Spontaneous Subdural Hematoma and Behavioral Changes Due to a Dural Arteriovenous Fistula. A Case Report and Literature Review

 ,
,
Abstract
1. Introduction
2. Method
3. Clinical Case
3.1. Laboratory Studies
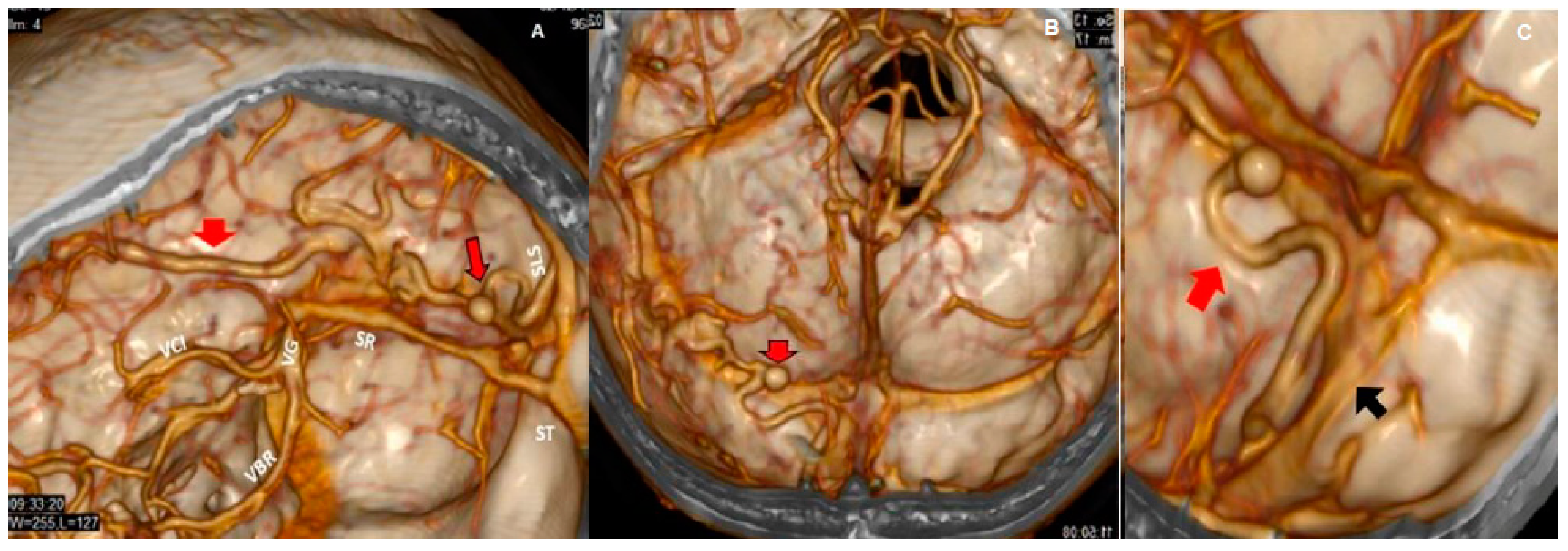
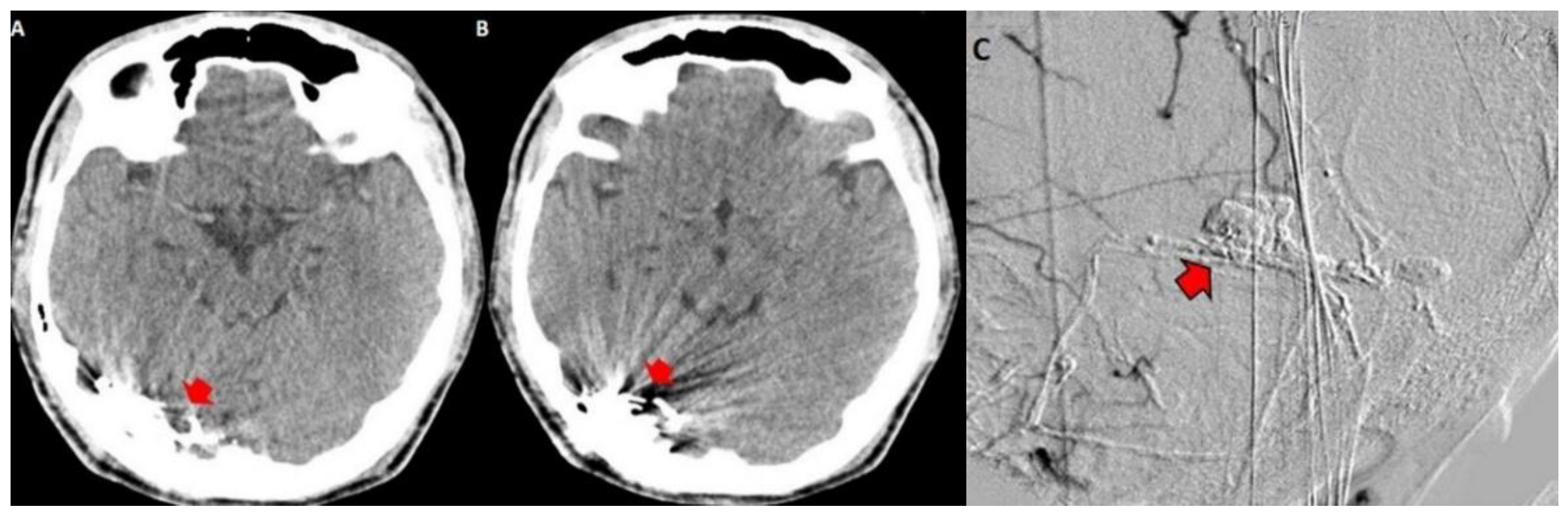
3.2. Imaging Studies
4. Discussion and Literature Review
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Chung, S.; Kim, J.; Kim, J.; Lee, S.; Kwon, S.; Lee, M.; Suh, D. Intracranial dural arteriovenous fistulas: Analysis of 60 patients. Cerebrovasc. Dis. 2002, 13, 79–88. [Google Scholar] [CrossRef] [PubMed]
- Kwon, B.J.; Han, M.H.; Kang, H.S.; Chang, K.H. MR imaging findings of intracranial dural arteriovenous fistulas: Relations with venous drainage patterns. Am. J. Neuroradiol. 2005, 26, 2500–2507. [Google Scholar] [PubMed]
- Quintanilla, J.O.; Pérez, R.F.O.; Herrera, V.C.; García, A.G.; Jarrín, I.G.; Deyá, A.M. 31 Congreso Nacional SERAM. In Proceedings of the Fístulas Arteriovenosas Durales: Historia Natural, diagnóstico, caracterización y tratamiento, Granada, Spain, 24–28 May 2012. [Google Scholar]
- Cognard, C.; Gobin, Y.P.; Pierot, L.; Bailly, A.L.; Houdart, E.; Casasco, A.; Chiras, J.; Merland, J.J. Cerebral dural arteriovenous fistulas: Clinical and angiographic correlation with a revised classification of venous drainage. Radiology 1995, 194, 671–680. [Google Scholar] [CrossRef] [PubMed]
- Borden, J.A.; Wu, J.K.; Shucart, W.A. A proposed classification for spinal and cranial dural arteriovenous fistulous malformations and implications for treatment. J. Neurosurg. 1995, 82, 166–179. [Google Scholar] [CrossRef] [PubMed]
- Brown, R.D.; Wiebers, D.O.; Torner, J.C.; O’Fallon, W.M. Incidence and prevalence of intracranial vascular malformations in Olmsted County, Minnesota, 1965 to 1992. Neurology 1996, 46, 949–952. [Google Scholar] [CrossRef] [PubMed]
- Satomi, J.; Satoh, K. Epidemiology and etiology of dural arteriovenous fistula. Brain Nerve 2008, 60, 883–886. [Google Scholar] [PubMed]
- Kobayashi, A.; Al-Shahi Salman, R. Prognosis and treatment of intracranial dural arteriovenous fistulae: A systematic review and meta-analysis. Int. J. Stroke 2014, 9, 670–677. [Google Scholar] [CrossRef]
- Gross, B.; Du, R. Natural history of cerebral arteriovenous malformations: A meta-analysis. J. Neurosurg. 2013, 118, 437–443. [Google Scholar] [CrossRef]
- Hiramatsu, M.; Sugiu, K.; Hishikawa, T.; Haruma, J.; Tokunaga, K.; Date, I.; Kuwayama, N.; Sakai, N. Epidemiology of Dural Arteriovenous Fistula in Japan: Analysis of Japanese Registry of Neuroendovascular Therapy (JR-NET2). Neurol. Med. Chir. (Tokyo) 2014, 54 (Suppl. 2), 63–71. [Google Scholar] [CrossRef]
- Hou, K.; Ji, T.; Guo, Y.; Xu, B.; Xu, K.; Yu, J. Current Status of Endovascular Treatment for Dural Arteriovenous Fistulas in the Superior Sagittal Sinus Region: A Systematic Review of the Literature. World Neurosurg. 2019, 122, 133–143. [Google Scholar] [CrossRef]
- Piippo, A.; Niemelä, M.; van Popta, J.; Kangasniemi, M.; Rinne, J.; Jääskeläinen, J.; Hernesniemi, J. Characteristics and long-term outcome of 251 patients with dural arteriovenous fistulas in a defined population. J. Neurosurg. 2013, 118, 923–934. [Google Scholar] [CrossRef] [PubMed]
- Maiuri, F.; Iaconetta, G.; Sardo, L.; Briganti, F. Dural arteriovenous malformation associated with recurrent subdural haematoma and intracranial hypertension. Br. J. Neurosurg. 2001, 15, 273–276. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, K.; Oishi, M.; Mizutani, T.; Maejima, S.; Mori, T. Dural arteriovenous fistula on the convexity presenting with pure acute subdural hematoma. Acta Neurol. Belg. 2010, 110, 190–192. [Google Scholar] [PubMed]
- Li, C.; Wang, Y.; Li, Y.; Jiang, C.; Yang, X.; Wu, Z. Clinical and Angioarchitectural Risk Factors Associated with Intracranial Hemorrhage in Dural Arteriovenous Fistulas: A Single-Center Retrospective Study. PLoS ONE 2015, 10, e0131235. [Google Scholar] [CrossRef] [PubMed]
- De Aguiar, G.B.; Veiga, J.C.; Silva, J.M.; Conti, M.L. Spontaneous acute subdural hematoma: A rare presentation of a dural intracranial fistula. J. Clin. Neurosci. 2016, 25, 159–160. [Google Scholar] [CrossRef] [PubMed]
- Kohyama, S.; Ishihara, S.; Yamane, F.; Kanazawa, R.; Ishihara, H. Dural arteriovenous fistula presenting as an acute subdural hemorrhage that subsequently progressed to a chronic subdural hemorrhage: Case report. Minim. Invasive Neurosurg. 2009, 52, 36–38. [Google Scholar] [CrossRef] [PubMed]
- Duffau, H.; Lopes, M.; Janosevic, V.; Sichez, J.P.; Faillot, T.; Capelle, L.; Ismail, M.; Bitar, A.; Arthuis, F.; Fohanno, D. Early rebleeding from intracranial dural arteriovenous fistulas: Report of 20 cases and review of the literature. J. Neurosurg. 1999, 90, 78–84. [Google Scholar] [CrossRef]
- Kitazono, M.; Yamane, K.; Toyota, A.; Okita, S.; Kumano, K.; Hashimoto, N. A case of dural arteriovenous fistula associated with subcortical and subdural hemorrhage. No Shinkei Geka. Neurol. Surg. 2010, 38, 757–762. [Google Scholar]
- Saito, A.; Kawaguchi, T.; Sasaki, T.; Nishijima, M. A Case of Dural Arteriovenous Fistula Presenting as Acute Subdural Hematoma. Case Rep. Neurol. 2014, 6, 122–125. [Google Scholar] [CrossRef]
- Kominato, Y.; Matsui, K.; Hata, Y.; Matsui, K.; Kuwayama, N.; Ishizawa, S.; Takizawa, H. Acute subdural hematoma due to arteriovenous malformation primarily in dura mater: A case report. Leg. Med. 2004, 6, 256–260. [Google Scholar] [CrossRef]
- Paredes, I.; Martinez-Perez, R.; Munarriz, P.M.; Castaño-León, A.M.; Campollo, J.; Alén, J.F.; Lobato, R.D.; Lagares, A. Fístulas durales arteriovenosas intracraneales. Experiencia con 81 casos y revisión de la literatura. Neurocirugía 2013, 24, 141–151. [Google Scholar] [CrossRef] [PubMed]
- Hasumi, T.; Fukushima, T.; Haisa, T.; Yonemitsu, T.; Waragai, M. Focal dural arteriovenous fistula (DAVF) presenting with progressive cognitive impairment including amnesia and alexia. Intern. Med. 2007, 46, 1317–1320. [Google Scholar] [CrossRef] [PubMed]
- Van Munster, C.E.; van den Ber, R.; Weinstein, H.C. A Dural Fistula as a Treatable Cause of Cognitive Impairment. Neurohospitalist 2014, 4, 111–112. [Google Scholar] [CrossRef] [PubMed]
- Goncalves, M.B.; Maia, O., Jr.; Correa, J.L.; Siqueira, S.B.; Christoph Dde, H.; Landeiro, J.A. Dural arteriovenous fistula presenting as thalamic dementia. Arquivos de Neuro-Psiquiatria 2008, 66, 264–267. [Google Scholar] [CrossRef] [PubMed]
- Hurst, R.; Bagley, L.; Galetta, S.; Glosser, G.; Lieberman, A.; Trojanowski, J.; Sinson, G.; Stecker, M.; Zager, E.; Raps, E.; et al. Dementia resulting from dural arteriovenous fistulas: The pathologic findings of venous hypertensive encephalopathy. Am. J. Neuroradiol. 1998, 19, 1267–1273. [Google Scholar]
- Magot, A.; Desal, H.; Wiertlewski, S.; Houdart, E.; Vercelletto, M.; Al Hammad Ibrahim, M.; Guillon, B. Dural arteriovenous fistula. A rare cause of treatable dementia. Rev. Neurol. 2004, 160, 425–433. [Google Scholar] [CrossRef]
- Racine, C.A.; Lawton, M.T.; Hetts, S.W.; Josephson, S.A. Neuropyschological profile of reversible cognitive impairment in a patient with a dural arteriovenous fistula. Neurocase 2008, 14, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Yoshihara, T.; Kanazawa, R.; Maeshima, S.; Osawa, A.; Ochiai, I.; Uemiya, N.; Kohyama, S.; Yamane, F.; Ishihara, S. A case of curable dementia treated by effective endovascular embolization for dural arteriovenous fistula. Case Rep. Neurol. 2014, 6, 116–121. [Google Scholar] [CrossRef]
- Zenteno, M.; Lee, A.; Satyarthee, G.; Pinilla, G.; Agrawal, A.; Moscote-Salazar, L. Cognitive Improvement After Endovascular Treatment in a Case of Intracranial Dural Fistula With Concomitant Dementia. MAMC J. Med. Sci. 2018, 4, 32–37. [Google Scholar]
- Enofe, I.; Thacker, I.; Shamim, S. Dural arteriovenous fistula as a treatable dementia. Proc. (Bayl. Univ. Med. Cent.) 2017, 30, 215–217. [Google Scholar] [CrossRef]
- Fujii, H.; Nagano, Y.; Hosomi, N.; Matsumoto, M. Dural arteriovenous fistula presenting with progressive dementia and parkinsonism. BMJ Case Rep. 2014, 2014. [Google Scholar] [CrossRef]
- Martínez-Burbano, B.; Correa, E.P.; Sánchez, C.J. Evolutionary History of Multiple Dural Fistula. J. Investig. Med. High Impact Case Rep. 2016, 4, 1–11. [Google Scholar] [CrossRef]
- Matsuda, S.; Waragai, M.; Shinotoh, H.; Takahashi, N.; Takagi, K.; Hattori, T. Intracranial dural arteriovenous fistula (DAVF) presenting progressive dementia and parkinsonism. J. Neurol. Sci. 1999, 165, 43–47. [Google Scholar] [CrossRef]
- Pu, J.; Si, X.; Ye, R.; Zhang, B. Straight sinus dural arteriovenous fistula presenting with reversible parkinsonism A case report and literature review. Medicine 2017, 96, 49. [Google Scholar] [CrossRef] [PubMed]
- Soderman, M.; Pavic, L.; Edner, G.; Holmin, S.; Andersson, T. Natural history of dural arteriovenous shunts. Stroke 2008, 39, 1735–1739. [Google Scholar] [CrossRef]
- Xu, K.; Ji, T.; Li, C.; Yu, J. Current status of endovascular treatment for dural arteriovenous fistulae in the anterior cranial fossa: A systematic literature review. Int. J. Med. Sci. 2019, 16, 203–211. [Google Scholar] [CrossRef] [PubMed]
- Geraldes, R.; Albuquerque, L.; Ferro, J.M.; Sousa, R.; Sequeira, P.; Campos, J. Rapidly progressive cognitive impairment, ataxia, and myoclonus: An unusual presentation of a dural arteriovenous fistula. J. Stroke Cereb. Dis. 2012, 21, e613–e615. [Google Scholar] [CrossRef]
- Gopinath, M.; Nagesh, C.; Santhosh, K.; Jayadevan, E. Dementia and Parkinsonism-a Rare Presentation of Intracranial Dural Arteriovenous Fistulae. Neurointervention 2017, 12, 125–129. [Google Scholar] [CrossRef] [PubMed]
- Hattori, T.; Takeuchi, T.; Kabeya, R.; Ando, K.; Tosaki, F. Transverse-sigmoid sinus dural arteriovenous fistula presenting with parkinsonism. Neurol. Med. Chir. 2013, 53, 224–227. [Google Scholar] [CrossRef]
- Jagtap, S.A.; Nair, S.S.; Jain, N.; Nair, M.D. Rapidly progressive dementia, parkinsonism and myoclonus: An unusual presentation of dural arteriovenous fistula. Neurol. India 2014, 62, 107–110. [Google Scholar] [CrossRef]
- Netravathi, M.; Pal, P.K.; Bharath, R.D.; Ravishankar, S. Intracranial dural arteriovenous fistula presenting as parkinsonism and cognitive dysfunction. J. Clin. Neurosci. 2011, 18, 138–140. [Google Scholar] [CrossRef] [PubMed]
- Waragai, M.; Takeuchi, H.; Fukushima, T.; Haisa, T.; Yonemitsu, T. MRI and SPECT studies of dural arteriovenous fistulas presenting as pure progressive dementia with leukoencephalopathy: A cause of treatable dementia. Eur. J. Neurol. 2006, 13, 754–759. [Google Scholar] [CrossRef] [PubMed]
- Lou, Y.; Qi, J.; Cen, Z.; Hu, H.; Jiang, B.; Lou, W. Two cases of dural arteriovenous fistula presenting with parkinsonism and progressive cognitive dysfunction. J. Neurol. Sci. 2014, 343, 211–214. [Google Scholar]
- Chahbazian, K.; Theaudin, M.; Lehmann, P.; Sachet, M.; Adams, D.; Saliou, G. Reversible pseudo-Creutzfeldt-Jakob syndrome related to cerebral dural arteriovenous fistula. J. Am. Geriatr. Soc. 2014, 62, 2024–2026. [Google Scholar] [CrossRef] [PubMed]
- Morparia, N.; Miller, G.; Rabinstein, A.; Lanzino, G.; Kumar, N. Cognitive decline and hypersomnolence: Thalamic manifestations of a tentorial dural arteriovenous fistula (dAVF). Neurocrit. Care 2012, 17, 429–433. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.; Quiali, L.; Wanchao, S.; Zhiguo, S.; Yujun, Z.; Chen, L.; Zhenlin, L. Diagnosis and treatment of a dural arteriovenous fistula presenting with progressive parkinsonism and dementia: A case report and literature review. Exp. Ther. Med. 2015, 9, 523–526. [Google Scholar]
- Holekamp, T.F.; Mollman, M.E.; Murphy, R.K.; Kolar, G.R.; Kramer, N.M.; Derdeyn, C.P.; Moran, C.J.; Perrin, R.J.; Rich, K.M.; Lanzino, G.; et al. Dural arteriovenous fistula-induced thalamic dementia: Report of 4 cases. J. Neurosurg. 2016, 124, 1752–1765. [Google Scholar] [CrossRef] [PubMed]
- Greenough, G.P.; Mamourian, A.; Harbaugh, R.E. Venous Hypertension Associated with a Posterior Fossa Dural Arteriovenous Fistula: Another Cause of Bithalamic Lesions on MR Images. Am. J. Neuroradiol. 1999, 20, 145–147. [Google Scholar] [PubMed]
- Abrahams, J.M.; Bagley, L.J.; Flamm, E.S.; Hurst, R.W.; Sinson, G.P. Alternative management considerations for ethmoidal dural arteriovenous fistulas. Surg. Neurol. 2002, 58, 410–416. [Google Scholar] [CrossRef]
- Chan, H.; Cheng, K.; Lo, M.; Chan, C.; Cheung, Y. A treatable case of dementia intracranial dural arteriovenous fistula. Hong Kong Med. J. 2006, 12, 74–76. [Google Scholar]
- Kajitani, M.; Yagura, H.; Kawahara, M.; Hirano, M.; Ueno, S.; Fujimoto, K.; Sakaki, T.; Taoka, T.; Nakagawa, H.; Kichikawa, K. Treatable fluctuating Parkinsonism and dementia in a patient with a dural arteriovenous fistula. Mov. Disord. 2007, 22, 437–439. [Google Scholar] [CrossRef] [PubMed]
- Lv, X.; Li, Y.; Liu, A.; Lv, M.; Jiang, C.; Wu, Z. Endovascular embolization of dural arteriovenous fistulas of the anterior cranial fossa: Three case reports. Neurol. Res. 2008, 30, 852–859. [Google Scholar] [CrossRef]
- Nogueira, R.G.; Baccin, C.E.; Rabinov, J.D.; Pryor, J.C.; Buonanno, F.S.; Hirsch, J.A. Reversible parkinsonism after treatment of dural arteriovenous fistula. J. Neuroimaging 2009, 19, 183–184. [Google Scholar] [CrossRef]
- Wilson, M.; Doran, M.; Enevoldson, T.P.; Larner, A.J. Cognitive profiles associated with intracranial dural arteriovenous fistula. Age Ageing 2010, 39, 389–392. [Google Scholar] [CrossRef] [PubMed]
- Iwasawa, E.; Ishibashi, S.; Miki, K.; Yoshino, Y.; Nemoto, S.; Mizusawa, H. Teaching NeuroImages: Reversible cognitive impairment with bithalamic lesions caused by a dural arteriovenous fistula. Neurology 2013, 81, e38–e39. [Google Scholar] [CrossRef]
- Labeyrie, M.A.; Lenck, S.; Saint-Maurice, J.P.; Bresson, D.; Houdart, E. Dural arteriovenous fistulas presenting with reversible dementia are associated with a specific venous drainage. Eur. J. Neurol. 2014, 21, 545–547. [Google Scholar] [CrossRef]
- Pasi, M.; Nappini, S.; Salvadori, E.; Mangiafico, S.; Limbucci, N.; Pantoni, L. Rapidly progressive cognitive impairment in a patient with high flow dural arteriovenous fistulas, cerebral sinus thrombosis and protein S deficiency. J. Clin. Neurosci. 2014, 21, 1654–1656. [Google Scholar] [CrossRef] [PubMed]
- Imazeki, R.; Amari, K.; Sekiguchi, T.; Mochizuki, T.; Shimizu, S.; Yamamoto, M.; Takizawa, S.; Johkura, K. Rapidly progressive dementia caused by a superior sagittal sinus dural arteriovenous fistula: A case report. Tokai J. Exp. Clin. Med. 2015, 40, 22–26. [Google Scholar] [PubMed]
- Lai, J.; Heran, M.K.S.; Stoessl, A.J.; Gooderham, P.A. Reversible Parkinsonism and rapidly progressive dementia due to dural arteriovenous fistula: Case series and literature review. Mov. Disord. Clin. Pract. 2017, 4, 607–611. [Google Scholar] [CrossRef] [PubMed]
- Brito, A.; Tsang, A.C.O.; Hilditch, C.; Nicholson, P.; Krings, T.; Brinjikji, W. Intracranial Dural Arteriovenous Fistula as a Reversible Cause of Dementia: Case Series and Literature Review. World Neurosurg. 2019, 121, e543–e553. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Source | Total Patients | Cognitive Impairment | Dementia | Parkinsonism | Behavioral and Mood Changes | Time and Spatial Disorientation | Hemorrhage | Treatment | Evolution |
|---|---|---|---|---|---|---|---|---|---|
| Hurst et al., 1998 [26] | 40/5 | X | 4 ET 1 ET and S | 1 Death 4 Improved | |||||
| Matsuda S., et al., 1999 [34] | 3 | X | X | ET | 2 Improved 1 Not improved | ||||
| Greenough et al., 1999 [49] | 1 | X | S | Improved | |||||
| Abrahams., et al., 2002 [50] | 1 | X | ET | Improved | |||||
| Magot A., et al., 2004 [27] | 2 | X | X | ET | Improved | ||||
| Kwon., et al., 2005 [2] | 27/1 | X | X | ET | Improved | ||||
| Chan H Y., et al., 2006 [51] | 1 | X | X | X | X | X | ET | Improved | |
| Waragai M., et al., 2006 [43] | 2 | X | ET | Improved | |||||
| Kajitani M et al., 2007 [52] | 1 | X | X | X | ET | Improved | |||
| Hasumi T et al., 2007 [23] | 1 | X | X | ET | Improved | ||||
| Gonçalves MB et al., 2008 [25] | 1 | X | X | ET | Improved | ||||
| Racine CA, et al., 2008 [28] | 1 | X | ET and S | Improved | |||||
| Lv et al., 2008 [53] | 3/1 | X | ET | Improved | |||||
| Nogueira RG., et al., 2009 [54] | 1 | X | ET and S | Improved | |||||
| Wilson M, et al., 2010 [55] | 3 | X | ET | Improved | |||||
| Netravathi M, et al., 2011 [42] | 2 | X | X | ET | Not improved | ||||
| Geraldes et al., 2012 [38] | 1 | X | X | ET | Improved | ||||
| Morparia N.., et al., 2012 [46] | 1 | X | ET | Improved | |||||
| Hattori T., et al., 2013 [40] | 1 | X | X | ET | Improved | ||||
| Iwasawa E., et al., 2013 [56] | 1 | X | ET | Improved | |||||
| Jagtap SA., et al., 2014 [41] | 1 | X | X | NE | Death | ||||
| Labeyrie MA., et al., 2014 [57] | 45/8 | X | X | ET | Improved | ||||
| Chahbazian K., et al., 2014 [45] | 1 | X | X | ET | Improved | ||||
| van Munster CE., et al., 2014 [24] | 1 | X | X | ET | Improved | ||||
| Pasi M., et al., 2014 [58] | 1 | X | ET | Improved | |||||
| Fujii H., et al., 2014 [32] | 1 | X | X | ET | Improved | ||||
| Yoshihara., et al., 2014 [29] | 1 | X | X | X | ET | Improved | |||
| Imazeki R., et al., 2015 [59] | 1 | X | ET and S | Improved | |||||
| Chen MA., et al., 2015 [47] | 1 | X | X | ET and S | Improved | ||||
| Martínez Burbano, et al., 2016 [33] | 1 | X | X | X | NE | Death | |||
| Holekamp T F., et al., 2016 [48] | 4 | X | X | X | 2 ET 2 ET and S | 3 Improved 1 Death | |||
| Pu J., et al., 2017 [35] | 1 | X | X | ET | Improved | ||||
| Lai J., et al., 2017 [60] | 2 | X | X | X | ET | Improved | |||
| Gopinath M., et al., 2017 [39] | 1 | X | X | ET | Improved | ||||
| Enofe I., et al., 2017 [31] | 1 | X | ET | Improved | |||||
| Zenteno M., et al., 2018 [30] | 1 | X | X | ET | Improved | ||||
| Brito A., et al., 2019 [61] | 389/6 | X | ET | Improved | |||||
| Current case report 2019 | 1 | X | X | ET |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hernández-Díaz, Z.M.; Llíbre-Guerra, J.C.; Arteche-Prior, M.; de la Paz-Bermúdez, T.; Águila-Ruiz, A.F.; Figueroa-García, L.M.; Robinson-Agramonte, M.d.l.Á. Spontaneous Subdural Hematoma and Behavioral Changes Due to a Dural Arteriovenous Fistula. A Case Report and Literature Review. Behav. Sci. 2019, 9, 63. https://doi.org/10.3390/bs9060063
Hernández-Díaz ZM, Llíbre-Guerra JC, Arteche-Prior M, de la Paz-Bermúdez T, Águila-Ruiz AF, Figueroa-García LM, Robinson-Agramonte MdlÁ. Spontaneous Subdural Hematoma and Behavioral Changes Due to a Dural Arteriovenous Fistula. A Case Report and Literature Review. Behavioral Sciences. 2019; 9(6):63. https://doi.org/10.3390/bs9060063
Chicago/Turabian StyleHernández-Díaz, Zenaida Milagros, Juan Carlos Llíbre-Guerra, Marianela Arteche-Prior, Tania de la Paz-Bermúdez, Angel Francisco Águila-Ruiz, Luisa María Figueroa-García, and María de los Ángeles Robinson-Agramonte. 2019. "Spontaneous Subdural Hematoma and Behavioral Changes Due to a Dural Arteriovenous Fistula. A Case Report and Literature Review" Behavioral Sciences 9, no. 6: 63. https://doi.org/10.3390/bs9060063
APA StyleHernández-Díaz, Z. M., Llíbre-Guerra, J. C., Arteche-Prior, M., de la Paz-Bermúdez, T., Águila-Ruiz, A. F., Figueroa-García, L. M., & Robinson-Agramonte, M. d. l. Á. (2019). Spontaneous Subdural Hematoma and Behavioral Changes Due to a Dural Arteriovenous Fistula. A Case Report and Literature Review. Behavioral Sciences, 9(6), 63. https://doi.org/10.3390/bs9060063