Meditation-Induced States, Vagal Tone, and Breathing Activity Are Related to Changes in Auditory Temporal Integration



Abstract
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants
2.3. Apparatus and Physiological Recordings
2.4. Instruments
2.4.1. Freiburg Mindfulness Inventory-14 (FMI-14)
2.4.2. Metronome Task
2.4.3. Interventions
2.5. Procedure
2.6. Data Reduction, Statistical Approach
2.7. Outlier Analysis
3. Results
3.1. Sample Description
3.2. Descriptive Analysis
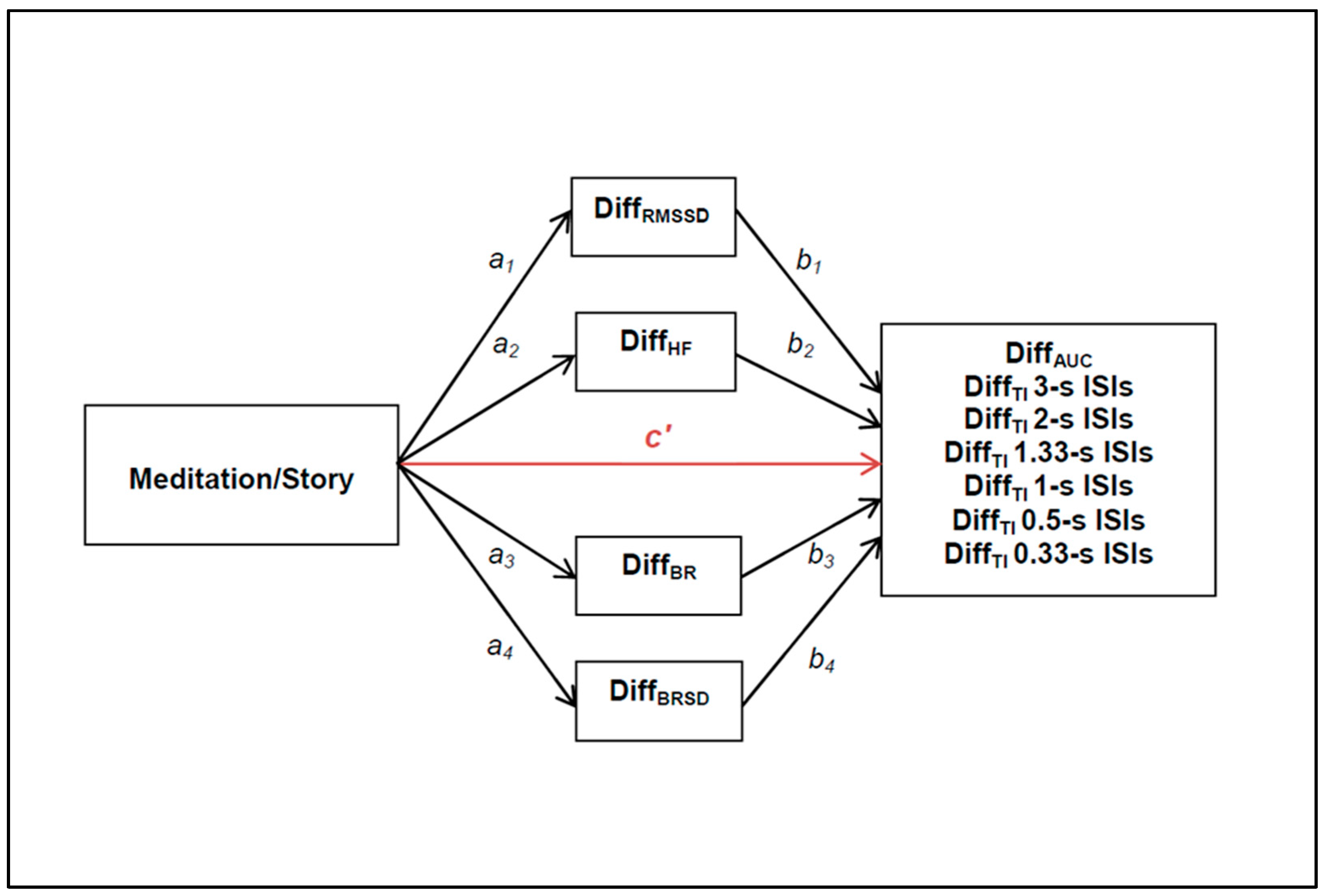
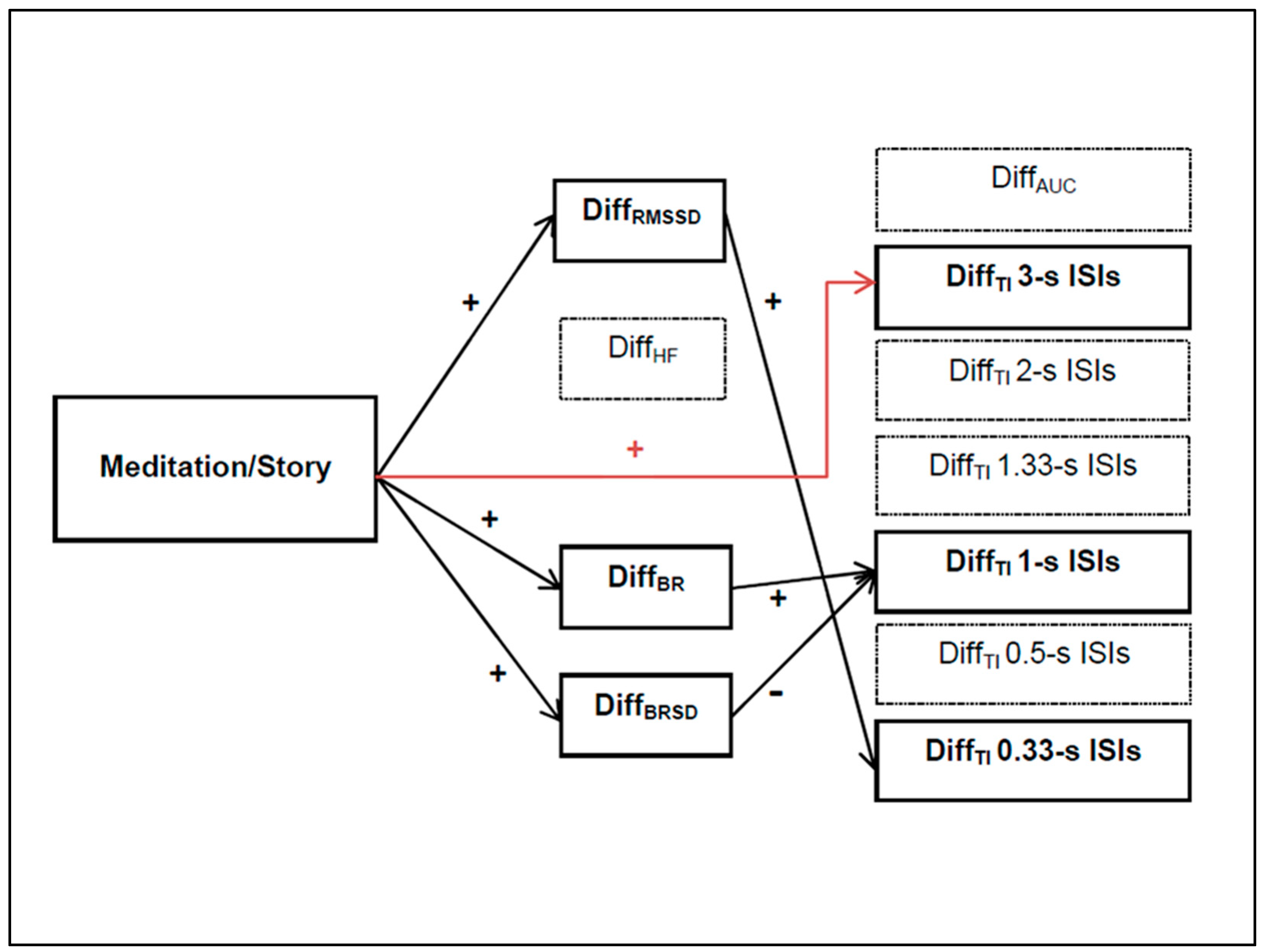
3.3. Mediation Analysis
3.4. Relationship Between Trait-mindfulness and the Metronome Task
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Integrated Beats | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
|---|---|---|---|---|---|---|---|---|
| ISI = 3 s | 0 s | 3 s | 6 s (excluded) | excluded | excluded | excluded | excluded | excluded |
| ISI = 2 s | 0 s | 2 s | 4 s (excluded) | excluded | excluded | excluded | excluded | excluded |
| ISI = 1.333 s | 0 s | 1.33 s | 2.66 s | 3.99 s (excluded) | excluded | excluded | excluded | excluded |
| ISI = 1 s | 0 s | 1 s | 2 s | 3 s | 4 s (excluded) | excluded | excluded | excluded |
| ISI = 0.5 s | 0 s | 0.5 s | 1 s | 1.5 s | 2 s | 2.5 s | 3 s | 3.5 s (excluded) |
| ISI = 0.333 s | 0 s | 0.33 s | 0.66 s | 0.99 s | 1.33 s | 1.665 s | 1.99 s | 2.33 s |
| ISI | > 3 s Criterion | > 8 Criterion | SUM (Both Criteria) | % of Trials |
|---|---|---|---|---|
| 0.333 | 0 | 4 | 4 | 0.53 |
| 0.5 | 93 | 2 | 95 | 12.63 |
| 1 | 29 | 1 | 30 | 3.98 |
| 1.333 | 201 | 0 | 201 | 26.72 |
| 2 | 164 | 0 | 164 | 21.80 |
| 3 | 93 | 0 | 93 | 12.36 |
| 580 | 7 | 587 | 13.01 | |
| % of trials | 12.86 | 0.15 | 13.01 |
| Grouping | % of Trials | Peak ISI |
|---|---|---|
| 1 | 18.54 | 3 |
| 2 | 35.44 | 1.333 |
| 3 | 8.58 | 0.5 |
| 4 | 27.70 | 0.5 |
| 5 | 0.95 | 0.333 |
| 6 | 1.62 | 0.333 |
| 7 | 0.53 | 0.333 |
| 8 | 6.48 | 0.333 |
| >8 | 0.16 | 0.33 |


References
- Craig, A.D.B. Emotional moments across time: A possible neural basis for time perception in the anterior insula. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2009, 364, 1933–1942. [Google Scholar] [CrossRef] [PubMed]
- Craig, A.D. How Do You Feel?: An Interoceptive Moment with Your Neurobiological Self; Princeton University Press: Princeton, NJ, USA, 2015; ISBN 978-0-691-15676-7. [Google Scholar]
- Wittmann, M. The inner experience of time. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2009, 364, 1955–1967. [Google Scholar] [CrossRef]
- Wittmann, M. The inner sense of time: How the brain creates a representation of duration. Nat. Rev. Neurosci. 2013, 14, 217–223. [Google Scholar] [CrossRef]
- Droit-Volet, S.; Fayolle, S.; Lamotte, M.; Gil, S. Time, Emotion and the Embodiment of Timing. Timing Time Percept. 2013, 1, 99–126. [Google Scholar] [CrossRef]
- Critchley, H.D.; Wiens, S.; Rotshtein, P.; Ohman, A.; Dolan, R.J. Neural systems supporting interoceptive awareness. Nat. Neurosci. 2004, 7, 189–195. [Google Scholar] [CrossRef]
- Kabat-Zinn, J. An outpatient program in behavioral medicine for chronic pain patients based on the practice of mindfulness meditation: Theoretical considerations and preliminary results. Gen. Hosp. Psychiatry 1982, 4, 33–47. [Google Scholar] [CrossRef]
- Marlatt, G.A.; Kristeller, J.L. Mindfulness and meditation. In Integrating Spirituality into Treatment: Resources for Practitioners; American Psychological Association: Washington, DC, USA, 1999; pp. 67–84. ISBN 978-1-55798-581-1. [Google Scholar]
- Hölzel, B.K.; Lazar, S.W.; Gard, T.; Schuman-Olivier, Z.; Vago, D.R.; Ott, U. How Does Mindfulness Meditation Work? Proposing Mechanisms of Action from a Conceptual and Neural Perspective. Perspect. Psychol. Sci. J. Assoc. Psychol. Sci. 2011, 6, 537–559. [Google Scholar] [CrossRef]
- Tang, Y.-Y.; Hölzel, B.K.; Posner, M.I. The neuroscience of mindfulness meditation. Nat. Rev. Neurosci. 2015, 16, 213–225. [Google Scholar] [CrossRef] [PubMed]
- Wittmann, M.; Schmidt, S. Mindfulness meditation and the experience of time. In Meditation-Neuroscientific Approaches and Philosophical Implications; Studies in Neuroscience, Consciousness and Spirituality; Springer International Publishing: Cham, Switzerland, 2014; pp. 199–209. ISBN 978-3-319-01633-7. [Google Scholar]
- Kabat-Zinn, J. Coming to Our Senses: Healing Ourselves and the World through Mindfulness; Hyperion: New York, NY, USA, 2005; ISBN 978-0-7499-2588-8. [Google Scholar]
- Wittmann, M.; Otten, S.; Schötz, E.; Sarikaya, A.; Lehnen, H.; Jo, H.-G.; Kohls, N.; Schmidt, S.; Meissner, K. Subjective expansion of extended time-spans in experienced meditators. Front. Psychol. 2015, 5, 1586. [Google Scholar] [CrossRef] [PubMed]
- Wittmann, M. Modulations of the experience of self and time. Conscious. Cogn. 2015, 38, 172–181. [Google Scholar] [PubMed]
- Sauer, S.; Lemke, J.; Wittmann, M.; Kohls, N.; Mochty, U.; Walach, H. How long is now for mindfulness meditators? Personal. Individ. Differ. 2012, 52, 750–754. [Google Scholar] [CrossRef]
- Kornmeier, J.; Friedel, E.; Wittmann, M.; Atmanspacher, H. EEG correlates of cognitive time scales in the Necker-Zeno model for bistable perception. Conscious. Cogn. 2017, 53, 136–150. [Google Scholar] [CrossRef]
- Pöppel, E. Pre-semantically defined temporal windows for cognitive processing. Philos. Trans. R. Soc. B Biol. Sci. 2009, 364, 1887–1896. [Google Scholar] [CrossRef]
- Montemayor, C.; Wittmann, M. The Varieties of Presence: Hierarchical Levels of Temporal Integration. Timing Time Percept. 2014, 2, 325–338. [Google Scholar] [CrossRef]
- White, P.A. The three-second “subjective present”: A critical review and a new proposal. Psychol. Bull. 2017, 143, 735–756. [Google Scholar] [CrossRef]
- Varela, F.J. Present-Time Consciousness. J. Conscious. Stud. 1999, 6, 111–140. [Google Scholar]
- Wernery, J.; Atmanspacher, H.; Kornmeier, J.; Candia, V.; Folkers, G.; Wittmann, M. Temporal Processing in Bistable Perception of the Necker Cube. Perception 2015, 44, 157–168. [Google Scholar] [CrossRef] [PubMed]
- Carter, O.L.; Presti, D.E.; Callistemon, C.; Ungerer, Y.; Liu, G.B.; Pettigrew, J.D. Meditation alters perceptual rivalry in Tibetan Buddhist monks. Curr. Biol. 2005, 15, R412–R413. [Google Scholar] [CrossRef]
- Berkovich-Ohana, A.; Glicksohn, J.; Goldstein, A. Mindfulness-induced changes in gamma band activity—Implications for the default mode network, self-reference and attention. Clin. Neurophysiol. 2012, 123, 700–710. [Google Scholar] [CrossRef] [PubMed]
- Lutz, A.; Jha, A.P.; Dunne, J.D.; Saron, C.D. Investigating the Phenomenological Matrix of Mindfulness-related Practices from a Neurocognitive Perspective. Am. Psychol. 2015, 70, 632–658. [Google Scholar] [CrossRef]
- Kramer, R.S.S.; Weger, U.W.; Sharma, D. The effect of mindfulness meditation on time perception. Conscious. Cogn. 2013, 22, 846–852. [Google Scholar] [CrossRef] [PubMed]
- Droit-Volet, S.; Fanget, M.; Dambrun, M. Mindfulness meditation and relaxation training increases time sensitivity. Conscious. Cogn. 2015, 31, 86–97. [Google Scholar] [CrossRef]
- Brochard, R.; Abecasis, D.; Potter, D.; Ragot, R.; Drake, C. The “ticktock” of our internal clock: Direct brain evidence of subjective accents in isochronous sequences. Psychol. Sci. 2003, 14, 362–366. [Google Scholar] [CrossRef] [PubMed]
- Szelag, E. Temporal Integration of the Brain as Studied with the Metronome Paradigm. In Time, Temporality, Now: Experiencing Time and Concepts of Time in an Interdisciplinary Perspective; Atmanspacher, H., Ruhnau, E., Eds.; Springer: Berlin/Heidelberg, Germany, 1997; pp. 121–131. ISBN 978-3-642-60707-3. [Google Scholar]
- Van Noorden, L.; Moelants, D. Resonance in the Perception of Musical Pulse. J. New Music Res. 1999, 28, 43–66. [Google Scholar] [CrossRef]
- Fraisse, P. 6—Rhythm and Tempo. In Psychology of Music; Deutsch, D., Ed.; Cognition and Perception; Academic Press: San Diego, CA, USA, 1982; pp. 149–180. ISBN 978-0-12-213562-0. [Google Scholar]
- Arnling Bååth, R. Subjective rhythmization: A replication and an assessment of two theoretical explanations. Music Percept. 2015, 33, 244–254. [Google Scholar] [CrossRef]
- Szelag, E.; von Steinbüchel, N.; Reiser, M.; Gilles de Langen, E.; Pöppel, E. Temporal constraints in processing of nonverbal rhythmic patterns. Acta Neurobiol. Exp. 1996, 56, 215–225. [Google Scholar]
- Szelag, E.; von Steinbüchel, N.; Pöppel, E. Temporal processing disorders in patients with Broca’s aphasia. Neurosci. Lett. 1997, 235, 33–36. [Google Scholar] [CrossRef]
- Von Steinbüchel, N.; Wittmann, M.; Strasburger, H.; Szelag, E. Auditory temporal-order judgement is impaired in patients with cortical lesions in posterior regions of the left hemisphere. Neurosci. Lett. 1999, 264, 168–171. [Google Scholar] [CrossRef]
- Wittmann, M. Moments in time. Front. Integr. Neurosci. 2011, 5, 66. [Google Scholar] [CrossRef]
- Pöppel, E. A hierarchical model of temporal perception. Trends Cogn. Sci. 1997, 1, 56–61. [Google Scholar] [CrossRef]
- Lutz, A.; Dunne, J.D.; Davidson, R.J. Meditation and the Neuroscience of Consciousness. In Cambridge Handbook of Consciousness; Zelazo, P.D., Moscovitch, M., Thompson, E., Eds.; Cambridge University Press: Cambridge, UK, 2007; pp. 19–497. [Google Scholar]
- Marchand, W.R. Neural mechanisms of mindfulness and meditation: Evidence from neuroimaging studies. World J. Radiol. 2014, 6, 471–479. [Google Scholar] [CrossRef]
- Farb, N.A.S.; Segal, Z.V.; Mayberg, H.; Bean, J.; McKeon, D.; Fatima, Z.; Anderson, A.K. Attending to the present: Mindfulness meditation reveals distinct neural modes of self-reference. Soc. Cogn. Affect. Neurosci. 2007, 2, 313–322. [Google Scholar] [CrossRef]
- Fox, K.C.R.; Dixon, M.L.; Nijeboer, S.; Girn, M.; Floman, J.L.; Lifshitz, M.; Ellamil, M.; Sedlmeier, P.; Christoff, K. Functional neuroanatomy of meditation: A review and meta-analysis of 78 functional neuroimaging investigations. Neurosci. Biobehav. Rev. 2016, 65, 208–228. [Google Scholar] [CrossRef] [PubMed]
- Wittmann, M.; Simmons, A.N.; Aron, J.L.; Paulus, M.P. Accumulation of neural activity in the posterior insula encodes the passage of time. Neuropsychologia 2010, 48, 3110–3120. [Google Scholar] [CrossRef]
- Meissner, K.; Wittmann, M. Body signals, cardiac awareness, and the perception of time. Biol. Psychol. 2011, 86, 289–297. [Google Scholar] [CrossRef] [PubMed]
- Cellini, N.; Mioni, G.; Levorato, I.; Grondin, S.; Stablum, F.; Sarlo, M. Heart rate variability helps tracking time more accurately. Brain Cogn. 2015, 101, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Walach, H.; Buchheld, N.; Buttenmüller, V.; Kleinknecht, N.; Schmidt, S. Measuring mindfulness—The Freiburg Mindfulness Inventory (FMI). Personal. Individ. Differ. 2006, 40, 1543–1555. [Google Scholar] [CrossRef]
- Sauer, S.; Walach, H.; Offenbächer, M.; Lynch, S.; Kohls, N. Measuring Mindfulness: A Rasch Analysis of the Freiburg Mindfulness Inventory. Religions 2011, 2, 693–706. [Google Scholar] [CrossRef]
- Sauer, S.; Walach, H.; Schmidt, S.; Hinterberger, T.; Lynch, S.; Büssing, A.; Kohls, N. Assessment of Mindfulness: Review on State of the Art. Mindfulness 2013, 4, 3–17. [Google Scholar] [CrossRef]
- Kabat-Zinn, J.; Kesper-Grossman, U. Die Heilende Kraft der Achtsamkeit; Arbor Verlag: Freiamt im Schwarzwald, Germany, 2004. [Google Scholar]
- Kabat-Zinn, J. Achtsamkeit und Meditation im Täglichen Leben; Arbor Verlag: Freiamt im Schwarzwald, Germany, 2007. [Google Scholar]
- Bakker, G. Der Umweg; Jumbo Neue Medien und Verlag: Hamburg, Germany, 2012. [Google Scholar]
- Leon, D. Mein Venedig; Diogenes Verlag: Zürich, Switzerland, 2005. [Google Scholar]
- Mazzantini, M. Das Meer am Morgen; Jumbo Neue Medien und Verlag: Hamburg, Germany, 2012. [Google Scholar]
- Tarvainen, M.P.; Ranta-aho, P.O.; Karjalainen, P.A. An advanced detrending method with application to HRV analysis. IEEE Trans. Biomed. Eng. 2002, 49, 172–175. [Google Scholar] [CrossRef] [PubMed]
- Laborde, S.; Mosley, E.; Thayer, J.F. Heart Rate Variability and Cardiac Vagal Tone in Psychophysiological Research—Recommendations for Experiment Planning, Data Analysis, and Data Reporting. Front. Psychol. 2017, 8, 213. [Google Scholar] [CrossRef] [PubMed]
- Friedman, B.H.; Allen, M.T.; Christie, I.C.; Santucci, A.K. Validity concerns of common heart-rate variability indices. IEEE Eng. Med. Biol. Mag. 2002, 21, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Kleiger, R.E.; Stein, P.K.; Bigger, J.T. Heart rate variability: Measurement and clinical utility. Ann. Noninvasive Electrocardiol. 2005, 10, 88–101. [Google Scholar] [CrossRef] [PubMed]
- Luft, C.D.B.; Takase, E.; Darby, D. Heart rate variability and cognitive function: Effects of physical effort. Biol. Psychol. 2009, 82, 164–168. [Google Scholar] [CrossRef]
- Khandoker, A.H.; Karmakar, C.; Brennan, M.; Palaniswami, M.; Voss, A. Poincaré Plot Methods for Heart Rate Variability Analysis; Springer: New York, NY, USA, 2013; ISBN 978-1-4614-7374-9. [Google Scholar]
- Shaffer, F.; Ginsberg, J.P. An Overview of Heart Rate Variability Metrics and Norms. Front. Public Health 2017, 5, 258. [Google Scholar] [CrossRef] [PubMed]
- Hill, L.K.; Siebenbrock, A. Are all measures created equal? Heart rate variability and respiration. Biomed. Sci. Instrum. 2009, 45, 71–76. [Google Scholar]
- Penttilä, J.; Helminen, A.; Jartti, T.; Kuusela, T.; Huikuri, H.V.; Tulppo, M.P.; Coffeng, R.; Scheinin, H. Time domain, geometrical and frequency domain analysis of cardiac vagal outflow: Effects of various respiratory patterns. Clin. Physiol. 2001, 21, 365–376. [Google Scholar] [CrossRef] [PubMed]
- Malik, M.; Bigger, J.T.; Camm, A.J.; Kleiger, R.E.; Malliani, A.; Moss, A.J.; Schwartz, P.J. Heart rate variabilityStandards of measurement, physiological interpretation, and clinical use. Eur. Heart J. 1996, 17, 354–381. [Google Scholar] [CrossRef]
- Berntson, G.G.; Bigger, J.T.; Eckberg, D.L.; Grossman, P.; Kaufmann, P.G.; Malik, M.; Nagaraja, H.N.; Porges, S.W.; Saul, J.P.; Stone, P.H.; et al. Heart rate variability: Origins, methods, and interpretive caveats. Psychophysiology 1997, 34, 623–648. [Google Scholar] [CrossRef] [PubMed]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford Press: New York, NY, USA, 2013; ISBN 978-1-60918-230-4. [Google Scholar]
- Preacher, K.J.; Hayes, A.F. SPSS and SAS procedures for estimating indirect effects in simple mediation models. Behav. Res. Methods Instrum. Comput. 2004, 36, 717–731. [Google Scholar] [CrossRef]
- MacKinnon, D.P.; Lockwood, C.M.; Williams, J. Confidence Limits for the Indirect Effect: Distribution of the Product and Resampling Methods. Multivar. Behav. Res. 2004, 39, 99. [Google Scholar] [CrossRef] [PubMed]
- Baron, R.M.; Kenny, D.A. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Pers. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef] [PubMed]
- Shrout, P.E.; Bolger, N. Mediation in experimental and nonexperimental studies: New procedures and recommendations. Psychol. Methods 2002, 7, 422–445. [Google Scholar] [CrossRef] [PubMed]
- Holmbeck, G.N. Toward terminological, conceptual, and statistical clarity in the study of mediators and moderators: Examples from the child-clinical and pediatric psychology literatures. J. Consult. Clin. Psychol. 1997, 65, 599–610. [Google Scholar] [CrossRef] [PubMed]
- Preacher, K.J.; Hayes, A.F. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav. Res. Methods 2008, 40, 879–891. [Google Scholar] [CrossRef]
- Vos, P.G. Waarneming van Metrische Toon Reeksen; Nijmegen: Nijmegen, The Netherlands, 1973. [Google Scholar]
- Parncutt, R. A Perceptual Model of Pulse Salience and Metrical Accent in Musical Rhythms. Music Percept. Interdiscip. J. 1994, 11, 409–464. [Google Scholar] [CrossRef]
- Arstila, V.; Lloyd, D. Subjective Time: The Philosophy, Psychology, and Neuroscience of Temporality; MIT Press: Cambridge, MA, USA, 2014; ISBN 978-0-262-01994-1. [Google Scholar]
- Berkovich-Ohana, A.; Wittmann, M. A typology of altered states according to the consciousness state space (CSS) model: A special reference to subjective time. J. Conscious. Stud. 2017, 24, 37–61. [Google Scholar]
- Pollatos, O.; Laubrock, J.; Wittmann, M. Interoceptive Focus Shapes the Experience of Time. PLoS ONE 2014, 9, e86934. [Google Scholar] [CrossRef]
- Thayer, J.F.; Lane, R.D. A model of neurovisceral integration in emotion regulation and dysregulation. J. Affect. Disord. 2000, 61, 201–216. [Google Scholar] [CrossRef]
- Thayer, J.F.; Lane, R.D. Claude Bernard and the heart-brain connection: Further elaboration of a model of neurovisceral integration. Neurosci. Biobehav. Rev. 2009, 33, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Thayer, J.F.; Ahs, F.; Fredrikson, M.; Sollers, J.J.; Wager, T.D. A meta-analysis of heart rate variability and neuroimaging studies: Implications for heart rate variability as a marker of stress and health. Neurosci. Biobehav. Rev. 2012, 36, 747–756. [Google Scholar] [CrossRef]
- Hansen, A.L.; Johnsen, B.H.; Thayer, J.F. Vagal influence on working memory and attention. Int. J. Psychophysiol. Psychophysiol. 2003, 48, 263–274. [Google Scholar] [CrossRef]
- Thompson, E. Waking, Dreaming, Being: Self and Consciousness in Neuroscience, Meditation, and Philosophy; Columbia University Press: New York, NY, USA, 2014; ISBN 978-0-231-53831-2. [Google Scholar]
- Wittmann, M. Altered States of Consciousness: Experiences Out of Time and Self; MIT Press: Cambridge, MA, USA, 2018; ISBN 978-0-262-03831-7. [Google Scholar]


| Variable | Meditation Group (n = 41) | Story Group (n = 43) | p-Value a |
|---|---|---|---|
| Age (mean ± SD) | 25 ± 3.7 | 25 ± 3.4 | 0.937 |
| Gender (female (%)) | 25 (29.8) | 25 (29.8) | 0.791 b |
| Educational level | 0.953 b | ||
| Secondary school (n (%)) | 1 (1.2) | 1 (1.2) | |
| High school (n (%)) | 27 (32.1) | 27 (32.1) | |
| University degree (n (%)) | 13 (15.5) | 15 (17.9) | |
| Meditation experience (mean ± SD) | 223 ± 511 | 218 ± 484 | 0.963 |
| Trait-mindfulness (FMI) | |||
| Acceptance (mean ± SD) | 24 ± 3.4 | 23 ± 2.6 | 0.204 |
| Presence (mean ± SD) | 19 ± 4.2 | 18 ± 2.1 | 0.203 |
| Sum (mean ± SD) | 42 ± 4.8 | 41 ± 3.9 | 0.213 |
| Variable | Meditation Group (n = 41) | Story Group (n = 43) | p-Value |
|---|---|---|---|
| Resting RMSSD (mean ± SD) | 36.8 ± 22.6 | 35.4 ± 22.3 | 0.774 |
| Resting HF (mean ± SD) | 48.7 ± 19.8 | 48.4 ± 21 | 0.950 |
| Resting BR (mean ± SD) | 4.3 ± 0.86 | 4.2 ± 0.96 | 0.692 |
| Resting BRSD (mean ± SD) | 0.90 ± 0.47 | 0.98 ± 0.56 | 0.480 |
| Intervention RMSSD (mean ± SD) | 48.4 ± 33.7 | 38.9 ± 23.3 | 0.139 |
| Intervention HF (mean ± SD) | 41.1 ± 21.3 | 35.9 ± 17.9 | 0.263 |
| Intervention BR (mean ± SD) | 5.1 ± 1 | 4.1 ± 0.88 | 0.000 *** |
| Intervention BRSD (mean ± SD) | 1.4 ± 0.65 | 1.1 ± 0.62 | 0.006 ** |
| Diff. RMSSD (mean ± SD) | 11.4 ± 18.3 | 3.4 ± 11.8 | 0.019 * |
| Diff. HF (mean ± SD) | −7.5 ± 26.3 | −9.1 ± 24.7 | 0.798 |
| Diff. BR (mean ± SD) | 0.73 ± 0.81 | −0.17 ± 0.69 | 0.000 *** |
| Diff. BRSD (mean ± SD) | 0.50 ± 0.55 | 0.03 ± 0.46 | 0.000 *** |
| X Independent Variable | M Diff Mediating Variables | Y Diff Dependent Variables | Effect of X→M (a) | Effect of M→Y (b) | Specific Indirect Effects (a, b) | Direct Effect X→Y (c’) | Total Effect (c) | Type of Effect |
|---|---|---|---|---|---|---|---|---|
| RMSSD | Area under the curve AUC | 8.59 * | −0.00 | −0.00 | 0.04 | 0.01 | none | |
| HF | 1.56 | 0.00 | 0.00 | |||||
| BR mean | 0.80 *** | 0.07 | 0.06 | |||||
| BR SD | 0.49 *** | −0.19 | −0.09 | |||||
| Meditation vs. Story | RMSSD | Integration interval at 3 s ISI | 8.87 * | −0.00 | −0.05 | 0.21 * | 0.06 | Direct effect |
| HF | 3.02 | 0.00 | 0.00 | |||||
| BR mean | 0.77 *** | −0.12 | −0.09 | |||||
| BR SD | 0.45 *** | −0.01 | −0.00 | |||||
| RMSSD | Integration interval at 2 s ISI | 8.31 * | 0.00 | 0.01 | −0.11 | −0.06 | none | |
| HF | 0.57 | 0.00 | 0.00 | |||||
| BR mean | 0.82 *** | 0.03 | 0.02 | |||||
| BR SD | 0.50 *** | 0.01 | 0.01 | |||||
| RMSSD | Integration interval at 1.33 s ISI | 9.67 * | 0.00 | 0.01 | −0.01 | 0.01 | none | |
| HF | −1.86 | −0.00 | 0.00 | |||||
| BR mean | 0.75 *** | 0.03 | 0.01 | |||||
| BR SD | 0.53 *** | −0.00 | −0.00 | |||||
| RMSSD | Integration interval at 1 s ISIs | 8.68 * | −0.00 | −0.00 | 0.00 | −0.01 | Indirect effect | |
| HF | −1.00 | −0.00 * | 0.00 | |||||
| BR mean | 0.77 *** | 0.17 *** | 0.13 * | |||||
| BR SD | 0.49 *** | −0.29 ** | −0.14 * | |||||
| RMSSD | Integration interval at 0.5 s ISIs | 9.68 * | 0.00 | −0.00 | 0.05 | 0.03 | none | |
| HF | 1.95 | 0.00 | 0.00 | |||||
| BR mean | 0.77 *** | 0.00 | 0.00 | |||||
| BR SD | 0.48 *** | −0.06 | −0.02 | |||||
| RMSSD | Integration interval at 0.33 s ISIs | 8.73 * | 0.00 * | 0.01 * | 0.00 | −0.00 | Indirect effect | |
| HF | 1.92 | 0.00 | 0.00 | |||||
| BR mean | 0.79 *** | 0.00 | 0.00 | |||||
| BR SD | 0.48 *** | −0.06 | −0.03 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Linares Gutierrez, D.; Kübel, S.; Giersch, A.; Schmidt, S.; Meissner, K.; Wittmann, M. Meditation-Induced States, Vagal Tone, and Breathing Activity Are Related to Changes in Auditory Temporal Integration. Behav. Sci. 2019, 9, 51. https://doi.org/10.3390/bs9050051
Linares Gutierrez D, Kübel S, Giersch A, Schmidt S, Meissner K, Wittmann M. Meditation-Induced States, Vagal Tone, and Breathing Activity Are Related to Changes in Auditory Temporal Integration. Behavioral Sciences. 2019; 9(5):51. https://doi.org/10.3390/bs9050051
Chicago/Turabian StyleLinares Gutierrez, Damisela, Sebastian Kübel, Anne Giersch, Stefan Schmidt, Karin Meissner, and Marc Wittmann. 2019. "Meditation-Induced States, Vagal Tone, and Breathing Activity Are Related to Changes in Auditory Temporal Integration" Behavioral Sciences 9, no. 5: 51. https://doi.org/10.3390/bs9050051
APA StyleLinares Gutierrez, D., Kübel, S., Giersch, A., Schmidt, S., Meissner, K., & Wittmann, M. (2019). Meditation-Induced States, Vagal Tone, and Breathing Activity Are Related to Changes in Auditory Temporal Integration. Behavioral Sciences, 9(5), 51. https://doi.org/10.3390/bs9050051