Biological Effect of Single or Combined Pharmacological Therapy Using Alendronate and Simvastatin on Implant Osseointegration: An In Vivo Study in Healthy and Osteoporotic Rat Models


 ,
,  , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Preparation of Mini-implants
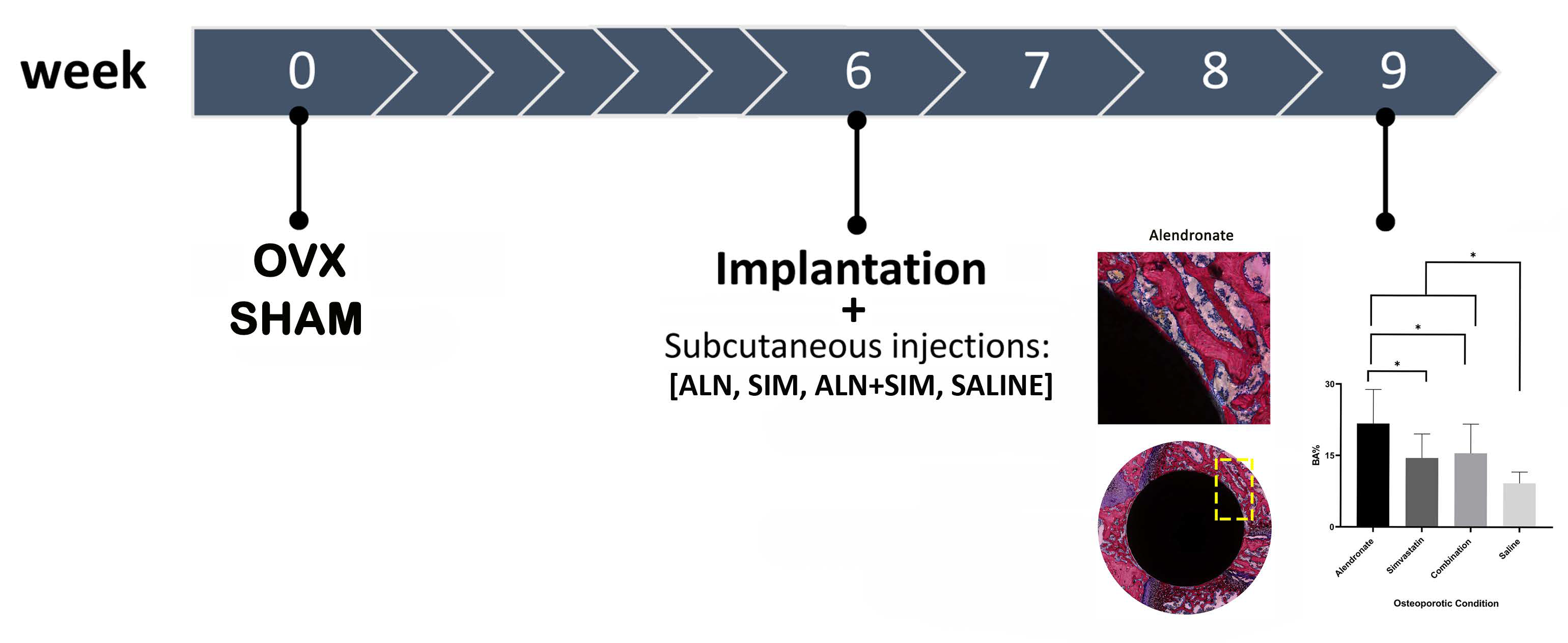
2.2. Animal Model
2.3. Implantation Procedures
2.4. Administration of Anti-Osteoporotic Drugs
- Alendronate treatment (ALN; Fosamax® 70 mg, Merck Sharp & Dohme Ltd, Hoddesdon, UK) was used for 20 animals (10 OVX, 10 SHAM).
- Simvastatin treatment (SIM; Zocor®, Merck Sharp & Dohme B.V, Haarlem, The Netherlands) was used for 20 animals (10 OVX, 10 SHAM).
- Combined treatment (ALN+SIM) was used for 20 animals (10 OVX, 10 SHAM).
- Saline administration (10 mL) was used for 20 animals (10 OVX, 10 SHAM) as non-treated controls.
2.5. Sample Retrieval, Preparation, and Analyses
2.6. Mechanical Push-out Testing
2.7. Histological Preparation and Evaluation
2.8. Statistical Analysis
3. Results
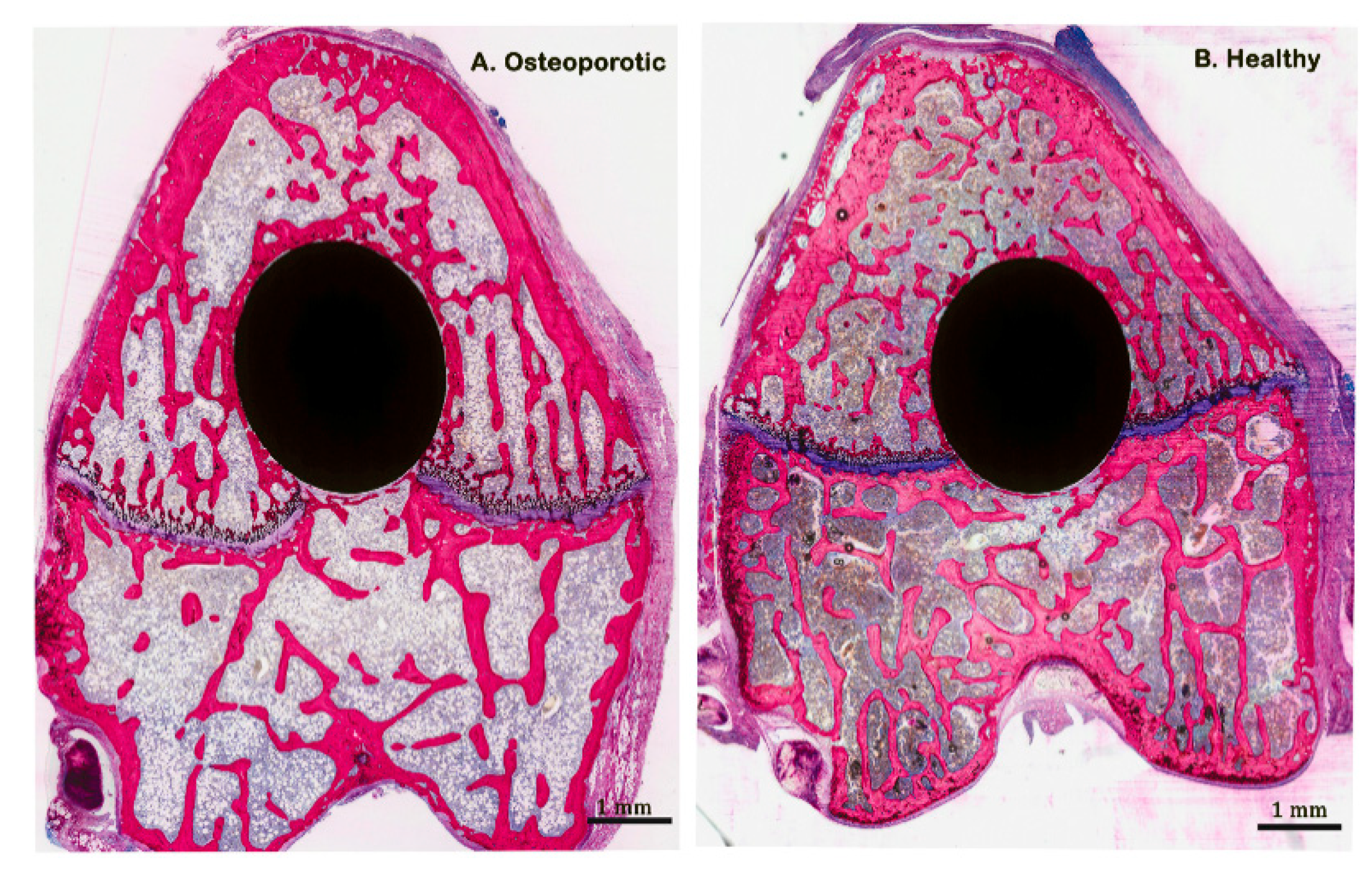
3.1. Animal Model
3.2. Biomechanical Push-Out Test
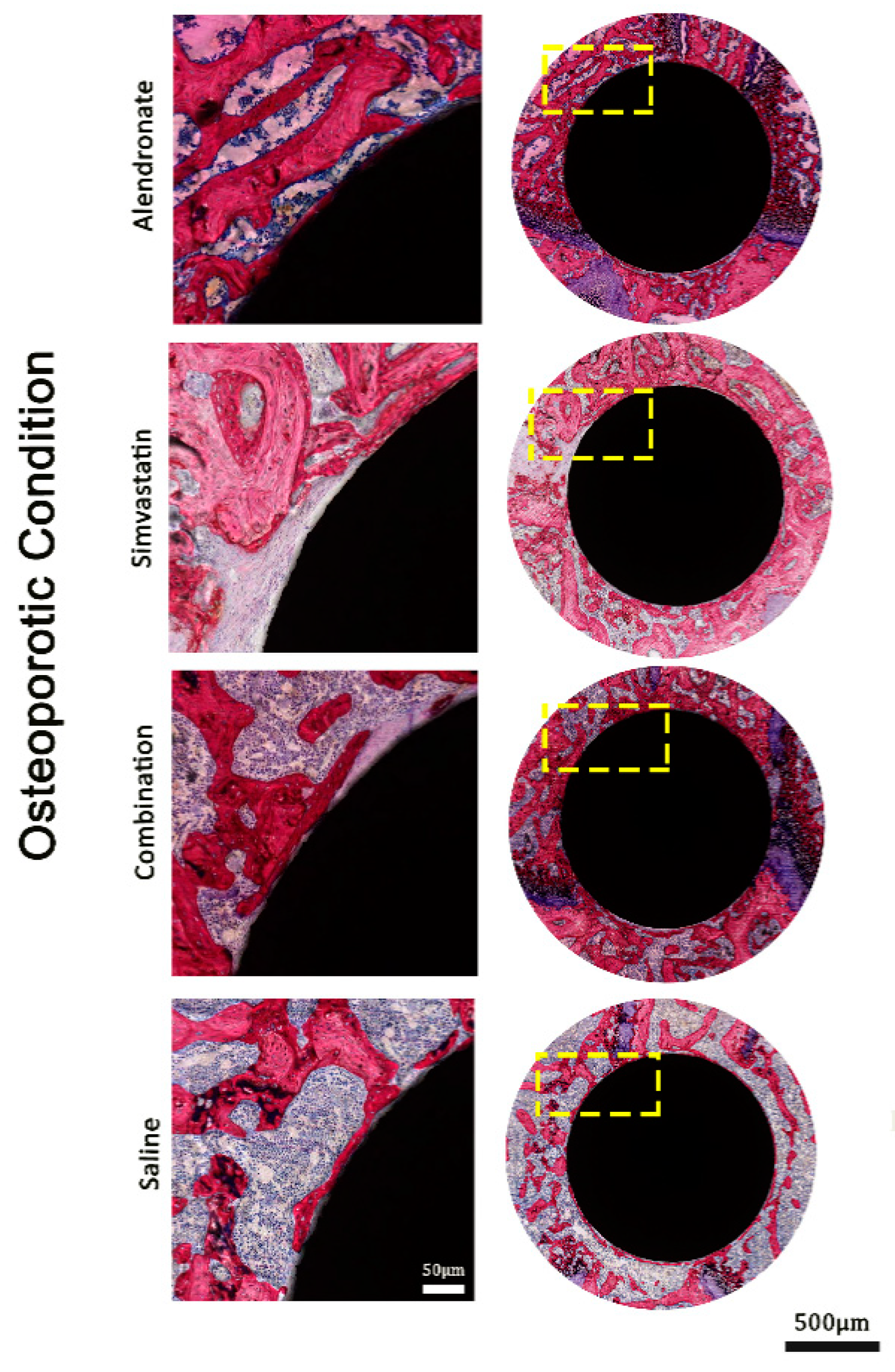
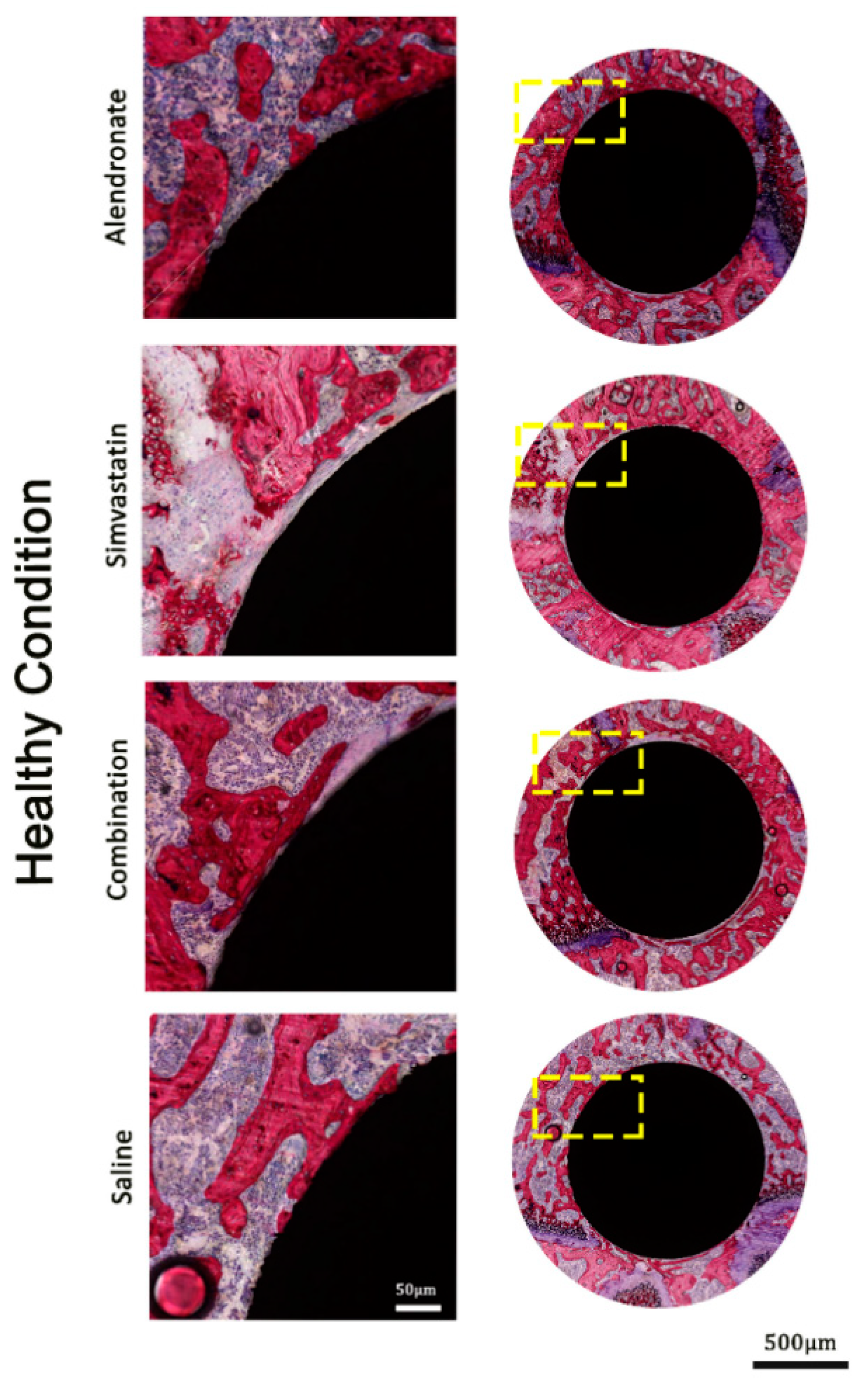
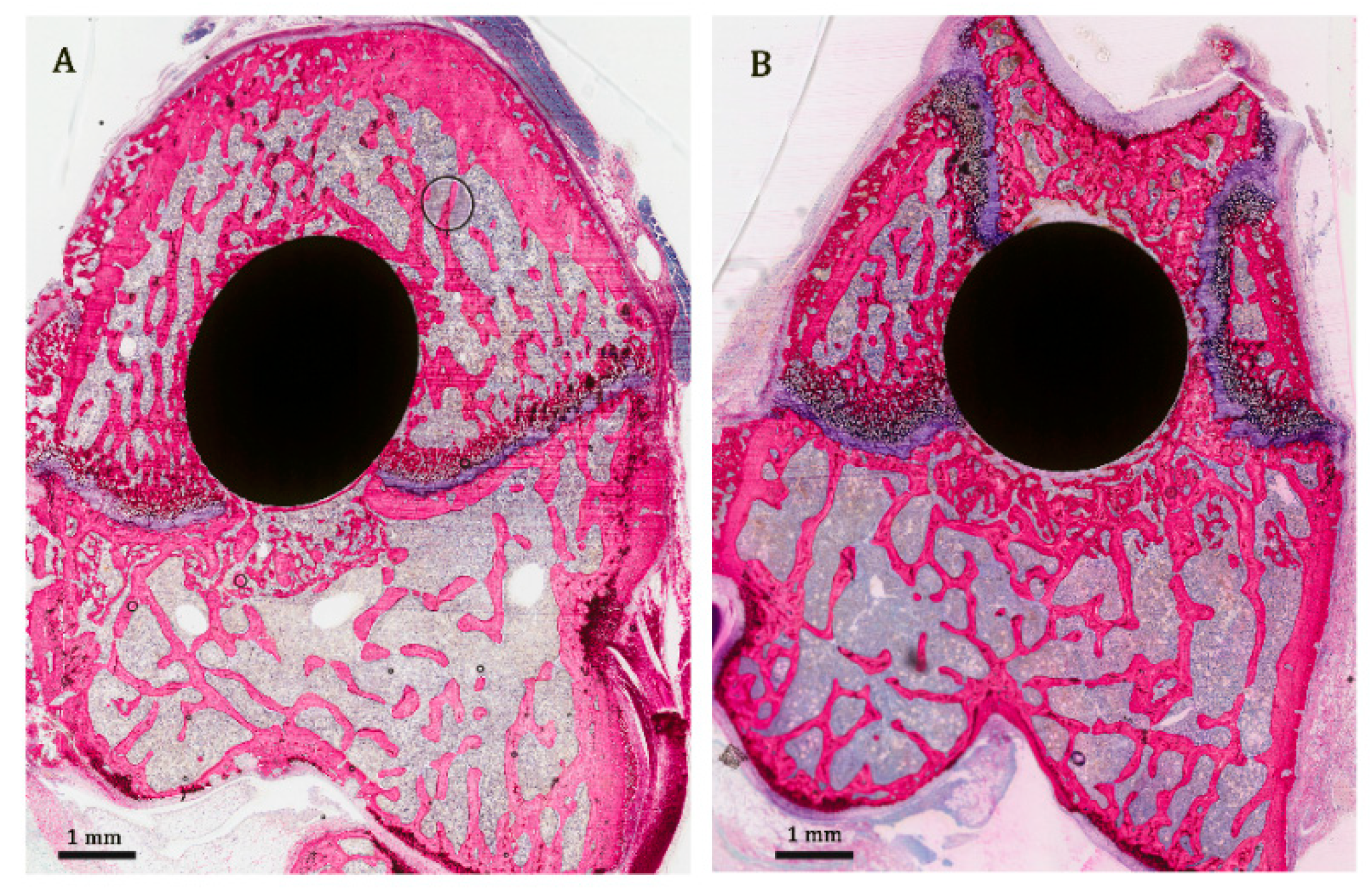
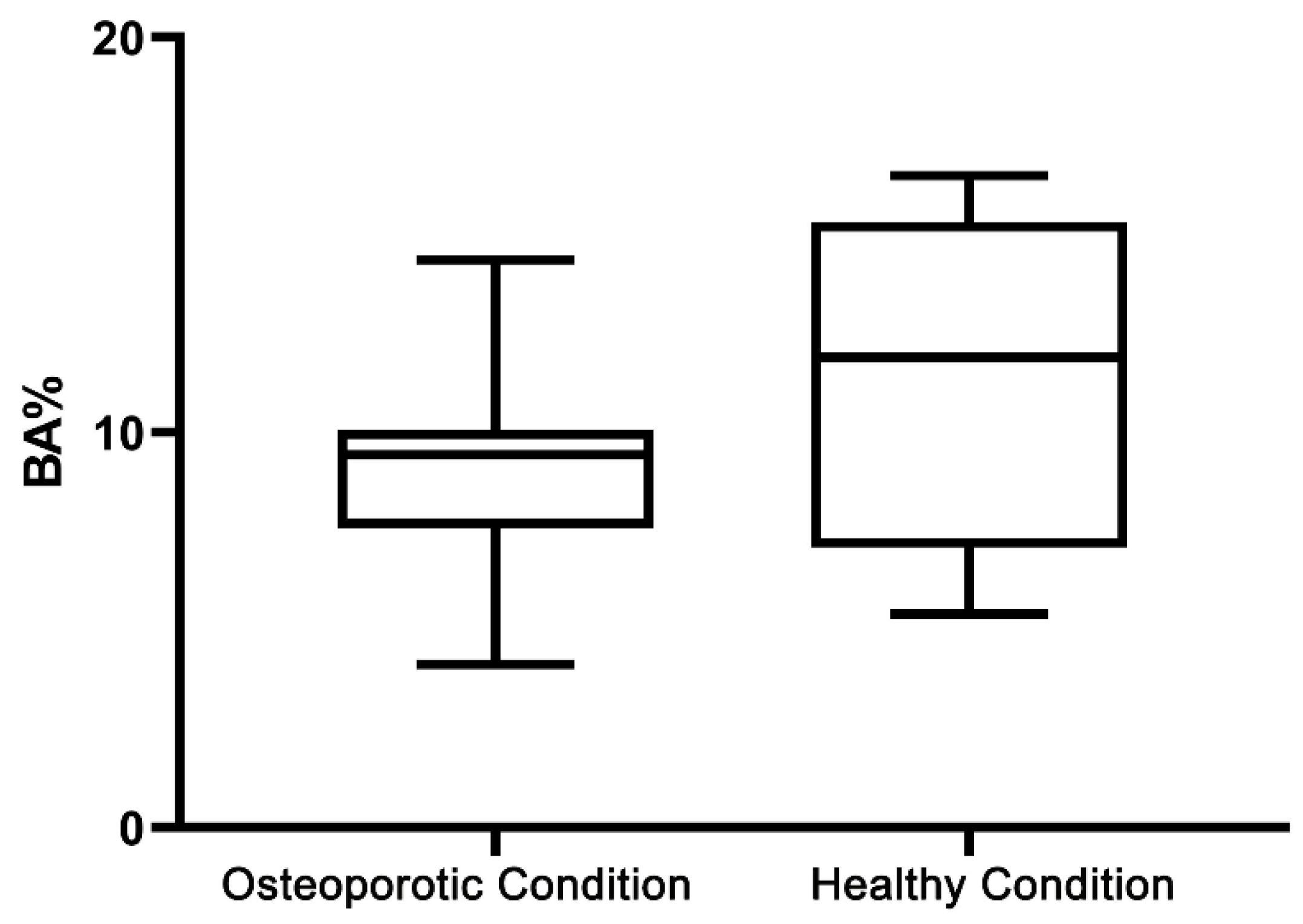
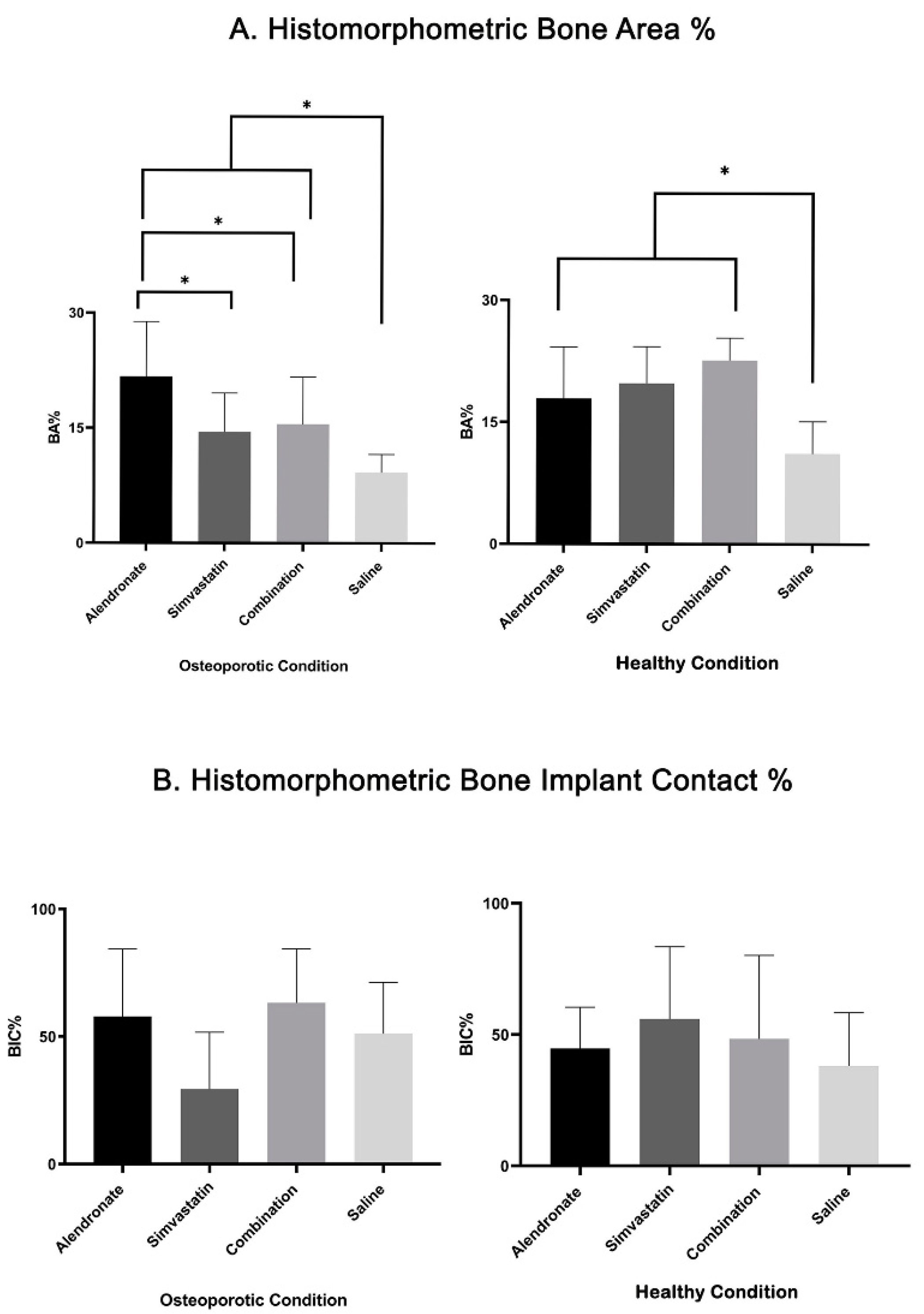
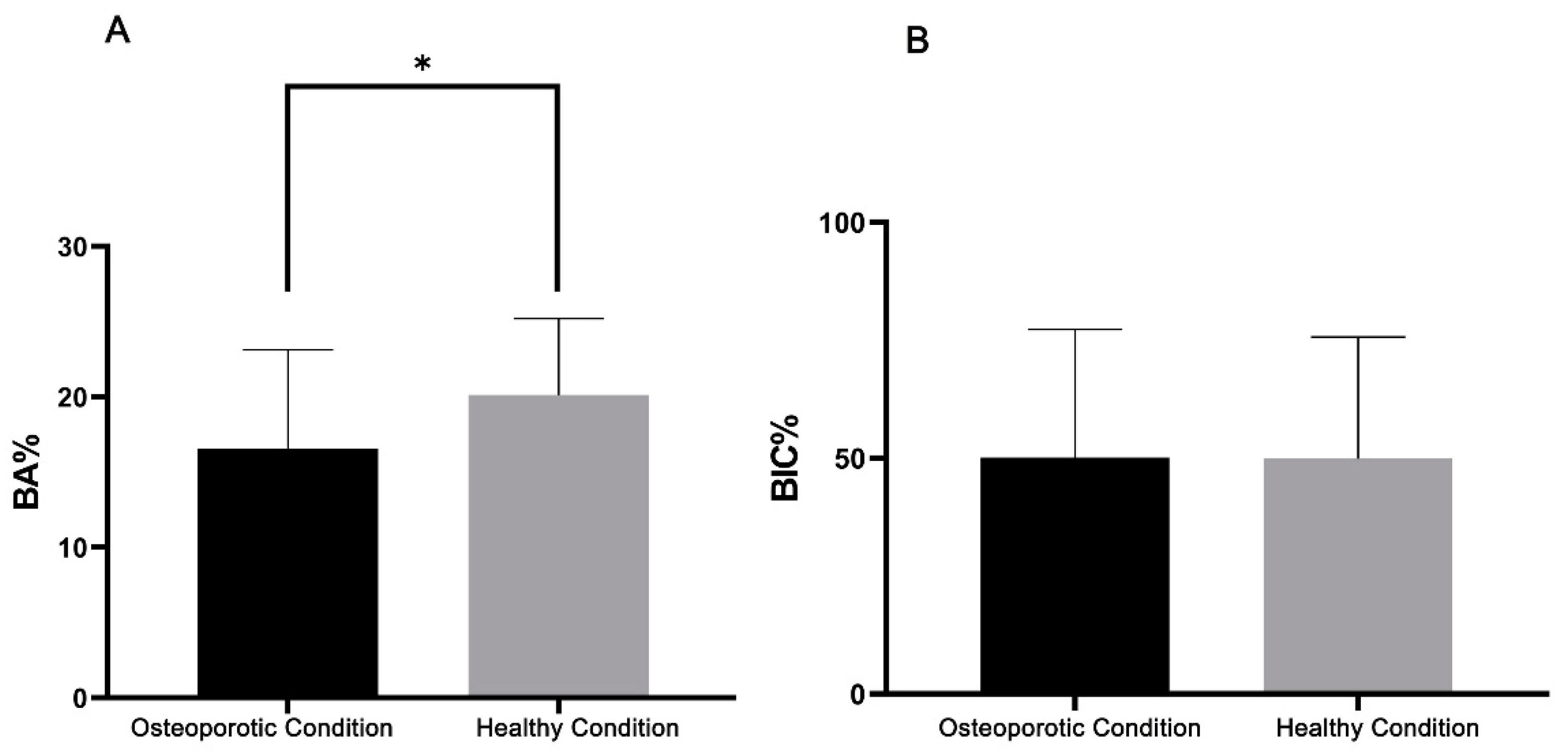
3.3. Histological and Histomorphometric Evaluation
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Heydecke, G.; Locker, D.; Awad, M.A.; Lund, J.P.; Feine, J. Oral and general health-related quality of life with conventional and implant dentures. Community Dent. Oral Epidemiol. 2003, 31, 161–168. [Google Scholar] [CrossRef]
- Petersen, P.E. The World Oral Health Report 2003: Continuous improvement of oral health in the 21st century--the approach of the WHO Global Oral Health Programme. Community Dent. Oral Epidemiol. 2003, 31 (Suppl. 1), 3–23. [Google Scholar] [CrossRef]
- Henry, P.J. Tooth loss and implant replacement. Aust. Dent. J. 2000, 45, 150–172. [Google Scholar] [CrossRef]
- Abtahi, J.; Tengvall, P.; Aspenberg, P. Bisphosphonate coating might improve fixation of dental implants in the maxilla: A pilot study. Int. J. Oral Maxillofac. Surg. 2010, 39, 673–677. [Google Scholar] [CrossRef]
- Von Wowern, N. General and oral aspects of osteoporosis: A review. Clin. Oral Investig. 2001, 5, 71–82. [Google Scholar] [CrossRef]
- Dennison, E.M.; Cole, Z.; Cooper, C. Diagnosis and epidemiology of osteoporosis. Curr. Opin. Rheumatol. 2005, 17, 456–461. [Google Scholar] [CrossRef]
- Garg, A.K.; Winkler, S.; Bakaeen, L.G.; Mekayarajjananonth, T. Dental implants and the geriatric patient. Implant. Dent. 1997, 6, 168–173. [Google Scholar] [CrossRef]
- Gaetti-Jardim, E.C.; Junior, J.S.; Goiato, M.C.; Pellizer, E.P.; Magro-Filho, O.; Gaetti-Jardim, E.C. Dental Implants in Patients With Osteoporosis. J. Craniofacial Surg. 2011, 22, 1111–1113. [Google Scholar] [CrossRef]
- Dundar, S.; Yaman, F.; Gecor, O.; Cakmak, O.; Kirtay, M.; Yildirim, T.T.; Karaman, T.; Benlidayi, M.E. Effects of Local and Systemic Zoledronic Acid Application on Titanium Implant Osseointegration. J. Craniofac. Surg. 2017, 28, 935–938. [Google Scholar] [CrossRef]
- Alghamdi, H.; A Jansen, J. Bone Regeneration Associated with Nontherapeutic and Therapeutic Surface Coatings for Dental Implants in Osteoporosis. Tissue Eng. Part B Rev. 2013, 19, 233–253. [Google Scholar] [CrossRef]
- Junker, R.; Dimakis, A.; Thoneick, M.; A Jansen, J. Effects of implant surface coatings and composition on bone integration: A systematic review. Clin. Oral Implant. Res. 2009, 20, 185–206. [Google Scholar] [CrossRef]
- Le Guehennec, L.; Soueidan, A.; Layrolle, P.; Amouriq, Y. Surface treatments of titanium dental implants for rapid osseointegration. Dent. Mater. 2007, 23, 844–854. [Google Scholar] [CrossRef] [PubMed]
- Alghamdi, H.; Van Oirschot, B.A.; Bosco, R.; Beucken, J.J.V.D.; Aldosari, A.A.F.; Anil, S.; A Jansen, J. Biological response to titanium implants coated with nanocrystals calcium phosphate or type 1 collagen in a dog model. Clin. Oral Implant. Res. 2012, 24, 475–483. [Google Scholar] [CrossRef] [PubMed]
- Davies, J.E. Understanding Peri-Implant Endosseous Healing. J. Dent. Educ. 2003, 67, 932–949. [Google Scholar] [CrossRef] [PubMed]
- Meng, H.-W.; Chien, E.Y.; Chien, H.-H. Dental implant bioactive surface modifications and their effects on osseointegration: A review. Biomark. Res. 2016, 4, 24. [Google Scholar] [CrossRef]
- James, A.W.; Lachaud, G.; Shen, J.; Asatrian, G.; Nguyen, V.; Zhang, X.; Ting, K.; Soo, C. A Review of the Clinical Side Effects of Bone Morphogenetic Protein-2. Tissue Eng. Part B Rev. 2016, 22, 284–297. [Google Scholar] [CrossRef]
- Nadar, R.A.; Beucken, J.J.V.D.; Leeuwenburgh, S.C. Chapter 10—Pharmacological Interventions Targeting Bone Diseases in Adjunction with Bone Grafting; Chapter 10; Alghamdi, H., Jansen, J.A., Eds.; Dental Implants and Bone Grafts, Woodhead Publishing, Elsevier: Amsterdam, The Netherlands, 2020; pp. 251–280. [Google Scholar]
- Ayukawa, Y.; Ogino, Y.; Moriyama, Y.; Atsuta, I.; Jinno, Y.; Kihara, M.; Tsukiyama, Y.; Koyano, K. Simvastatin enhances bone formation around titanium implants in rat tibiae. J. Oral Rehabil. 2010, 37, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Back, D.A.; Pauly, S.; Rommel, L.; Haas, N.P.; Schmidmaier, G.; Wildemann, B.; Greiner, S. Effect of local zoledronate on implant osseointegration in a rat model. BMC Musculoskelet. Disord. 2012, 13, 42. [Google Scholar] [CrossRef]
- Basudan, A.M.; Shaheen, M.Y.; De Vries, R.B.; Beucken, J.J.V.D.; Jansen, J.A.; Alghamdi, H.S. Antiosteoporotic Drugs to Promote Bone Regeneration Related to Titanium Implants: A Systematic Review and Meta-Analysis. Tissue Eng. Part B Rev. 2019, 25, 89–99. [Google Scholar] [CrossRef] [PubMed]
- Tarantino, U.; Cerocchi, I.; Celi, M.; Scialdoni, A.; Saturnino, L.; Gasbarra, E. Pharmacological agents and bone healing. Clin. Cases Miner. Bone Metab. 2009, 6, 144–148. [Google Scholar] [PubMed]
- Moraschini, V.; Almeida, D.; Calasans-Maia, J.; Calasans-Maia, M.D. The ability of topical and systemic statins to increase osteogenesis around dental implants: A systematic review of histomorphometric outcomes in animal studies. Int. J. Oral Maxillofac. Surg. 2018, 47, 1070–1078. [Google Scholar] [CrossRef] [PubMed]
- He, Y.; Bao, W.; Wu, X.-D.; Huang, W.; Chen, H.; Li, Z. Effects of Systemic or Local Administration of Zoledronate on Implant Osseointegration: A Preclinical Meta-Analysis. BioMed Res. Int. 2019, 2019, 9541485. [Google Scholar] [CrossRef] [PubMed]
- Abumoussa, S.; Ruppert, D.S.; Lindsay, C.; Dahners, L.; Weinhold, P.; Abumoussa, S. Local delivery of a zoledronate solution improves osseointegration of titanium implants in a rat distal femur model. J. Orthop. Res. 2018, 36, 3294–3298. [Google Scholar] [CrossRef] [PubMed]
- Hou, M.; Lee, R.S.; Du, Z.; Hamlet, S.; Vaquette, C.; Ivanovski, S. The influence of high-dose systemic zoledronate administration on osseointegration of implants with different surface topography. J. Periodontal Res. 2019, 54, 633–643. [Google Scholar] [CrossRef]
- Kellesarian, S.; Al Amri, M.; Al-Kheraif, A.; Ghanem, A.; Malmstrom, H.; Javed, F. Efficacy of Local and Systemic Statin Delivery on the Osseointegration of Implants: A Systematic Review. Int. J. Oral Maxillofac. Implant. 2017, 32, 497–506. [Google Scholar] [CrossRef]
- Ji, W.; Wang, H.; Beucken, J.J.V.D.; Yang, F.; Walboomers, X.F.; Leeuwenburgh, S.; A Jansen, J. Local delivery of small and large biomolecules in craniomaxillofacial bone. Adv. Drug Deliv. Rev. 2012, 64, 1152–1164. [Google Scholar] [CrossRef]
- Shi, J.; Votruba, A.R.; Farokhzad, O.C.; Langer, R. Nanotechnology in Drug Delivery and Tissue Engineering: From Discovery to Applications. Nano Lett. 2010, 10, 3223–3230. [Google Scholar] [CrossRef]
- Alghamdi, H.; Beucken, J.J.V.D.; Jansen, J.A. Osteoporotic Rat Models for Evaluation of Osseointegration of Bone Implants. Tissue Eng. Part C Methods 2014, 20, 493–505. [Google Scholar] [CrossRef]
- Giro, G.; Coelho, P.G.; Pereira, R.; Jorgetti, V.; Marcantonio-Junior, E.; Orrico, S.R.P. The effect of oestrogen and alendronate therapies on postmenopausal bone loss around osseointegrated titanium implants. Clin. Oral Implant. Res. 2010, 22, 259–264. [Google Scholar] [CrossRef]
- Orimo, H.; Nakamura, T.; Hosoi, T.; Iki, M.; Uenishi, K.; Endo, N.; Ohta, H.; Shiraki, M.; Sugimoto, T.; Suzuki, T.; et al. Japanese 2011 guidelines for prevention and treatment of osteoporosis—Executive summary. Arch. Osteoporos. 2012, 7, 3–20. [Google Scholar] [CrossRef]
- Orimo, H.; Nakamura, T.; Fukunaga, M.; Ohta, H.; Hosoi, T.; Uemura, Y.; Kuroda, T.; Miyakawa, N.; Ohashi, Y.; Shiraki, M.; et al. Effects of alendronate plus alfacalcidol in osteoporosis patients with a high risk of fracture: The Japanese Osteoporosis Intervention Trial (JOINT)–02. Curr. Med. Res. Opin. 2011, 27, 1273–1284. [Google Scholar] [CrossRef] [PubMed]
- Bobyn, J.D.; McKenzie, K.; Karabasz, D.; Krygier, J.J.; Tanzer, M. Locally Delivered Bisphosphonate for Enhancement of Bone Formation and Implant Fixation. J. Bone Jt. Surg. Am. 2009, 91, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Toker, H.; Ozdemir, H.; Ozer, H.; Eren, K. Alendronate enhances osseous healing in a rat calvarial defect model. Arch. Oral Biol. 2012, 57, 1545–1550. [Google Scholar] [CrossRef] [PubMed]
- Du, Z.; Chen, J.; Yan, F.; Doan, N.; Ivanovski, S.; Xiao, Y. Serum bone formation marker correlation with improved osseointegration in osteoporotic rats treated with simvastatin. Clin. Oral Implant. Res. 2011, 24, 422–427. [Google Scholar] [CrossRef]
- Jakobsen, T.; Bechtold, J.E.; Søballe, K.; Jensen, T.; Greiner, S.; Vestermark, M.T.; Baas, J. Local delivery of zoledronate from a poly (D,L-lactide)-Coating increases fixation of press-fit implants. J. Orthop. Res. 2015, 34, 65–71. [Google Scholar] [CrossRef]
- Vohra, F.; Al-Rifaiy, M.Q.; Almas, K.; Javed, F. Efficacy of systemic bisphosphonate delivery on osseointegration of implants under osteoporotic conditions: Lessons from animal studies. Arch. Oral Biol. 2014, 59, 912–920. [Google Scholar] [CrossRef]
- Eberhardt, C.; Stumpf, U.; Brankamp, J.; Schwarz, M.; Kurth, A. Osseointegration of Cementless Implants with Different Bisphosphonate Regimens. Clin. Orthop. Relat. Res. 2006, 447, 195–200. [Google Scholar] [CrossRef]
- An, T.; Hao, J.; Sun, S.; Li, R.; Yang, M.; Cheng, G.; Zou, M. Efficacy of statins for osteoporosis: A systematic review and meta-analysis. Osteoporos. Int. 2016, 28, 47–57. [Google Scholar] [CrossRef]
- Handool, K.O.; Ibrahim, S.; Kaka, U.; Omar, M.A.; Abu, J.; Sabri, M.Y.; Yusof, L.M. Optimization of a closed rat tibial fracture model. J. Exp. Orthop. 2018, 5, 13. [Google Scholar] [CrossRef]
- Shalabi, M.M.; Wolke, J.G.C.; De Ruijter, A.J.E.; A Jansen, J. Histological evaluation of oral implants inserted with different surgical techniques into the trabecular bone of goats. Clin. Oral Implant. Res. 2007, 18, 489–495. [Google Scholar] [CrossRef]
- Tabassum, A.; Meijer, G.J.; Walboomers, F.X.; A Jansen, J. Biological limits of the undersized surgical technique: A study in goats. Clin. Oral Implant. Res. 2010, 22, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Kurth, A.; Eberhardt, C.; Muller, S.; Steinacker, M.; Schwarz, M.; Bauss, F. The bisphosphonate ibandronate improves implant integration in osteopenic ovariectomized rats. Bone 2005, 37, 204–210. [Google Scholar] [CrossRef] [PubMed]
- Dhert, W.J.A.; Klein, C.P.A.T.; Wolke, J.G.C.; Van Der Velde, E.A.; De Groot, K.; Rozing, P.M. A mechanical investigation of fluorapatite, magnesiumwhitlockite, and hydroxylapatite plasma-sprayed coatings in goats. J. Biomed. Mater. Res. 1991, 25, 1183–1200. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Groups | Osteoporotic Condition | Healthy Condition | ||||||
|---|---|---|---|---|---|---|---|---|
| No. Placed Implants | No. Retrieved Implants | No. Used Implants | No. Placed Implants | No. Retrieved Implants | No. Used Implants | |||
| Push-Out | Histology | Push-Out | Histology | |||||
| ALN | 10 | 8 * | 3 | 5 | 10 | 9 * | 3 | 6 |
| SIM | 10 | 10 | 3 | 7 | 10 | 9 * | 3 | 6 |
| ALN+SIM | 10 | 9 * | 3 | 6 | 10 | 10 | 3 | 7 |
| Saline | 10 | 10 | 3 | 7 | 10 | 9 * | 3 | 6 |
| Groups | Osteoporotic Condition | Healthy Condition | ||||
|---|---|---|---|---|---|---|
| Push-Out (N) | Histomorphometric | Push-Out (N) | Histomorphometric | |||
| BA% | BIC% | BA% | BIC% | |||
| ALN | 12.0 ± 4.2 | 21.7 ± 7.1 | 57.9 ± 26.3 | 18.5 ± 7.2 | 18.0 ± 6.3 | 44.6 ± 15.7 |
| SIM | 9.0 ± 1.1 | 14.5 ± 5.0 | 29.4 ± 22.3 | 7.5 ± 1.4 | 19.8 ± 4.5 | 55.8 ± 27.6 |
| ALN+SIM | 12.7 ± 3.6 | 15.5 ± 6.1 | 63.2 ± 21.1 | 14.0 ± 3.0 | 22.6 ± 2.8 | 48.4 ± 31.7 |
| Saline | 13.5 ± 3.8 | 9.2 ± 2.4 | 51.1 ± 20.2 | 15.2 ± 5.2 | 11.1 ± 3.5 | 38.0 ± 20.3 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Basudan, A.M.; Shaheen, M.Y.; Niazy, A.A.; van den Beucken, J.J.J.P.; Jansen, J.A.; Alghamdi, H.S. Biological Effect of Single or Combined Pharmacological Therapy Using Alendronate and Simvastatin on Implant Osseointegration: An In Vivo Study in Healthy and Osteoporotic Rat Models. Appl. Sci. 2020, 10, 4298. https://doi.org/10.3390/app10124298
Basudan AM, Shaheen MY, Niazy AA, van den Beucken JJJP, Jansen JA, Alghamdi HS. Biological Effect of Single or Combined Pharmacological Therapy Using Alendronate and Simvastatin on Implant Osseointegration: An In Vivo Study in Healthy and Osteoporotic Rat Models. Applied Sciences. 2020; 10(12):4298. https://doi.org/10.3390/app10124298
Chicago/Turabian StyleBasudan, Amani M., Marwa Y. Shaheen, Abdurahman A. Niazy, Jeroen J.J.P. van den Beucken, John A. Jansen, and Hamdan S. Alghamdi. 2020. "Biological Effect of Single or Combined Pharmacological Therapy Using Alendronate and Simvastatin on Implant Osseointegration: An In Vivo Study in Healthy and Osteoporotic Rat Models" Applied Sciences 10, no. 12: 4298. https://doi.org/10.3390/app10124298
APA StyleBasudan, A. M., Shaheen, M. Y., Niazy, A. A., van den Beucken, J. J. J. P., Jansen, J. A., & Alghamdi, H. S. (2020). Biological Effect of Single or Combined Pharmacological Therapy Using Alendronate and Simvastatin on Implant Osseointegration: An In Vivo Study in Healthy and Osteoporotic Rat Models. Applied Sciences, 10(12), 4298. https://doi.org/10.3390/app10124298