A Systematic Review on the Possible Relationship Between Bilingualism, Cognitive Decline, and the Onset of Dementia

 , ,
, , 

Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategies
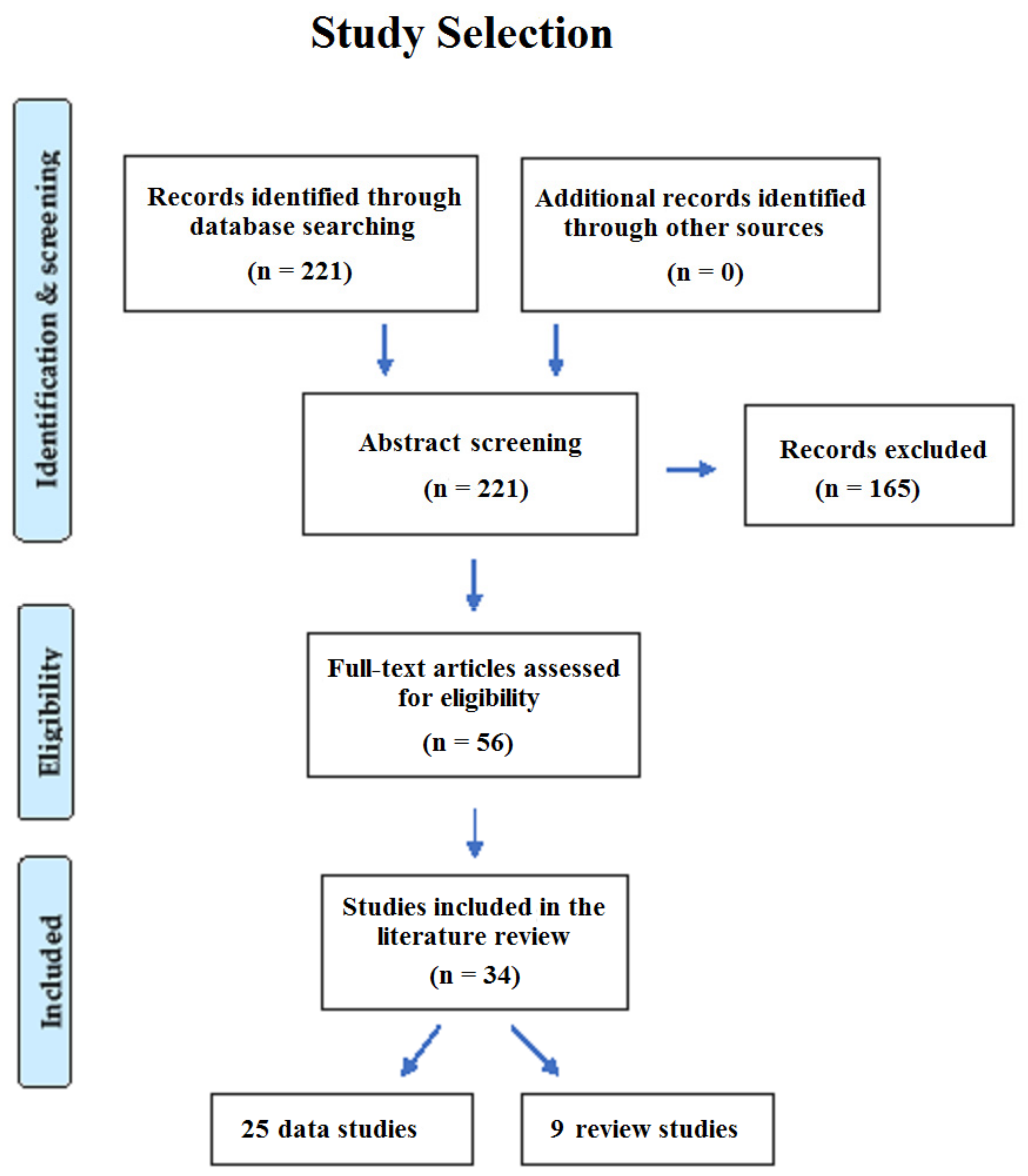
2.2. Study Selection and Data Extraction
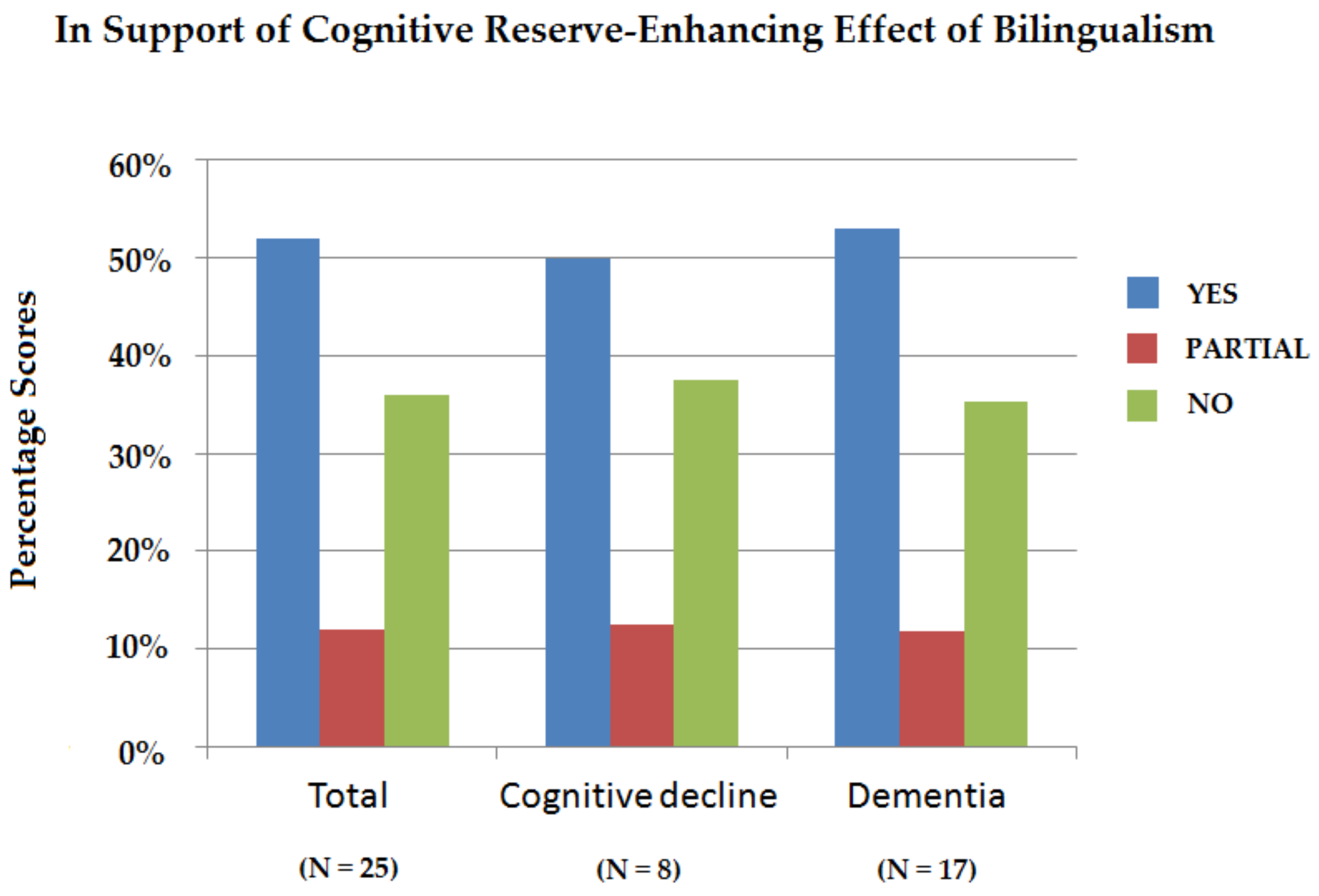
3. Results
3.1. Protection against Cognitive Decline
3.2. Delaying the Onset of Dementia
4. Discussion
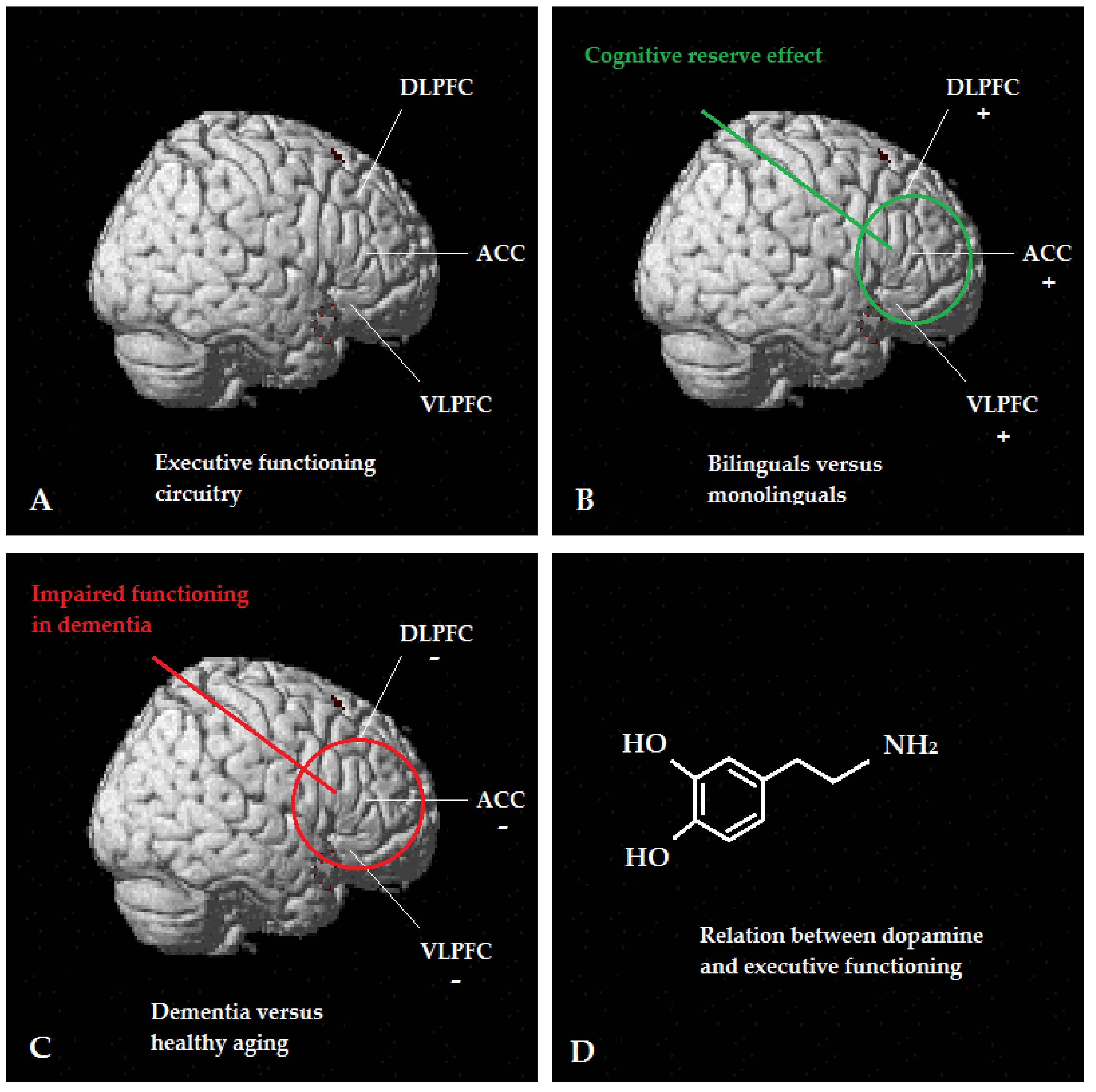
4.1. Neuroscience Research
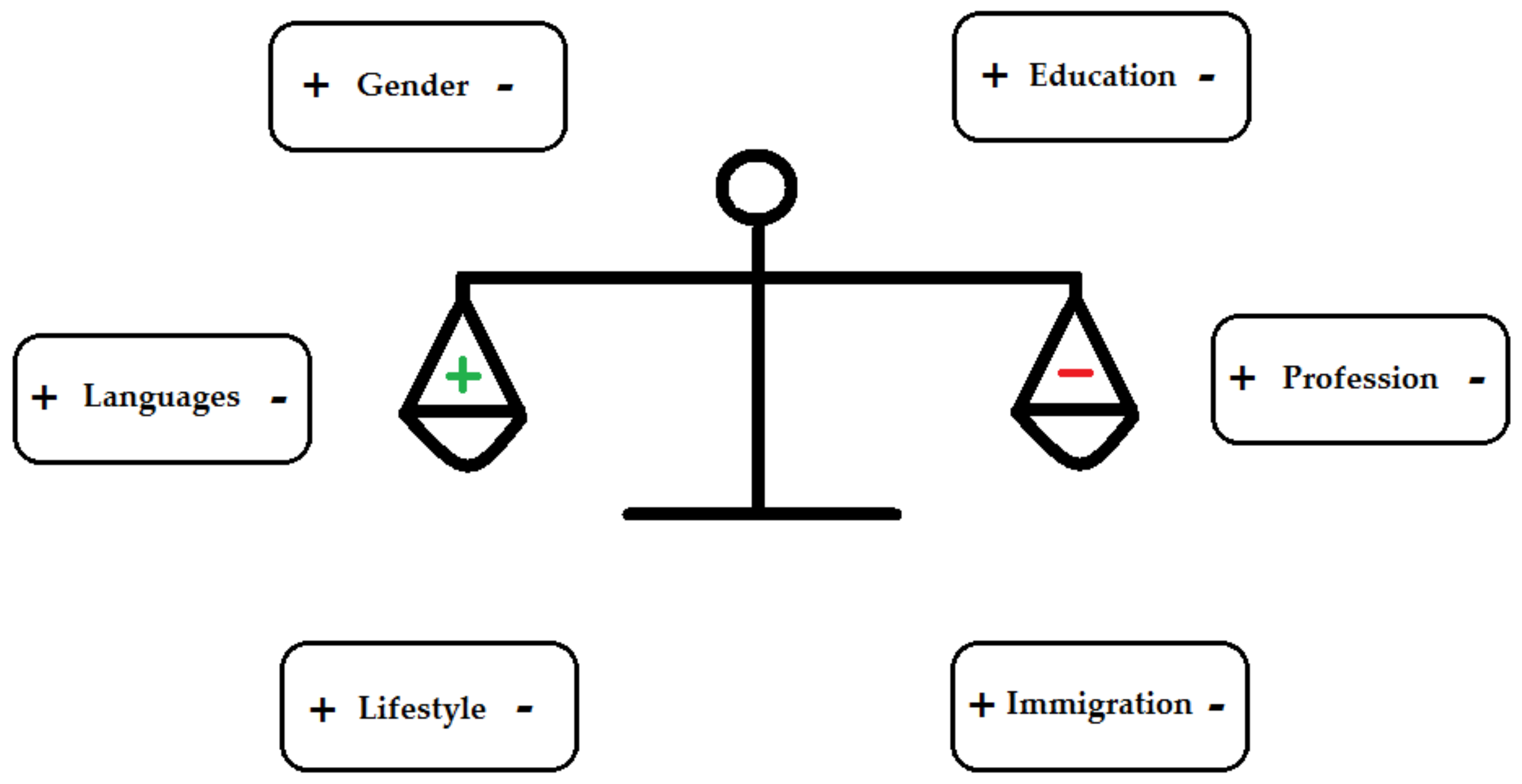
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Mertz, L. The coming gray tide: Wanted: Health innovations for an increasingly older population. IEEE Pulse 2017, 8, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Corrada, M.M.; Brookmeyer, R.; Paganini-Hill, A.; Berlau, D.; Kawas, C.H. Dementia incidence continues to increase with age in the oldest old the 90+ study. Ann. Neurol. 2010, 67, 114–121. [Google Scholar] [CrossRef] [PubMed]
- Prince, M.J.; Wimo, A.G.M.; Ali, G.C.; Wu, Y.T.; Prina, M. World Alzheimer Report 2015: The Global Impact of Dementia. An Analysis of Prevalence, Incidence, Cost, and Trends; Alzheimer’s Disease International: London, UK, 2015. [Google Scholar]
- Norton, S.; Matthews, F.E.; Barnes, D.E.; Yaffe, K.; Brayne, C. Potential for primary prevention of Alzheimer’s disease: An analysis of population-based data. Lancet Neurol. 2014, 13, 788–794. [Google Scholar] [CrossRef]
- Cosentino, S.; Stern, Y. Consideration of cognitive reserve. In Handbook on the Neuropsychology of Aging and Dementia; Ravdin, L.D., Katzen, H.L., Eds.; Springer: New York, NY, USA, 2013; pp. 11–23. ISBN 9781461491408. [Google Scholar]
- Stern, Y. What is cognitive reserve? Theory and research application of the reserve concept. J. Int. Neuropsychol. Soc. 2002, 8, 448–460. [Google Scholar] [CrossRef] [PubMed]
- Stern, Y. Cognitive reserve. Neuropsychologia 2009, 47, 2015–2028. [Google Scholar] [CrossRef] [PubMed]
- Barulli, D.; Stern, Y. Efficiency, capacity, compensation, maintenance, plasticity: Emerging concepts in cognitive reserve. Trends Cogn. Sci. 2013, 17, 502–509. [Google Scholar] [CrossRef] [PubMed]
- Chodosh, J.; Reuben, D.B.; Albert, M.S.; Seeman, T.E. Predicting cognitive impairment in high-functioning community-dwelling older persons: MacArthur Studies of Successful Aging. J. Am. Geriatr. Soc. 2002, 50, 1051–1060. [Google Scholar] [CrossRef] [PubMed]
- Schooler, C.; Mulatu, M.S.; Oates, G. The continuing effects of substantively complex work on the intellectual functioning of older workers. Psychol. Aging 1999, 14, 483–506. [Google Scholar] [CrossRef]
- Opdebeeck, C.; Martyr, A.; Clare, L. Cognitive reserve and cognitive function in healthy older people: A meta-analysis. Neuropsychol. Dev. Cogn. B Aging Neuropsychol. Cogn. 2016, 23, 40–60. [Google Scholar] [CrossRef]
- Prince, M.; Acosta, D.; Ferri, C.P.; Guerra, M.; Huang, Y.; Rodriguez, J.J.L.; Salas, A.; Sosa, A.L.; Williams, J.D.; Dewey, M.E.; et al. Dementia incidence and mortality in middle-income countries, and associations with indicators of cognitive reserve: A 10/66 Dementia Research Group population-based cohort study. Lancet 2012, 380, 50–58. [Google Scholar] [CrossRef]
- Bialystok, E.; Craik, F.I.; Freedman, M. Bilingualism as a protection against the onset of symptoms of dementia. Neuropsychologia 2007, 45, 459–464. [Google Scholar] [CrossRef] [PubMed]
- Ansaldo, A.I.; Marcotte, K.; Scherer, L.; Raboyeau, G. Language therapy and bilingual aphasia: Clinical implications of psycholinguistic and neuroimaging research. J. Neurolinguistics 2008, 21, 539–557. [Google Scholar] [CrossRef]
- Janson, T. Speak: A Short History of Languages; Oxford University Press: Oxford, UK, 2002; pp. 1–316. ISBN 978-0198299783. [Google Scholar]
- Van den Noort, M.; Struys, E.; Bosch, P.; Jaswetz, L.; Perriard, B.; Yeo, S.; Barisch, P.; Vermeire, K.; Lee, S.H.; Lim, S. Does the bilingual advantage in cognitive control exist and if so, what are its modulating factors? A systematic review. Behav. Sci. 2019, 9, 27. [Google Scholar] [CrossRef] [PubMed]
- Bialystok, E. Cognitive complexity and attentional control in the bilingual mind. Child Dev. 1999, 70, 636–644. [Google Scholar] [CrossRef]
- Colzato, L.S.; Bajo, M.T.; van den Wildenberg, W.; Paolieri, D.; Nieuwenhuis, S.; La Heij, W.; Hommel, B. How does bilingualism improve executive control? A comparison of active and reactive inhibition mechanisms. J. Exp. Psychol. Learn. Mem. Cogn. 2008, 34, 302–312. [Google Scholar] [CrossRef] [PubMed]
- Bialystok, E.; Craik, F.I.M.; Klein, R.; Viswanathan, M. Bilingualism, aging, and cognitive control: Evidence from the Simon task. Psychol. Aging 2004, 19, 290–303. [Google Scholar] [CrossRef]
- Costa, A.; Hernández, M.; Sebastián-Gallés, N. Bilingualism aids conflict resolution: Evidence from the ANT task. Cognition 2008, 106, 59–86. [Google Scholar] [CrossRef] [PubMed]
- Collette, F.; Hogge, M.; Salmon, E.; Van der Linden, M. Exploration of the neural substrates of executive functioning by functional neuroimaging. Neuroscience 2006, 139, 209–221. [Google Scholar] [CrossRef]
- Miyake, A.; Friedman, N.P.; Emerson, M.J.; Witzki, A.H.; Howerter, A.; Wager, T.D. The unity and diversity of executive functions and their contribution to complex “frontal lobe” tasks: A latent variable analysis. Cogn. Psychol. 2000, 41, 49–100. [Google Scholar] [CrossRef] [PubMed]
- Kenny, E.R.; Burton, E.J.; O’Brien, J.T. A volumetric magnetic resonance imaging study of entorhinal cortex volume in dementia with lewy bodies. A comparison with Alzheimer’s disease and Parkinson’s disease with and without dementia. Dement. Geriatr. Cogn. Disord. 2008, 26, 218–225. [Google Scholar] [CrossRef]
- Firbank, M.J.; Blamire, A.M.; Teodorczuk, A.; Teper, E.; Burton, E.J.; Mitra, D.; O’Brien, J.T. High resolution imaging of the medial temporal lobe in Alzheimer’s disease and dementia with Lewy bodies. J. Alzheimer’s Dis. 2010, 21, 1129–1140. [Google Scholar] [CrossRef]
- Kenny, E.R.; Blamire, A.M.; Firbank, M.J.; O’Brien, J.T. Functional connectivity in cortical regions in dementia with Lewy bodies and Alzheimer’s disease. Brain 2012, 135, 569–581. [Google Scholar] [CrossRef] [PubMed]
- Bakkour, A.; Morris, J.C.; Wolk, D.A.; Dickerson, B.C. The effects of aging and Alzheimer’s disease on cerebral cortical anatomy: Specificity and differential relationships with cognition. Neuroimage 2013, 76, 332–344. [Google Scholar] [CrossRef] [PubMed]
- Jawabri, K.H.; Sharma, S. Physiology, Cerebral Cortex Functions; StatPearls Publishing: Treasure Island, FL, USA, 2019. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, eb2535. [Google Scholar] [CrossRef] [PubMed]
- Kavé, G.; Eyal, N.; Shorek, A.; Cohen-Mansfield, J. Multilingualism and cognitive state in the oldest old. Psychol. Aging 2008, 23, 70–78. [Google Scholar] [CrossRef]
- Chertkow, H.; Whitehead, V.; Phillips, N.; Wolfson, C.; Atherton, J.; Bergman, H. Multilingualism (but not always bilingualism) delays the onset of Alzheimer disease: Evidence from a bilingual community. Alzheimer Dis. Assoc. Disord. 2010, 24, 118–125. [Google Scholar] [CrossRef] [PubMed]
- Craik, F.I.; Bialystok, E.; Freedman, M. Delaying the onset of Alzheimer disease: Bilingualism as a form of cognitive reserve. Neurology 2010, 75, 1726–1729. [Google Scholar] [CrossRef]
- Crane, P.K.; Gruhl, J.C.; Erosheva, E.A.; Gibbons, L.E.; McCurry, S.M.; Rhoads, K.; Nguyen, V.; Arani, K.; Masaki, K.; White, L. Use of spoken and written Japanese did not protect Japanese-American men from cognitive decline in late life. J. Gerontol. B Psychol. Sci. Soc. Sci. 2010, 65, 654–666. [Google Scholar] [CrossRef]
- Gollan, T.H.; Salmon, D.P.; Montoya, R.I.; Galasko, D.R. Degree of bilingualism predicts age of diagnosis of Alzheimer’s disease in low-education but not in highly educated Hispanics. Neuropsychologia 2011, 49, 3826–3830. [Google Scholar] [CrossRef]
- Kousaie, S.; Phillips, N.A. Ageing and bilingualism: Absence of a “bilingual advantage” in Stroop interference in a nonimmigrant sample. Q. J. Exp. Psychol. 2012, 65, 356–369. [Google Scholar] [CrossRef]
- Sanders, A.E.; Hall, C.B.; Katz, M.J.; Lipton, R.B. Non-native language use and risk of incident dementia in the elderly. J. Alzheimer’s Dis. 2012, 29, 99–108. [Google Scholar] [CrossRef] [PubMed]
- Schweizer, T.A.; Ware, J.; Fischer, C.E.; Craik, F.I.; Bialystok, E. Bilingualism as a contributor to cognitive reserve: Evidence from brain atrophy in Alzheimer’s disease. Cortex 2012, 48, 991–996. [Google Scholar] [CrossRef] [PubMed]
- Alladi, S.; Bak, T.H.; Duggirala, V.; Surampudi, B.; Shailaja, M.; Shukla, A.K.; Chaudhuri, J.R.; Kaul, S. Bilingualism delays age at onset of dementia, independent of education and immigration status. Neurology 2013, 81, 1938–1944. [Google Scholar] [CrossRef] [PubMed]
- Bak, T.H.; Nissan, J.J.; Allerhand, M.M.; Deary, I.J. Does bilingualism influence cognitive aging? Ann. Neurol. 2014, 75, 959–963. [Google Scholar] [CrossRef] [PubMed]
- Bialystok, E.; Craik, F.I.M.; Binns, M.A.; Ossher, L.; Freedman, M. Effects of bilingualism on the age of onset and progression of MCI and AD: Evidence from executive function tests. Neuropsychology 2014, 28, 290–304. [Google Scholar] [CrossRef] [PubMed]
- Yeung, C.M.; St John, P.D.; Menec, V.; Tyas, S.L. Is bilingualism associated with a lower risk of dementia in community-living older adults? Cross-sectional and prospective analyses. Alzheimer Dis. Assoc. Disord. 2014, 28, 326–332. [Google Scholar] [CrossRef] [PubMed]
- Zahodne, L.B.; Schofield, P.W.; Farrell, M.T.; Stern, Y.; Manly, J.J. Bilingualism does not alter cognitive decline or dementia risk among Spanish-speaking immigrants. Neuropsychology 2014, 28, 238–246. [Google Scholar] [CrossRef] [PubMed]
- Kowoll, M.E.; Degen, C.; Gladis, S.; Schröder, J. Neuropsychological profiles and verbal abilities in lifelong bilinguals with mild cognitive impairment and Alzheimer’s disease. J. Alzheimers. Dis. 2015, 45, 1257–1268. [Google Scholar] [CrossRef] [PubMed]
- Lawton, D.M.; Gasquoine, P.Q.; Weimer, A.A. Age of dementia diagnosis in community dwelling bilingual and monolingual Hispanic Americans. Cortex 2015, 66, 141–145. [Google Scholar] [CrossRef]
- Woumans, E.; Santens, P.; Sieben, A.; Versijpt, J.; Stevens, M.; Duyck, W. Bilingualism delays clinical manifestation of Alzheimer’s disease. Biling. Lang. Cogn. 2015, 18, 568–574. [Google Scholar] [CrossRef]
- Clare, L.; Whitaker, C.J.; Craik, F.I.; Bialystok, E.; Martyr, A.; Martin-Forbes, P.A.; Bastable, A.J.; Pye, K.L.; Quinn, C.; Thomas, E.M.; et al. Bilingualism, executive control, and age at diagnosis among people with early-stage Alzheimer’s disease in Wales. J. Neuropsychol. 2016, 10, 163–185. [Google Scholar] [CrossRef] [PubMed]
- Ihle, A.; Oris, M.; Fagot, D.; Kliegel, M. The relation of the number of languages spoken to performance in different cognitive abilities in old age. J. Clin. Exp. Neuropsychol. 2016, 38, 1103–1114. [Google Scholar] [CrossRef] [PubMed]
- Kowoll, M.E.; Degen, C.; Gorenc, L.; Küntzelmann, A.; Fellhauer, I.; Giesel, F.; Haberkorn, U.; Schröder, J. Bilingualism as a contributor to cognitive reserve? Evidence from cerebral glucose metabolism in mild cognitive impairment and Alzheimer’s disease. Front. Psychiatry 2016, 7, 62. [Google Scholar] [CrossRef] [PubMed]
- Estanga, A.; Ecay-Torres, M.; Ibañez, A.; Izagirre, A.; Villanua, J.; Garcia-Sebastian, M.; Iglesias Gaspar, M.T.; Otaegui-Arrazola, A.; Iriondo, A.; Clerigue, M.; et al. Beneficial effect of bilingualism on Alzheimer’s disease CSF biomarkers and cognition. Neurobiol. Aging 2017, 50, 144–151. [Google Scholar] [CrossRef] [PubMed]
- Perani, D.; Farsad, M.; Ballarini, T.; Lubian, F.; Malpetti, M.; Fracchetti, A.; Magnani, G.; March, A.; Abutalebi, J. The impact of bilingualism on brain reserve and metabolic connectivity in Alzheimer’s dementia. Proc. Natl. Acad. Sci. USA 2017, 114, 1690–1695. [Google Scholar] [CrossRef] [PubMed]
- Anderson, J.A.E.; Grundy, J.G.; De Frutos, J.; Barker, R.M.; Grady, C.; Bialystok, E. Effects of bilingualism on white matter integrity in older adults. Neuroimage 2018, 167, 143–150. [Google Scholar] [CrossRef] [PubMed]
- Mukadam, N.; Jichi, F.; Green, D.; Livingston, G. The relationship of bilingualism to cognitive decline: The Australian Longitudinal Study of Ageing. Int. J. Geriatr. Psychiatry 2018, 33, e249–e256. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.; Wu, Q.; Su, F.; Fang, Y.; Zeng, J.; Pei, Z. The protective effect of Cantonese/Mandarin bilingualism on the onset of Alzheimer disease. Dement. Geriatr. Cogn. Disord. 2018, 45, 210–219. [Google Scholar] [CrossRef]
- Bialystok, E.; Abutalebi, J.; Bak, T.H.; Burke, D.M.; Kroll, J.F. Aging in two languages: Implications for public health. Ageing Res. Rev. 2016, 27, 56–60. [Google Scholar] [CrossRef]
- Quinteros Baumgart, C.; Billick, S.B. Positive cognitive effects of bilingualism and multilingualism on cerebral function: A review. Psychiatr. Q. 2018, 89, 273–283. [Google Scholar] [CrossRef]
- Freedman, M.; Alladi, S.; Chertkow, H.; Bialystok, E.; Craik, F.I.; Phillips, N.A.; Duggirala, V.; Raju, S.B.; Bak, T.H. Delaying onset of dementia: Are two languages enough? Behav. Neurol. 2014, 2014, 808137. [Google Scholar] [CrossRef] [PubMed]
- Gold, B.T. Lifelong bilingualism and neural reserve against Alzheimer’s disease: A review of findings and potential mechanisms. Behav. Brain Res. 2015, 281, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Guzmán-Vélez, E.; Tranel, D. Does bilingualism contribute to cognitive reserve? Cognitive and neural perspectives. Neuropsychology 2015, 29, 139–150. [Google Scholar] [CrossRef] [PubMed]
- Perani, D.; Abutalebi, J. Bilingualism, dementia, cognitive and neural reserve. Curr. Opin. Neurol. 2015, 28, 618–625. [Google Scholar] [CrossRef] [PubMed]
- Calvo, N.; García, A.M.; Manoiloff, L.; Ibáñez, A. Bilingualism and cognitive reserve: A critical overview and a plea for methodological innovations. Front. Aging Neurosci. 2016, 7, 249. [Google Scholar] [CrossRef] [PubMed]
- Klimova, B.; Valis, M.; Kuca, K. Bilingualism as a strategy to delay the onset of Alzheimer’s disease. Clin. Interv. Aging 2017, 12, 1731–1737. [Google Scholar] [CrossRef] [PubMed]
- Mukadam, N.; Sommerlad, A.; Livingston, G. The relationship of bilingualism compared to monolingualism to the risk of cognitive decline or dementia: A systematic review and meta-analysis. J. Alzheimer’s Dis. 2017, 58, 45–54. [Google Scholar] [CrossRef]
- Katzman, R.; Brown, T.; Fuld, P.; Peck, A.; Schechter, R.; Schimmel, H. Validation of a short Orientation-Memory-Concentration Test of cognitive impairment. Am. J. Psychiatry 1983, 140, 734–739. [Google Scholar]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Wechsler, D. WAIS-III Administration and Scoring Manual; The Psychological Association: San Antonio, TX, USA, 1997. [Google Scholar]
- Wechsler, D. Wechsler Memory Scale-Third Edition Administration and Scoring Manual; Pearson Assessments: San Antonio, TX, USA, 1997. [Google Scholar]
- Nelson, H.; Willison, J. The National Adult Reading Test (NART); NFER-Nelson: Windsor, UK, 1991. [Google Scholar]
- Paap, K.R.; Johnson, H.A.; Sawi, O. Should the search for bilingual advantages in executive functioning continue? Cortex 2016, 74, 305–314. [Google Scholar] [CrossRef]
- Deltour, J. Echelle de Vocabulaire Mill Hill de J. C. Raven; Raven Mill Hill Vocabulary Scale; Editions l’Application des Techniques Modernes: Braine-le Chateau, Belgium, 1993. [Google Scholar]
- Reitan, R.M. Validity of the Trail Making Test as an indicator of organic brain damage. Percept. Mot. Skills 1958, 8, 271–276. [Google Scholar] [CrossRef]
- Stroop, J.R. Studies of interference in serial verbal reactions. J. Exp. Psychol. 1935, 18, 643–662. [Google Scholar] [CrossRef]
- Kaplan, E.; Goodglass, H.; Weintraub, S. Boston Naming Test-2; Pro-Ed: Austin, TX, USA, 2001. [Google Scholar]
- Bryan, J.; Luszcz, M.A.; Crawford, J.R. Verbal knowledge and speed of information processing as mediators of age differences in verbal fluency performance among older adults. Psychol. Aging 1997, 12, 473–478. [Google Scholar] [CrossRef] [PubMed]
- Buschke, H. Cued recall in amnesia. J. Clin. Neuropsychol. 1984, 6, 433–440. [Google Scholar] [CrossRef] [PubMed]
- Benton, A.L.; Hamsher, K.; Varney, N.; Spreen, O. Contributions to Neuropsychological Assessment: A Clinical Manual; Oxford University Press: New York, NY, USA, 1983. [Google Scholar]
- Pillon, B.; Dubois, B.; Bonnet, A.M.; Esteguy, M.; Guimaraes, J.; Vigouret, J.M.; Lhermitte, F.; Agid, Y. Cognitive slowing in Parkinson’s disease fails to respond to levodopa treatment: The 15-objects test. Neurology 1989, 39, 762–768. [Google Scholar] [CrossRef] [PubMed]
- Osterrieth, P.A. Le test de copie d’une figure complexe. Arch. Psychol. 1944, 30, 206–356. [Google Scholar]
- Teng, E.L.; Hasegawa, K.; Homma, A.; Imai, Y.; Larson, E.; Graves, A.; Sugimoto, K.; Yamaguchi, T.; Sasaki, H.; Chiu, D.; et al. The Cognitive Abilities Screening Instrument (CASI): A practical test for cross-cultural epidemiological studies of dementia. Int. Psychogeriatr. 1994, 6, 45–58. [Google Scholar] [CrossRef] [PubMed]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Stefani, A.; Sancesario, G.; Pierantozzi, M.; Leone, G.; Galati, S.; Hainsworth, A.H.; Diomedi, M. CSF biomarkers, impairment of cerebral hemodynamics and degree of cognitive decline in Alzheimer’s and mixed dementia. J. Neurol. Sci. 2009, 283, 109–115. [Google Scholar] [CrossRef]
- Smits, L.L.; van Harten, A.C.; Pijnenburg, Y.A.; Koedam, E.L.; Bouwman, F.H.; Sistermans, N.; Reuling, I.E.; Prins, N.D.; Lemstra, A.W.; Scheltens, P.; et al. Trajectories of cognitive decline in different types of dementia. Psychol. Med. 2015, 45, 1051–1059. [Google Scholar] [CrossRef]
- Darvesh, S.; Leach, L.; Black, S.E.; Kaplan, E.; Freedman, M. The behavioural neurology assessment. Can. J. Neurol. Sci. 2005, 32, 167–177. [Google Scholar] [CrossRef] [PubMed]
- Delis, D.C.; Kaplan, E.; Kramer, J. Delis Kaplan Executive Function System; The Psychological Corporation: San Antonio, TX, USA, 2001. [Google Scholar]
- Teng, E.L.; Chui, H.C. The Modified Mini-Mental State (3MS) examination. J. Clin. Psychiatry 1987, 48, 314–318. [Google Scholar] [PubMed]
- Kaplan, E.; Goodglass, H.; Weintraub, S. The Boston Naming Test; Lea & Febiger: Philadelphia, PA, USA, 1983. [Google Scholar]
- Buschke, H.; Fuld, P.A. Evaluating storage, retention, and retrieval in disordered memory and learning. Neurology 1974, 24, 1019–1025. [Google Scholar] [CrossRef] [PubMed]
- Wechsler, D. Wechsler Adult Intelligence Scale-Revised; The Psychological Corporation: New York, NY, USA, 1981. [Google Scholar]
- Mattis, S. Mental Status Examination for Organic Mental Syndrome in the Elderly Patient; Grune & Stratton: New York, NY, USA, 1976. [Google Scholar]
- D’Elia, L.F.; Satz, P.; Uchiyama, C.L.; White, T. Color Trails Test (CTT); Psychological Assessment Resources, Inc.: Odessa, FL, USA, 1996. [Google Scholar]
- Shulman, K.I.; Gold, D.P.; Cohen, C.A.; Zucchero, C.A. Clock-drawing and dementia in the community: A longitudinal study. Int. J. Geriatr. Psychiatry 1993, 8, 487–496. [Google Scholar] [CrossRef]
- Petermann, F.; Lepach, A.C. Wechsler Memory Scale-Fourth Edition [German Edition]; Pearson: Frankfurt, Germany, 2012. [Google Scholar]
- Härting, C.; Markowitsch, H.J.; Neufeld, H.; Calabrese, P.; Deisinger, K.; Kessler, J. Wechsler Memory Scale-Revised Edition [German Edition]; Huber: Bern, Switzerland, 2000. [Google Scholar]
- González, H.M.; Mungas, D.; Reed, B.R.; Marshall, S.; Haan, M.N. A new verbal learning and memory test for English- and Spanish-speaking older people. J. Int. Neuropsychol. Soc. 2001, 7, 544–555. [Google Scholar] [CrossRef] [PubMed]
- Mungas, D.; Reed, B.R.; Crane, P.K.; Haan, M.N.; González, H. Spanish and English Neuropsychological Assessment Scales (SENAS): Further development and psychometric characteristics. Psychol. Assess. 2004, 16, 347–359. [Google Scholar] [CrossRef] [PubMed]
- Jorm, A.F.; Jacomb, P.A. The Informant Questionnaire on Cognitive Decline in the Elderly (IQCODE): Sociodemographic correlates, reliability, validity, and some norms. Psychol. Med. 1989, 19, 1015–1022. [Google Scholar] [CrossRef] [PubMed]
- Sperling, R.A.; Aisen, P.S.; Beckett, L.A.; Bennett, D.A.; Craft, S.; Fagan, A.M.; Iwatsubo, T.; Jack, C.R., Jr.; Kaye, J.; Montine, T.J.; et al. Toward defining the preclinical stages of Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimer’s Dement. 2011, 7, 280–292. [Google Scholar] [CrossRef]
- Luk, G.; Bialystok, E.; Craik, F.I.M.; Grady, C.L. Lifelong bilingualism maintains white matter integrity in older adults. J. Neurosci. 2011, 31, 16808–16813. [Google Scholar] [CrossRef]
- Grady, C.L.; Luk, G.; Craik, F.I.M.; Bialystok, E. Brain network activity in monolingual and bilingual older adults. Neuropsychologia 2015, 66, 170–181. [Google Scholar] [CrossRef]
- Diniz, B.S.; Yassuda, M.S.; Nunes, P.V.; Radanovic, M.; Forlenza, O.V. Mini-mental State Examination performance in mild cognitive impairment subtypes. Int. Psychogeriatr. 2007, 19, 647–656. [Google Scholar] [CrossRef] [PubMed]
- Everitt, B.S.; Skrondal, A. The Cambridge Dictionary of Statistics, 4th ed.; Cambridge University Press: Cambridge, UK, 2010; pp. 1–480. ISBN 13-978-0521766999. [Google Scholar]
- EClipSE Collaborative Members; Brayne, C.; Ince, P.G.; Keage, H.A.; McKeith, I.G.; Matthews, F.E.; Polvikoski, T.; Sulkava, R. Education, the brain and dementia: Neuroprotection or compensation? Brain 2010, 133, 2210–2216. [Google Scholar] [CrossRef] [PubMed]
- McCabe, A.; Tamis-LeMonda, C.S.; Bornstein, M.H.; Cates, C.B.; Golinkoff, R.; Guerra, A.W.; Hirsh-Pasek, K.; Hoff, E.; Kuchirko, Y.; Melzi, G.; et al. Multilingual children: Beyond myths and towards best practices. Soc. Pol. Rep. 2013, 27, 1–21. [Google Scholar] [CrossRef]
- Scarmeas, N.; Stern, Y. Cognitive reserve and lifestyle. J. Clin. Exp. Neuropsychol. 2003, 25, 625–633. [Google Scholar] [CrossRef] [PubMed]
- Hultsch, D.F.; Hertzog, C.; Small, B.J.; Dixon, R.A. Use it or lose it: Engaged lifestyle as a buffer of cognitive decline in aging? Psychol. Aging 1999, 14, 245–263. [Google Scholar] [CrossRef]
- Adam, S.; Bonsang, E.; Grotz, C.; Perelman, S. Occupational activity and cognitive reserve: Implications in terms of prevention of cognitive aging and Alzheimer’s disease. Clin. Interv. Aging 2013, 8, 377–390. [Google Scholar] [CrossRef]
- Capurso, A.; Panza, F.; Solfrizzi, V.; Torres, F.; Capurso, C.; Mastroianni, F.; Del Parigi, A. Age-related cognitive decline: Evaluation and prevention strategy. Recenti Prog. Med. 2000, 91, 127–134. (In Italian) [Google Scholar]
- Irvine, K.; Laws, K.R.; Gale, T.M.; Kondel, T.K. Greater cognitive deterioration in women than men with Alzheimer’s disease: A meta analysis. J. Clin. Exp. Neuropsychol. 2012, 34, 989–998. [Google Scholar] [CrossRef]
- Laws, K.R.; Irvine, K.; Gale, T.M. Sex differences in cognitive impairment in Alzheimer’s disease. World J. Psychiatry 2016, 6, 54–65. [Google Scholar] [CrossRef]
- Woumans, E.; Versijpt, J.; Sieben, A.; Santens, P.; Duyck, W. Bilingualism and cognitive decline: A story of pride and prejudice. J. Alzheimer’s Dis. 2017, 60, 1237–1239. [Google Scholar] [CrossRef]
- Ramakrishnan, S.; Mekala, S.; Mamidipudi, A.; Yareeda, S.; Mridula, R.; Bak, T.H.; Alladi, S.; Kaul, S. Comparative effects of education and bilingualism on the onset of mild cognitive impairment. Dement. Geriatr. Cogn. Disord. 2017, 44, 222–231. [Google Scholar] [CrossRef] [PubMed]
- Logue, S.F.; Gould, T.J. The neural and genetic basis of executive function: Attention, cognitive flexibility, and response inhibition. Pharmacol. Biochem. Behav. 2014, 123, 45–54. [Google Scholar] [CrossRef] [PubMed]
- Green, D.W.; Abutalebi, J. Language control in bilinguals: The adaptive control hypothesis. J. Cogn. Psychol. 2013, 25, 515–530. [Google Scholar] [CrossRef] [PubMed]
- Kroll, J.F.; Bialystok, E. Understanding the consequences of bilingualism for language processing and cognition. J. Cogn. Psychol. 2013, 25, 497–514. [Google Scholar] [CrossRef] [PubMed]
- Gold, B.T.; Kim, C.; Johnson, N.F.; Kryscio, R.J.; Smith, C.D. Lifelong bilingualism maintains neural efficiency for cognitive control in aging. J. Neurosci. 2013, 33, 387–396. [Google Scholar] [CrossRef] [PubMed]
- Tekin, S.; Mega, M.S.; Masterman, D.M.; Chow, T.; Garakian, J.; Vinters, H.V.; Cummings, J.L. Orbitofrontal and anterior cingulate cortex neurofibrillary tangle burden is associated with agitation in Alzheimer disease. Ann. Neurol. 2001, 49, 355–361. [Google Scholar] [CrossRef] [PubMed]
- Lim, H.K.; Juh, R.; Pae, C.U.; Lee, B.T.; Yoo, S.S.; Ryu, S.H.; Kwak, K.R.; Lee, C.; Lee, C.U. Altered verbal working memory process in patients with Alzheimer’s disease: An fMRI investigation. Neuropsychobiology 2008, 57, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Zomorrodi, R.; Ghazala, Z.; Goodman, M.S.; Blumberger, D.M.; Cheam, A.; Fischer, C.; Daskalakis, Z.J.; Mulsant, B.H.; Pollock, B.G.; et al. Extent of dorsolateral prefrontal cortex plasticity and its association with working memory in patients with Alzheimer disease. JAMA Psychiatry 2017, 74, 1266–1274. [Google Scholar] [CrossRef] [PubMed]
- Jahn, H. Memory loss in Alzheimer’s disease. Dialogues Clin. Neurosci. 2013, 15, 445–454. [Google Scholar] [PubMed]
- Volkow, N.D.; Gur, R.C.; Wang, G.J.; Fowler, J.S.; Moberg, P.J.; Ding, Y.S.; Hitzemann, R.; Smith, G.; Logan, J. Association between decline in brain dopamine activity with age and cognitive and motor impairment in healthy individuals. Am. J. Psychiatry 1998, 155, 344–349. [Google Scholar] [PubMed]
- Badgaiyan, R.D.; Wack, D. Evidence of dopaminergic processing of executive inhibition. PLoS ONE 2011, 6, e28075. [Google Scholar] [CrossRef] [PubMed]
- Finke, K.; Dodds, C.M.; Bublak, P.; Regenthal, R.; Baumann, F.; Manly, T.; Müller, U. Effects of modafinil and methylphenidate on visual attention capacity: A TVA-based study. Psychopharmacology 2010, 210, 317–329. [Google Scholar] [CrossRef] [PubMed]
- Nandam, L.S.; Hester, R.; Wagner, J.; Cummins, T.D.; Garner, K.; Dean, A.J.; Kim, B.N.; Nathan, P.J.; Mattingley, J.B.; Bellgrove, M.A. Methylphenidate but not atomoxetine or citalopram modulates inhibitory control and response time variability. Biol. Psychiatry 2011, 69, 902–904. [Google Scholar] [CrossRef] [PubMed]
- Gutchess, A. Plasticity of the aging brain: New directions in cognitive neuroscience. Science 2014, 346, 579–582. [Google Scholar] [CrossRef] [PubMed]
- Van den Noort, M.; Lim, S.; Bosch, P. Recognizing the risks of brain stimulation. Science 2014, 346, 1307. [Google Scholar] [CrossRef]
- Patz, S.; Fovargue, D.; Schregel, K.; Nazari, N.; Palotai, M.; Barbone, P.E.; Fabry, B.; Hammers, A.; Holm, S.; Kozerke, S.; et al. Imaging localized neuronal activity at fast time scales through biomechanics. Sci. Adv. 2019, 5, eaav3816. [Google Scholar] [CrossRef]
- Skehan, P. Individual differences in second language learning. Stud. Second Lang. Acquis. 1991, 13, 275–298. [Google Scholar] [CrossRef]
- Au, R.; Piers, R.J.; Lancashire, L. Back to the future: Alzheimer’s disease heterogeneity revisited. Alzheimer’s Dement. 2015, 1, 368–370. [Google Scholar] [CrossRef]
- Vanclay, F.; Baines, J.T.; Taylor, C.N. Principles for ethical research involving humans: Ethical professional practice in impact assessment Part 1. Impact Assess. Proj. Apprais. 2013, 31, 243–253. [Google Scholar] [CrossRef]
- Paap, K.R.; Johnson, H.A.; Sawi, O. Bilingual advantages in executive functioning either do not exist or are restricted to very specific and undetermined circumstances. Cortex 2015, 69, 265–278. [Google Scholar] [CrossRef]
- Paap, K.R.; Johnson, H.A.; Sawi, O. Are bilingual advantages dependent upon specific tasks or specific bilingual experiences? J. Cogn. Psychol. 2014, 26, 615–639. [Google Scholar] [CrossRef]
- Miller, G.A.; Chapman, J.P. Misundertanding analysis of covariance. J. Abnorm. Psychol. 2001, 110, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Berken, J.A.; Chai, X.; Chen, J.K.; Gracco, V.L.; Klein, D. Effects of early and late bilingualism on resting-state functional connectivity. J. Neurosci. 2016, 36, 1165–1172. [Google Scholar] [CrossRef] [PubMed]
- Rama, T. Phonotactic diversity predicts the time depth of the world’s language families. PLoS ONE 2013, 8, e63238. [Google Scholar] [CrossRef] [PubMed]
- Hindle, J.V.; Martin-Forbes, P.A.; Bastable, A.J.M.; Pye, K.L.; Martyr, A.; Whitaker, C.J.; Craik, F.I.M.; Bialystok, E.; Thomas, E.M.; Mueller Gathercole, V.C.; et al. Cognitive reserve in Parkinson’s disease: The effects of Welsh-English bilingualism on executive function. Parkinsons. Dis. 2015, 2015, 943572. [Google Scholar] [CrossRef] [PubMed]
- Seeman, M.V. Bilingualism and schizophrenia. World. J. Psychiatry 2016, 6, 192–198. [Google Scholar] [CrossRef]
- Malpetti, M.; Ballarini, T.; Presotto, L.; Garibotto, V.; Tettamanti, M.; Perani, D.; Alzheimer’s Disease Neuroimaging Initiative (ADNI) database; Network for Efficiency and Standardization of Dementia Diagnosis (NEST-DD) database. Gender differences in healthy aging and Alzheimer’s dementia: A 18F-FDG-PET study of brain and cognitive reserve. Hum. Brain Mapp. 2017, 38, 4212–4227. [Google Scholar]
- Van der Slik, F.W.; van Hout, R.W.; Schepens, J.J. The gender gap in second language acquisition: Gender differences in the acquisition of Dutch among immigrants from 88 countries with 49 mother tongues. PLoS ONE 2015, 10, e0142056. [Google Scholar] [CrossRef]
- Rocca, W.A. Time, sex, gender, history, and dementia. Alzheimer Dis. Assoc. Disord. 2017, 31, 76–79. [Google Scholar] [CrossRef]
- Antoniou, M.; Wright, S.M. Uncovering the mechanisms responsible for why language learning may promote healthy cognitive aging. Front. Psychol. 2017, 8, 2217. [Google Scholar] [CrossRef]
- Van den Noort, M.; Struys, E.; Kim, K.; Bosch, P.; Mondt, K.; van Kralingen, R.; Lee, M.; van de Craen, P. Multilingual processing in the brain. Int. J. Multiling 2014, 11, 182–201. [Google Scholar] [CrossRef]
- Perquin, M.; Vaillant, M.; Schuller, A.M.; Pastore, J.; Dartigues, J.F.; Lair, M.L.; Diederich, N.; MemoVie Group. Lifelong exposure to multilingualism: New evidence to support cognitive reserve hypothesis. PLoS ONE 2013, 8, e62030. [Google Scholar] [CrossRef] [PubMed]
- Klein, R.M.; Christie, J.; Parkvall, M. Does multilingualism affect the incidence of Alzheimer’s disease? A worldwide analysis by country. SSM Popul. Health 2016, 2, 463–467. [Google Scholar] [CrossRef]
- Padilla, C.; Mendez, M.F.; Jimenez, E.E.; Teng, E. Bilingualism in older Mexican-American immigrants is associated with higher scores on cognitive screening. BMC Geriatr. 2016, 16, 189. [Google Scholar] [CrossRef]
- Bak, T.H. The impact of bilingualism on cognitive ageing and dementia: Finding a path through a forest of confounding variables. Linguist Approaches Biling. 2016, 6, 205–226. [Google Scholar] [CrossRef]
- Lehtonen, M.; Soveri, A.; Laine, A.; Järvenpää, J.; de Bruin, A.; Antfolk, J. Is bilingualism associated with enhanced executive functioning in adults? A meta-analytic review. Psychol. Bull. 2018, 144, 394–425. [Google Scholar] [CrossRef] [PubMed]
- Paap, K.R. The bilingual advantage debate: Quantity and quality of the evidence. In The Handbook of the Neuroscience of Multilingualism; Schwieter, J.W., Ed.; Wiley-Blackwell: West Sussex, UK, 2018; pp. 701–735. ISBN 9781119387701. [Google Scholar]
- Nickerson, R.S. Confirmation bias: A ubiquitous phenomenon in many guises. Rev. Gen. Psychol. 1998, 2, 175–220. [Google Scholar] [CrossRef]
- Pashler, H.; Harris, C.R. Is the replicability crisis overblown? Three arguments examined. Perspec. Psychol. Sci. 2012, 7, 531–536. [Google Scholar] [CrossRef]
- Ferguson, C.J.; Heene, M. A vast graveyard of undead theories: Publication bias and psychological science’s aversion to the null. Perspect. Psychol. Sci. 2012, 7, 555–561. [Google Scholar] [CrossRef]
- De Bruin, A.; Treccani, B.; Della Sala, S. Cognitive advantage in bilingualism: An example of publication bias? Psychol. Sci. 2015, 49, 287–296. [Google Scholar] [CrossRef]
- Van den Noort, M.; Bosch, P. The twilight of dementia. Lancet 2010, 376, 1537–1538. [Google Scholar] [CrossRef]
- Honig, L.S.; Vellas, B.; Woodward, M.; Boada, M.; Bullock, R.; Borrie, M.; Hager, K.; Andreasen, N.; Scarpini, E.; Liu-Seifert, H.; et al. Trial of solanezumab for mild dementia due to Alzheimer’s disease. N. Engl. J. Med. 2018, 378, 321–330. [Google Scholar] [CrossRef] [PubMed]
- Murphy, M.P. Amyloid-beta solubility in the treatment of Alzheimer’s disease. N. Engl. J. Med. 2018, 378, 391–392. [Google Scholar] [CrossRef] [PubMed]
- Richards, R.I.; Robertson, S.A.; Kastner, D.L. Neurodegenerative diseases have genetic hallmarks of autoinflammatory disease. Hum. Mol. Genet. 2018, 27, R108–R118. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors/Publication Year | Number of Subjects | Type of Measurement | Results | In Support of Cognitive Reserve Hypothesis? | Authors’ Conclusions |
|---|---|---|---|---|---|
| Kavé et al., 2008 [29] | 814 healthy, older adults: 211 were bilingual, 230 were trilingual, and 373 individuals spoke more than three languages | KCST1 and MMSE2 | The number of languages spoken predicted cognitive test scores. This result could not be explained by other variables, such as age, gender, place of birth, age at immigration, or education. Multilingualism was found to be a significant predictor of cognitive state. The individuals who were better in their foreign language than in their mother tongue on average showed better results than the individuals whose mother tongue was their best language. The effect of the number of languages on cognitive state was significant in both groups. | YES | Evidence was found for a cognitive reserve-enhancing effect of lifelong bilingualism, trilingualism, and especially multilingualism. |
| Crane et al., 2010 [32] | 2520 bilingual older adults without dementia | CASI3 | Neither the use of spoken nor written Japanese in midlife was found to affect cognitive decline in late life. | NO | No evidence was found for a cognitive reserve-enhancing effect of lifelong bilingualism. |
| Kousaie and Phillips, 2012 [34] | 45 healthy older adults: 20 were bilingual and 25 were monolingual | MoCA4, Stroop test | No smaller Stroop interference was found for the healthy older bilingual adults as compared to the healthy older monolingual adults. No effect of bilingualism was found in aging on the Stroop task. | NO | No bilingual advantage was found in older adults, questioning the robustness and/or specificity of the cognitive reserve-enhancing effect of lifelong bilingualism. |
| Bak et al., 2014 [38] | 853 healthy older adults: 160 knew 2 languages, 61 knew 3, 16 knew 4, and 8 knew 5 | Letter-number sequencing, Matrix reasoning, Block design, Digit symbol, Symbol search, Digit span backward, Logical memory, Spatial span, Moray House Test, NART5, and verbal fluency | A beneficial effect of bilingualism on cognition in aging was found, affecting the domains of reading, verbal fluency, and general intelligence more than the domains of memory, reasoning, and speed of processing. No effect of age of acquisition was found. These results cannot be explained by gender, socioeconomic status, or immigration. | YES6 | Evidence was found for a cognitive reserve-enhancing effect of lifelong bilingualism and multilingualism, even after controlling for childhood intelligence. No effect of age of acquisition was found. |
| Ihle et al., 2016 [46] | 2812 healthy older adults: 1884 spoke one language, 492 two, 281 three, 115 four, 31 five, and 9 six | Mill Hill vocabulary scale, TMT7, and interview | The number of languages spoken was found to be a better predictor of cognitive performance than leisure activities and physical demand of job/gainful activity. Educational attainment and cognitive level of job were as good as predictors of cognitive performance. | PARTIAL | Speaking different languages on a regular basis may contribute to cognitive reserve in old age, yet this may not be universal. |
| Estanga et al., 2017 [48] | 278 healthy middle-aged adults: 100 were monolingual, 81 were early bilingual, and 97 were late bilingual | Cerebrospinal fluid AD8 markers, MMSE, FCSRT9, Digit span test, Stroop test, TMT, verbal fluency, BNT, JLO10, 15 object test, and ROCF11 | A moderation effect was found for bilingualism on both the relationship between age and the presence of AD biomarkers in cerebrospinal fluid and on the relationship between age and executive functioning. Early bilingualism was found to be associated with a better profile of AD biomarkers in cerebrospinal fluid. | YES | Bilingualism contributes to cognitive reserve. It enhances executive and visual-spatial functioning. |
| Anderson et al., 2018 [50] | 61 healthy older adults: 31 were bilingual and 30 were monolingual | Diffusion tensor imaging, MMSE | After controlling and matching for confounds (e.g., intelligence, mini-mental state scores, and demographic variables), a greater axial diffusivity in the left superior longitudinal fasciculus was found in bilinguals compared to monolinguals, indicating a neural reserve in bilingual older adults. | YES | A greater axial diffusivity in the left superior longitudinal fasciculus was found in bilingual older adults compared to monolingual older adults, supporting the cognitive reserve hypothesis. |
| Mukadam et al., 2018 [51] | 2087 healthy older adults: 193 were bilingual and 1894 were monolingual | MMSE, NART, Boston naming test, and verbal fluency | Bilingual older adults had lower MMSE scores than monolingual older adults. This result was entirely explained by education, which also partly explained differences between the two groups in baseline executive functioning. No differences between bilingual older adults and monolingual older adults were found in MMSE decline over time or on baseline tests of executive function. | NO | The authors conclude that bilingualism is a complex phenomenon. When bilingualism is not the result of greater educational attainment, it does not always protect older individuals from cognitive decline. |
| Authors/Publication Year | Number of Reviewed Studies | Main Results | Authors’ Conclusions |
|---|---|---|---|
| Bialystok et al., 2016 [53] 1 | No information given | Bilingualism was found to have protective effects across the lifespan. Bilingual individuals outperformed monolinguals on executive functioning tasks and selective attention tasks. | The results show that bilingualism is a potent source of cognitive reserve. |
| Quinteros Baumgart and Billick, 2018 [54] | No information given | The results showed that a link exists between bilingualism and higher levels of controlled attention and inhibition in executive control; moreover, bilingualism can protect individuals against the decline of executive control later in life as a result of the increased cognitive reserve. Several factors, like immigration and personal experiences, seem to affect the cognitive reserve-enhancing effect of lifelong bilingualism and multilingualism. | Evidence was found for the cognitive reserve-enhancing effect of lifelong bilingualism and multilingualism. Depending on several factors and individual experiences bilingualism can protect individuals against the decline of executive control in aging. |
| Authors/Publication Year | Number of Subjects | Type of Measurement | Results | In Support of Cognitive Reserve Hypothesis? | Authors’ Conclusions |
|---|---|---|---|---|---|
| Bialystok et al., 2007 [13] | 184 patients with dementia: 93 were bilingual and 91 were monolingual | MMSE1 | The symptoms of dementia appeared 4 years later in the group of older bilingual adults as compared to the group of older monolingual adults. The same results on the MMSE for the bilinguals and the monolinguals were found 4 years prior to the diagnosis of dementia. A shift in onset age of dementia with no change in rate of progression was found in favor of the bilingual older adults. | YES | Evidence was found for the cognitive reserve hypothesis and for the cognitive reserve-enhancing effect of lifelong bilingualism. |
| Chertkow et al., 2010 [30] | 632 patients with probable AD2: 253 were multilingual and 379 were monolingual | MMSE | The results showed a protective effect of bilingualism in native Canadians whose first language was French, but not in those whose first language was English. A protective effect of bilingualism was found in immigrants to Canada. | PARTIAL | Overall, lifelong multilingualism (but not bilingualism) was found to have a protective effect. |
| Craik et al., 2010 [31] | 211 patients with probable AD: 102 were bilingual and 109 were monolingual | MMSE | The bilingual patient group showed a later onset of symptoms (5.1 years) and were diagnosed later (on average 4.3 years) than the monolingual patient group. | YES | Lifelong bilingualism was found to be a protective factor against the onset of AD. Support was found for the cognitive reserve hypothesis and the idea of a cognitive reserve-enhancing effect of lifelong bilingualism. |
| Gollan et al., 2011 [33] | 44 bilingual patients with probable AD: 22 were highly educated and 22 were patients with low education | BNT3 and subjective rating instrument of second language proficiency | An association was found between higher degrees of bilingualism and increasingly later age-of-diagnosis of AD. The degree of education was found to be an interacting factor. Only objective measures, not self-reported degree of bilingualism, were found to predict age-of-diagnosis of AD. | PARTIAL | Lifelong bilingualism was found to delay the onset of AD, but this was only the case for the patients with a low education level and not for the patients with a high education level. Objective measures, not subjective measures, were found to be predictors. |
| Sanders et al., 2012 [35] | 1779 older adults: 390 were bilingual and 1389 were monolingual | Several language background questions | No association was found between non-native speakers of English and dementia or between non-native speakers of English and AD. When education was assessed further, an increased risk of dementia was found for the non-native speakers of English with more than 16 years of education. | NO | No evidence for a relationship between lifelong bilingualism and the onset of AD was found. A relation might exist in an education-dependent manner, but then in the opposite direction; highly educated bilinguals might be at increased risk. |
| Schweizer et al., 2012 [36] | 40 older adults with probable AD: 20 were bilingual and 20 were monolingual | Analysis of CT4 scans | Substantially greater amounts of brain atrophy were found in bilingual patients than in monolingual patients in areas traditionally used to clinically diagnose AD, indicating that greater amounts of neuropathology are needed before the clinical symptoms of AD become visible in bilinguals. | YES | Evidence was found for the cognitive reserve-enhancing effect of lifelong bilingualism and for a delay in the onset of AD in bilinguals. |
| Alladi et al., 2013 [37] | Case records of 648 middle-aged to older-aged patients with dementia were analyzed: 391 were bilingual and 257 were monolingual | MMSE, ACE-R5, and CDR6 | The bilingual participants developed dementia 4.5 years later than the monolingual participants. This finding could not be explained by other factors, such as education, gender, occupation, living in a city or in the countryside. | YES | Evidence was found for the cognitive reserve hypothesis and for the cognitive reserve-enhancing effect of lifelong bilingualism. |
| Bialystok et al., 2014 [39] | 149 older adults: 76 were bilingual and 73 were monolingual. 74 of the patients had MCI9 and 75 had probable AD | MMSE, BNA7, D-KEFS8 | Bilinguals reported later onset ages of the disorder than monolinguals. In the MCI group, the delay was 4.7 years and in the AD group, the delay was 7.3 years in comparison with the monolinguals. These results could not be explained by differences in lifestyle variables, such as smoking, alcohol use, physical activity, diet, or social contacts. | YES | Bilinguals reported later onset ages than monolinguals, supporting the idea that lifelong bilingualism contributes to cognitive reserve. This result could not be explained by differences in lifestyle. |
| Yeung et al., 2014 [40] | 1616 community-living older adults: 703 were bilingual and 913 were monolingual | Structured interview, 3MSE10 | No association was found between bilingualism and dementia at the first measurement. Also, for the individuals who were cognitively healthy at the first measurement, no association was found between speaking more than one language and dementia at the second measurement five years later. | NO | No association was found between speaking more than one language and dementia. |
| Zahodne et al., 2014 [41] | 1067 older adults: 430 were bilingual and 637 were monolingual. The participants did not initially suffer from dementia | 15-item BNT, SRT11, WAIS12, MDRS13, CTT14 | Although older bilingual adults were found to have better memory and executive function skills at baseline than monolinguals, no protective effect of bilingualism was found among Spanish-speaking immigrants. | NO | No cognitive reserve-enhancing effect of lifelong bilingualism was found. The results show that bilingualism did not alter cognitive decline or protect against dementia. |
| Kowoll et al., 2015 [42] | 86 older adults: 41 were bilingual and 45 were monolingual. 22 of them suffered from MCI and 47 from AD; 17 were healthy controls | MMSE, BNT, TMT15, clock drawing test, CERAD-NP16, Wechsler memory scale | The study revealed that the dominant language is first affected in bilingual patients with MCI. The bilingual MCI group showed significantly lower verbal fluency and picture-naming scores in their dominant language than bilingual controls. Deficits of the second language appeared later in bilingual patients suffering from AD when compared to bilingual controls. | NO | No cognitive reserve-enhancing effect of lifelong bilingualism was found. |
| Lawton et al., 2015 [43] | 81 older adults with AD: 27 were bilingual and 54 were monolingual | Verbal learning test, SENAS17, IQCODE18 3MSE | The bilingual older adults were more highly educated than the monolingual older adults. This was not the case for the U.S. born bilinguals and monolinguals. No differences between the bilinguals and monolinguals were found in the mean age of dementia diagnosis. | NO | No differences in age of onset of AD were found between bilinguals and monolinguals, showing no evidence for a protective effect of lifelong bilingualism. |
| Woumans et al., 2015 [44] | 134 patients with probable AD: 65 were bilingual and 69 were monolingual | MMSE | For the bilingual patients, a delay was found, on average, of 4.6 years in manifestation and 4.8 years in diagnosis compared to the monolingual patients. | YES | Evidence was found for the cognitive reserve hypothesis and for the cognitive reserve-enhancing effect of lifelong bilingualism. |
| Clare et al., 2016 [45] | 86 older adults with probable AD: 37 were bilingual and 49 were monolingual | Background measures, MMSE, a whole test battery of executive functioning tasks | No clear advantage in executive functioning was found in the bilinguals compared to the monolinguals. A delay in AD may exist in bilinguals, but if so, the results are less convincing than in previous studies. The bilingual patients came later to the attention services than the monolingual patients. | NO | A delay in the onset of AD may occur, but if so, the results are less convincing than the previously reported results in the literature. |
| Kowoll et al., 2016 [47] | 30 older adults: 16 were lifelong bilingual and 14 were monolingual. 12 were diagnosed with MCI and 18 with early stage AD | FDG19 and PET20 | The results showed that the bilingual patients showed substantially greater impairment of glucose uptake in frontotemporal regions, patietal regions, and in the left cerebellum in comparison with monolingual patients. | YES | Bilingualism is likely to contribute to cognitive reserve on a neural level. |
| Perani et al., 2017 [49] | 85 patients with probable AD: 45 were bilingual and 40 were monolingual | Brain metabolism and neural connectivity | An increased connectivity in the executive control and in the default mode networks was found in the bilingual patients compared to the monolingual patients. The degree of lifelong bilingualism (i.e., high, moderate, or low use) was found to significantly correlate to functional modulations in crucial neural networks. | YES | Evidence was found for both neural reserve and compensatory mechanisms in bilingual patients with probable AD, supporting the cognitive reserve-enhancing effect of lifelong bilingualism. |
| Zheng et al., 2018 [52] | 129 older adults with probable AD: 61 were bilingual and 68 were monolingual | Structured interview, MMSE | The results showed that the Cantonese/Mandarin bilinguals had a delay in onset of AD of 5.5 years and, furthermore, visited the clinic later compared to the monolinguals. | YES | Constantly speaking two languages from at least early adulthood can delay the onset of AD, supporting the cognitive reserve hypothesis. |
| Authors/Publication Year | Number of Reviewed Studies | Main Results | Authors’ Conclusions |
|---|---|---|---|
| Freedman et al., 2014 [55] | 4 original studies | One Canadian (Toronto) and one Indian (Hyderabad) study showed a significant effect of lifelong bilingualism in delaying the onset of AD by up to 5 years whereas another Canadian study (Montreal) showed this effect only for multilingual individuals who speak at least four languages or for immigrants who speak at least two languages. | A protective effect of bilingualism in delaying onset of dementia was found. In the context of specific cultural and immigration factors, only multilingualism, not bilingualism, leads to a postponement of dementia. This needs to be investigated further in future cross-cultural studies. |
| Gold 2015 [56] | No information given | The protective and delaying effect of bilingualism against the symptoms of AD may work via the frontostriatal and frontoparietal executive functioning networks rather than medial temporal lobe memory networks. In addition, the beneficial effects of bilingualism to cognitive reserve may work via specific cellular and molecular mechanisms. | Evidence exists in the literature for a delay of the onset of AD symptoms in bilingual older adults by several years. |
| Guzmán-Vélez et al., 2015 [57] | 15 original studies | Lifelong bilingualism was found to be related to more efficient use of brain resources, helping bilingual individuals to maintain cognitive functioning in the presence of neuropathology. The authors discuss several neural mechanisms underlying this phenomenon. | Evidence was found for the idea that lifelong bilingualism is a cognitive (and possibly brain) reserve enhancing factor. More research on the relationship between bilingualism, education, and the onset of dementia is warranted. This might help individuals in the prevention of and/or coping with a brain disease in a better way in the future. |
| Perani and Abutalebi 2015 [58] | No information given | The use of two or more languages was reported to affect the human brain in terms of anatomo-structural changes. A significant delay of dementia onset was found in bilingual/multilingual individuals. This result was found in different studies conducted in different countries and with different cultural backgrounds of the individuals. | Lifelong bilingualism was found to be a powerful cognitive reserve factor. The onset of dementia in bilingual individuals is delayed by approximately 4 years as compared to monolingual individuals. Lifelong bilingualism results in increases of gray and white matter, especially when frequent second language exposure and use is present throughout life. |
| Bialystok et al., 2016 [53] 1 | No information given | A 4- to 5-year delay in onset age of dementia was found in retrospective studies for bilingual older adults compared to monolingual older adults. These results could not be explained away by factors such as immigration, education, socio-economic background, and age of second language acquisition. | The results showed a protective effect of bilingualism against symptoms of dementia. In general, a delay of between 4 and 5 years in the onset age of dementia was found. |
| Calvo et al., 2016 [59] | 17 original studies | Interpreting the results on the possible relationship between bilingualism and cognitive reserve has been difficult so far. More stringent control of relevant variables is needed. The focus is only on the delay of AD, instead of the changes during the different stages of the disease. | A better methodology in the studies on the relationship between bilingualism and cognitive reserve is needed in order to draw any firm conclusions about the unique cognitive reserve contribution of bilingualism in patients with AD at the different stages of the disease. |
| Klimova et al., 2017 [60] | 14 original studies | Bilingualism was found to delay the onset of dementia in retrospective studies, but this result was not confirmed in prospective studies. More research on the relationship between bilingualism and a delay in the onset of dementia is warranted, especially because positive findings were found in brain studies that investigated the relationship between bilingualism and cognitive reserve. | Evidence was found for the contribution of bilingualism to cognitive reserve in retrospective studies, but this result was not confirmed in prospective studies. Methodological weaknesses in the retrospective studies seem to explain the different findings. |
| Mukadam et al., 2017 [61] | 13 original studies included in qualitative synthesis, of which 4 were included in the meta-analysis | The prospective studies showed no evidence that bilingualism protects against cognitive decline or dementia. Retrospective studies show a different picture, supporting the hypothesis that it contributes to cognitive reserve, protects against cognitive decline, and delays the onset of dementia. These beneficial effects of bilingualism in retrospective studies are affected by differences in education and culture. Therefore, these studies give no insight into the causative relations. | The results obtained in retrospective studies show support for the cognitive reserve hypothesis and for the cognitive reserve-enhancing effect of lifelong bilingualism, but the results obtained in prospective studies do not. Retrospective studies are not suitable to provide any information about the causative relations between bilingualism and cognitive reserve. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Van den Noort, M.; Vermeire, K.; Bosch, P.; Staudte, H.; Krajenbrink, T.; Jaswetz, L.; Struys, E.; Yeo, S.; Barisch, P.; Perriard, B.; et al. A Systematic Review on the Possible Relationship Between Bilingualism, Cognitive Decline, and the Onset of Dementia. Behav. Sci. 2019, 9, 81. https://doi.org/10.3390/bs9070081
Van den Noort M, Vermeire K, Bosch P, Staudte H, Krajenbrink T, Jaswetz L, Struys E, Yeo S, Barisch P, Perriard B, et al. A Systematic Review on the Possible Relationship Between Bilingualism, Cognitive Decline, and the Onset of Dementia. Behavioral Sciences. 2019; 9(7):81. https://doi.org/10.3390/bs9070081
Chicago/Turabian StyleVan den Noort, Maurits, Katrien Vermeire, Peggy Bosch, Heike Staudte, Trudy Krajenbrink, Lars Jaswetz, Esli Struys, Sujung Yeo, Pia Barisch, Benoît Perriard, and et al. 2019. "A Systematic Review on the Possible Relationship Between Bilingualism, Cognitive Decline, and the Onset of Dementia" Behavioral Sciences 9, no. 7: 81. https://doi.org/10.3390/bs9070081
APA StyleVan den Noort, M., Vermeire, K., Bosch, P., Staudte, H., Krajenbrink, T., Jaswetz, L., Struys, E., Yeo, S., Barisch, P., Perriard, B., Lee, S.-H., & Lim, S. (2019). A Systematic Review on the Possible Relationship Between Bilingualism, Cognitive Decline, and the Onset of Dementia. Behavioral Sciences, 9(7), 81. https://doi.org/10.3390/bs9070081