

The Development and Reliability Testing of a Tool to Assess Women’s Perceptions and Avoidance of Endocrine Disruptors in Personal and Household Products

 ,
, 
Abstract
1. Introduction
2. Methods
2.1. Study Design
2.2. Development of the Questionnaire
2.3. Questionnaire Piloting and Testing
2.4. Data Analysis
3. Results and Discussion
3.1. Literature Review
3.2. Questionnaire Development
3.3. Pilot Sample Characteristics
3.4. Calculating Respondent Scores
3.5. Reliability Testing
4. Conclusions
Strengths and Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| Endocrine-Disrupting Chemicals (EDCs) | Endocrine-disrupting chemicals (EDCs) are natural or human-made chemicals that may mimic, block, or interfere with the body’s hormones |
References
- Khalid, M.; Abdollahi, M. Environmental Distribution of Personal Care Products and Their Effects on Human Health. Iran. J. Pharm. Res. 2021, 20, e124466. [Google Scholar] [CrossRef]
- Martín-Pozo, L.; Gómez-Regalado, M.; Moscoso-Ruiz, I.; Zafra-Gómez, A. Analytical methods for the determination of endocrine disrupting chemicals in cosmetics And personal care products: A review. Talanta 2021, 234, 122642. [Google Scholar] [CrossRef] [PubMed]
- Klančič, V.; Gobec, M.; Jakopin, Ž. Halogenated ingredients of household and personal care products as emerging endocrine disruptors. Chemosphere 2022, 303, 134824. [Google Scholar] [CrossRef] [PubMed]
- Malits, J.; Naidu, M.; Trasande, L. Exposure to endocrine disrupting chemicals in canada: Population-based estimates of disease burden and economic costs. Toxics 2022, 10, 146. [Google Scholar] [CrossRef]
- Lang, C.; Fisher, M.; Neisa, A.; MacKinnon, L.; Kuchta, S.; MacPherson, S.; Probert, A.; Arbuckle, T. Personal care product use in pregnancy and the postpartum period: Implications for exposure assessment. Int. J. Environ. Res. Public. Health 2016, 13, 105. [Google Scholar] [CrossRef]
- Land, K.L.; Ghuneim, S.M.; Williams, B.A.; Hannon, P.R. IMPACT OF REAL-LIFE ENVIRONMENTAL EXPOSURES ON REPRODUCTION: Phthalates disrupt female reproductive health: A call for enhanced investigation into mixtures. Reproduction 2025, 169, e240117. [Google Scholar] [CrossRef]
- Al-Saleh, I.; Al-Enazi, S.; Shinwari, N. Assessment of lead in cosmetic products. Regul. Toxicol. Pharmacol. 2009, 54, 105–113. [Google Scholar] [CrossRef]
- Garcia-Hidalgo, E.; von Goetz, N.; Siegrist, M.; Hungerbühler, K. Use-patterns of personal care and household cleaning products in switzerland. Food Chem. Toxicol. 2017, 99, 24–39. [Google Scholar] [CrossRef]
- ChemicalSafety Facts. Perchloroethylene—Chemical Safety Facts. 2024. Available online: https://www.chemicalsafetyfacts.org/chemicals/perchloroethylene/ (accessed on 3 May 2022).
- Liu, B.; Lu, X.; Jiang, A.; Lv, Y.; Zhang, H.; Xu, B. Influence of maternal endocrine disrupting chemicals exposure on adverse pregnancy outcomes: A systematic review and meta-analysis. Ecotoxicol. Environ. Saf. 2024, 270, 115851. [Google Scholar] [CrossRef]
- Ceballos, D.M.; Fellows, K.M.; Evans, A.E.; Janulewicz, P.A.; Lee, E.; Whittaker, S.G. Perchloroethylene and dry cleaning: It’s time to move the industry to safer alternatives. Front. Public. Health 2021, 9, 638082. [Google Scholar] [CrossRef]
- Pfadenhauer, L.; Burns, J.; Rohwer, A.; Rehfuess, E. Effectiveness of interventions to reduce exposure to lead through consumer products and drinking water: A systematic review. Environ. Res. 2016, 147, 525–536. [Google Scholar] [CrossRef] [PubMed]
- Wan, M.; Co, V.; El-Nezami, H. Endocrine disrupting chemicals and breast cancer: A systematic review of epidemiological studies. Crit. Rev. Food Sci. Nutr. 2021, 62, 6549–6576. [Google Scholar] [CrossRef] [PubMed]
- Abed, M.S.; Moosa, A.A.; Alzuhairi, M.A. Heavy metals in cosmetics and tattoos: A review of historical background, health impact, and regulatory limits. J. Hazard. Mater. Adv. 2024, 13, 100390. [Google Scholar] [CrossRef]
- Barton, C. Tetrachloroethylene. In Encyclopedia of Toxicology; Elsevier: Amsterdam, The Netherlands, 2014; pp. 498–502. [Google Scholar] [CrossRef]
- Aishwarya, S.; Vinodhini, V.; Renuka, P.; Saravanan, R.; Anuradha, M.; Gomathi, T.; Amuthavalli, V. Investigating the impact of endocrine-disrupting compounds on antepartum mental health at the nexus of genetic insights and maternal-fetal outcomes: A prospective study. Gen. Hosp. Psychiatry 2025, 94, 174–183. [Google Scholar] [CrossRef]
- Haggerty, D.K.; Upson, K.; Pacyga, D.C.; Franko, J.; Braun, J.M.; Strakovsky, R.S. Reproductive toxicology: Pregnancy exposure to endocrine disrupting chemicals: Implications for women’s health. Reproduction 2021, 162, F169–F180. [Google Scholar] [CrossRef]
- Barrett, E.S.; Sathyanarayana, S.; Janssen, S.; Redmon, J.; Nguyen, R.H.; Kobrosly, R.; Swan, S.H. Environmental health attitudes and behaviors: Findings from a large pregnancy cohort study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2014, 176, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Marie, C.; Cabut, S.; Vendittelli, F.; Sauvant-Rochat, M.-P. Changes in cosmetics use during pregnancy and risk perception by women. Int. J. Environ. Res. Public. Health 2016, 13, 383. [Google Scholar] [CrossRef]
- Rouillon, S.; El Ouazzani, H.; Rabouan, S.; Migeot, V.; Albouy-Llaty, M. Determinants of risk perception related to exposure to endocrine disruptors during pregnancy: A qualitative and quantitative study on french women. Int. J. Environ. Res. Public. Health 2018, 15, 2231. [Google Scholar] [CrossRef]
- Ricke, I.J.; Oglesby, A.; Lyden, G.R.; Barrett, E.S.; Moe, S.; Nguyen, R.H.N. Knowledge, Attitudes, and Behaviors Regarding Chemical Exposure among a Population Sample of Reproductive-Aged Women. Int. J. Environ. Res. Public. Health 2022, 19, 3015. [Google Scholar] [CrossRef]
- Zhao, Z.; Gong, Y.; Li, Y.; Zhang, L.; Sun, Y. Gender-related beliefs, norms, and the link with green consumption. Front. Psychol. 2021, 12, 710239. [Google Scholar] [CrossRef]
- Steinemann, A. Fragranced consumer products: Exposures and effects from emissions. Air Qual. Atmos. Health 2016, 9, 861–866. [Google Scholar] [CrossRef]
- FitzPatrick, M. Endocrine Disrupting Chemicals and Personal Care Products: Risk Awareness and Exposure Assessment for Women’s Reproductive Health. Ph.D. Thesis, Boston University, Boston, MA, USA, 2021. Available online: https://open.bu.edu/items/9b1d4020-eb0c-4fd9-9604-6c3be994f30f (accessed on 7 October 2022).
- Environmental Working Group (EWG). Ewg Verified®: Products for Your Health; EWG: Washington, DC, USA, 2025; Available online: https://www.ewg.org/ewgverified/ (accessed on 1 April 2025).
- Yuka. Yuka—The Mobile App That Scans Your Diet and Cosmetics; Yuka: Paris, France, 2024; Available online: https://yuka.io/en/ (accessed on 1 April 2025).
- Hawkins, M.; Elsworth, G.R.; Hoban, E.; Osborne, R.H. Questionnaire validation practice within a theoretical framework: A systematic descriptive literature review of health literacy assessments. BMJ Open 2020, 10, e035974. [Google Scholar] [CrossRef]
- Souza, A.; Alexandre, N.; Guirardello, E.; Souza, A.; Alexandre, N.; Guirardello, E. Propriedades psicométricas na avaliação de instrumentos: Avaliação da confiabilidade e da validade. Epidemiol. E Serviços De. Saúde 2017, 26, 649–659. [Google Scholar] [CrossRef]
- Rosenstock, I.M.; Strecher, V.J.; Becker, M.H. Social learning theory and the health belief model. Health Educ. Q. 1988, 15, 175–183. [Google Scholar] [CrossRef]
- Norman, P.; Conner, M. Health behavior. In Reference Module in Neuroscience and Biobehavioral Psychology; Elsevier: Amsterdam, The Netherlands, 2017. [Google Scholar] [CrossRef]
- Che, S.-R.; Barrett, E.S.; Velez, M.; Conn, K.; Heinert, S.; Qiu, X. Using the health belief model to illustrate factors that influence risk assessment during pregnancy and implications for prenatal education about endocrine disruptors. Policy Futures Educ. 2014, 12, 961–974. [Google Scholar] [CrossRef]
- Albadr, T.; Alfawzan, S.; Aljarba, B.; Alshehri, R.; Mahboub, S. Use of health belief model to explain the behaviour of following safety measures during the use of household chemical products among adult females in Riyadh. Int. J. Res. Med. Sci. 2020, 9, 9–14. [Google Scholar] [CrossRef]
- Chyung, S.; Roberts, K.; Swanson, I.; Hankinson, A. Evidence-based survey design:The use of a midpoint on the likert scale. Perform. Improv. 2017, 56, 15–23. [Google Scholar] [CrossRef]
- Statistics Canada. Fertility: Overview, 2012 to 2016. 2018. Available online: https://www150.statcan.gc.ca/n1/pub/91-209-x/2018001/article/54956-eng.htm (accessed on 4 September 2022).
- Mi, M.; Zhang, Y. Culturally competent library services and related factors among health sciences librarians: An exploratory study. J. Med. Libr. Assoc. 2017, 105, 132. [Google Scholar] [CrossRef]
- Joo, S.; Kim, S.; Kim, Y. An exploratory study of health scientists’ data reuse behaviors. Aslib J. Inf. Manag. 2017, 69, 389–407. [Google Scholar] [CrossRef]
- Lally, M.; Valentine-French, S. Emerging and Early Adulthood—Parenting and Family Diversity Issues; Iowa State University: Ames, IA, ISA, 2020; Available online: https://iastate.pressbooks.pub/parentingfamilydiversity/chapter/early-adulthood/ (accessed on 14 May 2023).
- Statistics Canada. Low Income Cut-Offs. Government of Canada. Retrieved 2023. 2021. Available online: https://www.canada.ca/en/employment-social-development/services/foreign-workers/caregiver/financial-ability.html (accessed on 14 May 2023).
- Li, P.; Stuart, E.A.; Allison, D.B. Multiple imputation. JAMA 2015, 314, 1966. [Google Scholar] [CrossRef]
- Sullivan, G.M.; Artino, A.R. Analyzing and interpreting data from likert-type scales. J. Grad. Med. Educ. 2013, 5, 541–542. [Google Scholar] [CrossRef]
- Zhan, W.; Yang, H.; Zhang, J.; Chen, Q. Association between co-exposure to phenols and phthalates mixture and infertility risk in women. Environ. Res. 2022, 215, 114244. [Google Scholar] [CrossRef]
- Deierlein, A.L.; Grayon, A.R.; Zhu, X.; Sun, Y.; Liu, X.; Kohlasch, K.; Stein, C.R. Personal care and household cleaning product use among pregnant women and new Mothers during the COVID-19 pandemic. Int. J. Environ. Res. Public. Health 2022, 19, 5645. [Google Scholar] [CrossRef]
- Ministry of Finance. Educational Attainment. 2022. Available online: https://www150.statcan.gc.ca/n1/daily-quotidien/211004/dq211004c-eng.htm (accessed on 5 May 2023).
- Miral, M.T.; Koç, E. Awareness and attitudes of pregnant women regarding endocrine disruptors. Afr. J. Reprod. Health 2025, 29, 59–69. [Google Scholar] [CrossRef]
- Trifunovski, A.; Rotondi, N.K.; Abbass-Dick, J.; Barakat, C. Hidden Hazards: Knowledge, Health Risk Perceptions, Beliefs and Avoidance Behaviour of Women in Relation to Toxic Chemicals Commonly Found in Personal Care and Household Products. Toxics 2025, in press.
- Lu, X.; Hisada, A.; Anai, A.; Nakashita, C.; Masuda, S.; Fujiwara, Y.; Kunugita, N.; Katoh, T. Study of the correlation between multiple chemical sensitivity and personality using the quick environmental exposure sensitivity inventory questionnaire and the temperament and character inventory. J. Occup. Environ. Med. 2020, 62, e348–e354. [Google Scholar] [CrossRef]
- Peris, R. Multiple Chemical Sensitivity (MCS)—Aseq-Ehaq. ASEQ-EHAQ. 8 April 2021. Available online: https://aseq-ehaq.ca/en/multiple-chemical-sensitivity-mcs/ (accessed on 4 October 2024).
- Živančević, K.; Marić, Đ.; Manić, L.; Bonderović, V.; Živanović, J.; Djukic-Cosic, D.; Bulat, Z.; Antonijevic, B.; Vilendecic, Z.; Ilić, S.; et al. Perceptions and awareness of endocrine disruptors among mothers in serbia and health implications. Endocr. Connect. 2025, 14, e240678. [Google Scholar] [CrossRef]
- The International Fragrance Association (IFRA). n.d. Home. Available online: https://ifrafragrance.org/ (accessed on 2 April 2025).
- IFRA. IFRA Position Statement on Diethyl Phthalate (DEP) [PDF]. 2005. Available online: https://www.sunseye.com/wp-content/uploads/2018/05/IFRA-position-on-DEP.pdf (accessed on 2 April 2025).
- Good Authority. How the Media Put Bpa on the Agenda in the States. 2013. Available online: https://goodauthority.org/news/how-the-media-put-bpa-on-the-agenda-in-the-states/?utm (accessed on 3 April 2025).
- Fong, D.; Ho, S.Y.; Lam, T.H. Evaluation of internal reliability in the presence of inconsistent responses. Health Qual. Life Outcomes 2010, 8, 27. [Google Scholar] [CrossRef]
- Tavakol, M.; Dennick, R. Making sense of cronbach. Int. J. Med. Educ. 2011, 2, 53–55. [Google Scholar] [CrossRef]
- Taber, K.S. The Use of Cronbach’s Alpha When Developing and Reporting Research Instruments in Science Education. Res. Sci. Educ. 2018, 48, 1273–1296. [Google Scholar] [CrossRef]
- Preston, C.C.; Colman, A.M. Optimal number of response categories in rating scales: Reliability, validity, discriminating power, and respondent preferences. Acta Psychol. 2000, 104, 1–15. [Google Scholar] [CrossRef]
- Price, P.C.; Jhangiani, R.; Chiang, C.A. Reliability and Validity of Measurement. In Research Methods in Psychology, 2nd ed.; BC Campus: Victoria, BC, Canada, 2020; Available online: https://opentextbc.ca/researchmethods/chapter/reliability-and-validity-of-measurement/ (accessed on 27 May 2024).
- Austin, P.C.; White, I.R.; Lee, D.S.; van Buuren, S. Missing data in clinical research: A tutorial on multiple imputation. Can. J. Cardiol. 2021, 37, 1322–1331. [Google Scholar] [CrossRef]

{kind=link}
| Assessed Construct | Scale Item | Reference |
|---|---|---|
| Risk perceptions/Attitudes | 1. Chemicals in the environment can pose health risks 2. Do you think there is a risk related to exposure to these chemical molecules for yourself? And for your baby? 3. Do you think that exposure to chemicals presents a risk to the health of pregnant women and their unborn babies? | [18] [19] [20] [21] |
| Knowledge (product safety) | 1. Do you want to learn more about what makes products safe? | [24] |
| Behavior | 1. I try to Buy “Eco-Friendly”, and “Chemical-Free” personal care products 2. I try to Buy “Eco-Friendly”, and “Chemical-Free” Household Products 3. When I buy bath soap, cosmetics, and toiletries, I try to make sure they are “Eco-Friendly, Chemical-Free, or Environmentally Friendly” | [18] [41] |
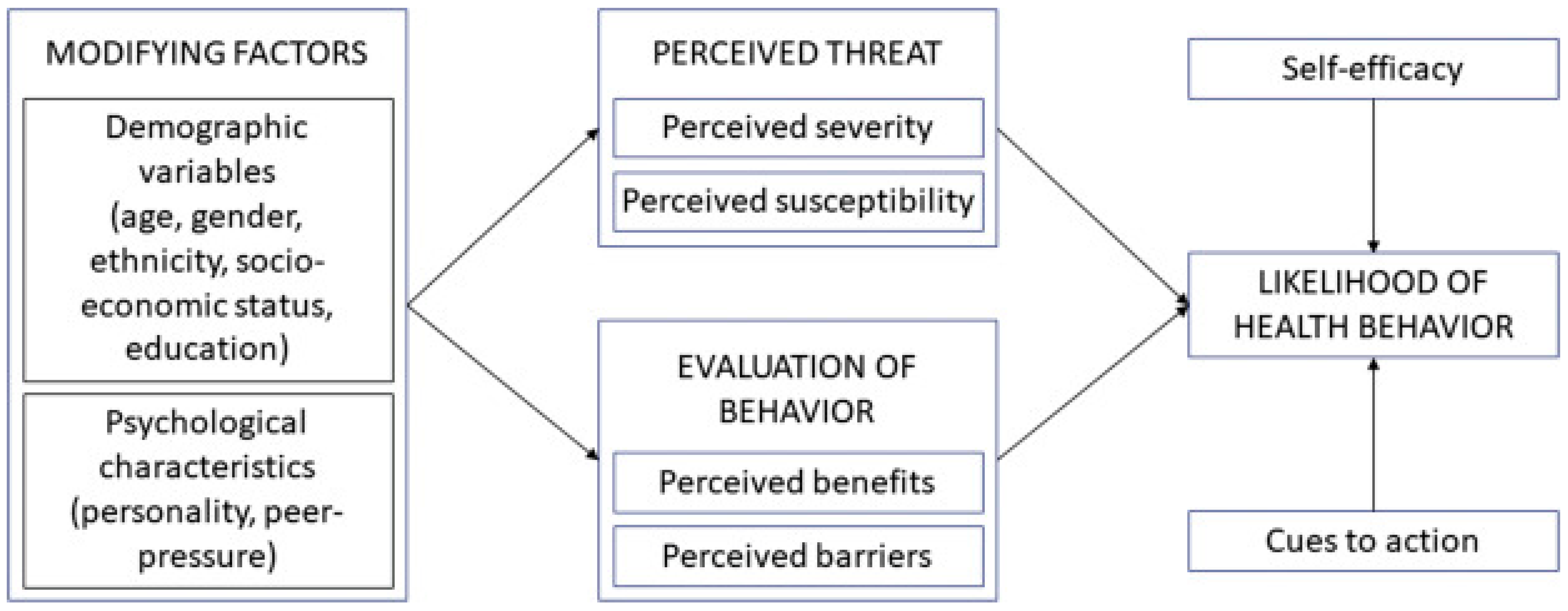
| Modifying Factors Demographic variables
|
| Perceived Threat Perceived Susceptibility (Beliefs)
|
| Evaluation of Behavior Perceived barriers and benefits (Knowledge—access to resources)
|
| Behavior Purchasing behaviors (Avoidance behaviour)
|
| Demographic Factors | N% |
|---|---|
| Age | |
| 18–25 | 114 (57) |
| 26–35 | 76 (38) |
| Prefer not to say | 10 (5) |
| Education | |
| High school completed | 58 (29) |
| Post-secondary completed | 133 (66) |
| Prefer not to say | 9 (5) |
| Annual household income | |
| Below or equal to Low-income-cut-off | 42 (21) |
| Above Low-income-cut-off | 131 (65) |
| Prefer not to say | 27 (13) |
| Ethnicity | |
| White | 84 (42) |
| South Asian | 34 (17) |
| Chinese | 21 (11) |
| African Descent | 15 (8) |
| West Asian | 9 (5) |
| Mixed race | 12 (6) |
| South East Asian | 10 (5) |
| First Nation | 4 (2) |
| Other | 4 (2) |
| Birthplace | |
| Canada | 157 (79) |
| Other | 38 (19) |
| Prefer not to say | 5 (2) |
| Diagnosed with chemical sensitivity | |
| Yes | 20 (10) |
| No | 153 (76) |
| Don’t know | 22 (11) |
| Prefer not to say | 5 (3) |
| Pregnant | |
| Yes | 3 (1.5) |
| No | 193 (96.5) |
| Prefer not to say | 1 (0.5) |
| Attempting pregnancy | |
| Yes | 9 (5) |
| No | 183 (92) |
| Prefer not to say | 2 (1) |
| Parent to a child under the age of 18 years old | |
| Yes | 26 (13) |
| No | 171 (86) |
| Prefer not to say | 3 (1) |
| Toxic Chemical | Mean (SD); Median | |||
|---|---|---|---|---|
| Health Risk Perceptions (7–35) | Beliefs (5–25) | Knowledge (Access to Resources) (6–30) | Avoidance Behavior (6–30) | |
| Lead (n = 161) | 29 (4); 28 | 19 (4); 20 | 23 (4); 23 | 19 (7); 18 |
| Parabens (n = 44) | 27 (5); 28 | 17 (4); 17 | 23 (4); 23 | 21 (6); 21 |
| BPA (n = 76) | 29 (5); 29 | 20 (3); 20 | 24 (4); 24 | 23 (6); 24 |
| Phthalates (n = 55) | 28 (5); 28 | 18 (4); 18 | 23 (4); 24 | 22 (6); 22 |
| Triclosan (n = 14) | 31 (6); 32 | 22 (3); 23 | 26 (4); 25 | 24 (8); 30 |
| PERC (n = 12) | 32 (4); 35 | 22 (4); 23 | 25 (5); 25 | 23 (6); 24 |
| EDC | Risk Perceptions (7 Items) | Belief (5 Items) | Knowledge (Resource Access) (6 Items) | Avoidance Behavior (6 Items) |
|---|---|---|---|---|
| Parabens | 0.87 | 0.82 | 0.77 | 0.93 |
| Lead | 0.87 | 0.76 | 0.81 | 0.95 |
| Phthalates | 0.92 | 0.82 | 0.81 | 0.96 |
| BPA | 0.93 | 0.83 | 0.93 | 0.95 |
| Triclosan | 0.90 | 0.96 | 0.87 | 0.98 |
| PERC | 0.87 | 0.83 | 0.93 | 0.97 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trifunovski, A.; Rotondi, N.K.; Abbass-Dick, J.; Al Ghali, R.; Barakat, C. The Development and Reliability Testing of a Tool to Assess Women’s Perceptions and Avoidance of Endocrine Disruptors in Personal and Household Products. Environments 2025, 12, 138. https://doi.org/10.3390/environments12050138
Trifunovski A, Rotondi NK, Abbass-Dick J, Al Ghali R, Barakat C. The Development and Reliability Testing of a Tool to Assess Women’s Perceptions and Avoidance of Endocrine Disruptors in Personal and Household Products. Environments. 2025; 12(5):138. https://doi.org/10.3390/environments12050138
Chicago/Turabian StyleTrifunovski, Adrianna, Nooshin Khobzi Rotondi, Jennifer Abbass-Dick, Rola Al Ghali, and Caroline Barakat. 2025. "The Development and Reliability Testing of a Tool to Assess Women’s Perceptions and Avoidance of Endocrine Disruptors in Personal and Household Products" Environments 12, no. 5: 138. https://doi.org/10.3390/environments12050138
APA StyleTrifunovski, A., Rotondi, N. K., Abbass-Dick, J., Al Ghali, R., & Barakat, C. (2025). The Development and Reliability Testing of a Tool to Assess Women’s Perceptions and Avoidance of Endocrine Disruptors in Personal and Household Products. Environments, 12(5), 138. https://doi.org/10.3390/environments12050138