]
- Buckthorpe, M.W.; Hannah, R.; Pain, T.G.; Folland, J.P. Reliability of neuromuscular measurements during explosive isometric contractions, with special reference to electromyography normalization techniques. Muscle Nerve 2012, 46, 566–576. [Google Scholar] [CrossRef]
- Oranchuk, D.J.; Switaj, Z.J.; Zuleger, B.M. The Addition of a “Rapid Response” Neuromuscular Activation To a Standard Dynamic Warm-Up Improves Isometric Force and Rate of Force Development. J. Aust. Strength Cond. 2017, 25, 19–24. [Google Scholar]
- Buckthorpe, M.W.; Roi, G.S. The time has come to incorporate a greater focus on rate of force development training in the sports injury rehabilitation process. Muscles Ligaments Tendonsj. 2017, 7, 435. [Google Scholar] [CrossRef]
- Tillin, N.A.; Jimenez-Reyes, P.; Pain, M.T.G.; Folland, J.P. Neuromuscular performance of explosive power athletes versus untrained individuals. Med. Sci. Sports Exerc. 2010, 42, 781–790. [Google Scholar] [CrossRef] [PubMed]
- Stastny, P.; Tufano, J.; Kregl, J.; Petr, M.; Blazek, D.; Steffl, M.; Roczniok, R.; Fiala, M.; Golas, A.; Zmijewski, P. The Role of Visual Feedback on Power Output During Intermittent Wingate Testing in Ice Hockey Players. Sports 2018, 6, 32. [Google Scholar] [CrossRef] [PubMed]
- Duchateau, J.; Baudry, S. Maximal discharge rate of motor units determines the maximal rate of force development during ballistic contractions in human. Front. Hum. Neurosci. 2014, 8, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Dirnberger, J.; Wiesinger, H.P.; Wiemer, N.; Kösters, A.; Müller, E. Explosive strength of the knee extensors: The influence of criterion trial detection methodology on measurement reproducibility. J. Hum. Kinet. 2016, 50, 15–25. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of selecting and reporting intraclasscorrelation coefficients for reliability research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef]
- Atkinson, G.; Nevill, A. Statistical methods for assssing measurement Error (reliability) in variables relevant to sports medicine. Sports Med. 1998, 26, 217–238. [Google Scholar] [CrossRef]
- Bishop, C.; Turner, A.; Read, P. Effects of inter-limb asymmetries on physical and sports performance: A systematic review. J. Sports Sci. 2018, 36, 1135–1144. [Google Scholar] [CrossRef]
- Lakens, D. Calculating and reporting effect sizes to facilitate cumulative science: A practical primer for t-tests and ANOVAs. Front. Psychol. 2013, 4, 863. [Google Scholar] [CrossRef]
- Kiff, A.B. Effect of Focus of Attention on Rate of Torque Development in the Knee Extensors; Oregon State University: Corvallis, OR, USA, 2017. [Google Scholar]



{kind=link}
{kind=link}
| Raw Data | Dominant Leg | Non-Dominant Leg | Diff% | ||||||
|---|---|---|---|---|---|---|---|---|---|
| M (SD) | CV | SEM | ICC | M (SD) | CV | SEM | ICC | ||
| MVC (N) | |||||||||
| Session 1 | 649 (115) | 9.1% | 59.9 | 0.887 | 598 (91) | 5.8% | 34.0 | 0.869 | −8.9% |
| Session 2 | 676 (117) | 5.0% | 33.9 | 0.966 | 618 (102) | 4.4% | 26.9 | 0.975 | −8.3% |
| Impulse0–50 (N·s) | |||||||||
| Session 1 | 7.1 (3.7) | 37.8% | 2.6 | 0.788 | 6.2 (3.3) | 29.3% | 1.8 | 0.896 | −10.2% |
| Session 2 | 7.6 (3.1) | 30.3% | 2.2 | 0.798 | 7.3 (3.3) | 21.5% | 1.6 | 0.815 | −2.4% |
| Impulse0–150 (N·s) | |||||||||
| Session 1 | 48.6 (15.1) | 16.0% | 7.8 | 0.910 | 42.9 (14.0) | 11.9% | 5.1 | 0.956 | −13.1% |
| Session 2 | 49.5 (14.0) | 10.7% | 5.3 | 0.954 | 45.8 (13.5) | 16.6% | 7.6 | 0.909 | −8.0% |
| Impulse0–250 (N·s) | |||||||||
| Session 1 | 102.8 (26.2) | 11.7% | 12.0 | 0.928 | 93.4 (24.8) | 8.2% | 7.7 | 0.969 | −10.0% |
| Session 2 | 105.1 (25.1) | 6.7% | 7.0 | 0.976 | 96.6 (24.1) | 12.7% | 12.2 | 0.926 | −8.8% |
| RFD0–50 (N·s−1) | |||||||||
| Session 1 | 4446 (2275) | 34.8% | 1548 | 0.802 | 3959 (2209) | 26.9% | 1064 | 0.914 | −12.4% |
| Session 2 | 4667 (1951) | 21.8% | 1016 | 0.901 | 4256 (1989) | 32.1% | 1367 | 0.816 | −9.7% |
| RFD0–150 (N·s−1) | |||||||||
| Session 1 | 3074 (695) | 8.3% | 254 | 0.956 | 2771 (706) | 13.3% | 369 | 0.934 | −10.9% |
| Session 2 | 3087 (760) | 8.0% | 247 | 0.966 | 2881 (677) | 9.3% | 268 | 0.959 | −7.2% |
| RFD0–250 (N·s−1) | |||||||||
| Session 1 | 2122 (426) | 7.0% | 148 | 0.959 | 1954 (430) | 9.6% | 189 | 0.950 | −8.6% |
| Session 2 | 2211 (491) | 7.7% | 170 | 0.958 | 2010 (393) | 6.0% | 122 | 0.968 | −10.0% |
| RFDmax (N·s−1) | |||||||||
| Session 1 | 6988 (2278) | 16.2% | 1135 | 0.912 | 6118 (1933) | 21.3% | 1302 | 0.944 | −14.2% |
| Session 2 | 7098 (2346) | 12.7% | 899 | 0.952 | 6800 (1858) | 24.4% | 1660 | 0.874 | −4.4% |
| Fitted Data | Dominant Leg | Non-Dominant Leg | %Diff | ||||||
|---|---|---|---|---|---|---|---|---|---|
| M (SD) | CV | SEM | ICC | M (SD) | CV | SEM | ICC | ||
| MVC (N) | |||||||||
| Session 1 | 628 (111) | 5.9% | 37.7 | 0.887 | 568 (93) | 6.2% | 35.2 | 0.869 | −10.5% |
| Session 2 | 646 (117) | 5.6% | 35.9 | 0.969 | 597 (96) | 4.7% | 27.9 | 0.975 | −8.2% |
| Impulse0–50 (N·s) | |||||||||
| Session 1 | 7.6 (2.9) | 22.6% | 1.7 | 0.788 | 7.3 (2.6) | 25.8% | 1.9 | 0.815 | −15.9% |
| Session 2 | 7.7 (2.8) | 15.8% | 1.2 | 0.798 | 6.5 (2.6) | 15.1% | 1.0 | 0.896 | −5.3% |
| Impulse0–150 (N·s) | |||||||||
| Session 1 | 48.4 (14.6) | 15.7% | 7.6 | 0.910 | 43.1 (13.5) | 10.6% | 4.6 | 0.956 | −12.3% |
| Session 2 | 49.3 (13.8) | 9.8% | 4.8 | 0.954 | 46.1 (12.7) | 15.0% | 6.9 | 0.909 | −6.8% |
| Impulse0–250 (N·s) | |||||||||
| Session 1 | 102.8 (26.4) | 11.7% | 12.1 | 0.928 | 96.4 (23.8) | 12.6% | 12.1 | 0.926 | −8.8% |
| Session 2 | 104.9 (25.3) | 7.1% | 7.4 | 0.976 | 93.3 (25.0) | 8.4% | 7.8 | 0.969 | −10.2% |
| RFD0–50 (N·s−1) | |||||||||
| Session 1 | 5465 (2000) | 21.2% | 1161 | 0.802 | 4801 (1756) | 13.6% | 651 | 0.914 | −13.8% |
| Session 2 | 5589 (1840) | 13.6% | 761 | 0.901 | 5308 (1637) | 18.7% | 991 | 0.816 | −5.3% |
| RFD0–150 (N·s−1) | |||||||||
| Session 1 | 3315 (850) | 12.2% | 406 | 0.956 | 3119 (766) | 11.5% | 358.2 | 0.934 | −6.3% |
| Session 2 | 3411 (808) | 6.8% | 232 | 0.966 | 3042 (790) | 8.1% | 244.9 | 0.959 | −12.1% |
| RFD0–250 (N·s−1) | |||||||||
| Session 1 | 2318 (463) | 8.1% | 188 | 0.959 | 2120 (457) | 8.5% | 181 | 0.950 | −9.3% |
| Session 2 | 2365 (484) | 5.3% | 126 | 0.958 | 2142 (448) | 5.9% | 126 | 0.968 | −10.4% |
| RFDmax (N·s−1) | |||||||||
| Session 1 | 7561 (3447) | 28.8% | 2179 | 0.912 | 6363 (2892) | 18.9% | 1202 | 0.874 | −21.3% |
| Session 2 | 7721 (3340) | 21.3% | 1644 | 0.952 | 7459 (2763) | 24.9% | 1856 | 0.944 | −1.4% |
| Test-Retest | Dominant Leg | Non-Dominant Leg | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CV | SEM | ICC | %Diff | p | ES | CV | SEM | ICC | %Diff | p | ES | |
| Raw | ||||||||||||
| MVC (N) | 5.7% | 38.0 | 0.948 | +2.5% | 0.290 | 0.14 | 5.4% | 33.4 | 0.939 | +2.7% | 0.248 | 0.17 |
| Impulse0–50 (N·s) | 19.7% | 1.8 | 0.801 | +1.1% | 0.882 | 0.03 | 24.1% | 1.9 | 0.713 | −19.6% | 0.075 | 0.50 |
| Impulse0–150 (N·s) | 10.0% | 5.4 | 0.908 | −0.6% | 0.891 | 0.02 | 11.4% | 5.6 | 0.955 | −6.5% | 0.154 | 0.26 |
| Impulse0–250 (N·s) | 9.2% | 10.2 | 0.904 | <0.1% | 0.994 | 0.01 | 7.4% | 7.5 | 0.929 | −3.5% | 0.265 | 0.17 |
| RFD0–50 (N·s−1) | 15.6% | 868 | 0.848 | −1.1% | 0.870 | 0.04 | 23.7% | 1184 | 0.742 | −7.6% | 0.497 | 0.19 |
| RFD0–150 (N·s−1) | 8.7% | 283 | 0.914 | −0.1% | 0.980 | 0.01 | 10.4% | 313 | 0.840 | +2.9% | 0.530 | 0.14 |
| RFD0–250 (N·s−1) | 7.3% | 165 | 0.938 | +5.0% | 0.081 | 0.24 | 5.7% | 120 | 0.952 | −0.1% | 0.982 | 0.01 |
| RFDmax (N·s−1) | 17.2% | 1349 | 0.799 | −0.8% | 0.918 | 0.03 | 22.0% | 1658 | 0.212 | +14.5% | 0.095 | 0.67 |
| Fitted | ||||||||||||
| MVC (N) | 6.1% | 40.0 | 0.938 | +2.4% | 0.306 | 0.13 | 5.0% | 30.2 | 0.947 | +2.5% | 0.261 | 0.15 |
| Impulse0–50 (N·s) | 13.3% | 1.2 | 0.901 | −0.5% | 0.932 | 0.02 | 17.1% | 1.4 | 0.810 | −16.4% | 0.030 | 0.49 |
| Impulse0–150 (N·s) | 10.5% | 5.6 | 0.900 | −0.4% | 0.937 | 0.01 | 10.8% | 5.3 | 0.879 | −7.0% | 0.146 | 0.28 |
| Impulse0–250 (N·s) | 9.1% | 10.1 | 0.904 | +0.3% | 0.942 | 0.01 | 7.5% | 7.7 | 0.925 | −3.5% | 0.311 | 0.16 |
| RFD0–50 (N·s−1) | 12.4% | 778 | 0.898 | −0.6% | 0.906 | 0.02 | 14.8% | 841 | 0.823 | −10.5% | 0.115 | 0.38 |
| RFD0–150 (N·s−1) | 8.9% | 318 | 0.907 | +0.4% | 0.923 | 0.02 | 6.5% | 218 | 0.940 | −2.6% | 0.411 | 0.21 |
| RFD0–250 (N·s−1) | 7.1% | 173 | 0.930 | +0.3% | 0.925 | 0.01 | 4.6% | 102 | 0.967 | −0.1% | 0.958 | 0.01 |
| RFDmax (N·s−1) | 16.9% | 1548 | 0.891 | −0.2% | 0.975 | 0.01 | 22.9% | 1864 | 0.717 | −17.3% | 0.106 | 0.45 |
| Isometric Knee Extension Force | Reliability | Preferable Signal | Influence of Familiarization | Inter-Limb Asymmetry |
|---|---|---|---|---|
| MVC(N) | High | Raw/Fitted | Low | Low |
| RFD0–250(N·s−1) | High | Fitted | Low | low |
| Impulse0–250(N·s) | High | Raw/Fitted | Low | Moderate |
| RFD0–150(N·s−1) | Moderate | Raw/Fitted | High | Moderate |
| Impulse0–150(N·s) | Moderate | Fitted | High | High |
| RFD0–50(N·s−1) | Moderate | Fitted | Very high | High |
| Impulse0–50(N·s) | Low | Fitted | Very high | Very high |
| RFDmax(N·s−1) | Low | Raw | Very high | Very high |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Courel-Ibáñez, J.; Hernández-Belmonte, A.; Cava-Martínez, A.; Pallarés, J.G. Familiarization and Reliability of the Isometric Knee Extension Test for Rapid Force Production Assessment. Appl. Sci. 2020, 10, 4499. https://doi.org/10.3390/app10134499
Courel-Ibáñez J, Hernández-Belmonte A, Cava-Martínez A, Pallarés JG. Familiarization and Reliability of the Isometric Knee Extension Test for Rapid Force Production Assessment. Applied Sciences. 2020; 10(13):4499. https://doi.org/10.3390/app10134499
Chicago/Turabian StyleCourel-Ibáñez, Javier, Alejandro Hernández-Belmonte, Alejandro Cava-Martínez, and Jesús G. Pallarés. 2020. "Familiarization and Reliability of the Isometric Knee Extension Test for Rapid Force Production Assessment" Applied Sciences 10, no. 13: 4499. https://doi.org/10.3390/app10134499
APA StyleCourel-Ibáñez, J., Hernández-Belmonte, A., Cava-Martínez, A., & Pallarés, J. G. (2020). Familiarization and Reliability of the Isometric Knee Extension Test for Rapid Force Production Assessment. Applied Sciences, 10(13), 4499. https://doi.org/10.3390/app10134499