Self-Leadership and Psychological Capital as Key Cognitive Resources for Shaping Health-Protective Behaviors during the COVID-19 Pandemic





Abstract
1. Introduction
2. Literature Review
2.1. Self-Leadership
2.2. Psychological Capital (PsyCap)
2.3. Coping Self-Efficacy
2.4. Health-Protective Behaviors
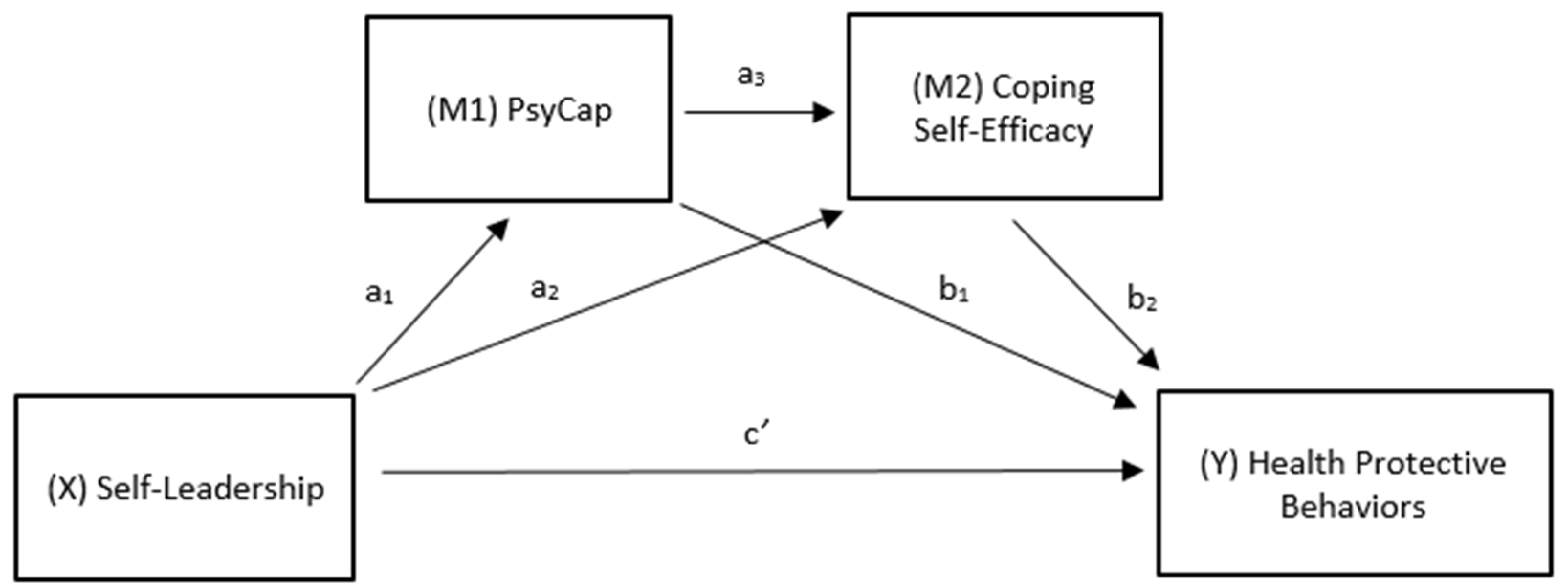
3. Conceptual Model and Hypothesis Development
4. Method
4.1. Participants and Procedures
4.2. Measures
5. Results
6. Discussion
6.1. Research Implications
6.2. Practical Implications
6.3. Limitations and Future Research
6.4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ajzen, Icek A. 2002. Perceived behavioral control, self-efficacy, locus of control, and the theory of planned behavior. Journal of Applied Social Psychology 32: 665–83. [Google Scholar] [CrossRef]
- Ali, Shahmir H., Joshua Foreman, Yesim Tozan, Ariadna Capasso, Abbey M. Jones, and Ralph J. DiClemente. 2020. Trends and Predictors of COVID-19 Information Sources and Their Relationship with Knowledge and Beliefs Related to the Pandemic: Nationwide Cross-Sectional Study. JMIR Public Health and Surveillance 6: e21071. [Google Scholar] [CrossRef] [PubMed]
- Andrasik, Frank, and Judy S. Heimberg. 1982. Self-Management Procedures. In Handbook of Organizational Behavior Management. Edited by Lee W. Frederikson. New York: Wiley, pp. 219–47. [Google Scholar]
- Andressen, Panja, Udo Konradt, and Christopher P. Neck. 2012. The relation between self-leadership and transformational leadership: Competing models and the moderating role of virtuality. Journal of Leadership & Organizational Studies 19: 68–82. [Google Scholar]
- Avey, James B., Fred Luthans, and Susan M. Jensen. 2009. Psychological capital: A positive resource for combating employee stress and turnover. Human Resource Management 48: 677–93. [Google Scholar] [CrossRef]
- Avey, James B., Rebecca J. Reichard, Fred Luthans, and Ketan H. Mhatre. 2011. Meta-analysis of the impact of positive psychological capital on employee attitudes, behaviors, and performance. Human Resource Development Quarterly 22: 127–52. [Google Scholar] [CrossRef]
- Bandura, Albert. 1986. Social Foundations of Thought and Action: A Social Cognitive Theory. Englewood Cliffs: Prentice-Hall. [Google Scholar]
- Bassett-Gunter, Rebecca L., Amy E. Latimer-Cheung, Kathleen A. Martin Ginis, and Monica Castelhano. 2014. I spy with my little eye: Cognitive processing of framed physical activity messages. Journal of Health Communication 19: 676–91. [Google Scholar] [CrossRef] [PubMed]
- Benight, Charles C., Erika Swift, Jean Sanger, Anne Smith, and Dan Zeppelin. 1999. Coping self-efficacy as a mediator of distress following a natural disaster. Journal of Applied Social Psychology 29: 2443–64. [Google Scholar] [CrossRef]
- Berkanovic, Emil. 1981. Who Engages in Health Protective Behaviors? International Quarterly of Community Health Education 2: 225–37. [Google Scholar] [CrossRef]
- Bishop, Scott R., Mark Lau, Shauna Shapiro, Linda Carlson, Nicole D. Anderson, James Carmody, Zindel V. Segal, Susan Abbey, Michael Speca, Drew Velting, and et al. 2004. Mindfulness: A proposed operational definition. Clinical Psychology: Science and Practice 11: 230–41. [Google Scholar] [CrossRef]
- Carpenter, Christopher J. 2010. A meta-analysis of the effectiveness of Health Belief Model variables in predicting behavior. Health Communication 25: 661–69. [Google Scholar] [CrossRef]
- Carver, Charles S., and Michael F. Scheier. 1998. On the Self-Regulation of Behavior. Cambridge: Cambridge University Press. [Google Scholar]
- Centers for Disease Control and Prevention. 2021a. COVID-19: Considerations for Wearing Masks; Washington, DC: Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/cloth-face-cover-guidance.html (accessed on 21 February 2021).
- Centers for Disease Control and Prevention. 2021b. CDC COVID Data Tracker; Washington, DC: Centers for Disease Control and Prevention. Available online: https://covid.cdc.gov/covid-data-tracker/#cases_casesper100klast7days (accessed on 21 February 2021).
- Chesney, Margaret A., Donald B. Chambers, Jonelle M. Taylor, Lisa M. Johnson, and Susan Folkman. 2003. Coping effectiveness training for men living with HIV: Results from a randomized clinical trial testing a group-based intervention. Psychosomatic Medicine 65: 1038–46. [Google Scholar] [CrossRef]
- Chesney, Margaret A., Torsten B. Neilands, Donald B. Chambers, Jonelle M. Taylor, and Susan Folkman. 2006. A validity and reliability study of the coping self-efficacy scale. British Journal of Health Psychology 11: 421–37. [Google Scholar] [CrossRef]
- Cieslak, Roman, Charles C. Benight, and Victoria Caden Lehman. 2008. Coping self-efficacy mediates the effects of negative cognitions on posttraumatic distress. Behaviour Research and Therapy 46: 788–98. [Google Scholar] [CrossRef]
- Dawkins, Sarah, Angela Martin, Jenn Scott, and Kristy Sanderson. 2013. Building on the positives: A psychometric review and critical analysis of the construct of psychological capital. Journal of Occupational & Organizational Psychology 86: 348–70. [Google Scholar]
- Duckworth, Angela Lee, and Patrick D. Quinn. 2009. Development and validation of the Short Grit Scale (GRIT–S). Journal of Personality Assessment 91: 166–74. [Google Scholar] [CrossRef]
- Fridman, Ilona, Nicole Lucas, Debra Henke, and Christina K. Zigler. 2020. Association Between Public Knowledge About COVID-19, Trust in Information Sources, and Adherence to Social Distancing: Cross-Sectional Survey. JMIR Public Health and Surveillance 6: e22060. [Google Scholar] [CrossRef] [PubMed]
- Glanz, Karen, Barbara K. Rimer, and K. Viswanath. 2015. Health Behavior: Theory, Research, and Practice, 5th ed. San Francisco: Jossey-Bass. [Google Scholar]
- Godwin, Jeffrey L., Christopher P. Neck, and Robert S. D’Intino 2016. Self-leadership, spirituality, and entrepreneur performance: A conceptual model. Journal of Management, Spirituality & Religion 13: 64–78.
- Gupta, Bindu, Rakesh Singh, Sandeep Puri, and Pankaj Rawat. 2020. Psychological Capital and Performance: Roles of Thought Self-Leadership, Engagement, and Feedback. In Academy of Management Proceedings. Briarcliff Manor: Academy of Management, p. 19263. [Google Scholar]
- Harunavamwe, Martha, Petrus Nel, and Ebben Van Zyl. 2020. The influence of self-leadership strategies, psychological resources, and job embeddedness on work engagement in the banking industry. South African Journal of Psychology 50: 507–19. [Google Scholar] [CrossRef]
- Hauser, Christine. 2020. The mask slackers of 1918. The New York Times. August 3. Available online: https://www.nytimes.com/2020/08/03/us/mask-protests-1918.html (accessed on 25 February 2021).
- Hayes, Andrew F. 2013. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach. New York: Guilford. [Google Scholar]
- Hayes, Andrew F., and Nicholas J. Rockwood. 2017. Regression-based statistical mediation and moderation analysis in clinical research: Observations, recommendations, and implementation. Behaviour Research and Therapy 98: 39–57. [Google Scholar] [CrossRef]
- Hobfoll, Stevan E. 2002. Social and psychological resources and adaptation. Review of General Psychology 6: 307–24. [Google Scholar] [CrossRef]
- Ho, Jessie, and Paul L. Nesbit. 2009. A refinement and extension of the self-leadership scale for the Chinese context. Journal of Managerial Psychology 24: 450–76. [Google Scholar] [CrossRef]
- Ho, Shirley S., Xianghong Peh, and Veronica W. L. Soh. 2013. The cognitive mediation model: Factors influencing public knowledge of the H1N1 pandemic and intention to take precautionary behaviors. Journal of Health Communication 18: 773–94. [Google Scholar] [CrossRef]
- Holton, Kim, Adam E. Barry, and J. Don Chaney. 2016. Employee stress management: An examination of adaptive and maladaptive coping strategies on employee health. Work 53: 299–305. [Google Scholar] [CrossRef] [PubMed]
- Houghton, Jeffery D., David Dawley, and Trudy C. DiLiello. 2012a. The abbreviated self-leadership questionnaire (ASLQ): A more concise measure of self-leadership. International Journal of Leadership Studies 7: 216–32. [Google Scholar]
- Houghton, Jeffery D., Jinpei Wu, Jeffrey L. Godwin, Christopher P. Neck, and Charles C. Manz. 2012b. Effective stress management: A model of emotional intelligence, self-leadership, and student stress coping. Journal of Management Education 36: 220–38. [Google Scholar] [CrossRef]
- Jones, Christina L., Jacob D. Jensen, Courtney L. Scherr, Natasha R. Brown, Katheryn Christy, and Jeremy Weaver. 2015. The health belief model as an explanatory framework in communication research: Exploring parallel, serial, and moderated mediation. Health Communication 30: 566–76. [Google Scholar] [CrossRef] [PubMed]
- Kotzé, Martina. 2018. The influence of psychological capital, self-leadership, and mindfulness on work engagement. South African Journal of Psychology 48: 279–92. [Google Scholar] [CrossRef]
- Kotzé, Martina. 2021. The relationship between public service employees’ personal resources and psychological well-being. International Review of Administrative Sciences. [Google Scholar] [CrossRef]
- Krick, John P., and Jeffery Sobal. 1990. Relationships between health protective behaviors. Journal of Community Health 15: 19–34. [Google Scholar] [CrossRef]
- Lazarus, Richard S., and Susan Folkman. 1984. Stress, Appraisal, and Coping. New York: Springer. [Google Scholar]
- Lindell, Michael K., and David J. Whitney. 2001. Accounting for common method variance in cross-sectional research designs. Journal of Applied Psychology 86: 114. [Google Scholar] [CrossRef]
- Little, Becky. 2020. When Mask-Wearing Rules in the 1918 Pandemic Faced Resistance. Available online: https://www.history.com/news/1918-spanish-flu-mask-wearing-resistance (accessed on 28 February 2021).
- Lovelace, Kathi J., Charles C. Manz, and Jose C. Alves. 2007. Work stress and leadership development: The role of self-leadership, shared leadership, physical fitness and flow in managing demands and increasing job control. Human Resource Management Review 17: 374–87. [Google Scholar] [CrossRef]
- Luberto, Christina M., Sian Cotton, Allison C. McLeish, Carolyn J. Mingione, and Emily M. O’Bryan. 2014. Mindfulness skills and emotion regulation: The mediating role of coping self-efficacy. Mindfulness 5: 373–80. [Google Scholar] [CrossRef]
- Luthans, Fred, Bruce J. Avolio, James B. Avey, and Steven M. Norman. 2007. Positive psychological capital: Measurement and relationship with performance and satisfaction. Personnel Psychology 60: 541–72. [Google Scholar] [CrossRef]
- Luthans, Fred, James B. Avey, and Jaime L. Patera. 2008. Experimental analysis of a web-based training intervention to develop positive psychological capital. Academy of Management Learning & Education 7: 209–21. [Google Scholar]
- Malhotra, Naresh K., Sung S. Kim, and Ashutosh Patil. 2006. Common method variance in IS research: A comparison of alternative approaches and a reanalysis of past research. Management Science 52: 1865–83. [Google Scholar] [CrossRef]
- Manz, Charles C. 1986. Self-leadership: Toward an expanded theory of self-influence processes in organizations. Academy of Management Review 11: 585–600. [Google Scholar] [CrossRef]
- Manz, Charles C., and Henry P. Sims, Jr. 1980. Self-management as a substitute for leadership: A social learning perspective. Academy of Management Review 5: 361–67. [Google Scholar] [CrossRef]
- Maykrantz, Sherry A., and Jeffery D. Houghton. 2020. Self-leadership and stress among college students: Examining the moderating role of coping skills. Journal of American College Health 68: 89–96. [Google Scholar] [CrossRef]
- Neck, Christopher P., and Charles C. Manz. 1992. Thought Self-Leadership: The Influence of Self-Talk and Mental Imagery on Performance. Journal of Organizational Behavior 13: 681–99. [Google Scholar] [CrossRef]
- Neck, Christopher P., and Charles C. Manz. 1996. Thought Self-Leadership: The Impact of Mental Strategies Training on Employee Cognition, Behavior, and Affect. Journal of Organizational Behavior 17: 445–67. [Google Scholar] [CrossRef]
- Neck, Christopher P., and Jeffery D. Houghton. 2006. Two decades of self-leadership theory and research: Past developments, present trends, and future possibilities. Journal of Managerial Psychology 21: 270–95. [Google Scholar] [CrossRef]
- Neck, Christopher P., Charles C. Manz, and Jeffery D. Houghton. 2020. Self-Leadership: The Definitive Guide to Personal Excellence (2e). Thousand Oaks: SAGE Publications. [Google Scholar]
- Neck, Christopher P., Jeffery D. Houghton, Shruti R. Sardeshmukh, Michael Goldsby, and Jeffery L. Godwin. 2013. Self-leadership: A cognitive resource for entrepreneurs. Journal of Small Business & Entrepreneurship 26: 463–80. [Google Scholar]
- Nobiling, Brandye D., and Sherry A. Maykrantz. 2017. Exploring perceptions about and behaviors related to mental illness and mental health service utilization among college students using the Health Belief Model (HBM). American Journal of Health Education 48: 306–19. [Google Scholar] [CrossRef]
- O’Keefe, Daniel J., and Jakob D. Jensen. 2007. The relative persuasiveness of gain-framed loss-framed messages for encouraging disease prevention behaviors: A meta-analytic review. Journal of Health Communication 12: 623–44. [Google Scholar]
- O’Keefe, Daniel J., and Jakob D. Jensen. 2008. Do loss-framed persuasive messages engender greater message processing than do gain-framed messages? A meta-analytic review. Communication Studies 59: 51–67. [Google Scholar] [CrossRef]
- Podsakoff, Philip M., Scott B. MacKenzie, Jeong-Yeon Lee, and Nathan P. Podsakoff. 2003. Common method biases in behavioral research: A critical review of the literature and recommended remedies. Journal of Applied Psychology 88: 879–903. [Google Scholar] [CrossRef]
- Prati, Gabriele, Luca Pietrantoni, and Bruna Zani. 2011. A social-cognitive model of pandemic influenza H1N1 risk perception and recommended behaviors in Italy. Risk Analysis: An International Journal 31: 645–56. [Google Scholar] [CrossRef]
- Prussia, Gregory E., Joe S. Anderson, and Charles C. Manz. 1998. Self-leadership and performance outcomes: The mediating influence of self-efficacy. Journal of Organizational Behavior 19: 523–38. [Google Scholar] [CrossRef]
- Qazi, Atika, Javaria Qazi, Khulla Naseer, Muhammad Zeeshan, Glenn Hardaker, Jaafar Z. Maitama, and Khalid Haruna. 2020. Analyzing situational awareness through public opinion to predict adoption of social distancing amid pandemic COVID-19. Journal of Medical Virology 92: 849–55. [Google Scholar] [CrossRef] [PubMed]
- Rosenstock, Irwin M., Victor J. Strecher, and Marshall H. Becker. 1988. Social learning theory and the Health Belief Model. Health Education Quarterly 15: 175–83. [Google Scholar] [CrossRef] [PubMed]
- Rossman, Christian, Michaela O’Brian, Gloria Poisson, and Abubakry Tunkra. 2017. Models and mechanisms of public health. In Chapter 5: Key Principles of Health Behavior Change. Available online: https://courses.lumenlearning.com/suny-buffalo-environmentalhealth/part/chapter-5/ (accessed on 25 February 2021).
- Rothman, Alexander J., and Peter Salovey. 1997. Shaping perceptions to motivate healthy behavior: The role of message framing. Psychological Bulletin 121: 3. [Google Scholar] [CrossRef]
- Schelleman-Offermans, Karen, and Karlijn Massar. 2020. Explaining socioeconomic inequalities in self-reported health outcomes: The mediating role of perceived life stress, financial self-reliance, psychological capital, and time perspective orientations. PLoS ONE 15: e0243730. [Google Scholar] [CrossRef]
- Slambl, James. K. 2021. The effect of self-leadership competencies on the perceived ability of school leaders to cope with COVID-19 pandemic crisis challenges in Jeddah schools, Saudi Arabia. Research & Reviews: Journal of Educational Studies 7: 1–13. [Google Scholar]
- Spector, Paul E. 2006. Method variance in organizational research: Truth or urban legend? Organizational Research Methods 9: 221–32. [Google Scholar]
- Spector, Paul E., Christopher C. Rosen, Hettie A. Richardson, Larry J. Williams, and Russell E. Johnson. 2019. A new perspective on method variance: A measure-centric approach. Journal of Management 45: 855–80. [Google Scholar] [CrossRef]
- Stewart, Greg L., Kenneth P. Carson, and Robert L. Cardy. 1996. The joint effects of conscientiousness and self-leadership training on employee self-directed behavior in a service setting. Personnel Psychology 49: 143–64. [Google Scholar] [CrossRef]
- Sumer, Nebi, Nuray A. Karanci, Sibel K. Berument, and Hatice Gunes. 2005. Personal resources, coping self-efficacy, and quake exposure as predictors of psychological distress following the 1999 earthquake in Turkey. Journal of Traumatic Stress: Official Publication of The International Society for Traumatic Stress Studies 18: 331–42. [Google Scholar] [CrossRef]
- Taylor, Shelley E., Margaret E. Kemeny, Geoffrey M. Reed, Julienne E. Bower, and Tara L. Gruenewald. 2000. Psychological resources, positive illusions, and health. American Psychologist 55: 99. [Google Scholar] [CrossRef]
- Thoresen, Carl E., and Michael J. Mahoney. 1974. Behavioral Self-Control. New York: Holt Rinehart & Winston. [Google Scholar]
- Wang, Yefei, Guangrong Xie, and Xilong Cui. 2016. Effects of emotional intelligence and selfleadership on students’ coping with stress. Social Behavior and Personality: An International Journal 44: 853–64. [Google Scholar] [CrossRef]
- Wood, Robert, and Albert Bandura. 1989. Social cognitive theory of organizational management. Academy of Management Review 14: 361–84. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Mean | SD | 1 | 2 | 3 | 4 |
|---|---|---|---|---|---|---|
| 1. Self-Leadership | 2.37 | 0.61 | (0.79) | |||
| 2. Psychological Capital | 4.62 | 0.58 | 0.50 * | (0.90) | ||
| 3. Coping Self-Efficacy | 6.74 | 1.43 | 0.36 * | 0.62 * | (0.94) | |
| 4. Health-Protective Behaviors a | 0.00 | 0.59 | 0.18 * | 0.21 * | 0.21 * | (0.84) |
| Regression Model | B | SE | t | p | LLCI | ULCI | |
|---|---|---|---|---|---|---|---|
| Outcome: PsyCap | |||||||
| F(1, 613) = 206.02, p < 0.001, R2 = 0.25 | |||||||
| Constant | 2.805 | 0.128 | 21.873 | <0.001 | 2.553 | 3.057 | |
| Self-Leadership (a1) | 0.471 | 0.033 | 14.354 | <0.001 | 0.407 | 0.536 | |
| Outcome: Coping Self-Efficacy | |||||||
| F(2, 612) = 188.97, p < 0.001, R2 = 0.38 | |||||||
| Constant | −0.541 | 0.386 | −1.401 | 0.162 | −1.300 | 0.217 | |
| PsyCap (a3) | 1.435 | 0.091 | 15.751 | <0.001 | 1.256 | 1.614 | |
| Self-Leadership (a2) | 0.1676 | 0.086 | 1.958 | 0.051 | −0.001 | 0.336 | |
| Outcome: Health-Protective Behaviors | |||||||
| F(3, 611) = 12.96, p < 0.001, R2 = 0.06 | |||||||
| Constant | −1.11 | 0.196 | −5.631 | <0.000 | −1.491 | −0.720 | |
| PsyCap (b1) | 0.103 | 0.055 | 1.875 | 0.0612 | −0.005 | 0.211 | |
| Coping Self-Efficacy (b2) | 0.046 | 0.021 | 2.251 | <0.05 | 0.006 | 0.087 | |
| Self-Leadership (c’) | 0.083 | 0.044 | 1.895 | 0.059 | −0.003 | 0.168 | |
| Bootstrapped | |||||||
| Indirect Effects and Serial Indirect Effect | SE | LLCI | ULCI | abcs | |||
| a1a3b2 (X → M1 → M2 → Y) = | 0.032 * | 0.014 | 0.005 | 0.060 | 0.033[0.005, 0.062] | ||
| a1b1 (X → M1 → Y) = | 0.049 | 0.028 | −0.005 | 0.102 | 0.051[−0.01, 0.107] | ||
| a2b2 (X → M2 → Y) = | 0.008 | 0.006 | −0.001 | 0.021 | 0.008[−0.001, 0.02] | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maykrantz, S.A.; Langlinais, L.A.; Houghton, J.D.; Neck, C.P. Self-Leadership and Psychological Capital as Key Cognitive Resources for Shaping Health-Protective Behaviors during the COVID-19 Pandemic. Adm. Sci. 2021, 11, 41. https://doi.org/10.3390/admsci11020041
Maykrantz SA, Langlinais LA, Houghton JD, Neck CP. Self-Leadership and Psychological Capital as Key Cognitive Resources for Shaping Health-Protective Behaviors during the COVID-19 Pandemic. Administrative Sciences. 2021; 11(2):41. https://doi.org/10.3390/admsci11020041
Chicago/Turabian StyleMaykrantz, Sherry A., Luke A. Langlinais, Jeffery D. Houghton, and Christopher P. Neck. 2021. "Self-Leadership and Psychological Capital as Key Cognitive Resources for Shaping Health-Protective Behaviors during the COVID-19 Pandemic" Administrative Sciences 11, no. 2: 41. https://doi.org/10.3390/admsci11020041
APA StyleMaykrantz, S. A., Langlinais, L. A., Houghton, J. D., & Neck, C. P. (2021). Self-Leadership and Psychological Capital as Key Cognitive Resources for Shaping Health-Protective Behaviors during the COVID-19 Pandemic. Administrative Sciences, 11(2), 41. https://doi.org/10.3390/admsci11020041