Virtual-Reality-Induced Visual Perturbations Impact Postural Control System Behavior

 ,
,  ,
,  , and
, and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
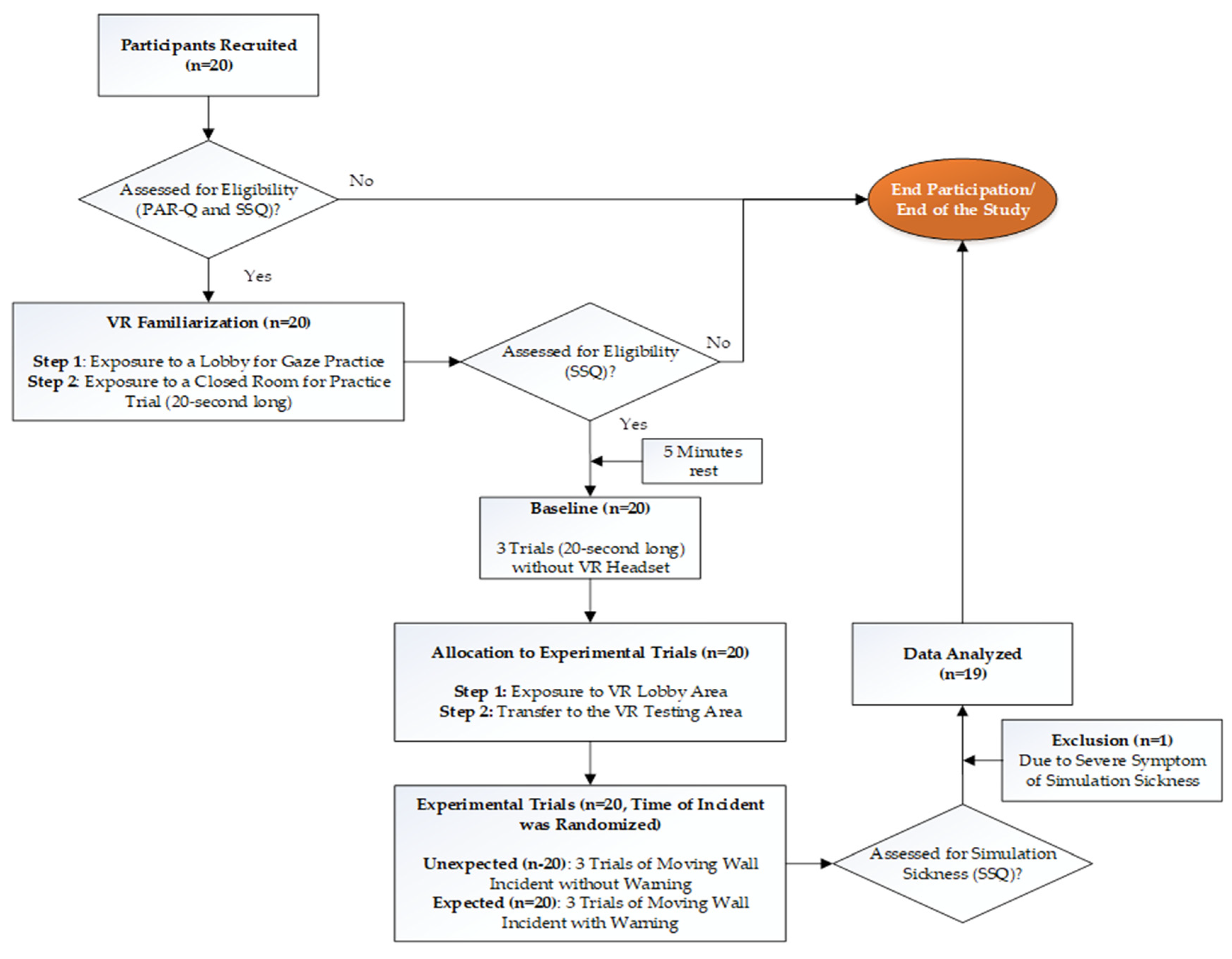
2. Materials and Methods
2.1. Participants
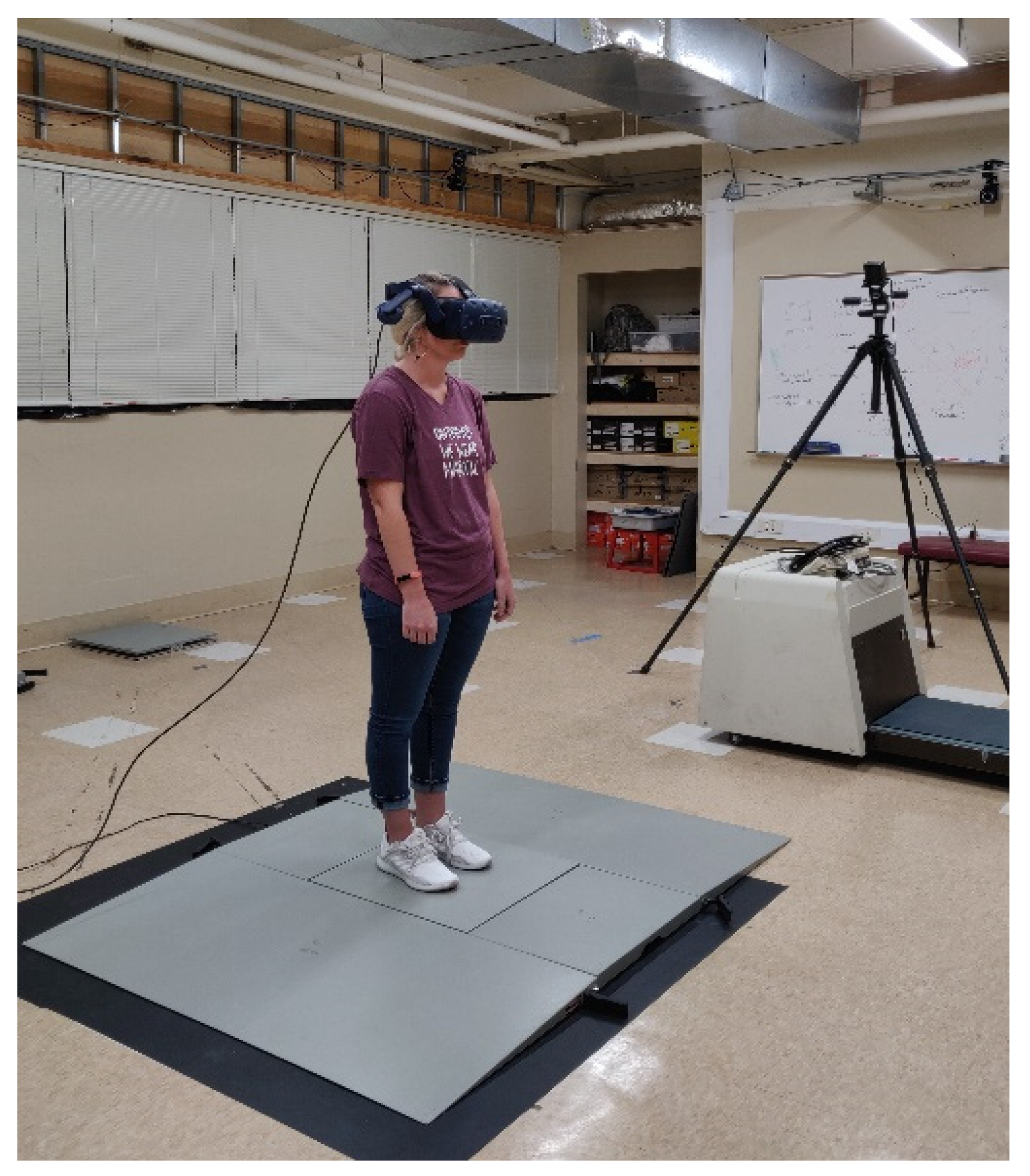
2.2. Instrumentation
2.3. Study Design
2.4. Experimental Procedures
2.5. Data Analyses
2.6. Statistical Analyses
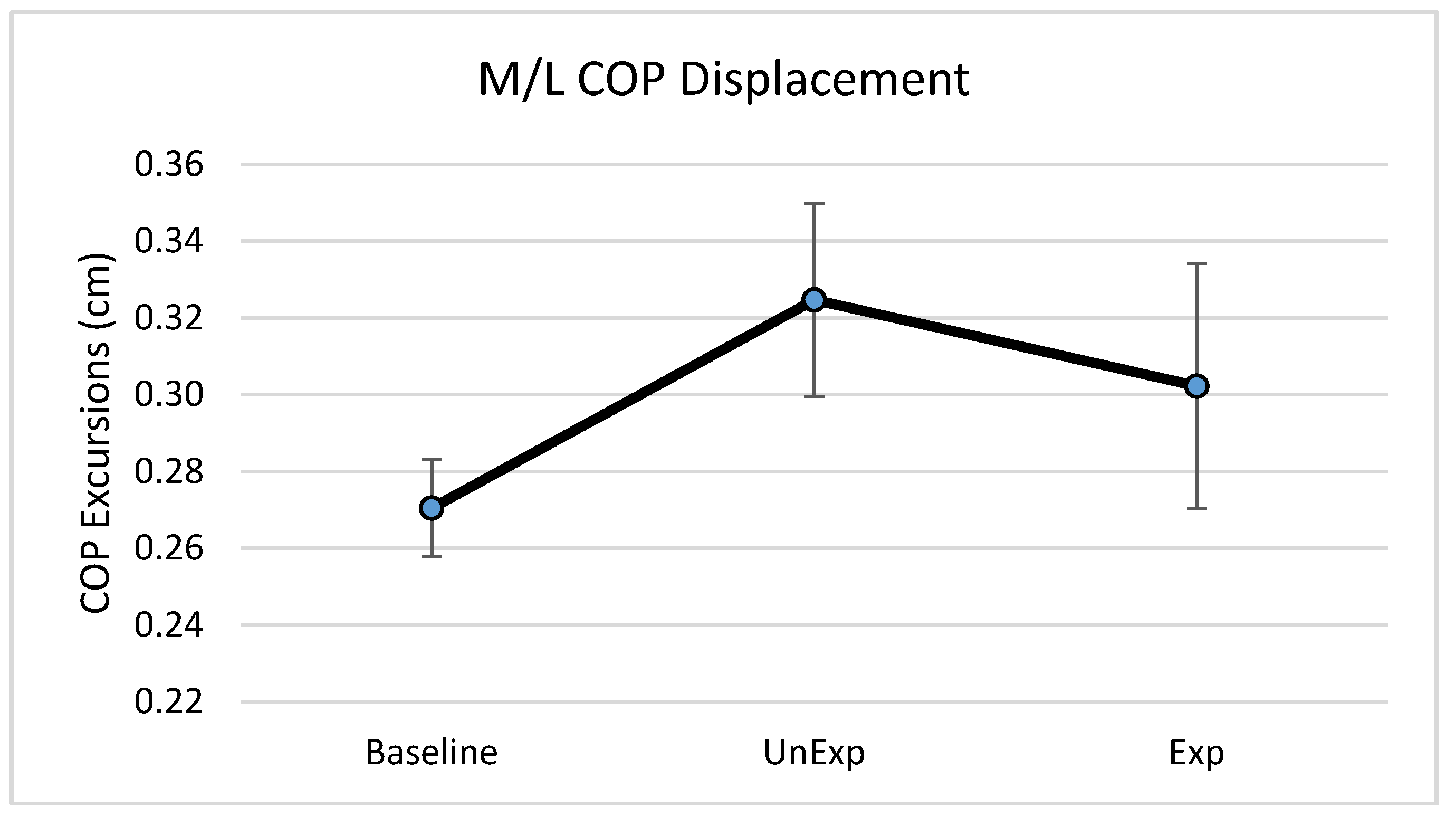
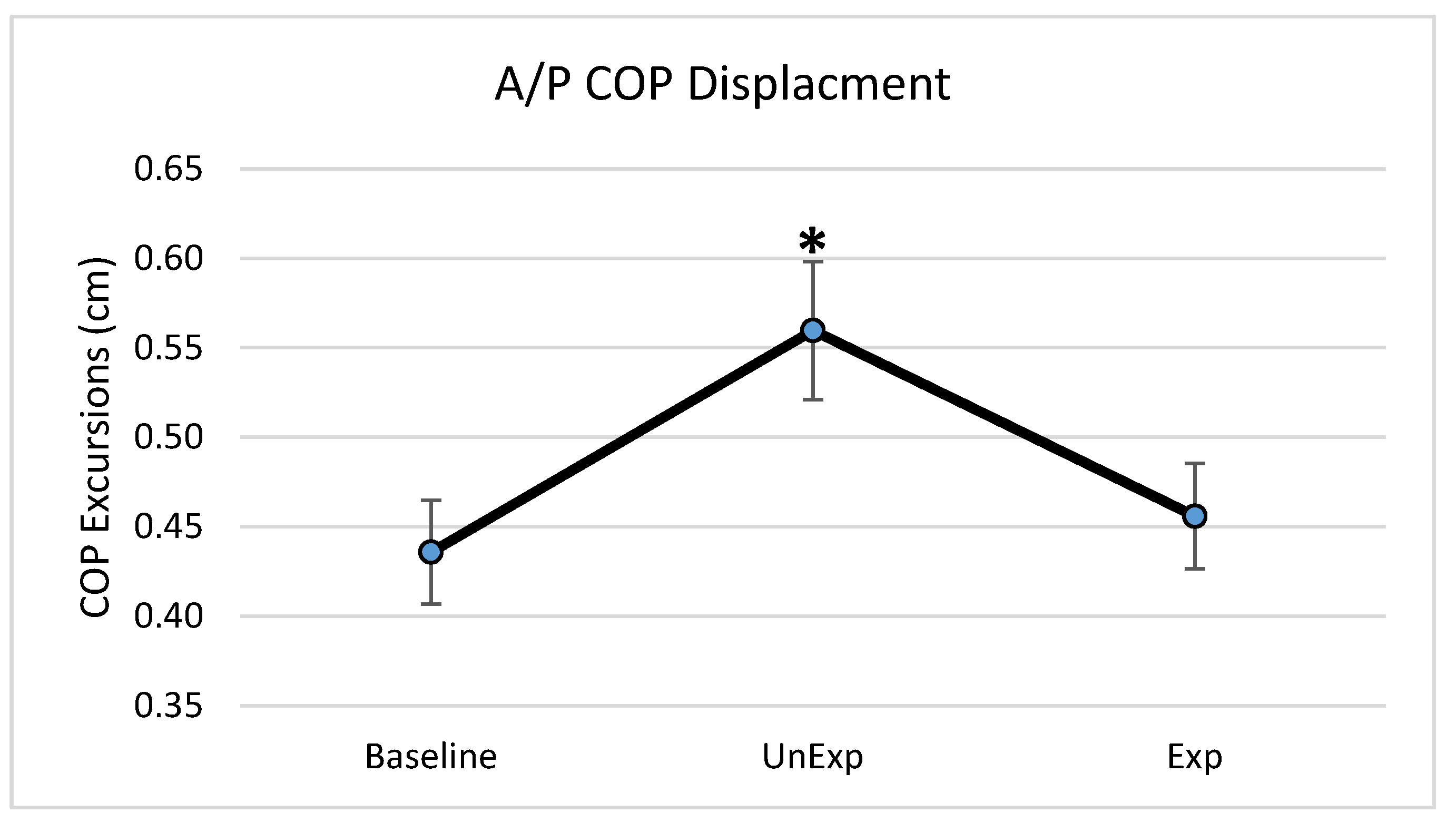
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Horak, F.B.; Nashner, L.M.; Diener, H.C. Postural strategies associated with somatosensory and vestibular loss. Exp. Brain Res. 1990, 82, 167–177. [Google Scholar] [CrossRef] [PubMed]
- Assländer, L.; Hettich, G.; Mergner, T. Visual contribution to human standing balance during support surface tilts. Hum. Mov. Sci. 2015, 41, 147–164. [Google Scholar] [CrossRef] [PubMed]
- Nagano, A.; Yoshioka, S.; Hay, D.C.; Himeno, R.; Fukashiro, S. Influence of vision and static stretch of the calf muscles on postural sway during quiet standing. Hum. Mov. Sci. 2006, 25, 422–434. [Google Scholar] [CrossRef] [PubMed]
- Sturnieks, D.L.; St George, R.; Lord, S.R. Balance disorders in the elderly. Neurophysiol. Clin. Clin. Neurophysiol. 2008, 38, 467–478. [Google Scholar] [CrossRef] [PubMed]
- Vuillerme, N.; Burdet, C.; Isableu, B.; Demetz, S. The magnitude of the effect of calf muscles fatigue on postural control during bipedal quiet standing with vision depends on the eye–visual target distance. Gait Posture 2006, 24, 169–172. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.N.; Aronson, E. Visual proprioceptive control of standing in human infants. Percept. Psychophys. 1974, 15, 529–532. [Google Scholar] [CrossRef]
- Belenkii, V.E.; Gurfinkel, V.S.; Paltsev, E.I. On the control elements of voluntary movements. Biofizika 1967, 12, 135–141. [Google Scholar]
- Horak, F.B.; Diener, H.C.; Nashner, L.M. Influence of central set on human postural responses. J. Neurophysiol. 1989, 62, 841–853. [Google Scholar] [CrossRef] [PubMed]
- Santos, M.J.; Aruin, A.S. Role of lateral muscles and body orientation in feedforward postural control. Exp. Brain Res. 2008, 184, 547–559. [Google Scholar] [CrossRef] [PubMed]
- Santos, M.J.; Kanekar, N.; Aruin, A.S. The role of anticipatory postural adjustments in compensatory control of posture: 1. Electromyographic analysis. J. Electromyogr. Kinesiol. 2010, 20, 388–397. [Google Scholar] [CrossRef] [PubMed]
- Santos, M.J.; Kanekar, N.; Aruin, A.S. The role of anticipatory postural adjustments in compensatory control of posture: 2. Biomechanical analysis. J. Electromyogr. Kinesiol. 2010, 20, 398–405. [Google Scholar] [CrossRef] [PubMed]
- Bugnariu, N.; Fung, J. Aging and selective sensorimotor strategies in the regulation of upright balance. J. NeuroEng. Rehabil. 2007, 4, 19. [Google Scholar] [CrossRef] [PubMed]
- Chiarovano, E.; Wang, W.; Rogers, S.J.; MacDougall, H.G.; Curthoys, I.S.; de Waele, C. Balance in virtual reality: Effect of age and bilateral vestibular loss. Front. Neurol. 2017, 8, 5. [Google Scholar] [CrossRef] [PubMed]
- Peterson, S.M.; Rios, E.; Ferris, D.P. Transient visual perturbations boost short-term balance learning in virtual reality by modulating electrocortical activity. J. Neurophysiol. 2018, 120, 1998–2010. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Jang, S.H.; Kim, C.S.; Jung, J.H.; You, J.H. Use of virtual reality to enhance balance and ambulation in chronic stroke: A double-blind, randomized controlled study. Am. J. Phys. Med. Rehabil. 2009, 88, 693–701. [Google Scholar] [CrossRef] [PubMed]
- Fung, J.; Richards, C.L.; Malouin, F.; McFadyen, B.J.; Lamontagne, A. A treadmill and motion coupled virtual reality system for gait training post-stroke. CyberPsychol. Behav. 2006, 9, 157–162. [Google Scholar] [CrossRef] [PubMed]
- Liao, Y.-Y.; Yang, Y.-R.; Cheng, S.-J.; Wu, Y.-R.; Fuh, J.-L.; Wang, R.-Y. Virtual reality–based training to improve obstacle-crossing performance and dynamic balance in patients with Parkinson’s disease. Neurorehabil. Neural Repair 2015, 29, 658–667. [Google Scholar] [CrossRef] [PubMed]
- Yang, W.-C.; Wang, H.-K.; Wu, R.-M.; Lo, C.-S.; Lin, K.-H. Home-based virtual reality balance training and conventional balance training in Parkinson’s disease: A randomized controlled trial. J. Formos. Med. Assoc. 2016, 115, 734–743. [Google Scholar] [CrossRef] [PubMed]
- American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2013; ISBN 978-1-4698-2666-0. [Google Scholar]
- Chander, H.; Garner, J.C.; Wade, C. Impact on balance while walking in occupational footwear. Footwear Sci. 2014, 6, 59–66. [Google Scholar] [CrossRef]
- Chander, H.; Morris, C.E.; Wilson, S.J.; Garner, J.C.; Wade, C. Impact of alternative footwear on human balance. Footwear Sci. 2016, 8, 165–174. [Google Scholar] [CrossRef]
- Chander, H.; Knight, A.C.; Garner, J.C.; Wade, C.; Carruth, D.; Wilson, S.J.; Gdovin, J.R.; Williams, C.C. Impact of military type footwear and load carrying workload on postural stability. Ergonomics 2019, 62, 103–114. [Google Scholar] [CrossRef] [PubMed]
- DeBusk, H.; Hill, C.M.; Chander, H.; Knight, A.C.; Babski-Reeves, K. Influence of military workload and footwear on static and dynamic balance performance. Int. J. Ind. Ergon. 2018, 64, 51–58. [Google Scholar] [CrossRef]
- Simpson, J.D.; Miller, B.L.; O’Neal, E.K.; Chander, H.; Knight, A.C. External load training does not alter balance performance in well-trained women. Sports Biomech. 2018, 17, 336–349. [Google Scholar] [CrossRef] [PubMed]
- Sobera, M.; Siedlecka, B.; Syczewska, M. Posture control development in children aged 2–7 years old, based on the changes of repeatability of the stability indices. Neurosci. Lett. 2011, 491, 13–17. [Google Scholar] [CrossRef] [PubMed]
- Knight, A.C.; Holmes, M.E.; Chander, H.; Kimble, A.; Stewart, J.T. Assessment of balance among adolescent track and field athletes. Sports Biomech. 2016, 15, 169–179. [Google Scholar] [CrossRef] [PubMed]
- Cordo, P.J.; Nashner, L.M. Properties of postural adjustments associated with rapid arm movements. J. Neurophysiol. 1982, 47, 287–302. [Google Scholar] [CrossRef] [PubMed]
- Pline, K.M.; Madigan, M.L.; Nussbaum, M.A. Influence of fatigue time and level on increases in postural sway. Ergonomics 2006, 49, 1639–1648. [Google Scholar] [CrossRef] [PubMed]
- Overstall, P.W.; Exton-Smith, A.N.; Imms, F.J.; Johnson, A.L. Falls in the elderly related to postural imbalance. Br. Med. J. 1977, 1, 261–264. [Google Scholar] [CrossRef] [PubMed]
- Warnica, M.J.; Weaver, T.B.; Prentice, S.D.; Laing, A.C. The influence of ankle muscle activation on postural sway during quiet stance. Gait Posture 2014, 39, 1115–1121. [Google Scholar] [CrossRef] [PubMed]
- Di Nardo, F.; Mengarelli, A.; Maranesi, E.; Burattini, L.; Fioretti, S. Assessment of the ankle muscle co-contraction during normal gait: A surface electromyography study. J. Electromyogr. Kinesiol. 2015, 25, 347–354. [Google Scholar] [CrossRef] [PubMed]
- Chambers, A.J.; Cham, R. Slip-related muscle activation patterns in the stance leg during walking. Gait Posture 2007, 25, 565–572. [Google Scholar] [CrossRef] [PubMed]
- Thapa, P.B.; Gideon, P.; Fought, R.L.; Kormicki, M.; Ray, W.A. Comparison of clinical and biomechanical measures of balance and mobility in elderly nursing home residents. J. Am. Geriatr. Soc. 1994, 42, 493–500. [Google Scholar] [CrossRef] [PubMed]
- Prieto, T.E.; Myklebust, J.B.; Hoffmann, R.G.; Lovett, E.G.; Myklebust, B.M. Measures of postural steadiness: Differences between healthy young and elderly adults. IEEE Trans. Biomed. Eng. 1996, 43, 956–966. [Google Scholar] [CrossRef] [PubMed]
- Schubert, P.; Kirchner, M. Ellipse area calculations and their applicability in posturography. Gait Posture 2014, 39, 518–522. [Google Scholar] [CrossRef] [PubMed]
- Aruin, A.S.; Latash, M.L. The role of motor action in anticipatory postural adjustments studied with self-induced and externally triggered perturbations. Exp. Brain Res. 1995, 106, 291–300. [Google Scholar] [CrossRef] [PubMed]
- Patel, P.; Bhatt, T. Adaptation to large-magnitude treadmill-based perturbations: Improvements in reactive balance response. Physiol. Rep. 2015, 3, e12247. [Google Scholar] [CrossRef] [PubMed]







© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chander, H.; Kodithuwakku Arachchige, S.N.K.; Hill, C.M.; Turner, A.J.; Deb, S.; Shojaei, A.; Hudson, C.; Knight, A.C.; Carruth, D.W. Virtual-Reality-Induced Visual Perturbations Impact Postural Control System Behavior. Behav. Sci. 2019, 9, 113. https://doi.org/10.3390/bs9110113
Chander H, Kodithuwakku Arachchige SNK, Hill CM, Turner AJ, Deb S, Shojaei A, Hudson C, Knight AC, Carruth DW. Virtual-Reality-Induced Visual Perturbations Impact Postural Control System Behavior. Behavioral Sciences. 2019; 9(11):113. https://doi.org/10.3390/bs9110113
Chicago/Turabian StyleChander, Harish, Sachini N. K. Kodithuwakku Arachchige, Christopher M. Hill, Alana J. Turner, Shuchisnigdha Deb, Alireza Shojaei, Christopher Hudson, Adam C. Knight, and Daniel W. Carruth. 2019. "Virtual-Reality-Induced Visual Perturbations Impact Postural Control System Behavior" Behavioral Sciences 9, no. 11: 113. https://doi.org/10.3390/bs9110113
APA StyleChander, H., Kodithuwakku Arachchige, S. N. K., Hill, C. M., Turner, A. J., Deb, S., Shojaei, A., Hudson, C., Knight, A. C., & Carruth, D. W. (2019). Virtual-Reality-Induced Visual Perturbations Impact Postural Control System Behavior. Behavioral Sciences, 9(11), 113. https://doi.org/10.3390/bs9110113