
FMECA Application in Tomotherapy: Comparison between Classic and Fuzzy Methodologies

 , , and
, , and
Abstract
1. Introduction
2. Classical and Fuzzy Approach of FMECA in Healthcare
- Failure/error modes;
- Potential causes;
- Failure consequences.
- Occurrence index, O, which represents the probability that a particular accidental event will occur;
- Severity index, S, which is a measure of the severity of consequences resulting from the undetected failure mode;
- Detection index, D, related to the probability that an incipient failure will be detected before the failure occurs.
- Relative importance among (O, D, S) is not taken into consideration;
- Different combinations of (O, D, S) produce the same RPN value (i.e., same rank order), even if risk levels are very different;
- It is difficult for the expert to accurately assess (O, D, S) parameters.
- Fuzzification process: numerical values of risk parameters (O, D, S) and RPN index are converted into linguistic variables to which fuzzy sets are associated. A degree of truth of each fuzzy set is characterized by a membership function generally defined by triangular or trapezoidal distributions [19,20,21,22]. For example, let us take parameter O relating to the occurrence probability of a failure mode; its value (in the range of 1–10) can be interpreted using fuzzy labels such as “low”, “medium”, “high”, etc. Each linguistic variable can be characterized by triangular distribution that is defined by three parameters: lower limit; peak value; upper limit. Peak value corresponds to the most probable value of the set data, whereas the lower and upper limit are the lower and upper bounds of the data interval;
- Fuzzy inference process: linguistic variables, classified as fuzzy sets, are processed using rules based on Fuzzy Logic (i.e., Fuzzy Rules of Inference). These rules are, generally, expressed as if-then conditions.
- An example of the if-then rule is: IF occurrence, O, is “Moderate” AND detectability, D, is “Low” AND severity, S, is “High” THEN risk priority number, RPN, is Moderate.
- Each rule has a weight w that denotes its degree of importance evaluated using weight wO, wD and wS assigned for O, D, S. More details are reported in [5];
- Defuzzification process: it maps RPN outputs from the fuzzy domain back into the crisp domain, in the range of 1–1000. In [5], RPN crisp value is evaluated using the analytical calculation of the “center of gravity” of the area produced by the combination of fuzzy RPN outputs.
3. FMECA Application in Tomotherapy
- Treatment planning (volume determination and treatment planning stages);
- Treatment execution (positioning and immobilization of the patient, execution of megavoltage (MV), computed tomography (CT) and irradiation).
- treatment planning: 74 failure/error modes are examined, 21 of them have exceeded the threshold value;
- treatment execution: 30 failure/error modes are examined, 9 of them have exceeded the threshold value.
3.1. Fuzzy Approach
4. Criteria of Comparison for Various FMECA Approaches
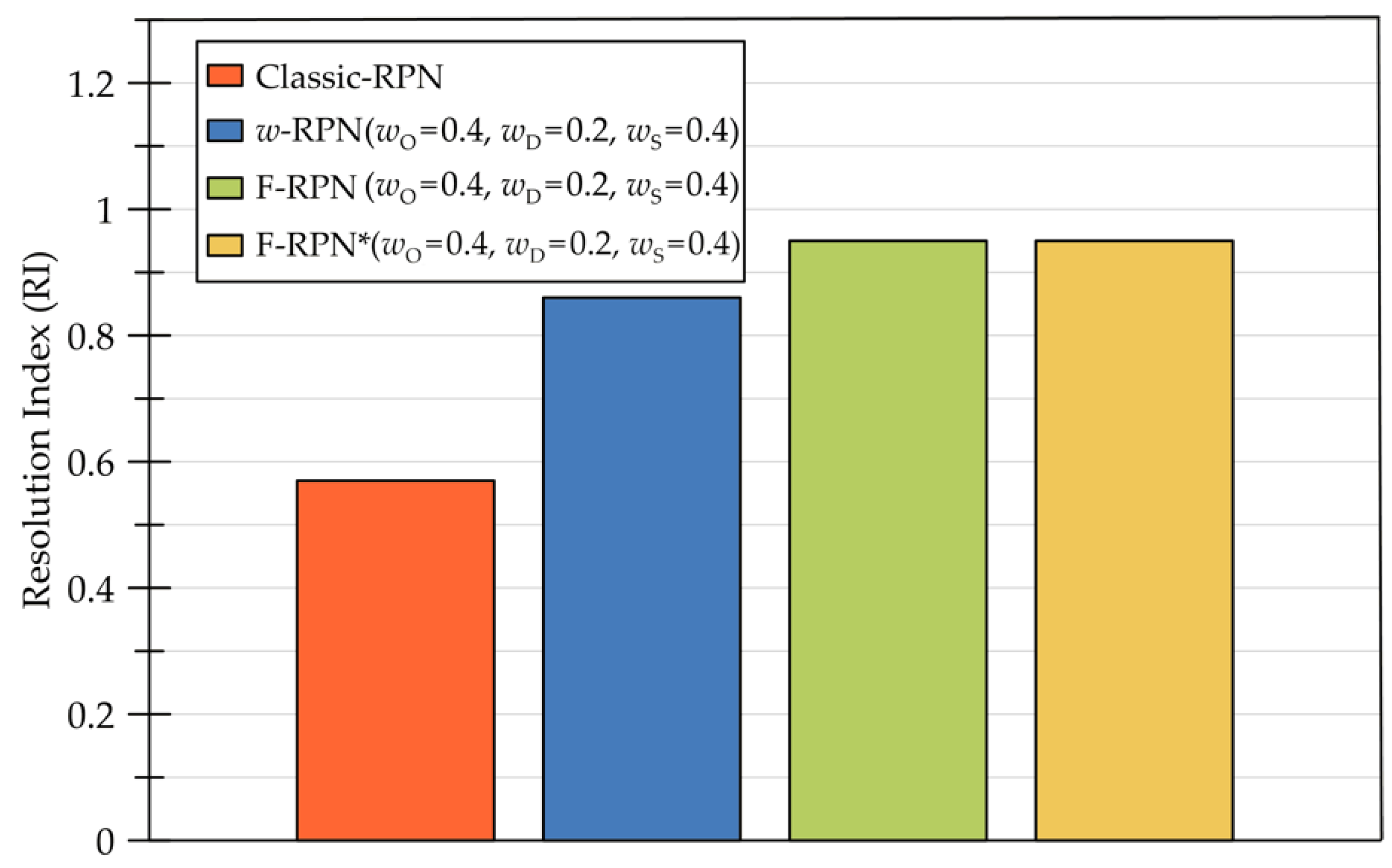
4.1. Resolving Capacity
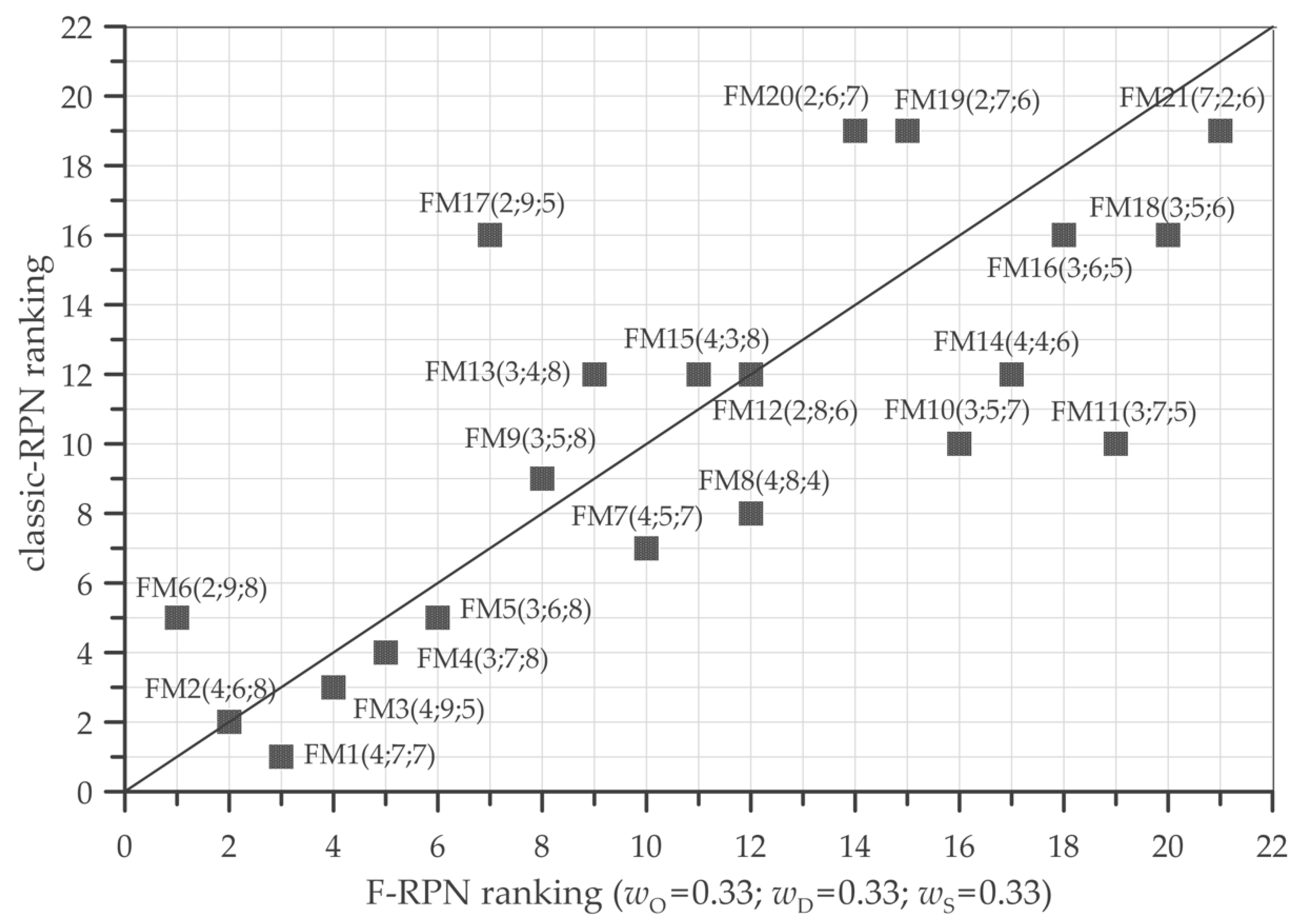
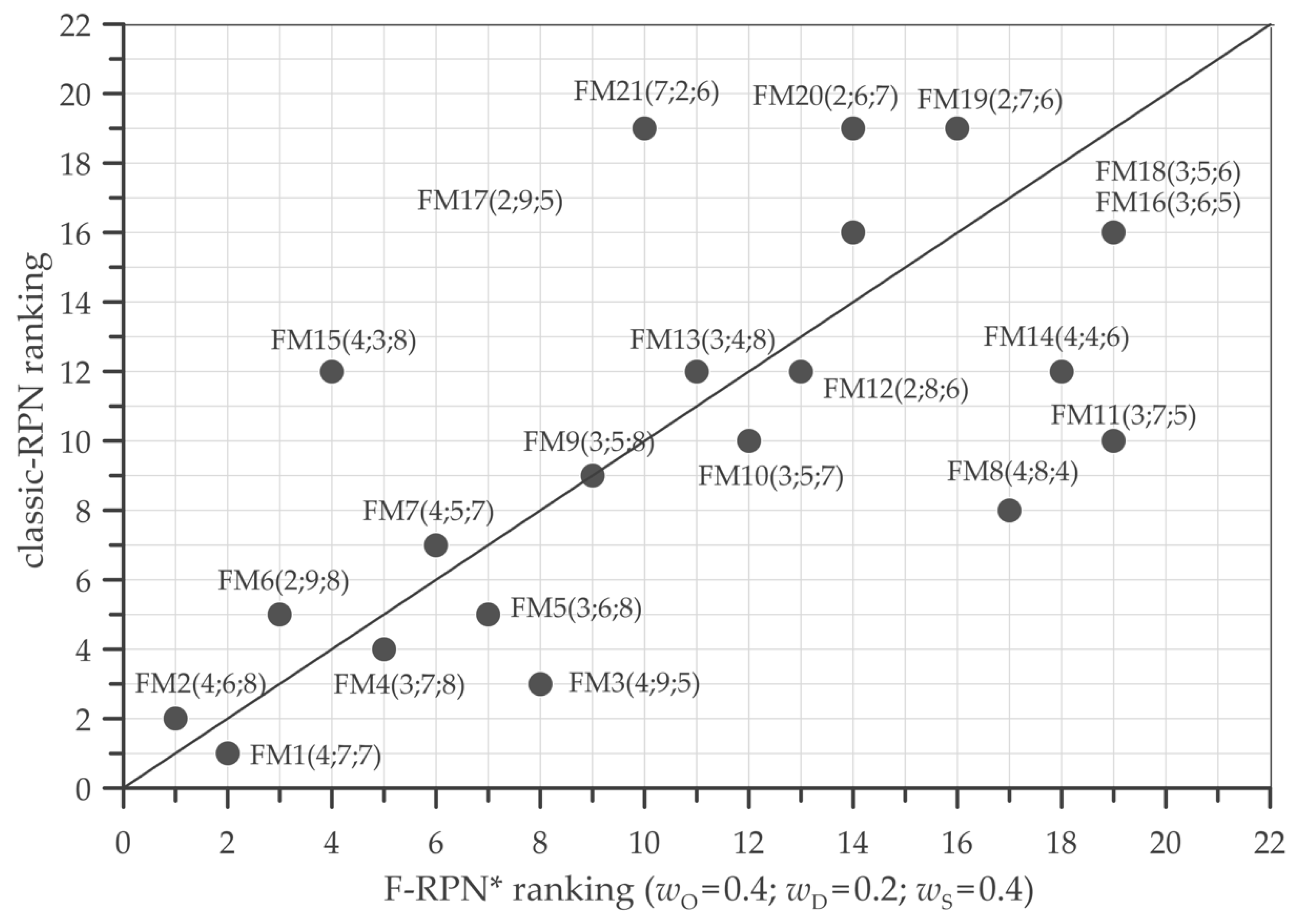
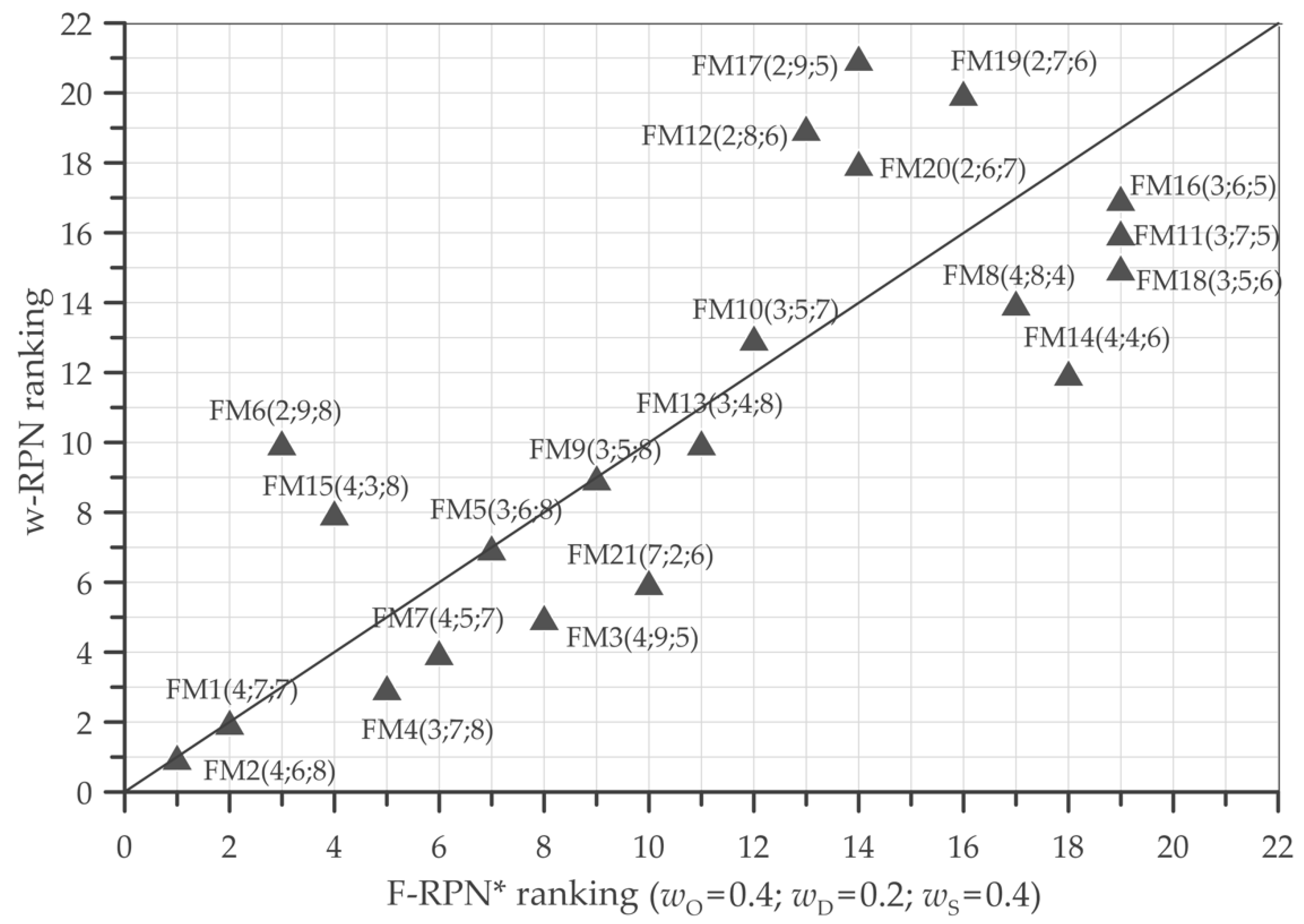
4.2. Ranking Capacity
5. Comparison Results
5.1. Comparison of Resolving Capacity for RPN Calculation
5.2. Ranking Capacity for RPN Calculation
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Huq, M.S.; Fraass, B.A.; Dunscombe, P.B.; Gibbons, J.P., Jr.; Ibbott, G.S.; Mundt, A.J.; Mutic, S.; Palta, J.R.; Rath, F.; Thomadsen, B.R.; et al. The report of Task Group 100 of the AAPM: Application of risk analysis methods to radiation therapy quality management. Med. Phys. 2016, 43, 4209–4262. [Google Scholar] [CrossRef] [PubMed]
- Thomadsen, B.R.; Dunscombe, P.; Ford, E.; Huq, S.; Pawlicki, T.; Sutlief, S. Quality and Safety in Radiotherapy: Learning the New Approaches in Task Group 100 and Beyond. In Medical Physics; Thomadsen, B., Ed.; Medical Physics Publishing, Inc.: Madison, WI, USA, 2013; pp. 274–349. ISBN 9781888340495. [Google Scholar]
- Bowles, J.B.; Pelaez, C.E. Fuzzy logic prioritization of failures in a system failure mode, effects and criticality analysis. Reliab. Eng. Syst. Saf. 1995, 50, 203–213. [Google Scholar] [CrossRef]
- Ford, E.C.; Gaudette, R.; Myers, L.; Vanderver, B.; Engineer, L.; Zellars, R.; Song, D.Y.; Wong, J.; DeWeese, T.L. Evaluation of Safety in a Radiation Oncology Setting Using Failure Mode and Effects Analysis. Int. J. Radiat. Oncol. Biol. Phys. 2009, 74, 852–858. [Google Scholar] [CrossRef] [PubMed]
- Giardina, M.; Castiglia, F.; Tomarchio, E. Risk assessment of component failure modes and human errors using a new FMECA approach: Application in the safety analysis of HDR brachytherapy. J. Radiol. Prot. 2014, 34, 891–914. [Google Scholar] [CrossRef] [PubMed]
- Giardina, M.; Morale, M. Safety study of an LNG regasification plant using an FMECA and HAZOP integrated methodology. J. Loss Prev. Process Ind. 2015, 35, 35–45. [Google Scholar] [CrossRef]
- Buffa, P.; Giardina, M.; Prete, G.; De Ruvo, L. Fuzzy FMECA analysis of radioactive gas recovery system in the SPES experimental facility. Nucl. Eng. Technol. 2021, 53, 1464–1478. [Google Scholar] [CrossRef]
- Broggi, S.; Cantone, M.C.; Chiara, A.; Di Muzio, N.; Longobardi, B.; Mangili, P.; Veronese, I. Application of failure mode and effects analysis (FMEA) to pretreatment phases in tomotherapy. J. Appl. Clin. Med. Phys. 2013, 14, 265–277. [Google Scholar] [CrossRef] [PubMed]
- Broggi, S.; Cantone, M.C.; Chiara, A.; Di Muzio, N.; Longobardi, B.; Mangili, P.; Veronese, I. Application of failure mode and effect analysis to tomotherapy treatment delivery. Radioprotection 2015, 50, 171–175. [Google Scholar] [CrossRef][Green Version]
- Patient Safety Standards-Hospitals: Standard LD.5.2; Joint Commission on Accreditation of Healthcare Organizations, Ed.; Joint Commission Resources: Oakbrook Terrace, IL, USA, 2001; Available online: https://www.jointcommission.org/accreditation-and-certification/health-care-settings/hospital/learn/our-standards (accessed on 5 April 2022).
- López, P.O. Preventing Accidental Exposures from New External Beam Radiation Therapy Technologies; International Commission on Radiological Protection: Ottawa, ON, Canada, 2009; Volume 39, pp. 63–74. [Google Scholar] [CrossRef]
- Failure Mode and Effects Analysis in Health Care: Proactive Risk Reduction, 3rd ed.; Joint Commission Resources, Ed.; Joint Commission Resources: Oakbrook Terrace, IL, USA, 2010; ISBN 9781599404066. Available online: https://www.jointcommission.org/accreditation-and-certification/health-care-settings/hospital/learn/our-standards (accessed on 5 April 2022).
- Giardina, M.; Cantone, M.; Tomarchio, E.; Veronese, I. A Review of Healthcare Failure Mode and Effects Analysis (HFMEA) in Radiotherapy. Health Phys. 2016, 111, 317–326. [Google Scholar] [CrossRef] [PubMed]
- Abujudeh, H.H.; Kaewlai, R. Radiology Failure Mode and Effect Analysis: What Is It? Radiology 2009, 252, 544–550. [Google Scholar] [CrossRef] [PubMed]
- Younge, K.C.; Wang, Y.; Thompson, J.; Giovinazzo, J.; Finlay, M.; Sankreacha, R. Practical Implementation of Failure Mode and Effects Analysis for Safety and Efficiency in Stereotactic Radiosurgery. Int. J. Radiat. Oncol. Biol. Phys. 2015, 91, 1003–1008. [Google Scholar] [CrossRef] [PubMed]
- Schuller, B.W.; Burns, A.; Ceilley, E.A.; King, A.; Letourneau, J.; Markovic, A.; Sterkel, L.; Taplin, B.; Wanner, J.; Albert, J.M. Failure mode and effects analysis: A community practice perspective. J. Appl. Clin. Med. Phys. 2017, 18, 258–267. [Google Scholar] [CrossRef] [PubMed]
- Xu, A.Y.; Bhatnagar, J.; Bednarz, G.; Flickinger, J.; Arai, Y.; Vacsulka, J.; Feng, W.; Monaco, E.; Niranjan, A.; Lunsford, L.D.; et al. Failure modes and effects analysis (FMEA) for Gamma Knife radiosurgery. J. Appl. Clin. Med. Phys. 2017, 18, 152–168. [Google Scholar] [CrossRef] [PubMed]
- Nolan, D.P. Specialized Reviews—CHAZOP, EHAZOP, Bow-Tie Analysis, Layers of Protection Analysis, Safety Integrity Level, Fishbone Diagram, and Cyber Security Vulnerability Analysis. In Safety and Security Review for the Process Industries; Elsevier: Amsterdam, The Netherlands, 2015; pp. 17–27. [Google Scholar] [CrossRef]
- Zadeh, L.A. Toward a theory of fuzzy information granulation and its centrality in human reasoning and fuzzy logic. Fuzzy Sets Syst. 1997, 90, 111–127. [Google Scholar] [CrossRef]
- Zadeh, L.A. The concept of a linguistic variable and its application to approximate reasoning—III. Inf. Sci. 1975, 9, 43–80. [Google Scholar] [CrossRef]
- Zadeh, L.A. The concept of a linguistic variable and its application to approximate reasoning—II. Inf. Sci. 1975, 8, 301–357. [Google Scholar] [CrossRef]
- Zadeh, L.A. The concept of a linguistic variable and its application to approximate reasoning—I. Inf. Sci. 1975, 8, 199–249. [Google Scholar] [CrossRef]
- Shepherd, A. Hierarchical Task Analysis, 1st ed.; CRC Press: Boca Raton, FL, USA, 2000; ISBN 9780748408382. [Google Scholar]
- Schraagen, J.M.; Chipman, S.F.; Shalin, V.L. Cognitive Task Analysis, 1st ed.; Schraagen, J.M., Chipman, S.F., Shalin, V.L., Eds.; Psychology Press: Hove, UK, 2000; ISBN 9780805833836. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| O | D | S | Classic RPN | Classic-RPN Ranking | F-RPN (wO = 0.3, wD = 0.3, wS = 0.3) | F-RPN Ranking | F-RPN* (wO = 0.4, wD = 0.2, wS = 0.4) | F-RPN* Ranking | w-RPN (wO = 0.4, wD = 0.2, wS = 0.4) | w-RPN Ranking | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| FM1 | 4 | 7 | 7 | 196 | 1 | 451 | 3 | 487 | 2 | 5.60 | 2 |
| FM2 | 4 | 6 | 8 | 192 | 2 | 454 | 2 | 491 | 1 | 5.72 | 1 |
| FM3 | 4 | 9 | 5 | 180 | 3 | 450 | 4 | 442 | 8 | 5.14 | 5 |
| FM4 | 3 | 7 | 8 | 168 | 4 | 427 | 5 | 450 | 5 | 5.26 | 3 |
| FM5 | 3 | 6 | 8 | 144 | 5 | 426 | 6 | 444 | 7 | 5.10 | 7 |
| FM6 | 2 | 9 | 8 | 144 | 5 | 534 | 1 | 468 | 3 | 4.70 | 10 |
| FM7 | 4 | 5 | 7 | 140 | 7 | 351 | 10 | 447 | 6 | 5.23 | 4 |
| FM8 | 4 | 8 | 4 | 128 | 8 | 348 | 12 | 320 | 17 | 4.59 | 14 |
| FM9 | 3 | 5 | 8 | 120 | 9 | 420 | 8 | 423 | 9 | 4.92 | 9 |
| FM10 | 3 | 5 | 7 | 105 | 10 | 316 | 16 | 400 | 12 | 4.66 | 13 |
| FM11 | 3 | 7 | 5 | 105 | 10 | 307 | 19 | 307 | 19 | 4.36 | 16 |
| FM12 | 2 | 8 | 6 | 96 | 12 | 348 | 12 | 326 | 13 | 4.10 | 19 |
| FM13 | 3 | 4 | 8 | 96 | 12 | 400 | 9 | 403 | 11 | 4.70 | 10 |
| FM14 | 4 | 4 | 6 | 96 | 12 | 313 | 17 | 317 | 18 | 4.70 | 12 |
| FM15 | 4 | 3 | 8 | 96 | 12 | 350 | 11 | 451 | 4 | 4.98 | 8 |
| FM16 | 3 | 6 | 5 | 90 | 16 | 308 | 18 | 307 | 19 | 4.23 | 17 |
| FM17 | 2 | 9 | 5 | 90 | 16 | 424 | 7 | 325 | 14 | 3.90 | 21 |
| FM18 | 3 | 5 | 6 | 90 | 16 | 306 | 20 | 307 | 19 | 4.38 | 15 |
| FM19 | 2 | 7 | 6 | 84 | 19 | 323 | 15 | 323 | 16 | 3.99 | 20 |
| FM20 | 2 | 6 | 7 | 84 | 19 | 325 | 14 | 325 | 14 | 4.11 | 18 |
| FM21 | 7 | 2 | 6 | 84 | 19 | 300 | 21 | 413 | 10 | 5.12 | 6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giardina, M.; Tomarchio, E.; Buffa, P.; Palagonia, M.; Veronese, I.; Cantone, M.C. FMECA Application in Tomotherapy: Comparison between Classic and Fuzzy Methodologies. Environments 2022, 9, 50. https://doi.org/10.3390/environments9040050
Giardina M, Tomarchio E, Buffa P, Palagonia M, Veronese I, Cantone MC. FMECA Application in Tomotherapy: Comparison between Classic and Fuzzy Methodologies. Environments. 2022; 9(4):50. https://doi.org/10.3390/environments9040050
Chicago/Turabian StyleGiardina, Mariarosa, Elio Tomarchio, Pietro Buffa, Maurizio Palagonia, Ivan Veronese, and Marie Claire Cantone. 2022. "FMECA Application in Tomotherapy: Comparison between Classic and Fuzzy Methodologies" Environments 9, no. 4: 50. https://doi.org/10.3390/environments9040050
APA StyleGiardina, M., Tomarchio, E., Buffa, P., Palagonia, M., Veronese, I., & Cantone, M. C. (2022). FMECA Application in Tomotherapy: Comparison between Classic and Fuzzy Methodologies. Environments, 9(4), 50. https://doi.org/10.3390/environments9040050